
Overview of Canada’s Answer to the COVID-19 Pandemic’s First Wave (January–April 2020)

Abstract
:1. Introduction
2. Case Presentation
2.1. Demographic, Economic, Geographic, Political and Climatic Characteristics of Canada
2.2. Health Care System
2.2.1. Generalities
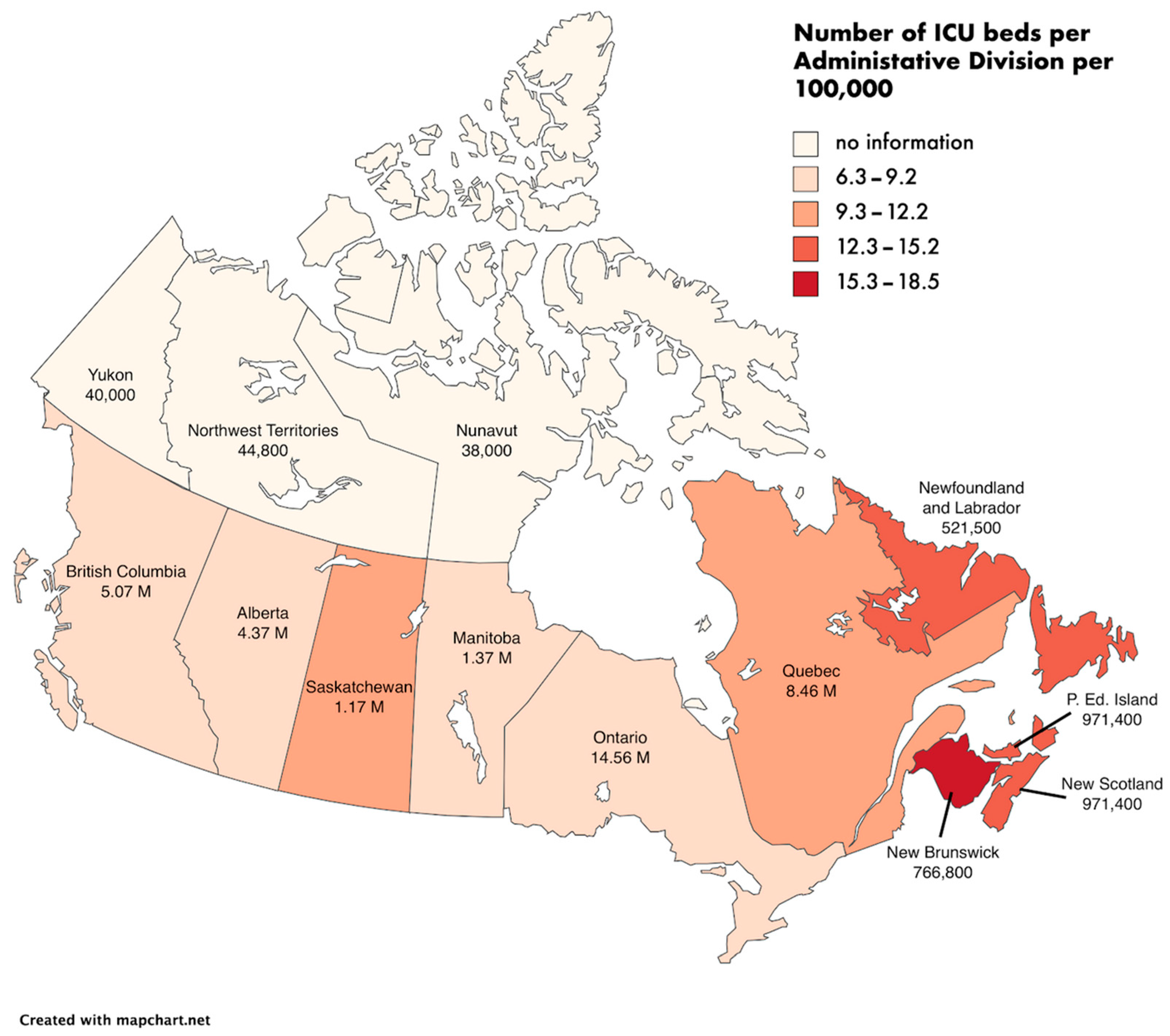
2.2.2. Health Infrastructure Capacity before COVID-19
2.2.3. Adapting the Health System to COVID-19
2.3. Epidemiological Situation of the Country Regarding COVID-19′s First Wave
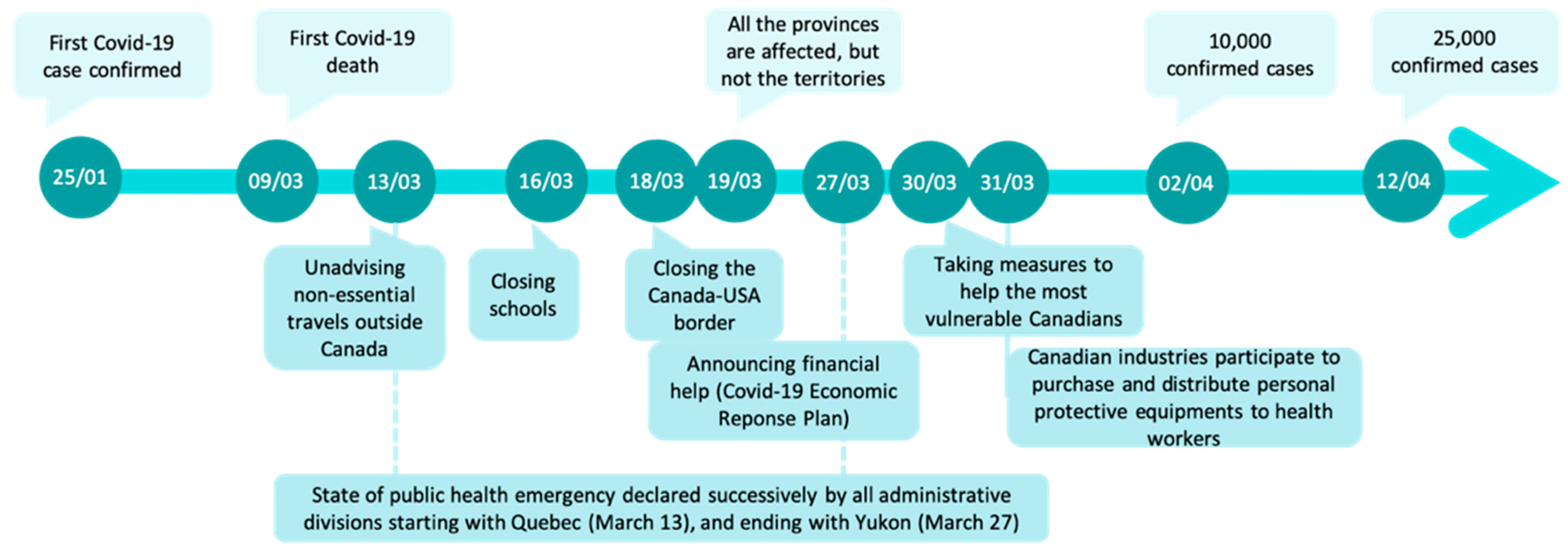
2.3.1. Epidemiological Summary (Dates)
2.3.2. Focus on the Long-Term Care Sector
2.3.3. Focus on Visible Minorities
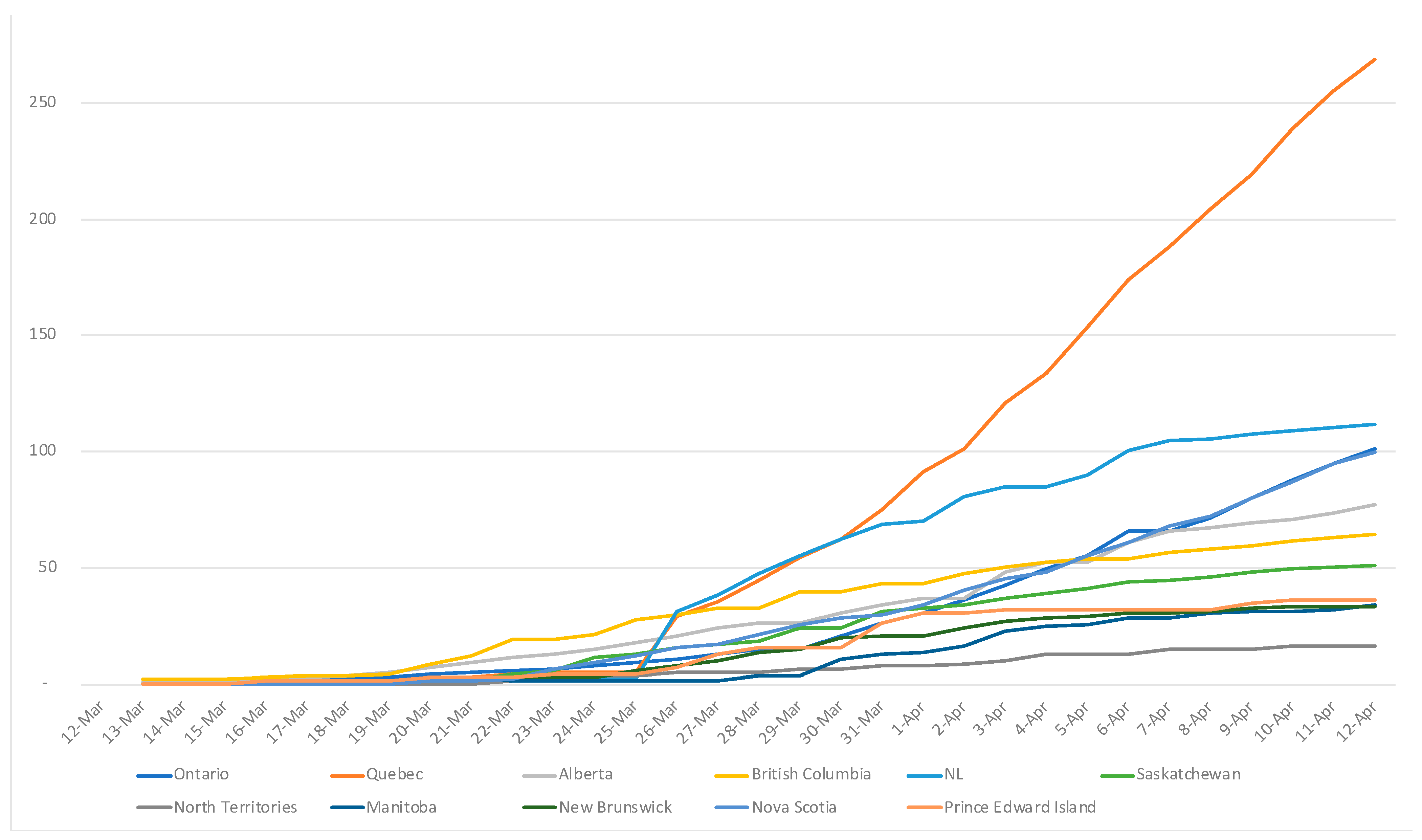
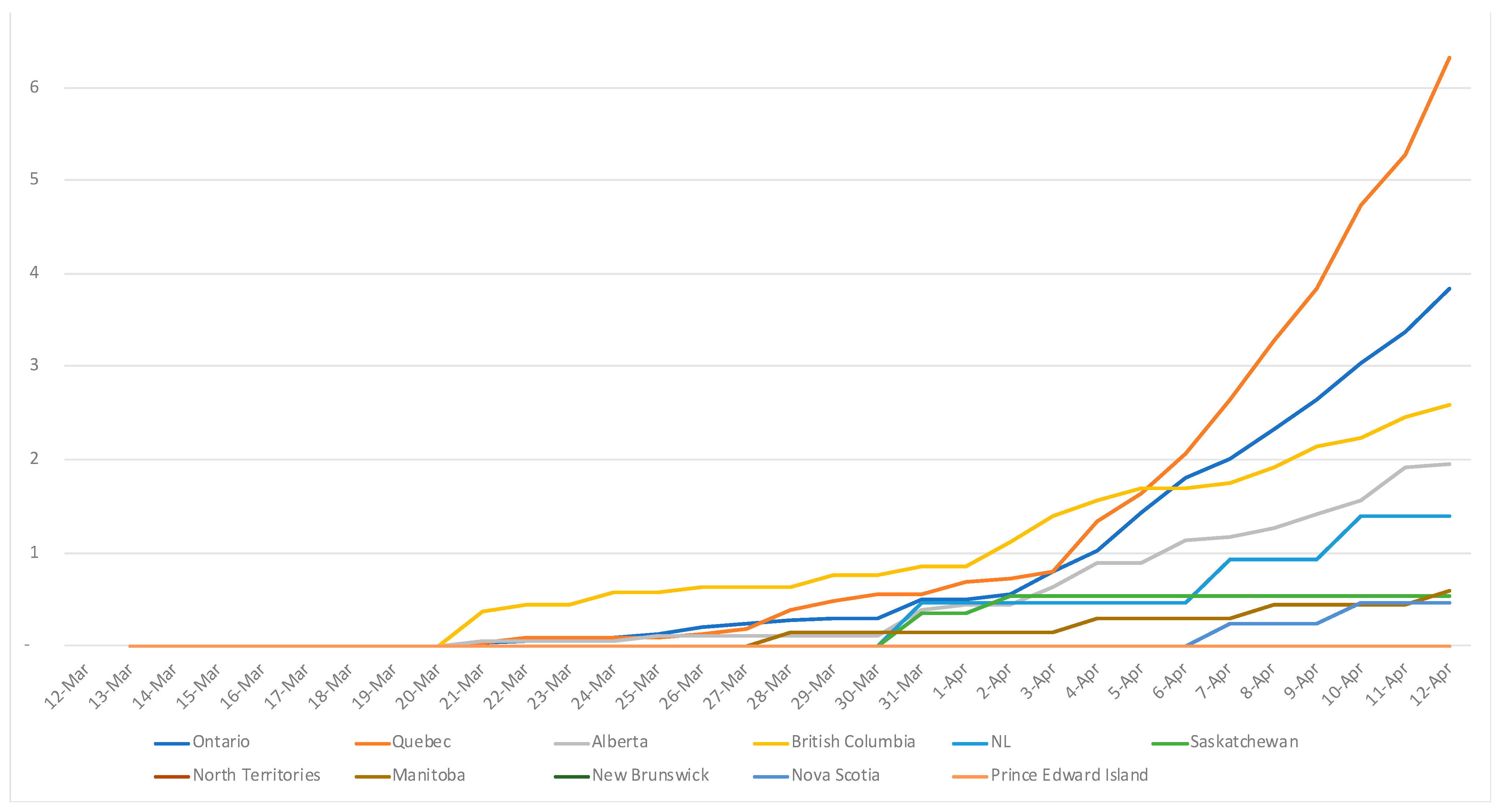
2.4. Measures Taken and Evolution of the COVID-19′s First Wave
2.4.1. At the Federal Level
2.4.2. By Administrative Division
2.5. Expected or Observed Impact on the Country Economy
2.6. Social Disruption and Indirect Public Health Consequences of COVID-19
3. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO|World Health Organization. Coronavirus. Symptoms. 2020. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_3 (accessed on 26 March 2021).
- Coronavirus Disease (COVID-19)—World Health Organization. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 21 December 2020).
- Jarvis, M.C. Aerosol Transmission of SARS-CoV-2: Physical Principles and Implications. Front. Public Health 2020, 8, 590041. [Google Scholar] [CrossRef] [PubMed]
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A Review of Viral, Host, and Environmental Factors. Ann. Intern. Med. 2021, 174, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Government of Canada, Statistics Canada. Analysis: Total Population. 27 September 2018. Available online: https://www150.statcan.gc.ca/n1/pub/91-215-x/2018001/sec1-eng.htm (accessed on 22 March 2020).
- Hindson, J. COVID-19: Faecal-Oral Transmission? Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 259. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Tao, W.; Flavell, R.A.; Zhu, S. Potential Intestinal Infection and Faecal-Oral Transmission of SARS-CoV-2. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Canada|History, Geography, & Culture|Britannica. 2020. Available online: https://www.britannica.com/place/Canada (accessed on 21 December 2020).
- Government of Canada, Health Canada. Canada’s Health Care System. Education and Awareness. 2011. Available online: https://www.canada.ca/en/health-canada/services/health-care-system/reports-publications/health-care-system/canada.html#a6 (accessed on 26 May 2020).
- Canadian Institute for Health Information, National Health Expenditure Trends|CIHI. 2021. Available online: https://www.cihi.ca/en/national-health-expenditure-trends (accessed on 17 April 2021).
- Government of Canada, Statistics Canada. The Open Database of Healthcare Facilities (ODHF) Metadata Document: Concepts, Methodology and Data Quality. 2020. Available online: https://www.statcan.gc.ca/eng/lode/databases/odhf/metadata (accessed on 17 April 2021).
- Canadian Institute for Health Information, Canada’s Health Care Providers|CIHI. 2021. Available online: https://www.cihi.ca/en/canadas-health-care-providers (accessed on 17 April 2021).
- Canadian Institute for Health Information. Long-Term Care Homes in Canada: How Many and Who Owns Them?|CIHI. 2021. Available online: https://www.cihi.ca/en/long-term-care-homes-in-canada-how-many-and-who-owns-them (accessed on 17 April 2021).
- Canadian Institute for Health Information. Care in Canadian ICUs: 36. “Canadian Institute for Health Information. Care in Canadian ICUs. Ottawa, ON: CIHI; 2016”. Available online: https://secure.cihi.ca/free_products/ICU_Report_EN.pdf (accessed on 2 March 2021).
- Shoukat, A.; Wells, C.R.; Langley, J.M.; Singer, B.H.; Galvani, A.P.; Moghadas, S.M. Projecting Demand for Critical Care Beds during COVID-19 Outbreaks in Canada. CMAJ 2020, 192, E489–E496. [Google Scholar] [CrossRef] [Green Version]
- Canadian Institute for Health Information|CIHI. 2021. Available online: https://www.cihi.ca/en (accessed on 15 March 2021).
- Fowler, R.A.; Abdelmalik, P.; Wood, G.; Foster, D.; Gibney, N.; Bandrauk, N.; Turgeon, A.F.; Lamontagne, F.; Kumar, A.; Zarychanski, R.; et al. Critical Care Capacity in Canada: Results of a National Cross-Sectional Study. Crit. Care 2015, 19, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Critical Care Society and Association of Medical Microbiology and Infectious Disease (AMMI) Canada. Clinical Management of Patients with Moderate to Severe COVID-19-Interim Guidance. 2 April 2020. Available online: https://www.ammi.ca/Content/Clinical%20Care%20COVID-19%20Guidance%20FINAL%20April2%20ENGLISH%281%29.pdf (accessed on 15 March 2021).
- The Critical Care Education Pandemic Preparedness (CCEPP) Team. Quick ICU Training. 2020. Available online: https://www.quickicutraining.com/ (accessed on 26 December 2020).
- Wiseman, S.M.; Crump, R.T.; Sutherland, J.M. Surgical Wait List Management in Canada during a Pandemic: Many Challenges Ahead. Can. J. Surg. 2020, 63, E226–E228. [Google Scholar] [CrossRef]
- British Columbia Ministry of Health. A Commitment to Surgical Renewal in B.C. 2020. Available online: https://www2.gov.bc.ca/assets/gov/health/conducting-health-research/surgical-renewal-plan.pdf (accessed on 2 March 2021).
- Worried You Might Have COVID-19? Try the Government’s New Online Self-Assessment|CTVNews. 2020. Available online: https://www.ctvnews.ca/health/coronavirus/worried-you-might-have-covid-19-try-the-government-s-new-online-self-assessment-1.4863421 (accessed on 22 March 2020).
- Health Canada Approves New Rapid COVID-Testing Kits|The Globe And Mail. 2021. Available online: https://www.theglobeandmail.com/canada/article-health-canada-approves-new-rapid-covid-testing-kits/ (accessed on 2 January 2021).
- WHO|World Health Organization. WHO|Cumulative Number of Reported Probable Cases of SARS. 2021. Available online: https://www.who.int/csr/sars/country/2003_07_11/en/ (accessed on 15 March 2021).
- Silverman, M.; Clarke, M.; Stranges, S. Did Lessons From SARS Help Canada’s Response to COVID-19? Am. J. Public Health 2020, 110, 1797–1799. [Google Scholar] [CrossRef] [PubMed]
- Webster, P. Canada and COVID-19: Learning from SARS. Lancet 2020, 395, 936–937. [Google Scholar] [CrossRef]
- Yu, A.; Prasad, S.; Akande, A.; Murariu, A.; Yuan, S.; Kathirkamanathan, S.; Ma, M.; Ladha, S. COVID-19 in Canada: A Self-Assessment and Review of Preparedness and Response. J. Glob. Health 2020, 10, 0203104. [Google Scholar] [CrossRef]
- COVID-19 in Canada: This Is How Each Province Is Handling the Pandemic|CTVNews. 2020. Available online: https://www.ctvnews.ca/politics/covid-19-in-canada-this-is-how-each-province-is-handling-the-pandemic-1.4867626 (accessed on 25 March 2020).
- COVID-19 Data Explorer. Our World in Data. 2021. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=earliest..85&pickerSort=asc&pickerMetric=location&Metric=Confirmed+deaths&Interval=Cumulative&Relative+to+Population=true&Align+outbreaks=false&country=USA~CAN~European+Union (accessed on 17 April 2021).
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M. Coronavirus Pandemic (COVID-19). Our World in Data. 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 29 April 2021).
- Hsu, A.T.; Lane, N. Report: Impact of COVID-19 on Residents of Canada’s Long-Term Care Homes—Ongoing Challenges and Policy Response. Article in LTCcovid.org, International Long-Term Care Policy Network, CPEC-LSE. 2020. Available online: https://ltccovid.org/2020/04/15/impact-of-covid-19-on-residents-of-canadas-long-term-care-homes-ongoing-challenges-and-policy-response/ (accessed on 2 March 2021).
- Estabrooks, C.A.; Straus, S.; Flood, C.M.; Keefe, J.; Armstrong, P.; Donner, G.; Boscart, V.; Ducharme, F.; Silvius, J.; Wolfson, M. Rétablir la Confiance: La COVID-19 et L’avenir des Soins de Longue Durée. Société Royale du Canada. 2020. Available online: https://rsc-src.ca/sites/default/files/LTC%20PB_FR.pdf (accessed on 2 March 2021).
- Béland, D.; Marier, P. COVID-19 and Long-Term Care Policy for Older People in Canada. J. Aging Soc. Policy 2020, 32, 358–364. [Google Scholar] [CrossRef]
- Government of Canada, Statistics Canada. COVID-19 Mortality Rates in Canada’s Ethno-Cultural Neighbourhoods. 28 October 2020. Available online: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00079-eng.htm (accessed on 2 March 2021).
- Ramraj, C.; Shahidi, F.V.; Darity, W.; Kawachi, I.; Zuberi, D.; Siddiqi, A. Equally Inequitable? A Cross-National Comparative Study of Racial Health Inequalities in the United States and Canada. Soc. Sci. Med. 2016, 161, 19–26. [Google Scholar] [CrossRef]
- Dmytriw, A.A.; Phan, K.; Schirmer, C.; Settecase, F.; Heran, M.K.S.; Efendizade, A.; Kühn, A.L.; Puri, A.S.; Menon, B.K.; Dibas, M.; et al. Ischaemic Stroke Associated with COVID-19 and Racial Outcome Disparity in North America. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1362–1364. [Google Scholar] [CrossRef]
- Government of Canada; Indigenous Services Canada. Epidemiological Summary of COVID-19 Cases in First Nations Communities; Report; 2020. Available online: https://www.sac-isc.gc.ca/eng/1589895506010/1589895527965 (accessed on 2 March 2021).
- 1st COVID-19 Death Involving First Nations Person in Manitoba Reported|CBC News. 2020. Available online: https://www.cbc.ca/news/canada/manitoba/indigenous-death-covid-19-manitoba-1.5765361 (accessed on 30 December 2020).
- Richardson, L.; Crawford, A. COVID-19 and the Decolonization of Indigenous Public Health. CMAJ 2020, 192, E1098–E1100. [Google Scholar] [CrossRef]
- The Road to Canada’s COVID-19 Outbreak: Timeline of Federal Government Failure at Border to Slow the Virus. Available online: https://edmontonjournal.com/news/national/the-road-to-canadas-covid-19-outbreak-timeline-of-federal-government-failure-at-border-to-slow-the-virus (accessed on 2 January 2021).
- Pan-Canadian Public Health Network. Special Advisory Committee on COVID-19. 2020. Available online: http://www.phn-rsp.ca/sac-covid-ccs/index-eng.php (accessed on 14 May 2021).
- Government of Canada. Government of Canada Takes Action on COVID-19. Education and Awareness. 2020. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/canadas-reponse/government-canada-takes-action-covid-19.html (accessed on 22 December 2020).
- Public Health Agency of Canada. Council of Chief Medical Officers of Health Communication: Use of Non-Medical Masks (or Facial Coverings) by the Public. Statements. 2020. Available online: https://www.canada.ca/en/public-health/news/2020/04/ccmoh-communication-use-of-non-medical-masks-or-facial-coverings-by-the-public.html (accessed on 6 April 2021).
- Bhatia, D.; Vaga, K.; Roerig, M.; Pawa, J.; Allin, S.; Marchildon, G. COVID-19 Case and Contact Management Strategies in Canada. Toronto: North American Observatory on Health Systems and Policies. Rapid Review (No. 27). 2020. Available online: https://ihpme.utoronto.ca/wp-content/uploads/2020/11/NAO-Rapid-Review-27_EN.pdf (accessed on 27 April 2021).
- Public Health Agency of Canada. Federal/Provincial/Territorial Public Health Response Plan for Ongoing Management of COVID-19. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/federal-provincial-territorial-public-health-response-plan-ongoing-management-covid-19.html (accessed on 9 June 2021).
- Canada, U.S. Border Temporarily Closing to Non-Essential Traffic to Slow COVID-19|CBC News. 2020. Available online: https://www.cbc.ca/news/politics/canada-us-border-deal-1.5501289 (accessed on 18 March 2020).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Best, L.A.; Law, M.A.; Roach, S.; Wilbiks, J.M.P. The Psychological Impact of COVID-19 in Canada: Effects of Social Isolation during the Initial Response. Can. Psychol. Psychol. Can. 2021, 62, 143–154. [Google Scholar] [CrossRef]
- Government of Canada, Statistics Canada. 2020. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/200527/dq200527b-eng.htm (accessed on 15 March 2021).
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Bartel, S.J.; Sherry, S.B.; Stewart, S.H. Self-Isolation: A Significant Contributor to Cannabis Use during the COVID-19 Pandemic. Subst. Abus. 2020, 41, 409–412. [Google Scholar] [CrossRef]
- Jang, H.; Rempel, E.; Roth, D.; Carenini, G.; Janjua, N.Z. Tracking COVID-19 Discourse on Twitter in North America: Infodemiology Study Using Topic Modeling and Aspect-Based Sentiment Analysis. J. Med. Internet Res. 2021, 23, e25431. [Google Scholar] [CrossRef] [PubMed]
- These Asian Canadians are Concerned as Hate Crimes Spike in the Coronavirus Pandemic—National|Globalnews.ca. 2021. Available online: https://globalnews.ca/news/6858850/these-asian-canadians-are-concerned-as-hate-crimes-spike-in-the-coronavirus-pandemic/ (accessed on 15 March 2021).
- Pearce, N.; Lawlor, D.A.; Brickley, E.B. Comparisons between Countries Are Essential for the Control of COVID-19. Int. J. Epidemiol. 2020, 49, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, T.R.; Jones, K.E.; Dobson, A.P.; Clennon, J.A.; Pascual, M. COVID-Clarity Demands Unification of Health and Environmental Policy. Glob. Chang. Biol. 2021, 27, 1319–1321. [Google Scholar] [CrossRef]
- Canadian Public Health Association. Review of Canada’s Initial Response to the COVID-19 Pandemic. 2021. Available online: https://www.cpha.ca/review-canadas-initial-response-covid-19-pandemic (accessed on 18 May 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Provinces/Territories | Emergency State | Precisions |
|---|---|---|
| Alberta | State of public health emergency March 17 | Gatherings of no more than 50 first and then only 15; closure of public area and popular facilities (gym, museums, arenas, galleries), self-isolation for 14 days after an international travel and 10 days for people with symptoms. |
| British Columbia | State of emergency March 18—This state of emergency will be extended or rescinded as necessary. | Gatherings of no more than 50; financial penalties for business and individuals; financial penalties for businesses and individuals violating public health directives (Vancouver) |
| Manitoba | State of emergency March 20—30 days and could be extended if necessary. | Gatherings to maximum 10 |
| New Brunswick | State of emergency March 19—until April 15 and could be extended if necessary. | Gatherings of no more than 10; closure of all retail operations, except for essential services (Public inquiries, Veterinary Field and Laboratory Services, Motor Vehicle Safety Enforcement…); financial penalties |
| Newfoundland and Labrador | Public health emergency March 18—until April 15 and could be extended if necessary. | Gatherings of no more than 10; no-essential businesses closure; fine or jail time |
| Nova Scotia | State of emergency March 22—until April 19 and could be extended if necessary. | Gatherings of no more than 5; Some non-essential services remain open with social distancing |
| Ontario | State of emergency March 17- until April 14 and extended for 28 days. | Gatherings of no more than 5; closure of public facilities and non-essential businesses |
| Prince Edward Island | State of public health emergency March 16—30 days and could be extended if necessary. | Encourage islanders to avoid social gatherings; fines up to CAD10,000 |
| Quebec | Public health emergency, March 13—until May 4. | Social gatherings are prohibited; fines |
| Saskatchewan | State of emergency March 18—until April 15 and could be extended if necessary. | Gatherings of no more than 10; closure of non-essential shops; individual fines |
| Northwest Territories | State of public health emergency March 18—until April 15 and could be extended if necessary. | Gatherings of no more than 10 |
| Nunavut | State of public health emergency March 18—until April 16 and could be extended if necessary. | Public gatherings prohibited |
| Yukon | State of emergency March 27—until April 30 and could be extended if necessary. | Gatherings of no more than 10; Reduce restaurant capacity to 50% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urrutia, D.; Manetti, E.; Williamson, M.; Lequy, E. Overview of Canada’s Answer to the COVID-19 Pandemic’s First Wave (January–April 2020). Int. J. Environ. Res. Public Health 2021, 18, 7131. https://doi.org/10.3390/ijerph18137131
Urrutia D, Manetti E, Williamson M, Lequy E. Overview of Canada’s Answer to the COVID-19 Pandemic’s First Wave (January–April 2020). International Journal of Environmental Research and Public Health. 2021; 18(13):7131. https://doi.org/10.3390/ijerph18137131
Chicago/Turabian StyleUrrutia, Deborah, Elisa Manetti, Megan Williamson, and Emeline Lequy. 2021. "Overview of Canada’s Answer to the COVID-19 Pandemic’s First Wave (January–April 2020)" International Journal of Environmental Research and Public Health 18, no. 13: 7131. https://doi.org/10.3390/ijerph18137131
APA StyleUrrutia, D., Manetti, E., Williamson, M., & Lequy, E. (2021). Overview of Canada’s Answer to the COVID-19 Pandemic’s First Wave (January–April 2020). International Journal of Environmental Research and Public Health, 18(13), 7131. https://doi.org/10.3390/ijerph18137131