
Management of Amelogenesis Imperfecta in Childhood: Two Case Reports

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Reports
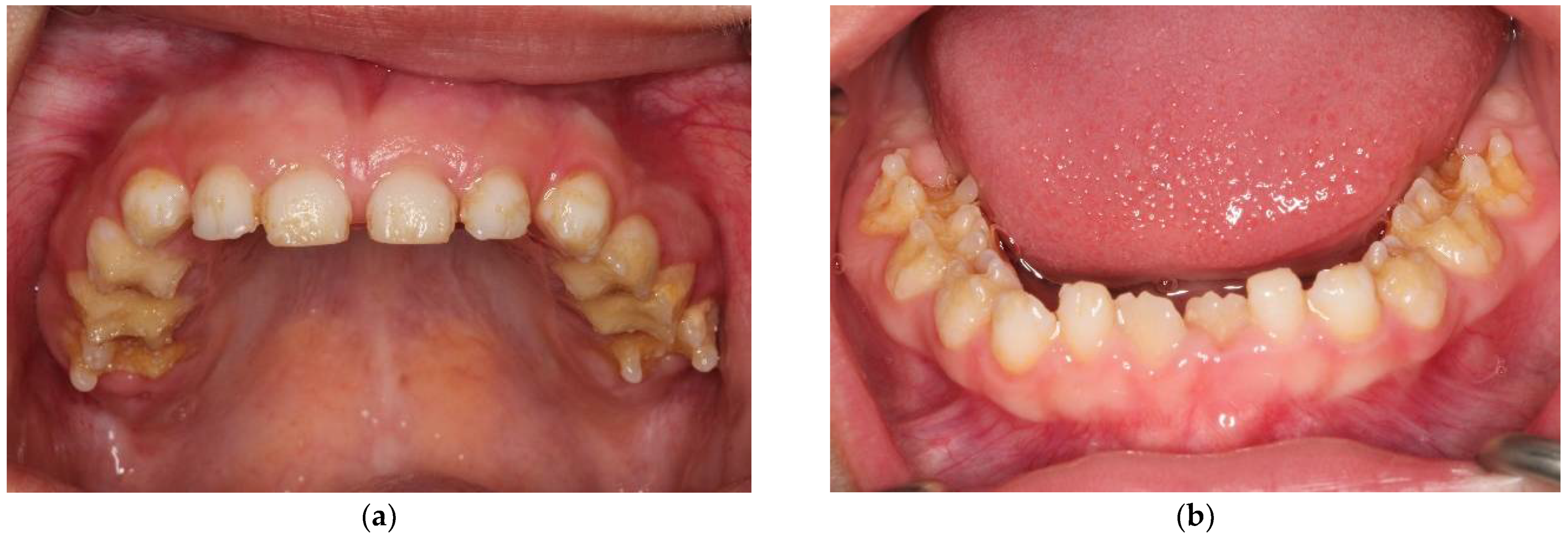
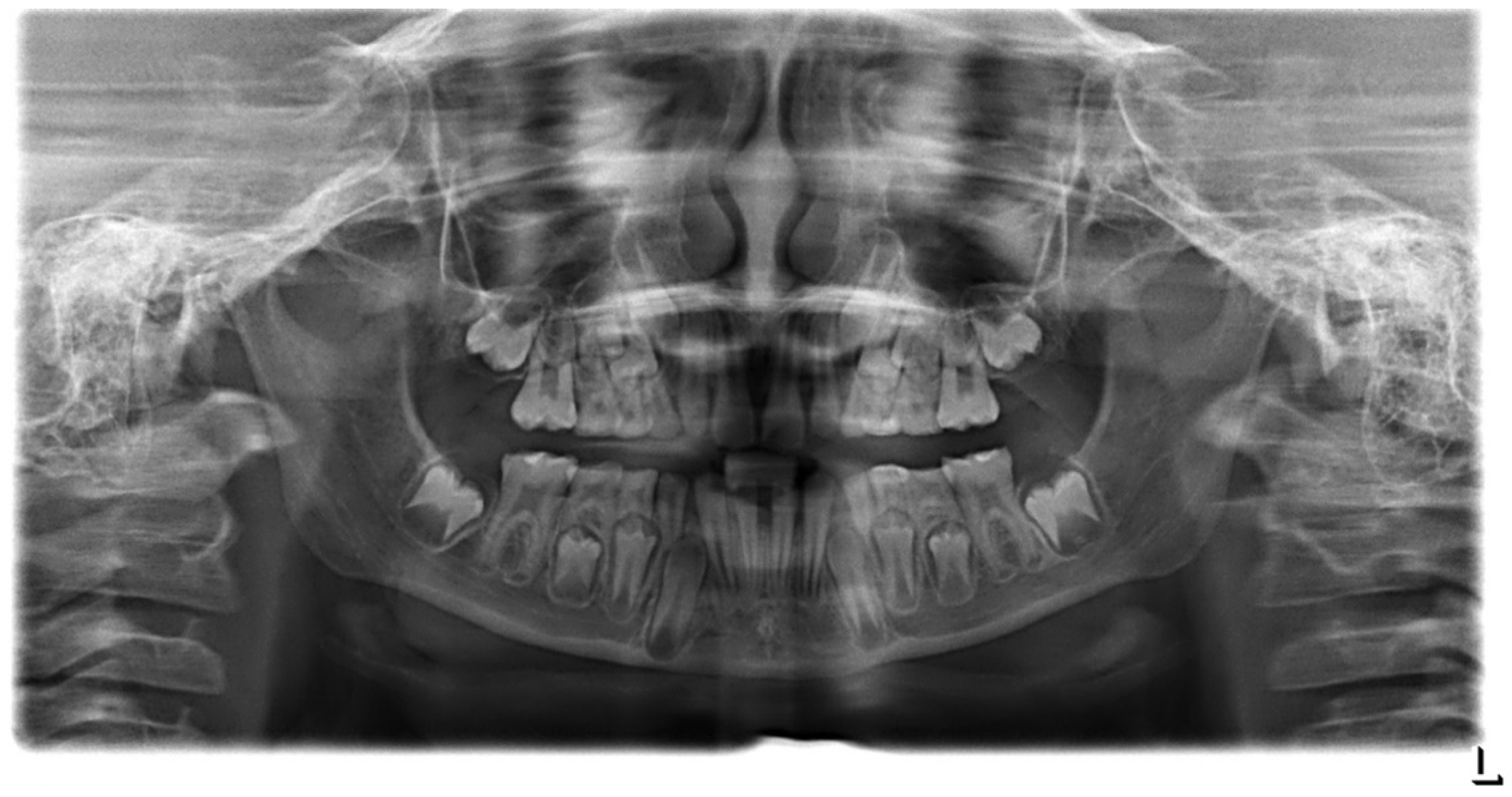
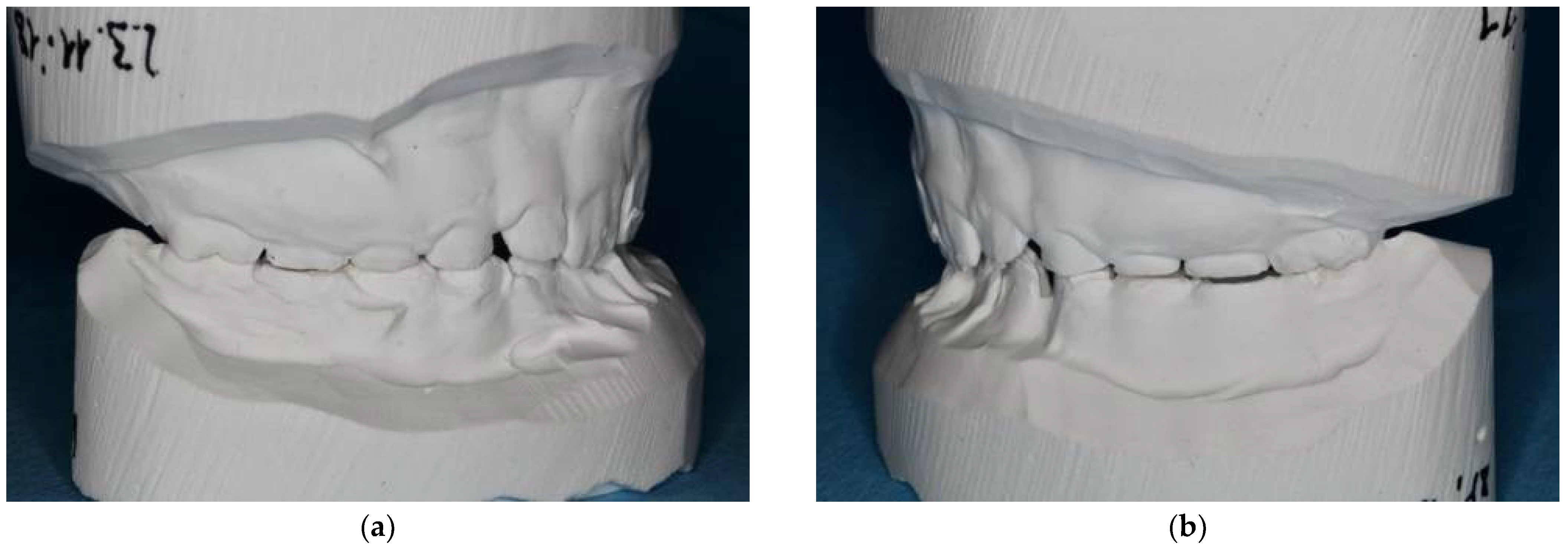
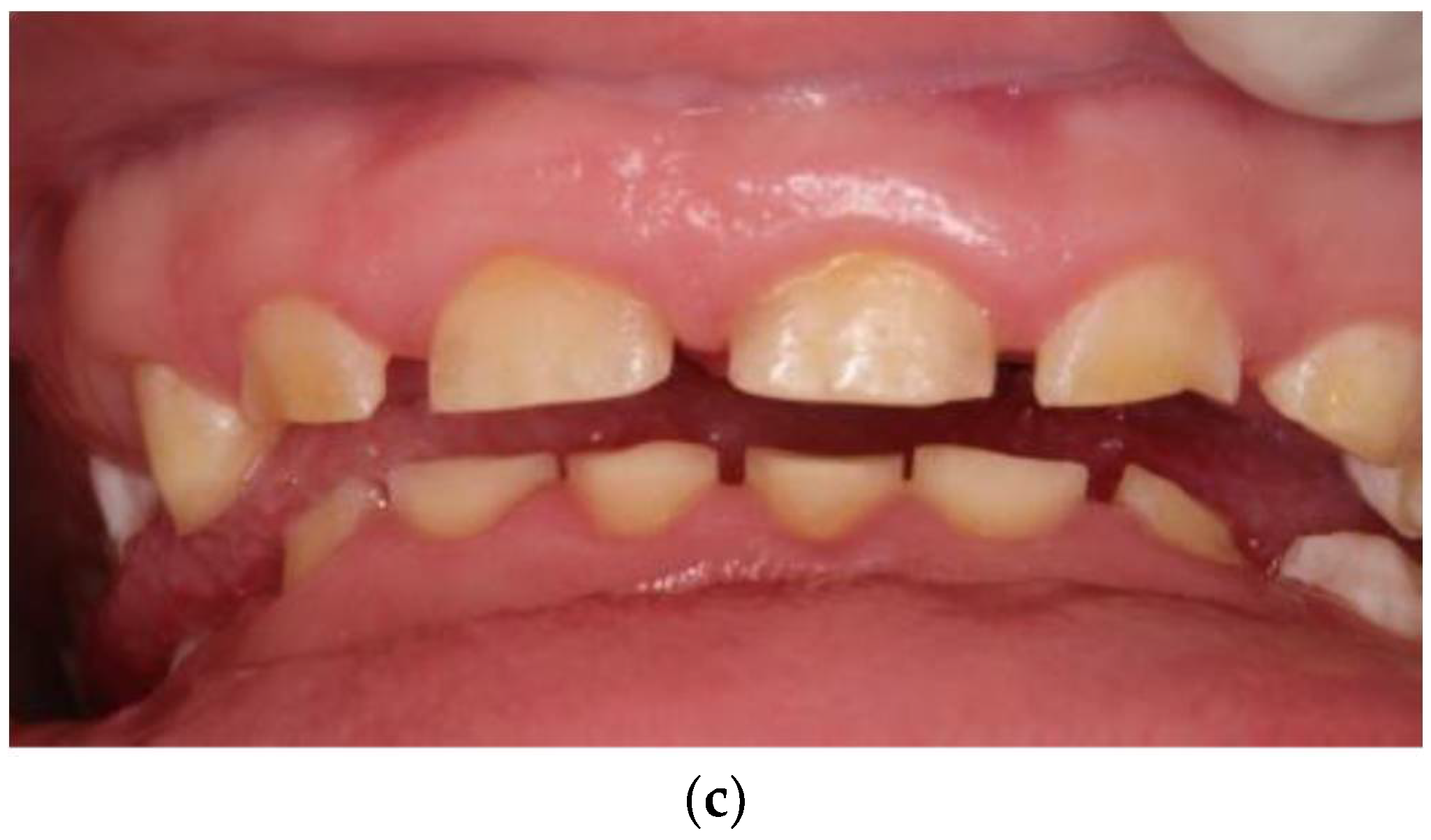
2.1. Case Report 1: Mixed Dentition
2.2. Case Report: Permanent Dentition
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gadhia, K.; McDonald, S.; Arkutu, N.; Malik, K. Amelogenesis imperfecta: An introduction. Br. Dent. J. 2012, 212, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Witkop, C.J., Jr. Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: Problems in classification. J. Oral Pathol. 1988, 17, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Toupenay, S.; Fournier, B.P.; Maniere, M.C.; Ifi-Naulin, C.; Berdal, A.; de La Dure-Molla, M. Amelogenesis imperfecta: Therapeutic strategy from primary to permanent dentition across case reports. BMC Oral Health 2018, 18, 108. [Google Scholar] [CrossRef] [PubMed]
- Crawford, P.J.; Aldred, M.; Bloch-Zupan, A. Amelogenesis imperfecta. Orphanet J. Rare Dis. 2007, 2, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohrvik, H.G.; Hjortsjo, C. Retrospective study of patients with amelogenesis imperfecta treated with different bonded restoration techniques. Clin. Exp. Dent. Res. 2020, 6, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quandalle, C.; Boillot, A.; Fournier, B.; Garrec, P.; De La Dure-Molla, M.; Kerner, S. Gingival inflammation, enamel defects, and tooth sensitivity in children with amelogenesis imperfecta: A case-control study. J. Appl. Oral Sci. 2020, 28, e20200170. [Google Scholar] [CrossRef] [PubMed]
- Ayers, K.M.; Drummond, B.K.; Harding, W.J.; Salis, S.G.; Liston, P.N. Amelogenesis imperfecta--multidisciplinary management from eruption to adulthood. Review and case report. N. Z. Dent. J. 2004, 100, 101–104. [Google Scholar] [PubMed]
- American Academy on Pediatric Dentistry Council on Clinical Affairs. Guideline on oral heath care/dental management of heritable dental development anomalies. Pediatr. Dent. 2008, 30, 196–201. [Google Scholar]
- Visram, S.; McKaig, S. Amelogenesis imperfecta—Clinical presentation and management: A case report. Dent. Update 2006, 33, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Robinson, F.G.; Haubenreich, J.E. Oral rehabilitation of a young adult with hypoplastic amelogenesis imperfecta: A clinical report. J. Prosthet. Dent. 2006, 95, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Chisini, L.A.; Collares, K.; Cademartori, M.G.; de Oliveira, L.J.C.; Conde, M.C.M.; Demarco, F.F.; Correa, M.B. Restorations in primary teeth: A systematic review on survival and reasons for failures. Int. J. Paediatr. Dent. 2018, 28, 123–139. [Google Scholar] [CrossRef] [PubMed]
- Pires, C.W.; Pedrotti, D.; Lenzi, T.L.; Soares, F.Z.M.; Ziegelmann, P.K.; Rocha, R.O. Is there a best conventional material for restoring posterior primary teeth? A network meta-analysis. Braz. Oral Res. 2018, 32, e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerli, B.; Strub, M.; Jeger, F.; Stadler, O.; Lussi, A. Composite materials: Composition, properties and clinical applications. A literature review. Schweiz Mon. Zahnmed 2010, 120, 972–986. [Google Scholar]
- Full, C.A.; Walker, J.D.; Pinkham, J.R. Stainless steel crowns for deciduous molars. J. Am. Dent. Assoc. 1974, 89, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Bae, I.H.; Noh, T.H.; Ju, S.W.; Lee, T.K.; Ahn, J.S.; Jeong, T.S.; Huh, J.B. Wear of primary teeth caused by opposed all-ceramic or stainless steel crowns. J. Adv. Prosthodont. 2016, 8, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foucher, F.; Mainjot, A.K. Polymer-Infiltrated-Ceramic-Network, CAD/CAM Restorations for Oral Rehabilitation of Pediatric Patients with X-Linked Ectodermal Dysplasia. Int. J. Prosthodont. 2018, 31, 610–612. [Google Scholar] [CrossRef] [PubMed]
- Sabandal, M.M.; Schafer, E. Amelogenesis imperfecta: Review of diagnostic findings and treatment concepts. Odontology 2016, 104, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Kramer, N.; Bui Khac, N.N.; Lucker, S.; Stachniss, V.; Frankenberger, R. Bonding strategies for MIH-affected enamel and dentin. Dent. Mater. 2018, 34, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef] [PubMed]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Möhn, M.; Bulski, J.C.; Krämer, N.; Rahman, A.; Schulz-Weidner, N. Management of Amelogenesis Imperfecta in Childhood: Two Case Reports. Int. J. Environ. Res. Public Health 2021, 18, 7204. https://doi.org/10.3390/ijerph18137204
Möhn M, Bulski JC, Krämer N, Rahman A, Schulz-Weidner N. Management of Amelogenesis Imperfecta in Childhood: Two Case Reports. International Journal of Environmental Research and Public Health. 2021; 18(13):7204. https://doi.org/10.3390/ijerph18137204
Chicago/Turabian StyleMöhn, Mirja, Julia Camilla Bulski, Norbert Krämer, Alexander Rahman, and Nelly Schulz-Weidner. 2021. "Management of Amelogenesis Imperfecta in Childhood: Two Case Reports" International Journal of Environmental Research and Public Health 18, no. 13: 7204. https://doi.org/10.3390/ijerph18137204
APA StyleMöhn, M., Bulski, J. C., Krämer, N., Rahman, A., & Schulz-Weidner, N. (2021). Management of Amelogenesis Imperfecta in Childhood: Two Case Reports. International Journal of Environmental Research and Public Health, 18(13), 7204. https://doi.org/10.3390/ijerph18137204