
Developing an Internet-Based Trauma Recovery Nursing Intervention Based on Swanson’s Theory of Caring for Trauma Recovery


Abstract
:1. Introduction
1.1. Background
1.2. Aim
2. Materials and Methods
2.1. Design
2.2. Ethical Considerations
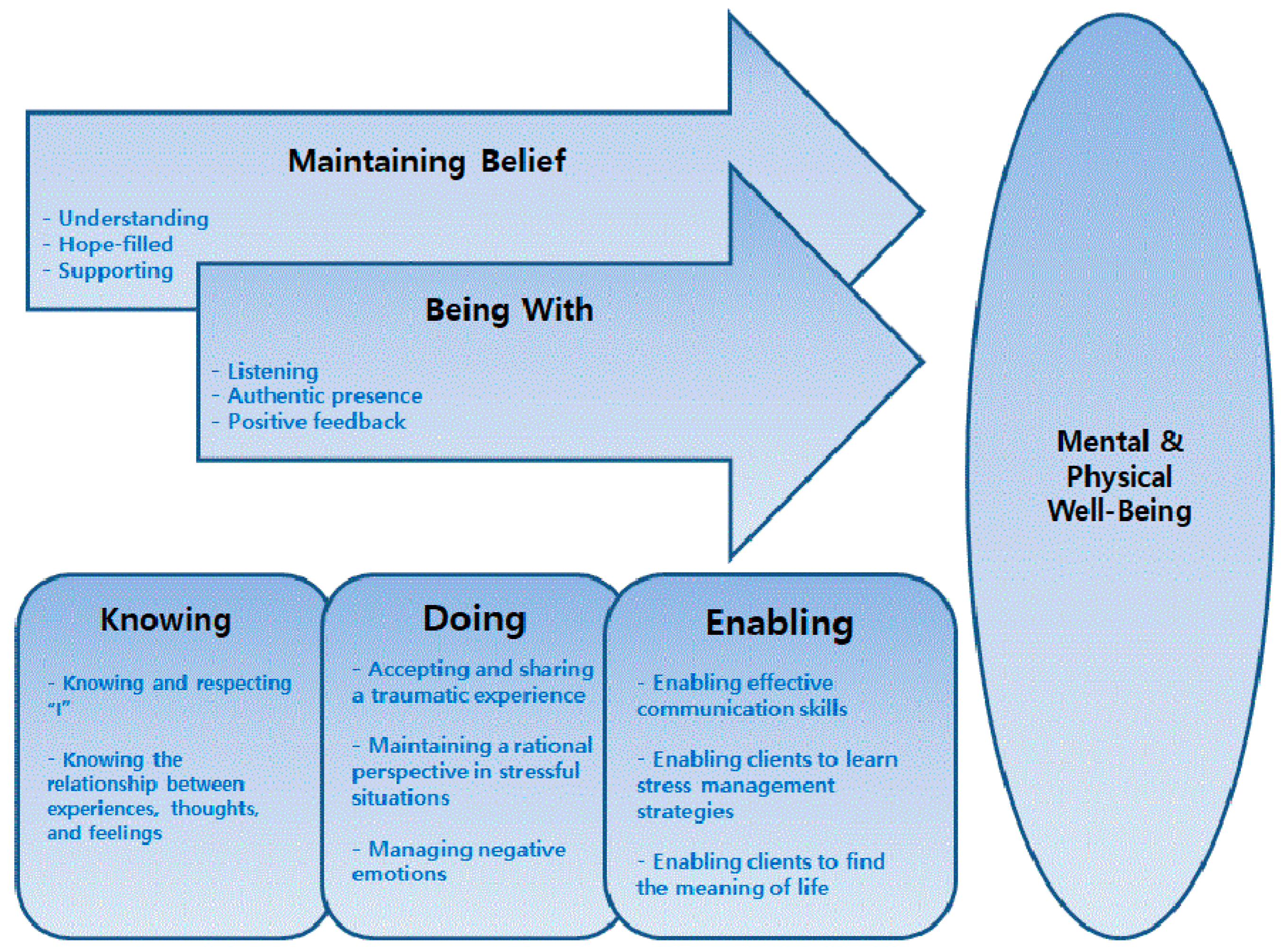
2.3. Conceptual Framework
2.4. Program Development Process
2.4.1. Stage I. Program Content Development Process
2.4.2. Stage II. Internet-Based Program Execution Process Development Process
3. Results
The Eight-Session Program
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kessler, R.C. Posttraumatic stress disorder: The burden to the individual and to society. J. Clin. Psychiatry 2000, 61 (Suppl. 5), 4–14. [Google Scholar] [PubMed]
- Magruder, K.M.; McLaughlin, K.A.; Elmore Borbon, D.L. Trauma is a public health issue. Eur. J. Psychotraumatol. 2017, 8, 1375338. [Google Scholar] [CrossRef]
- Simblett, S.; Birch, J.; Matcham, F.; Yaguez, L.; Morris, R. A systematic review and meta-analysis of e-mental health interventions to treat symptoms of posttraumatic stress. JMIR Ment. Health 2017, 4, e14. [Google Scholar] [CrossRef] [Green Version]
- Paik, J.-W.; Kim, H.-S.; Sim, M.; Lee, H.-K.; Woo, Y.S.; Chung, C.; Lee, S.-H.; Seok, J.-H.; Jeon, H.J.; Lee, S.-M.; et al. The Sewol ferry accident and early mental health care response by volunteer activities of Korean disaster mental health committee and members of Korean neuropsychiatric association. J. Korean Neuropsychiatr. Assoc. 2015, 54, 1–5. [Google Scholar] [CrossRef]
- Yang, H.J.; Cheong, H.K.; Choi, B.Y.; Shin, M.-H.; Yim, H.W.; Kim, D.-H.; Kim, G.; Lee, S.Y. Community mental health status six months after the Sewol ferry disaster in Ansan, Korea. Epidemiol. Health 2015, 37, e2015046. [Google Scholar] [CrossRef] [Green Version]
- Sijbrandij, M.; Olff, M.; Reitsma, J.B.; Carlier, I.V.; de Vries, M.H.; Gersons, B.P. Treatment of acute posttraumatic stress disorder with brief cognitive behavioral therapy: A randomized controlled trial. Am. J. Psychiatry 2007, 164, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Moulds, M.L.; Nixon, R.V. Cognitive behaviour therapy of acute stress disorder: A four-year follow-up. Behav. Res. Ther. 2003, 41, 489–494. [Google Scholar] [CrossRef]
- Mabey, L.; van Servellen, G. Treatment of post-traumatic stress disorder in patients with severe mental illness: A review. Int. J. Ment. Health Nurs. 2014, 23, 42–50. [Google Scholar] [CrossRef]
- Bride, B.E. Prevalence of secondary traumatic stress among social workers. Soc. Work 2007, 52, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Atkins, C.D.; Burnett, H.J., Jr. Specialized disaster behavioral health training: Its connection with response, practice, trauma health, and resilience. Disaster Health 2016, 3, 57–65. [Google Scholar] [CrossRef] [Green Version]
- Bruce, M.M.; Kassam-Adams, N.; Rogers, M.; Anderson, K.M.; Sluys, K.P.; Richmond, T.S. Trauma providers’ knowledge, views and practice of trauma-informed care. J. Trauma Nurs. 2018, 25, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, S.A.; Kong, S. Resilience mediates impact of some childhood maltreatment on post-traumatic stress symptoms in conscripted marines in the Republic of Korea. Res. Nurs. Health 2017, 40, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.S.; Kim, H.R. Impact of childhood trauma and social support on dissociative symptoms in Marines. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2016, 24, 257–266. [Google Scholar] [CrossRef]
- Lewis, C.E.; Farewell, D.; Groves, V.; Kitchiner, N.J.; Roberts, N.P.; Vick, T.; Bisson, J.I. Internet-based guided self-help for posttraumatic stress disorder (PTSD): Randomized controlled trial. Depress. Anxiety 2017, 34, 555–565. [Google Scholar] [CrossRef] [Green Version]
- Silva Butcher, R.G.C.; Jones, D.A. An integrative review of comprehensive nursing assessment tools developed based on Gordon’s Eleven Functional Health Patterns. Int. J. Nurs. Knowl. 2021. [Google Scholar] [CrossRef]
- Swanson, K.M. Empirical development of a middle range theory of caring. Nurs. Res. 1991, 40, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, K.; Roscigno, C.I.; Swanson, K.M.; Savage, T.A.; Kimura, R.E.; Kilpatrick, S.J. Perinatal palliative care: Parent perceptions of caring in interactions surrounding counseling for risk of delivering an extremely premature infant. Palliat. Support. Care 2015, 13, 145–155. [Google Scholar] [CrossRef]
- Higdon, K.; Shirey, M. Implementation of a caring theoretical framework in a multihospital system. J. Nurs. Adm. 2012, 42, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Tonges, M.; Ray, J. Translating caring theory into practice: The carolina care Model. J. Nurs. Adm. 2011, 41, 374–381. [Google Scholar] [CrossRef]
- Choi, Y.K. Evidence-based treatment of posttraumatic stress disorder. Korean J. Clin. Psychol. 2017, 36, 526–549. [Google Scholar] [CrossRef]
- Marshall, J.M.; Dunstan, D.A.; Bartik, W. The role of digital mental health resources to treat trauma symptoms in Australia during COVID-19. Psychol. Trauma 2020, 12 (Suppl. 1), S269–S271. [Google Scholar] [CrossRef] [PubMed]
- Price, M.; Sawyer, T.; Harris, M.; Skalka, C. Usability evaluation of a mobile monitoring system to assess symptoms after a traumatic injury: A mixed-methods study. JMIR Ment. Health 2016, 3, e3. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.; Roberts, N.P.; Bethell, A.; Robertson, L.; Bisson, J.I. Internet-based cognitive and behavioural therapies for post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst. Rev. 2018, CD011710. [Google Scholar] [CrossRef]
- Kalfoss, M.; Owe, J. Empirical verification of Swanson’s caring processes found in nursing actions: Systematic review. Open J. Nurs. 2015, 5, 976–986. [Google Scholar] [CrossRef] [Green Version]
- Swanson, K.M.; Chen, H.T.; Graham, J.C.; Wojnar, D.M.; Petras, A. Resolution of depression and grief during the first year after miscarriage: A randomized controlled clinical trial of couples-focused interventions. J. Women’s Health 2009, 18, 1245–1257. [Google Scholar] [CrossRef] [Green Version]
- Finfgeld-Connett, D. Meta-synthesis of caring in nursing. J. Clin. Nurs. 2008, 17, 196–204. [Google Scholar] [CrossRef]
- Huynh, T.; Alderson, M.; Thompson, M. Emotional labour underlying caring: An evolutionary concept analysis. J. Adv. Nurs. 2008, 64, 195–208. [Google Scholar] [CrossRef]
- Schlosser, D.; Campellone, T.; Kim, D.; Truong, B.; Vergani, S.; Ward, C.; Vinogradov, S. Feasibility of PRIME: A cognitive neuroscience-informed mobile app intervention to enhance motivated behavior and improve quality of life in recent onset schizophrenia. JMIR Res. Protoc. 2016, 5, e77. [Google Scholar] [CrossRef]
- Gander, F.; Proyer, R.T.; Ruch, W. Positive psychology interventions addressing pleasure, engagement, meaning, positive relationships, and accomplishment increase well-being and ameliorate depressive symptoms: A randomized, placebo-controlled online study. Front. Psychol. 2016, 7, 686. [Google Scholar] [CrossRef] [Green Version]
- Proyer, R.T.; Gander, F.; Wellenzohn, S.; Ruch, W. Strengths-based positive psychology interventions: A randomized placebo-controlled online trial on long-term effects for a signature strengths-vs. a lesser strengths-intervention. Front. Psychol. 2015, 6, 456. [Google Scholar] [CrossRef] [Green Version]
- Hudon, C.; Tribble, D.S.; Bravo, G.; Poitras, M.E. Enablement in health care context: A concept analysis. J. Eval. Clin. Pract. 2011, 17, 143–149. [Google Scholar] [CrossRef] [PubMed]
- de Zwaan, M.; Herpertz, S.; Zipfel, S.; Svaldi, J.; Friederich, H.C.; Schmidt, F.; Mayr, A.; Lam, T.; Schade-Brittinger, C.; Hilbert, A. Effect of internet-based guided self-help vs individual face-to-face treatment on full or subsyndromal binge eating disorder in overweight or obese patients: The interbed randomized clinical trial. JAMA Psychiatry 2017, 74, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Kim, G.-U.; Yoon, H.J.; Kim, S. A systematic review of the effect of web-based trauma-education programs for mental-health professionals. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2020, 29, 325–338. [Google Scholar] [CrossRef]
- Andrews, G.; Cuijpers, P.; Craske, M.G.; McEvoy, P.; Titov, N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: A meta-analysis. PLoS ONE 2010, 5, e13196. [Google Scholar] [CrossRef] [PubMed]
- Donker, T.; Petrie, K.; Proudfoot, J.; Clarke, J.; Birch, M.R.; Christensen, H. Smartphones for smarter delivery of mental health programs: A systematic review. J. Med. Internet Res. 2013, 15, e247. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Participant Feedback | Modifications Reflecting the Feedback |
|---|---|
| Lack of two-way communication “There is a lack of intimacy and communication with the therapist.” “There was no communication with the therapist. It felt as though the program was delivered unilaterally.” “It was unfortunate that I could not build a rapport with therapist.” “It would be good if a support system could be formed through constant communication with the therapist.” | Added individual response letter for interactive communication. If the client wished, an on/offline interview was made possible at any time. |
| Difficulty with narrative responses to questions “It was difficult because I was unfamiliar with describing narrative responses.” “I was hesitant about what to write for the question.” “It would be better to reduce the number of narrative questions and provide brief options for the answers.” | A guideline for the response was provided with examples of possible narrative responses. |
| Lack of program instruction “It would be nice if there were a guide available for the program before starting it.” “I started without knowing what kind of program it was, but it took more time than expected and it was difficult.” | Before the start of the program, detailed explanations were provided on the background and purpose of the program, and on how to respond. |
| Need for specific questions “Be specific about what you are asking. I wasn’t sure if I was responding correctly when I responded.” “When answering the question, it seemed that a specific example for each question is needed.” “It would be nice if you could explain exactly what the question was asking. For example, I was confused about how much anxiety ‘anxiety’ meant.” | The questions in each session were specifically changed and examples of the response were provided to make it easier for the clients to answer. |
| The amount and structure of the content in relation to providing it online “The content was only composed of text, so I grew tired easily.” “It would be nice to make the program less boring by including things like pictures and videos.” “It was difficult to concentrate on the program because there were too many explanations provided in text on my cellphone.” | The program was amended through reduction and simplification of the written content, and through the addition of pictures, photos, and videos that could be provided online. |
| Session | Swanson’s Caring Theory Process | Themes and Major Content | Guided Self-Help Questions for Trauma Recovery |
|---|---|---|---|
| 1 | Knowing | Knowing and respecting “I” Learning knowledge related to trauma Understanding the importance of living happily Trying to find my strengths Practicing mental control through abdominal breathing | Asking questions to find strengths Asking questions about happy experiences and situations Trying to introduce experiences of difficult times |
| 2 | Knowing | Knowing the relationship between experiences, thoughts, and feelings Recognizing changes after painful experiences Finding meaning and goals in life to find happiness away from traumatic experiences Understanding the link between physical activity and mental health Learning body stabilization Practicing mental control through body stabilization | Asking questions about difficult situations and hard times Asking questions about how to cope with getting out of difficult situations Remembering positive emotions and gratitude |
| 3 | Doing for | Accepting and sharing traumatic experiences Using self-disclosure Identifying the influencing factors of negative emotions and thoughts Learning to manage negative emotions Practicing mental control through abdominal breathing | Sharing traumatic experiences Remembering positive thoughts and emotions in daily life Asking questions that establish the relationship between negative thoughts, emotions, and behaviors Changing negative emotions using the “imagination” |
| 4 | Doing for | Maintaining a rational perspective in stressful situations Trying to have objectiveness Identifying the benefits of rational thinking Expanding one’s worldview and perspective in a safe environment Practicing mental through body stabilization | Remembering and enjoying strengths Recognizing the degree of negative emotion Applying a management strategy to change negative emotions Writing from a positive perspective |
| 5 | Doing for | Managing negative emotions Identifying positive and negative emotions Expanding positive emotions as a strength Recognizing and enjoying the benefits of positive emotions Practicing mental control through abdominal breathing | Asking questions to restore positive emotions Asking questions about experiences that encourage confidence and happiness in daily life |
| 6 | Enabling | Enabling effective communication skills Learning assertive and responsible communication skills Analyzing communication patterns in stressful situations Finding problems and weaknesses in communication in relationships that have conflict Practicing mental control through body stabilization | Asking questions about the types of communication Asking questions on how to communicate appropriately and effectively in difficult situations and situations with conflict Applying assertive communication skills in daily life |
| 7 | Enabling | Learning a stress management strategy Finding strategies to reduce stress Finding a way to manage stress by using strengths Learning confrontation and refusing skills for unreasonable requests Learning to “butterfly embrace” Practicing mental control through abdominal breathing | Identifying stressful situations Asking questions about experiences related to using strengths to manage stress Paying compliments for overcoming stress |
| 8 | Enabling | Finding the meaning of life in everyday living Identifying changes in daily life after participating in the program Finding gratitude in daily life Finding satisfaction and meaning in life Mind control through body stabilization | Asking questions to recognize self-change in daily life through the program Asking questions about perceived meaning and happiness in life Trying to incorporate positive self-talk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Kim, G.-U.; Lee, W.; Park, J. Developing an Internet-Based Trauma Recovery Nursing Intervention Based on Swanson’s Theory of Caring for Trauma Recovery. Int. J. Environ. Res. Public Health 2021, 18, 6715. https://doi.org/10.3390/ijerph18136715
Kim S, Kim G-U, Lee W, Park J. Developing an Internet-Based Trauma Recovery Nursing Intervention Based on Swanson’s Theory of Caring for Trauma Recovery. International Journal of Environmental Research and Public Health. 2021; 18(13):6715. https://doi.org/10.3390/ijerph18136715
Chicago/Turabian StyleKim, Sunah, Go-Un Kim, Wongyeong Lee, and Jinyoung Park. 2021. "Developing an Internet-Based Trauma Recovery Nursing Intervention Based on Swanson’s Theory of Caring for Trauma Recovery" International Journal of Environmental Research and Public Health 18, no. 13: 6715. https://doi.org/10.3390/ijerph18136715
APA StyleKim, S., Kim, G. -U., Lee, W., & Park, J. (2021). Developing an Internet-Based Trauma Recovery Nursing Intervention Based on Swanson’s Theory of Caring for Trauma Recovery. International Journal of Environmental Research and Public Health, 18(13), 6715. https://doi.org/10.3390/ijerph18136715