
Changes in Visual Performance under the Effects of Moderate–High Alcohol Consumption: The Influence of Biological Sex

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Alcohol Administration
2.3. Vision Assessment
2.3.1. Contrast Sensitivity and Night Vision
2.3.2. Stereopsis
2.3.3. Retinal Image Quality
2.4. Data Analysis
3. Results
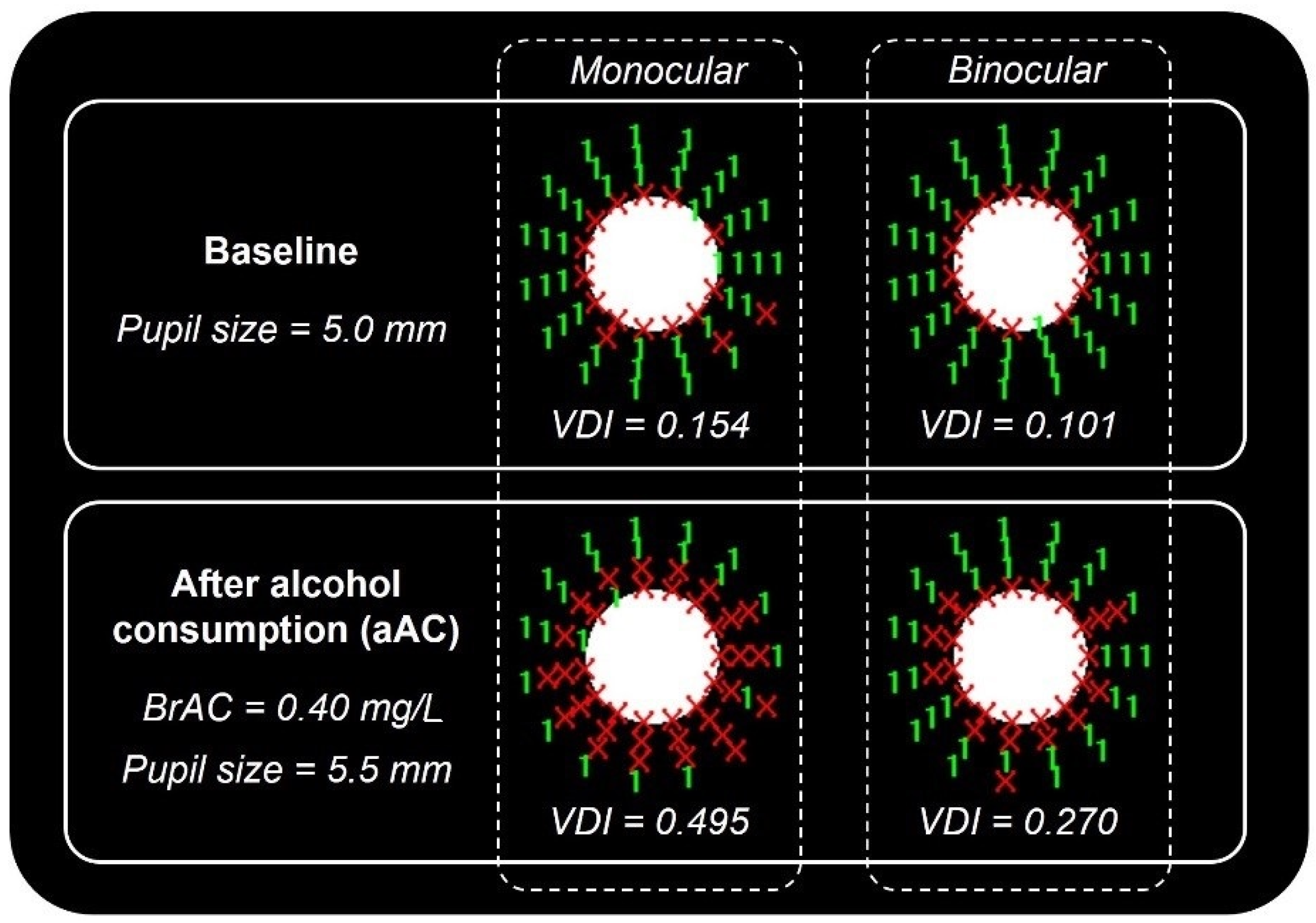
3.1. Visual Discrimination Capacity and Pupil Size
3.2. Stereopsis
3.3. Contrast Sensitivity
3.4. Retinal Image Quality
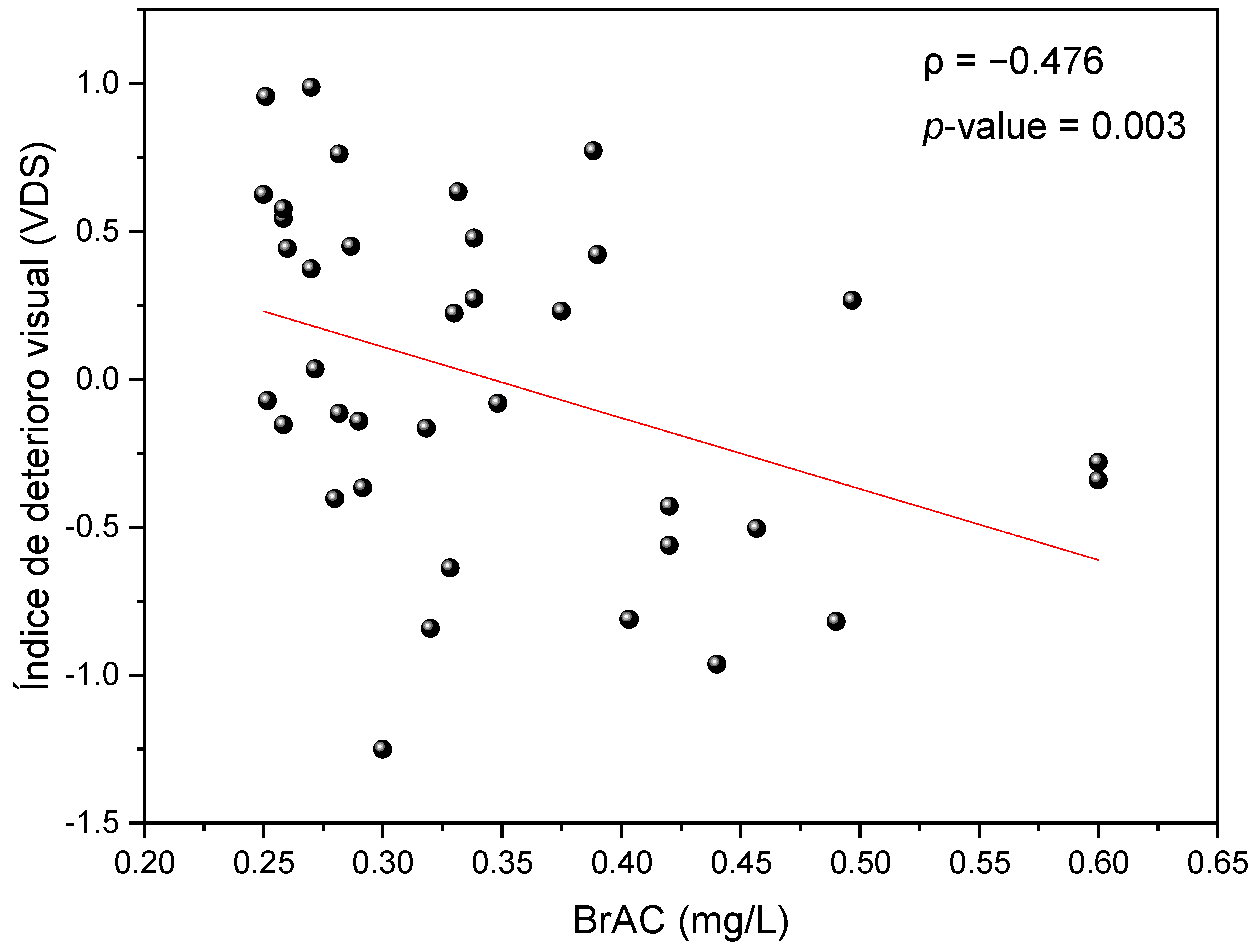
3.5. Influence of Biological Sex
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Casares-Lopez, M.; Castro-Torres, J.J.; Martino, F.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Contrast sensitivity and retinal straylight after alcohol consumption: Effects on driving performance. Sci. Rep. 2020, 10, 13599. [Google Scholar] [CrossRef]
- Watten, R.G.; Lie, I. Visual functions and acute ingestion of alcohol. Ophthalmic Physiol. Opt. 1996, 16, 460–466. [Google Scholar] [CrossRef]
- Roquelaure, Y.; Legargasson, J.F.; Kupper, S.; Girre, C.; Hispard, E.; Dally, S. Alcohol-consumption and visual contrast sensitivity. Alcohol Alcohol. 1995, 30, 681–685. [Google Scholar] [PubMed]
- Hill, J.C.; Toffolon, G. Effect of alcohol on sensory and sensorimotor visual functions. J. Stud. Alcohol 1990, 51, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Wilson, G.; Mitchell, R. The effect of alcohol on the visual and ocular motor systems. Aust. J. Ophthalmol. 1983, 11, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Hogan, R.E.; Gilmartin, B. The relationship between tonic vergence and oculomotor stress-induced by ethanol. Ophthalmic Physiol. Opt. 1985, 5, 43–51. [Google Scholar] [CrossRef]
- Munsamy, A.J.; Hamilton-Hoskins, R.S.; Bero, T.; Ximba, P.P.; Govender, D.; Soni, M.; Majola, L. The effect of acute ingestion of alcohol at 0.05% and 0.10% blood respiratory alcohol concentration on heterophoria. Afr. Vis. Eye Health J. 2016, 75, 7. [Google Scholar] [CrossRef]
- Casares-López, M.; Castro-Torres, J.J.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Changes in accommodation dynamics after alcohol consumption, for two different doses. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 919–928. [Google Scholar] [CrossRef]
- Saladin, J.J. Effects of Heterophoria on stereopsis. Optom. Vis. Sci. 1995, 72, 487–492. [Google Scholar] [CrossRef]
- Spencer, S.; Firth, A.Y. Stereoacuity is affected by induced phoria but returns toward baseline during vergence adaptation. J. Aapos 2007, 11, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Hogan, R.E.; Linfield, P.B. The effects of moderate doses of ethanol on heterophoria and other aspects of binocular vision. Ophthalmic Physiol. Opt. 1983, 3, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Martino, F.; Castro-Torres, J.J.; Casares-Lopez, M.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Deterioration of binocular vision after alcohol intake influences driving performance. Sci. Rep. 2021, 11, 8904. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.J.; Pozo, A.M.; Rubino, M.; Anera, R.G.; del Barco, L.J. Retinal-Image Quality and Night-Vision Performance after Alcohol Consumption. J. Ophthalmol. 2014, 2014, 704823. [Google Scholar] [CrossRef] [PubMed]
- Castro, J.J.; Ortiz, C.; Pozo, A.M.; Anera, R.G.; Soler, M. A visual test based on a freeware software for quantifying and displaying night-vision disturbances: Study in subjects after alcohol consumption. Theor. Biol. Med. Model. 2014, 11, S1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutker, P.B.; Tabakoff, B.; Goist, K.C.; Randall, C.L. Acute alcohol-intoxication, mood states and alcohol metabolism in women and men. Pharmacol. Biochem. Behav. 1983, 18, 349–354. [Google Scholar] [CrossRef]
- Coleharding, S.; Wilson, J.R. Ethanol-metabolism in men and women. J. Stud. Alcohol 1987, 48, 380–387. [Google Scholar] [CrossRef]
- Cederbaum, A.I. Alcohol Metabolism. Clin. Liver Dis. 2012, 16, 667–685. [Google Scholar] [CrossRef] [Green Version]
- Merritt, P.; Hirshman, E.; Wharton, W.; Stangl, B.; Devlin, J.; Lenz, A. Evidence for gender differences in visual selective attention. Personal. Individ. Differ. 2007, 43, 597–609. [Google Scholar] [CrossRef]
- Miller, R.J.; Pigion, R.G.; Martin, K.D. The effects of ingested alcohol on accommodation. Percept. Psychophys. 1985, 37, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.C.; Wang, H.; Tzvetanov, T.; Zhou, Y.F. Moderate acute alcohol intoxication increases visual motion repulsion. Sci. Rep. 2018, 8, 1607. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, M.E.; Andre, J.T.; Tyrrell, R.A.; Wang, M.Q.; Leibowitz, H.W. Effects of moderate dose alcohol on visual contrast sensitivity for stationary and moving targets. J. Stud. Alcohol 1995, 56, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Maissa, C.; Guillon, M. Tear film dynamics and lipid layer characteristics-Effect of age and gender. Contact Lens Anterior Eye 2010, 33, 176–182. [Google Scholar] [CrossRef]
- Maudens, K.E.; Patteet, L.; van Nuijs, A.L.N.; Van Broekhoven, C.; Covaci, A.; Neels, H. The influence of the body mass index (BMI) on the volume of distribution of ethanol. Forensic Sci. Int. 2014, 243, 74–78. [Google Scholar] [CrossRef]
- Babor, T.F.; de la Fuente, J.R.; Saunders, J.; Grant, M. AUDIT-The Alcohol Use Identification Test: Guidelines for Use in Primary Health Care; Department of Mental Health and Substance Dependence, World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Forrest, A.R.W. The estimation of Widmarks factor. J. Forensic Sci. Soc. 1986, 26, 249–252. [Google Scholar] [CrossRef]
- Armstrong, R.A. Statistical guidelines for the analysis of data obtained from one or both eyes. Ophthalmic Physiol. Opt. 2013, 33, 7–14. [Google Scholar] [CrossRef]
- Castro, J.J.; Jimenez, J.R.; Ortiz, C.; Alarcon, A.; Anera, R.G. New testing software for quantifying discrimination capacity in subjects with ocular pathologies. J. Biomed. Opt. 2011, 16, 015001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moganeswari, D.; Thomas, J.; Srinivasan, K.; Jacob, G.P. Test Re-Test Reliability and Validity of Different Visual Acuity and Stereoacuity Charts Used in Preschool Children. J. Clin. Diagn. Res. 2015, 9, NC01–NC05. [Google Scholar] [CrossRef]
- Westheimer, G. Clinical evaluation of stereopsis. Vis. Res. 2013, 90, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Artal, P.; Benito, A.; Perez, G.M.; Alcon, E.; De Casas, A.; Pujol, J.; Marin, J.M. An Objective Scatter Index Based on Double-Pass Retinal Images of a Point Source to Classify Cataracts. PLoS ONE 2011, 6, e16823. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Roda, J.A.; Vilaseca, M.; Ondategui, J.C.; Giner, A.; Burgos, F.J.; Cardona, G.; Pujol, J. Optical quality and intraocular scattering in a healthy young population. Clin. Exp. Optom. 2011, 94, 223–229. [Google Scholar] [CrossRef]
- Lee, H.; Lee, K.; Ahn, J.M.; Kim, E.K.; Sgrignoli, B. Double-Pass System Assessing the Optical Quality of Pseudophakic Eyes. Optom. Vis. Sci. 2014, 91, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Castro-Torres, J.J.; Martino, F.; Casares-Lopez, M.; Ortiz-Peregrina, S.; Ortiz, C. Visual performance after the deterioration of retinal image quality: Induced forward scattering using Bangerter foils and fog filters. Biomed. Opt. Express 2021, 12, 2902–2918. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Peregrina, S.; Ortiz, C.; Salas, C.; Casares-Lopez, M.; Soler, M.; Anera, R.G. Intraocular scattering as a predictor of driving performance in older adults with cataracts. PLoS ONE 2020, 15, e0227892. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.W.; Neri, A. Age-related differences in the effects of ethanol on performance and behavior in healthy-men. Alcohol Alcohol. 1994, 29, 171–179. [Google Scholar]
- Hindmarch, I.; Bhatti, J.Z.; Starmer, G.A.; Mascord, D.J.; Kerr, J.S.; Sherwood, N. The effects of alcohol on the cognitive function of males and females and on skills relating to car driving. Hum. Psychopharmacol. Clin. Exp. 1992, 7, 105–114. [Google Scholar]
- Piano, M.E.; Tidbury, L.P.; O’Connor, A.R. Normative Values for Near and Distance Clinical Tests of Stereoacuity. Strabismus 2016, 24, 169–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, S.; Vatsa, M.; Singh, R.; Jain, A. Iris Recognition under Alcohol Influence: A Preliminary Study. In Proceedings of the 2012 5th IAPR International Conference on Biometrics, New Delhi, India, 29 March–1 April 2012. [Google Scholar] [CrossRef] [Green Version]
- Piñero, D.P.; Ortiz, D.; Alio, J.L. Ocular Scattering. Optom. Vis. Sci. 2010, 87, E682–E696. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Nam, W.H.; Yi, K.; Choi, D.G.; Hyon, J.Y.; Wee, W.R.; Shin, Y.J. Oral Alcohol Administration Disturbs Tear Film and Ocular Surface. Ophthalmology 2012, 119, 965–971. [Google Scholar] [CrossRef]
- Simsek, C.; Kojima, T.; Dogru, M.; Tanaka, M.; Takano, Y.; Wakamatsu, T.; Ibrahim, O.; Toda, I.; Negishi, K.; Tsubota, K. The Early Effects of Alcohol Consumption on Functional Visual Acuity, Tear Functions, and the Ocular Surface. Eye Contact Lens 2021, 47, 20–26. [Google Scholar] [CrossRef]
- Adams, A.J.; Brown, B.; Flom, M.C. Alcohol-induced changes in contrast sensitivity following high-intensity light exposure. Percept. Psychophys. 1976, 19, 219–225. [Google Scholar] [CrossRef]
- Pearson, P.; Timney, B. Effects of moderate blood alcohol concentrations on spatial and temporal contrast sensitivity. J. Stud. Alcohol 1998, 59, 163–173. [Google Scholar] [CrossRef]
- Andre, J.T.; Tyrrell, R.A.; Leibowitz, H.W.; Nicholson, M.E.; Wang, M.Q. Measuring and predicting the effects of alcohol-consumption on contrast sensitivity for stationary and moving gratings. Percept. Psychophys. 1994, 56, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Owsley, C. Vision and Aging. In Annual Review of Vision Science2; Movshon, J.A., Wandell, B.A., Eds.; Annual Review of Vision Science; Annual Reviews: Palo Alto, CA, USA, 2016; Volume 2, pp. 255–271. [Google Scholar]
- Liang, J.Z.; Williams, D.R. Aberrations and retinal image quality of the normal human eye. J. Opt. Soc. Am. A-Opt. Image Sci. Vis. 1997, 14, 2873–2883. [Google Scholar] [CrossRef] [PubMed]
- Kobashi, H.; Kamiya, K.; Yanome, K.; Igarashi, A.; Shimizu, K. Effect of Pupil Size on Optical Quality Parameters in Astigmatic Eyes Using a Double-Pass Instrument. Biomed. Res. Int. 2013, 2013, 124327. [Google Scholar] [CrossRef]
- Iijima, A.; Shimizu, K.; Kobashi, H.; Saito, A.; Kamiya, K. Repeatability, Reproducibility, and Comparability of Subjective and Objective Measurements of Intraocular Forward Scattering in Healthy Subjects. Biomed. Res. Int. 2015, 2015, 925217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz-Peregrina, S.; Ortiz, C.; Castro-Torres, J.J.; Jimenez, J.R.; Anera, R.G. Effects of Smoking Cannabis on Visual Function and Driving Performance. A Driving-Simulator Based Study. Int. J. Environ. Res. Public Health 2020, 17, 9033. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Peregrina, S.; Ortiz, C.; Casares-López, M.; Jiménez, J.R.; Anera, R.G. Effects of cannabis on visual function and self-perceived visual quality. Sci. Rep. 2021, 11, 1655. [Google Scholar] [CrossRef]
- Nawrot, M.; Nordenstrom, B.; Olson, A. Disruption of eye movements by ethanol intoxication affects perception of depth from motion parallax. Psychol. Sci. 2004, 15, 858–865. [Google Scholar] [CrossRef]
- Brooks, J.O.; Tyrrell, R.A.; Frank, T.A. The effects of severe visual challenges on steering performance in visually healthy young drivers. Optom. Vis. Sci. 2005, 82, 689–697. [Google Scholar] [CrossRef]
- Michael, R.; van Rijn, L.J.; van den Berg, T.; Barraquer, R.I.; Grabner, G.; Wilhelm, H.; Coeckelbergh, T.; Emesz, M.; Marvan, P.; Nischler, C. Association of lens opacities, intraocular straylight, contrast sensitivity and visual acuity in European drivers. Acta Ophthalmol. 2009, 87, 666–671. [Google Scholar] [CrossRef]
- Charlton, S.G.; Starkey, N.J. Driving while drinking: Performance impairments resulting from social drinking. Accid. Anal. Prev. 2015, 74, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.L.; Li, X.W.; Zhao, X.H.; Zhang, Q.Z. Effects of Different Alcohol Dosages on Steering Behavior in Curve Driving. Hum. Factors 2019, 61, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Niaura, R.S.; Nathan, P.E.; Frankenstein, W.; Shapiro, A.P.; Brick, J. Gender differences in acute psychomotor, cognitive, and pharmacokinetic response to alcohol. Addict. Behav. 1987, 12, 345–356. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline | aAC | Z; p-Value | Cohen’s d | Deterioration | |
|---|---|---|---|---|---|
| VDI (MON) | 0.21 ± 0.02 | 0.31 ± 0.03 | Z(36) = −3.718 p < 0.001 | 1.545 | −0.09 ± 0.02 |
| VDI (BIN) | 0.14 ± 0.01 | 0.19 ± 0.02 | Z(36) = −2.826 p = 0.005 | 1.049 | −0.05 ± 0.02 |
| Pupil size (mm) | 5.6 ± 0.2 | 5.9 ± 0.2 | t(36) = −4.235 p < 0.001 | 0.696 | −0.3 ± 0.1 |
| Distance stereoacuity (arc sec) | 52.7 ± 6.66 | 128.3 ± 14.14 | Z(36) = −4.711 p < 0.001 | 2.449 | −80.3 ± 13.92 |
| Near stereoacuity (arc sec) | 18.2 ± 2.76 | 38.6 ± 6.38 | Z(36) = −4.482 p < 0.001 | 2.180 | −20.0 ± 2.96 |
| CS (MON) | 124.9 ± 3.39 | 99.9 ± 3.62 | t(36) = 6.690 p < 0.001 | 1.115 | 25.0 ± 3.62 |
| CS (BIN) | 149.8 ± 2.84 | 130.1 ± 4.76 | t(36) = 5.906 p < 0.001 | 0.984 | 9.8 ± 1.61 |
| Retinal Image Quality | Baseline | aAC | t; p-Value | Cohen’s d | Deterioration | |
|---|---|---|---|---|---|---|
| Strehl ratio | 4 mm | 0.23 ± 0.01 | 0.20 ± 0.01 | t(36) = 3.014; p = 0.005 | 0.191 | 0.03 ± 0.01 |
| 5 mm | 0.21 ± 0.01 | 0.17 ± 0.01 | t(36) = 3.672; p < 0.001 | 1.211 | 0.03 ± 0.01 | |
| MTF cut-off (cpd) | 4 mm | 41.13 ±1.50 | 35.34 ± 1.58 | t(36) = 5.492; p = 0.001 | 1.836 | 5.53 ± 0.92 |
| 5 mm | 36.31 ± 1.82 | 31.28 ± 1.65 | t(36) = 4.328; p < 0.001 | 1.405 | 6.21 ± 1.47 | |
| OSI (4 mm) | 0.56 ± 0.06 | 0.82 ± 0.10 | Z(36) = −4.166 p < 0.001 | 1.880 | −0.24 ± 0.06 | |
| Visual Variable | t Statistic | p-Value | Cohen’s d |
| Mon CS | −3.074 | 0.004 * | 0.913 |
| Bin CS | −1.510 | 0.140 | 0.489 |
| Strehl ratio 4 mm | −1.037 | 0.307 | 0.356 |
| Strehl ratio 5 mm | −2.217 | 0.034 * | 0.710 |
| MTF cut-off 4 mm | −1.566 | 0.127 | 0.527 |
| MTF cut-off 5 mm | −2.189 | 0.036 * | 0.702 |
| Visual Variable | Z Statistic | p-Value | Cohen’s d |
| Mon VDI | 0.701 | 0.497 | 0.232 |
| Bin VDI | 0.838 | 0.407 | 0.278 |
| Pupil size | 1.472 | 0.177 | 0.457 |
| OSI | 1.418 | 0.158 | 0.568 |
| Near stereoacuity | 1.244 | 0.220 | 0.414 |
| Distance Stereoacuity | 0.901 | 0.390 | 0.294 |
| Factor and Covariates | Degrees of Freedom | ANCOVA F | p-Value | Effect Size ηp2 |
|---|---|---|---|---|
| Fixed model | 4 | 3.332 | 0.022 | 0.289 |
| BrAC | 1 | 4.535 | 0.041 | 0.124 |
| Age | 1 | 1.921 | 0.103 | 0.081 |
| BMI | 1 | 2.939 | 0.096 | 0.084 |
| Biological sex * | 1 | 4.246 | 0.290 | 0.035 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casares-López, M.; Castro-Torres, J.J.; Ortiz-Peregrina, S.; Martino, F.; Ortiz, C. Changes in Visual Performance under the Effects of Moderate–High Alcohol Consumption: The Influence of Biological Sex. Int. J. Environ. Res. Public Health 2021, 18, 6790. https://doi.org/10.3390/ijerph18136790
Casares-López M, Castro-Torres JJ, Ortiz-Peregrina S, Martino F, Ortiz C. Changes in Visual Performance under the Effects of Moderate–High Alcohol Consumption: The Influence of Biological Sex. International Journal of Environmental Research and Public Health. 2021; 18(13):6790. https://doi.org/10.3390/ijerph18136790
Chicago/Turabian StyleCasares-López, Miriam, José J. Castro-Torres, Sonia Ortiz-Peregrina, Francesco Martino, and Carolina Ortiz. 2021. "Changes in Visual Performance under the Effects of Moderate–High Alcohol Consumption: The Influence of Biological Sex" International Journal of Environmental Research and Public Health 18, no. 13: 6790. https://doi.org/10.3390/ijerph18136790
APA StyleCasares-López, M., Castro-Torres, J. J., Ortiz-Peregrina, S., Martino, F., & Ortiz, C. (2021). Changes in Visual Performance under the Effects of Moderate–High Alcohol Consumption: The Influence of Biological Sex. International Journal of Environmental Research and Public Health, 18(13), 6790. https://doi.org/10.3390/ijerph18136790