
Physical Activity among Adults Residing in 11 Countries during the COVID-19 Pandemic Lockdown

 , ,
, ,  ,
,  ,
,  ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey Instrument
2.3. Procedures
2.4. Study Variables and Measures
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
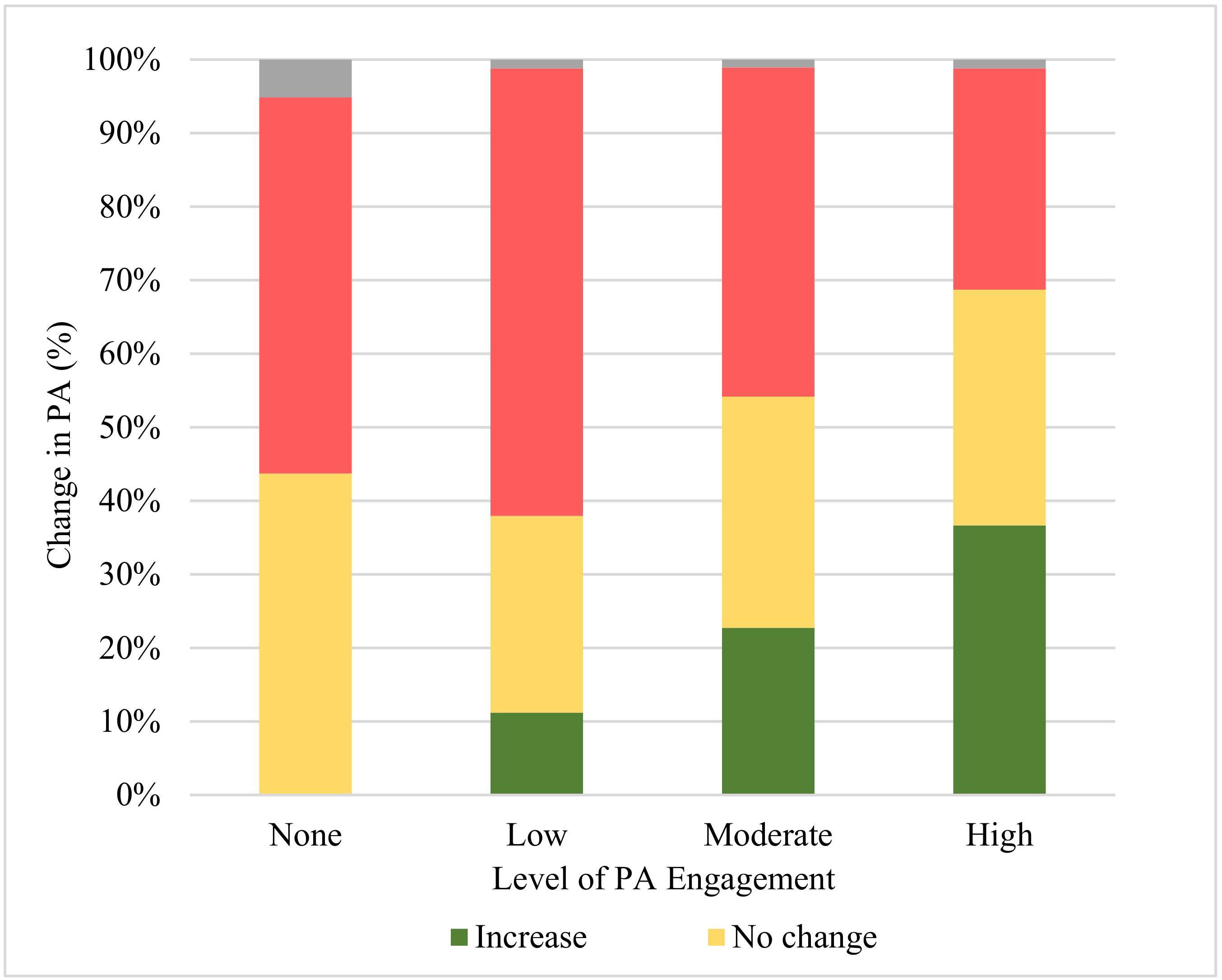
3.2. PA during Lockdown
3.3. PA during Lockdown by Country
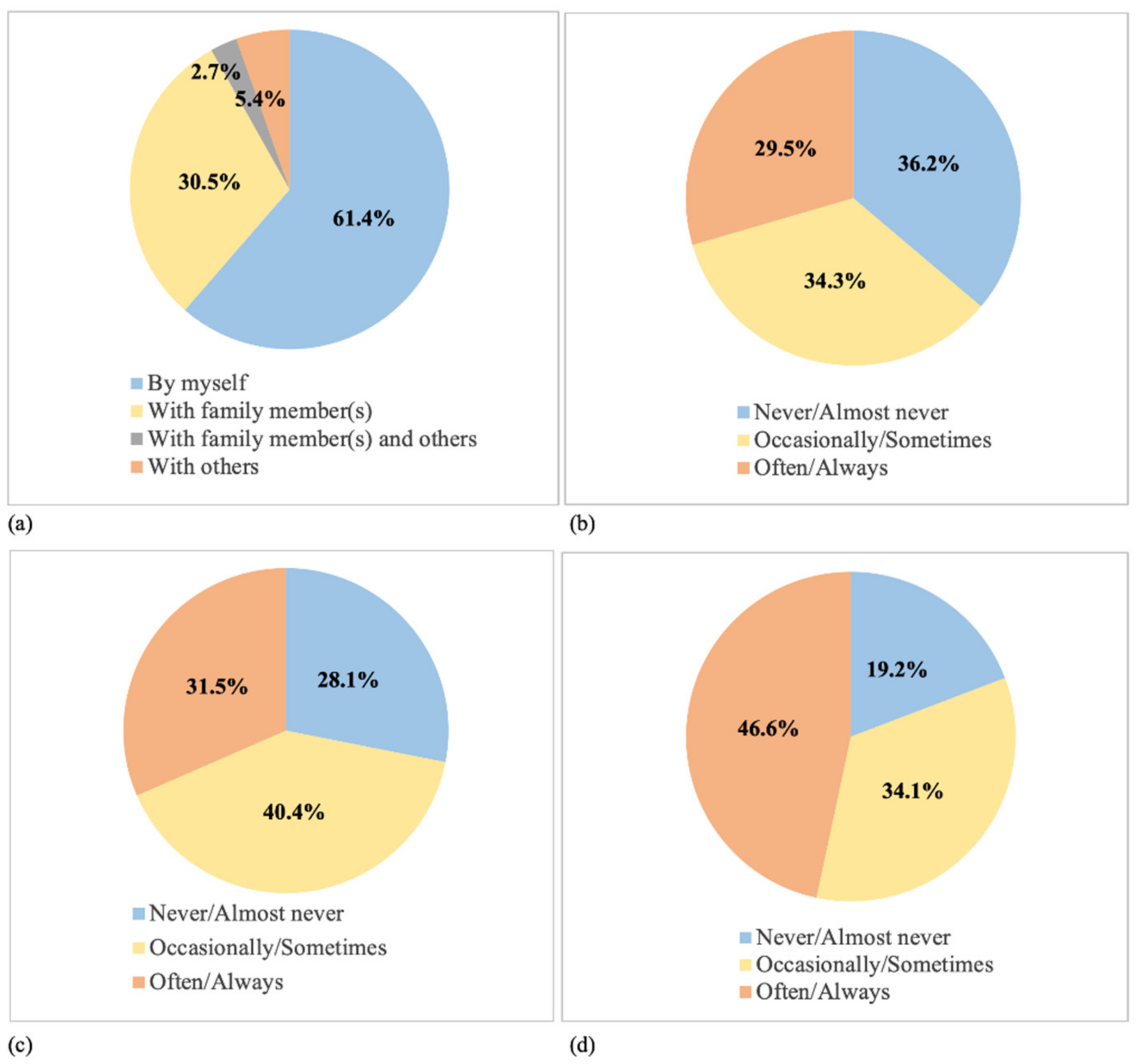
3.4. Location and Mode of PA during Lockdown
3.5. Factors Associated with PA Engagement during Lockdown
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Global Community Health-COVID-19 Collaborative Research Team
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta. BioMed. 2020, 91, 157–160. [Google Scholar]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Druckenmiller, H.; Huang, L.Y.; Hultgren, A.; Krasovich, E.; et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nat. Cell Biol. 2020, 584, 262–267. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Ahmad, A.; Mueller, C.; Tsamakis, K. COVID-19 pandemic: A public and global mental health opportunity for social transformation? BMJ 2020, 369, m1383. [Google Scholar] [CrossRef] [Green Version]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 6, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Ashdown-Franks, G.; Sabiston, C.M.; Stubbs, B. The evidence for physical activity in the management of major mental illnesses: A concise overview to inform busy clinicians’ practice and guide policy. Curr. Opin. Psychiatry 2019, 32, 375–380. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. How to Stay Physically Active during COVID-19 Self-Quarantine. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/physical-activity/news/news/2020/3/how-to-stay-physically-active-during-covid-19-self-quarantine (accessed on 25 March 2021).
- Woods, J.A.; Hutchinson, N.T.; Powers, S.K.; Roberts, W.O.; Gomez-Cabrera, M.C.; Radak, Z.; Berkes, I.; Boros, A.; Boldogh, I.; Leeuwenburgh, C.; et al. The COVID-19 pandemic and physical activity. Sports Med. Health Sci. 2020, 2, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Shariat, A.; Cleland, J.A.; Hakakzadeh, A. Home-based exercises during the COVID-19 quarantine situation for office workers: A commentary. Work 2020, 66, 381–382. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, M.Á.; Crespo, I.; Olmedillas, H. Exercising in times of COVID-19: What do experts recommend doing within four walls? Rev. Esp. Cardiol. 2020, 73, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Khoury, S.R.; Evans, N.S.; Ratchford, E.V. Exercise as medicine. Vasc. Med. 2019, 24, 371–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Regional Office for Europe of the World Health Organization. Motion for Your Mind: Physical Activity for Mental Health Promotion, Protection and Care. Available online: https://www.euro.who.int/__data/assets/pdf_file/0018/403182/WHO-Motion-for-your-mind-ENG.pdf (accessed on 25 March 2021).
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental health problems during the COVID-19 pandemics and the mitigation effects of exercise: A longitudinal study of college students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical activity change during COVID-19 confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 US adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef] [PubMed]
- Pépin, J.L.; Bruno, R.M.; Yang, R.Y.; Vercamer, V.; Jouhaud, P.; Escourrou, P.; Boutouyrie, P. Wearable Activity Trackers for Monitoring Adherence to Home Confinement during the COVID-19 Pandemic Worldwide: Data Aggregation and Analysis. J. Med. Internet Res. 2020, 22, e19787. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The impact of COVID-19 on physical activity behavior and well-being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Smith, L.; Jacob, L.; Butler, L.; Schuch, F.; Barnett, Y.; Grabovac, I.; Veronese, N.; Caperchione, C.; Lopez-Sanchez, G.F.; Meyer, J.; et al. Prevalence and correlates of physical activity in a sample of UK adults observing social distancing during the COVID-19 pandemic. BMJ Open Sport Exerc. Med. 2020, 6, e000850. [Google Scholar] [CrossRef]
- Faulkner, J.; O’Brien, W.J.; McGrane, B.; Wadsworth, D.; Batten, J.; Askew, C.D.; Badenhorst, C.; Byrd, E.; Coulter, M.; Draper, N.; et al. Physical activity, mental health and well-being of adults during initial COVID-19 containment strategies: A multi-country cross-sectional analysis. J. Sci. Med. Sport 2021, 24, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; Vancampfort, D.; Firth, J.; Stubbs, B.; Grabovac, I.; Willeit, P.; Tavares, V.D.O.; Calegaro, V.C.; et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Res. 2020, 292, 113339. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Ding, K.; Yang, J.Z.; Chin, M.K.; Sullivan, L.; Demirhan, G.; Violant-Holz, V.; Uvinha, R.R.; Dai, J.; Xu, X.; Popeksa, B.; et al. Mental health among adults during the COVID-19 pandemic lockdown: A cross-sectional multi-country comparison. Int. J. Environ. Res. Public Health 2021, 18, 2686. [Google Scholar] [CrossRef] [PubMed]
- Pilkonis, P.A.; Choi, S.W.; Reise, S.P.; Stover, A.M.; Riley, W.T.; Cella, D. PROMIS cooperative group item banks for measuring emotional distress from the Patient-Reported Outcomes Measurement Information System (PROMIS®): Depression, anxiety, and anger. Assessment 2011, 18, 263–283. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H., Jr.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S516. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sember, V.; Meh, K.; Sorić, M.; Starc, G.; Rocha, P.; Jurak, G. Validity and reliability of international physical activity questionnaires for adults across EU countries: Systematic review and meta analysis. Int. J. Environ. Res. Public Health 2020, 17, 7161. [Google Scholar] [CrossRef] [PubMed]
- The IPAQ Group. IPAQ Scoring Protocol. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 25 March 2021).
- Our World in Data. COVID-19: Stringency Index. Available online: https://ourworldindata.org/grapher/covid-stringency-index (accessed on 25 March 2021).
- The PROMIS Health Organization. Obtain & Administer Measures. Available online: https://www.healthmeasures.net/index.php?option=com_content&view=category&layout=blog&id=71&Itemid=817 (accessed on 25 March 2021).
- Anastasi, A. Psychological Testing; Macmillan Publishing Company: New York, NY, USA, 1988; pp. 122–127. [Google Scholar]
- Merlo, J.; Yang, M.; Chaix, B.; Lynch, J.; Rastam, L. A brief conceptual tutorial on multilevel analysis in social epidemiology: Investigating contextual phenomena indifferent groups of people. J. Epidemiol. Community Health 2005, 59, 729–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoramipour, K.; Basereh, A.; Hekmatikar, A.A.; Castell, L.; Ruhee, R.T.; Suzuki, K. Physical activity and nutrition guidelines to help with the fight against COVID-19. J. Sports Sci. 2021, 39, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in times of lockdown: An analysis of the impact of COVID-19 on levels and patterns of exercise among adults in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 4144. [Google Scholar] [CrossRef]
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27, taaa037. [Google Scholar] [CrossRef] [Green Version]
- Aquino, E.M.L.; Silveira, I.H.; Pescarini, J.M.; Aquino, R.; Souza-Filho, J.A.; Rocha, A.S.; Ferreira, A.; Victor, A.; Teixeira, C.; Machado, D.B.; et al. Social distancing measures to control the COVID-19 pandemic: Potential impacts and challenges in Brazil. Cienc. Saude Coletiva 2020, 25, 2423–2446. [Google Scholar] [CrossRef]
- Benham, J.L.; Lang, R.; Kovacs Burns, K.; MacKean, G.; Léveillé, T.; McCormack, B.; Sheikh, H.; Fullerton, M.M.; Tang, T.; Boucher, J.C.; et al. Attitudes, current behaviours and barriers to public health measures that reduce COVID-19 transmission: A qualitative study to inform public health messaging. PLoS ONE 2021, 16, e0246941. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biviá-Roig, G.; La Rosa, V.L.; Gómez-Tébar, M.; Serrano-Raya, L.; Amer-Cuenca, J.J.; Caruso, S.; Commodari, E.; Barrasa-Shaw, A.; Lisón, J.F. Analysis of the impact of the confinement resulting from COVID-19 on the lifestyle and psychological wellbeing of Spanish pregnant women: An internet-based cross-sectional survey. Int. J. Environ. Res. Public Health 2020, 17, 5933. [Google Scholar] [CrossRef]
- Brand, R.; Timme, S.; Nosrat, S. When pandemic hits: Exercise frequency and subjective well-being during COVID-19 pandemic. Front. Psychol. 2020, 11, 570567. [Google Scholar] [CrossRef]
- Jacob, L.; Tully, M.A.; Barnett, Y.; Lopez-Sanchez, G.F.; Butler, L.; Schuch, F.; López-Bueno, R.; McDermott, D.; Firth, J.; Grabovac, I.; et al. The relationship between physical activity and mental health in a sample of the UK public: A cross-sectional study during the implementation of COVID-19 social distancing measures. Ment. Health Phys. Act. 2020, 19, 100345. [Google Scholar] [CrossRef] [PubMed]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef]
- Khosravi, M. COVID-19 quarantine: Two-way interaction between physical activity and mental health. Eur. J. Transl. Myol. 2021, 30, 9509. [Google Scholar] [CrossRef]
- Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; Sansano-Nadal, O.; Guerra-Balic, M. Psychological health and physical activity levels during the COVID-19 pandemic: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 9419. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, G.; Rhodes, R.E.; Vanderloo, L.M.; Chulak-Bozer, T.; O’Reilly, N.; Ferguson, L.; Spence, J.C. Physical activity as a coping strategy for mental health due to the COVID-19 virus: A potential disconnect among Canadian adults? Front. Commun. 2020, 5, 74. [Google Scholar] [CrossRef]
- Marashi, M.Y.; Nicholson, E.; Ogrodnik, M.; Fenesi, B.; Heisz, J.J. A mental health paradox: Mental health was both a motivator and barrier to physical activity during the COVID-19 pandemic. PLoS ONE 2021, 16, e0239244. [Google Scholar] [CrossRef]
- Dwyer, M.J.; Pasini, M.; De Dominicis, S.; Righi, E. Physical activity: Benefits and challenges during the COVID-19 pandemic. Scand. J. Med. Sci. Sports 2020, 30, 1291–1294. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sustainable Development Goals (SDGs). Available online: https://www.who.int/health-topics/sustainable-development-goals#tab=tab_1 (accessed on 23 April 2021).
- Dhingra, M.; Chattopadhyay, S. Advancing smartness of traditional settlements-case analysis of Indian and Arab old cities. Int. J. Sustain. Built Environ. 2016, 5, 549–563. [Google Scholar] [CrossRef] [Green Version]
- Nam, T.; Pardo, T.A. Conceptualizing Smart City with Dimensions of Technology, People, and Institutions. In Proceedings of the 12th Annual International Digital Government Research Conference: Digital Government Innovation in Challenging Times, New York, NY, USA, 12 June 2011; pp. 282–291. [Google Scholar] [CrossRef]
- Cocchia, A. Smart and digital city: A systematic literature review. In Smart City; Dameri, R., Rosenthal-Sabroux, C., Eds.; Springer: Cham, Switzerland, 2014. [Google Scholar] [CrossRef]
- Lara, A.P.; Da Costa, E.M.; Furlani, T.Z.; Yigitcanla, T. Smartness that matters: Towards a comprehensive and human-centred characterisation of smart cities. J. Open Innov. Technol. Mark. Complex. 2016, 2, 8. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N (%) | |
|---|---|---|
| Country | Brazil | 1432 (12.2) |
| Bulgaria | 933 (7.9) | |
| China | 1952 (16.6) | |
| India | 848 (7.2) | |
| Ireland | 930 (7.9) | |
| Malaysia | 766 (6.5) | |
| North Macedonia | 804 (6.8) | |
| Singapore | 800 (6.8) | |
| Spain | 962 (8.2) | |
| Turkey | 1360 (11.6) | |
| United States | 988 (8.4) | |
| Sex | Female | 7498 (63.7) |
| Male | 4170 (35.4) | |
| Other | 107 (0.9) | |
| Age group | 18–24 | 3560 (30.3) |
| 25–34 | 2540 (21.6) | |
| 35–44 | 2369 (20.1) | |
| 45–54 | 1703 (14.5) | |
| 55–64 | 1111 (9.4) | |
| 65 years or older | 480 (4.1) | |
| Marital status | Married | 5179 (44.0) |
| Single | 5783 (49.1) | |
| Other | 813 (6.9) | |
| Education level | High school degree or lower | 2679 (22.8) |
| Associate degree | 1681 (14.3) | |
| Bachelor’s degree | 4281 (36.4) | |
| Graduate degree | 3111 (26.5) | |
| General health before COVID-19 | Excellent | 2927 (24.9) |
| Very Good | 5083 (43.2) | |
| Good | 3144 (26.7) | |
| Fair | 621 (5.3) | |
| Living with person(s) ≥65 years old during lockdown | Yes | 2468 (21.0) |
| No | 9307 (79.0) | |
| Having a child in the household during lockdown | Yes | 3720 (31.6) |
| No | 8055 (68.4) | |
| Required to go out of the home to work during lockdown | Full-time | 2091 (17.8) |
| Part-time | 2202 (18.7) | |
| No | 7482 (63.5) | |
| Mental health symptoms during lockdown (mean, standard deviation) | Anxiety score | 56.4 (9.7) |
| Depression score | 52.2 (9.7) |
| Insufficiently Active | Level of Physical Activity | Change in Physical Activity | Increase in Confirmed Cases a | Governmental Policy Response a | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | None | Low | Moderate | High | Increase | No Change | Decrease | |||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | Per million population | Standardized score | |
| Brazil | 834 (58.2) | 598 (41.8) | 481 (33.6) | 353 (24.7) | 270 (18.9) | 328 (22.9) | 239 (16.7) | 343 (24.0) | 800 (55.9) | 106.3 | 75.6 |
| Bulgaria | 197 (21.1) | 736 (78.9) | 83 (8.9) | 114 (12.2) | 290 (31.1) | 446 (47.8) | 75 (8.0) | 448 (48.0) | 400 (42.9) | 14.0 | 51.7 |
| China | 1064 (54.5) | 888 (45.5) | 618 (31.7) | 446 (22.9) | 405 (20.8) | 483 (24.7) | 329 (16.9) | 844 (43.2) | 779 (39.9) | 0.3 | 73.3 |
| India | 435 (51.3) | 413 (48.7) | 362 (42.7) | 73 (8.6) | 178 (21.0) | 235 (27.7) | 172 (20.3) | 265 (31.3) | 348 (41.0) | 15.7 | 82.9 |
| Ireland | 233 (25.1) | 697 (75.0) | 92 (9.9) | 141 (15.2) | 274 (29.5 | 423 (45.5) | 336 (36.1) | 238 (25.6) | 314 (33.8) | 34.2 | 67.6 |
| Malaysia | 423 (55.2) | 343 (44.8) | 265 (34.6) | 158 (20.6) | 123 (16.1) | 220 (28.7) | 129 (16.8) | 258 (33.7) | 379 (49.5) | 1.6 | 61.6 |
| North Macedonia | 240 (29.9) | 564 (70.2) | 99 (12.3) | 141 (17.5) | 163 (20.3) | 401 (49.9) | 152 (18.9) | 326 (40.6) | 324 (40.3) | 40.8 | 65.5 |
| Singapore | 342 (42.8) | 458 (57.3) | 140 (17.5) | 202 (25.3) | 188 (23.5) | 270 (33.8) | 241 (30.1) | 352 (44.0) | 207 (25.9) | 52.9 | 60.5 |
| Spain | 411 (42.7) | 551 (57.3) | 213 (22.1) | 198 (20.6) | 252 (26.2) | 299 (31.1) | 198 (20.6) | 202 (21.0) | 524 (54.5) | 54.4 | 65.3 |
| Turkey | 604 (44.4) | 756 (55.6) | 289 (21.3) | 315 (23.2) | 342 (25.2) | 414 (30.4) | 206 (15.2) | 350 (25.7) | 804 (59.1) | 19.1 | 64.2 |
| United States | 386 (39.1) | 602 (60.9) | 138 (14.0) | 248 (25.1) | 307 (31.1) | 295 (29.9) | 222 (22.5) | 328 (33.2) | 394 (39.9) | 100.1 | 66.8 |
| Overall | 5169 (43.9) † | 6606 (56.1) | 2780 (23.6) | 2389 (20.3) | 2792 (23.7) | 3814 (32.4) † | 2522 (21.4) | 3175 (27.0) | 5273 (44.8) † | 39.4 | 67.7 § |
| Factors | Insufficiently Active | Decrease in Physical Activity | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | ||
| Country-level COVID-19 risk | 10-unit change of confirmed cases | 0.97 (0.90, 1.05) | 0.98 (0.92, 1.04) |
| 5-unit change of policy response score | 1.22 (1.03, 1.45) | 1.01 (0.88, 1.15) | |
| Mental health symptoms during lockdown | 10-unit change of anxiety score | 0.98 (0.92, 1.05) | 1.18 (1.11, 1.26) |
| 10-unit change of depression score | 1.44 (1.07, 1.22) | 1.15 (1.08, 1.22) | |
| Sex a | Female | 1.30 (1.19, 1.42) | 0.92 (0.85, 1.00) |
| Male | Reference | Reference | |
| Age group | 18–24 | Reference | Reference |
| 25–34 | 1.15 (1.01, 1.30) | 1.06 (0.93, 1.20) | |
| 35–44 | 1.16 (0.99, 1.36) | 1.19 (1.03, 1.39) | |
| 45–54 | 1.09 (0.92, 1.29) | 1.24 (1.05, 1.46) | |
| 55–64 | 0.98 (0.81, 1.18) | 1.37 (1.14, 1.64) | |
| 65 years or older | 1.50 (1.18, 1.91) | 1.10 (0.87, 1.40) | |
| Marital status a | Married | 1.15 (1.02, 1.31) | 0.98 (0.87, 1.11) |
| Single | Reference | Reference | |
| Education level | High school degree or lower | Reference | Reference |
| Associate degree | 1.01 (0.88, 1.15) | 1.06 (0.93, 1.21) | |
| Bachelor’s degree | 0.79 (0.71, 0.88) | 1.20(1.08, 1.33) | |
| Graduate degree | 0.79 (0.70, 0.89) | 1.30(1.16, 1.47) | |
| General health before COVID-19 | Excellent | 0.34 (0.28, 0.41) | 1.00 (0.83, 1.20) |
| Very Good | 0.47 (0.39, 0.56) | 1.18 (0.99, 1.40) | |
| Good | 0.72 (0.59, 0.86) | 1.17 (0.97, 1.40) | |
| Fair | Reference | Reference | |
| Living with person(s) ≥65 years old during lockdown | Yes | 0.96 (0.86, 1.06) | 0.93 (0.84, 1.03) |
| No | Reference | Reference | |
| Having a child in the household during lockdown | Yes | 1.17 (1.05, 1.31) | 0.89 (0.80, 0.99) |
| No | Reference | Reference | |
| Required to go out of the home to work during lockdown | Full-time | 1.16 (1.04, 1.30) | 0.91 (0.81, 1.01) |
| Part-time | 1.03 (0.93, 1.14) | 1.00 (0.90, 1.11) | |
| No | Reference | Reference | |
| ICC (null model) b | 0.075 | 0.045 | |
| AIC (full model) b | 14,798.77 | 15,369.79 | |
| BIC (full model) b | 14,808.72 | 15,379.73 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, K.; Yang, J.; Chin, M.-K.; Sullivan, L.; Durstine, J.L.; Violant-Holz, V.; Demirhan, G.; Oliveira, N.R.C.; Popeska, B.; Kuan, G.; et al. Physical Activity among Adults Residing in 11 Countries during the COVID-19 Pandemic Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 7056. https://doi.org/10.3390/ijerph18137056
Ding K, Yang J, Chin M-K, Sullivan L, Durstine JL, Violant-Holz V, Demirhan G, Oliveira NRC, Popeska B, Kuan G, et al. Physical Activity among Adults Residing in 11 Countries during the COVID-19 Pandemic Lockdown. International Journal of Environmental Research and Public Health. 2021; 18(13):7056. https://doi.org/10.3390/ijerph18137056
Chicago/Turabian StyleDing, Kele, Jingzhen Yang, Ming-Kai Chin, Lindsay Sullivan, J. Larry Durstine, Verónica Violant-Holz, Giyasettin Demirhan, Nara R.C. Oliveira, Biljana Popeska, Garry Kuan, and et al. 2021. "Physical Activity among Adults Residing in 11 Countries during the COVID-19 Pandemic Lockdown" International Journal of Environmental Research and Public Health 18, no. 13: 7056. https://doi.org/10.3390/ijerph18137056
APA StyleDing, K., Yang, J., Chin, M. -K., Sullivan, L., Durstine, J. L., Violant-Holz, V., Demirhan, G., Oliveira, N. R. C., Popeska, B., Kuan, G., Khan, W., Dai, J., Xu, X., Mladenova, Z., Balasekaran, G., Smith, G. A., & on behalf of Global Community Health-COVID-19 Collaborative Research Team. (2021). Physical Activity among Adults Residing in 11 Countries during the COVID-19 Pandemic Lockdown. International Journal of Environmental Research and Public Health, 18(13), 7056. https://doi.org/10.3390/ijerph18137056