
Lean Healthcare Tools for Processes Evaluation: An Integrative Review

 ,
,  and
and
Abstract
:1. Introduction
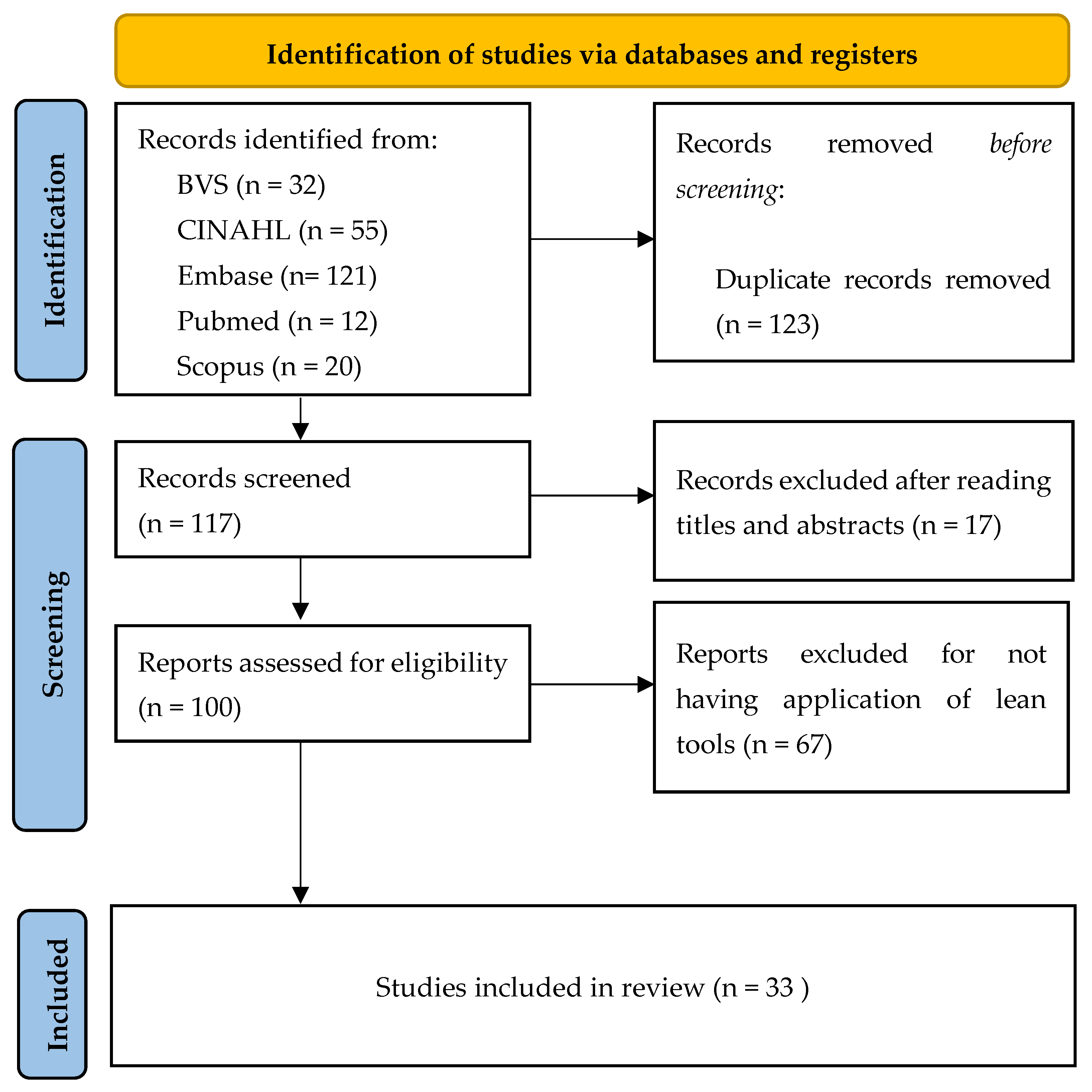
2. Materials and Methods

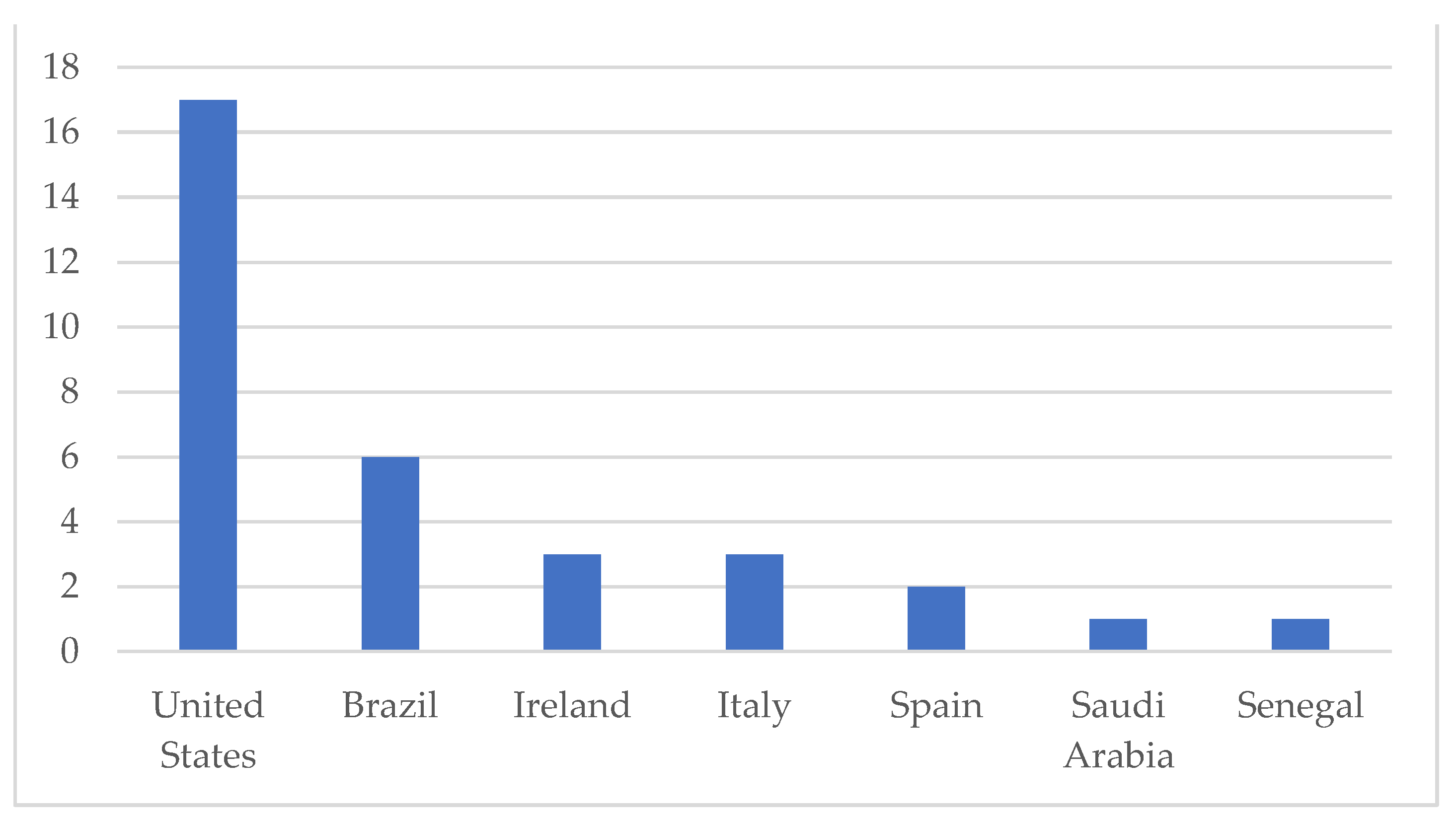
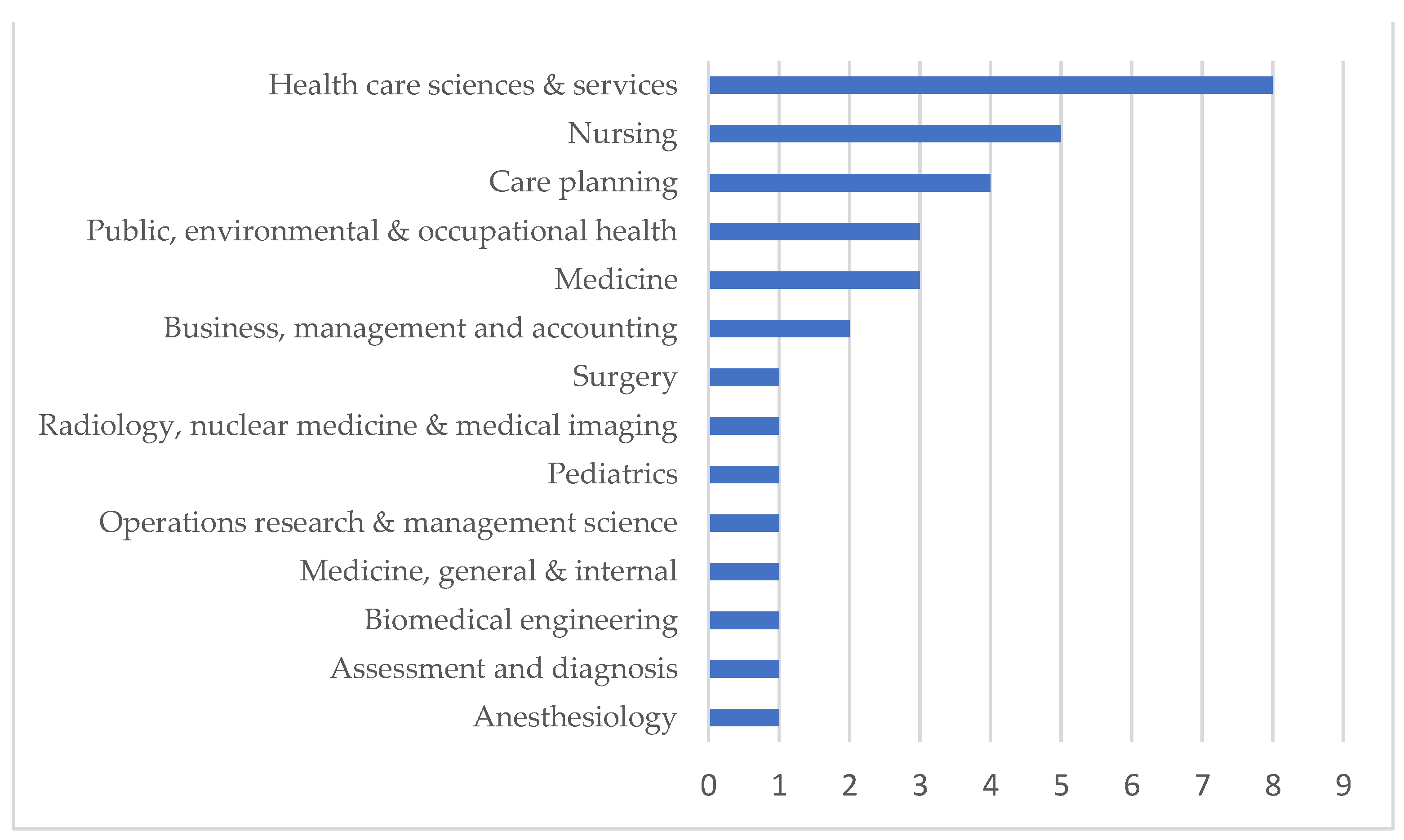
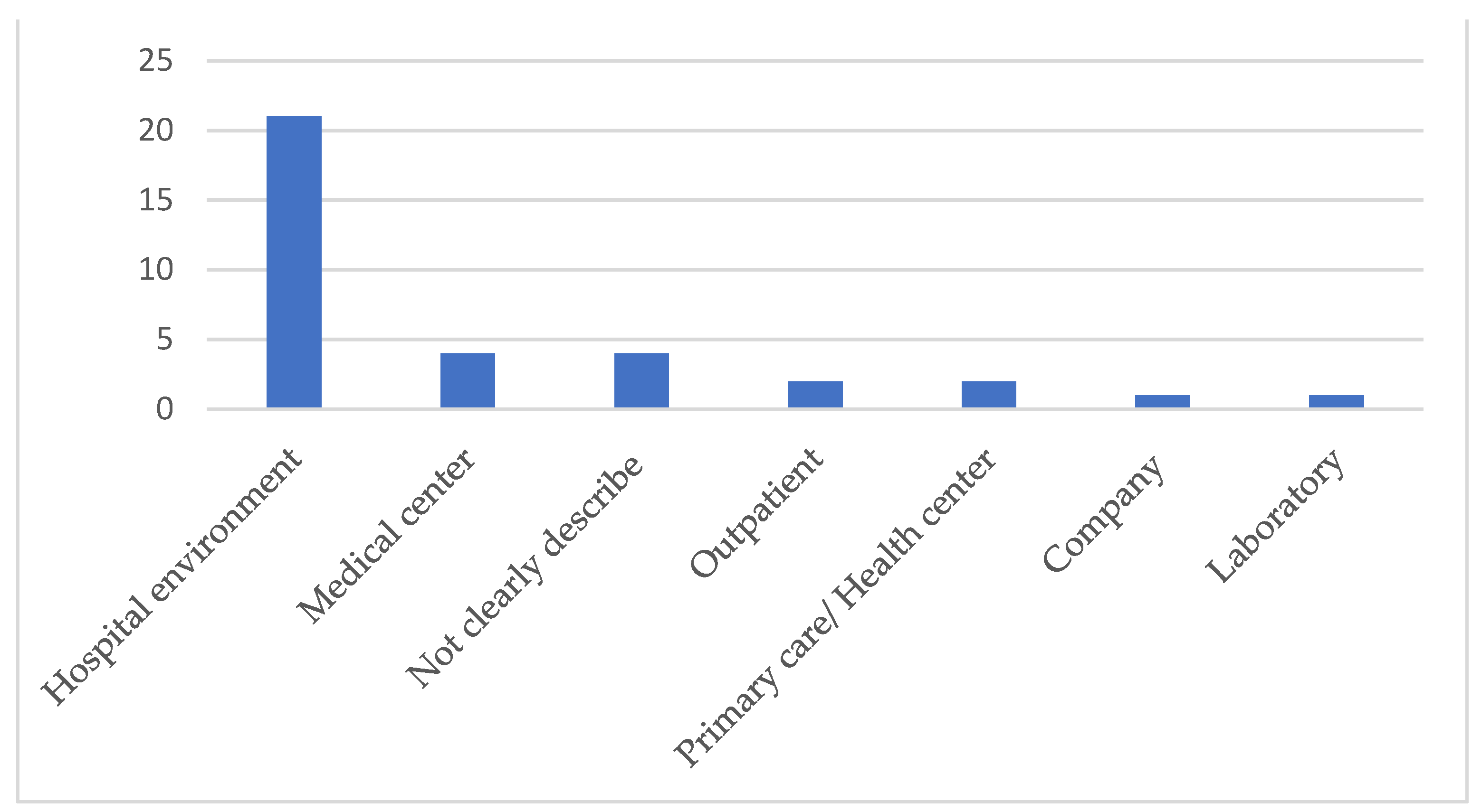
3. Results
4. Discussion
5. Conclusions
5.1. Study Limitations
5.2. Contributions to the Area
5.3. Future Studies
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year Country Journal | Levels of Evidency | Objectives | Tools | Outcomes |
|---|---|---|---|---|
| 2015 [64] Spain. Metas Enfermería., | Not rated. | Identify the factors that influence waiting times and implement solutions to reduce it. | - Map of steps; - Spaghetti diagram; - Value Stream Map (VSM) | - Increase in added value in the care of pregnant women and women who have recently given birth. |
| 2015 [50] Brazil. Rev. Lat. Am Enfermagem | Six. | Compare the application of the Total Quality (TQ) models with another health institution and also with the cases of lean healthcare exposed in the literature. | - 5S; - A3; - Failure Mode and Effect Analysis (FMEA); - VSM; - Plan-Do-Check-Act (PDCA); - Kaizen. | - Decreased workload in 70 min; - Increase in the time allocated for assistance of 9 min. |
| 2015 [23] United States. Prof Case Manag, | Not rated. | Equip leaders in the field of case management to facilitate alignment with the hospital’s pay-for-performance measures. | - Strengths, Weaknesses, Opportunities, Threats (SWOT). | - Reduction of the patient’s permanence time by 2.6% for managed patients. |
| 2015 [46]. United States. Cardiovasc Revasc Med. | Six. | To study the impact of Lean Six Sigma (LSS) in improving the efficiency and transfer of patients in a catheterization laboratory. | - VSM. | - Decrease in length of stay from 20.6% to 17.8%; - Increase in cases with punctual onset from 76.1 to 81.9%; - Increase in cases with ideal shift time from 50.9% to 60.4%. |
| 2015 [44]. Senegal. Glob Health Action. | Not rated. | Evaluate how 5S assists in changes in the workplace, in the process and in the results of health services. | - 5S. | - Areas with less unwanted items, better organization and visualization; - More efficient and patient-centered services; - Change in the behavior of the team and patients. |
| 2015 [47]. United States. Am J Med Qual, 2015. | Not rated. | Evaluate the implementation of an automated infusion system to reduce waste. | - VSM. | - Reduction in the distance covered by professionals by 14.6%; - Cost increase from US $ 2.68 to US $ 14.61/patient; - Reduction of time to perform tasks in 26 min/day. |
| 2016 [31]. Brazil. Prod. plan. Control. | Not rated. | Propose a new approach to value stream mapping that serves as a standard model for Lean applications in hospitals. | - VSM. | - Reduction of treatment time from 187 to 60 days; - Reduction in transitions between departments from 23 to 17; - Reduction, for patients, of trips to the hospital from 9 to 5. |
| 2016 [48]. United States. Ann Plast Surg, | Six. | Assess the impact of a Six Sigma program at a medical center. | - Voice of the Costumer (VOC); - Suppliers, inputs, process, outputs, customers analysis (SIPOC); - Define, Measure, Analyze, Improve, Control (DMAIC); - Ishikawa Diagram. | - Decreased total operative time from 714 to 607 min; - Decrease in hospital stay by 1.1 days; (6.3 to 5.2 days); - Increase of US $ 1.31 in medical prescription/minute and US $ 3.27 in hospital/minute. |
| 2016 [42]. United States. J. Oncol. Pract. | Not rated. | Evaluate the chemotherapy prescription process to improve your safety. | - Ishikawa Diagram. | - Increased time spent with the patient by 22 min. |
| 2016 [54]. Saudi Arabia. Stud. Health Technol. Inform. | Six. | Improve the use of glucose reagent strips. | - DMAIC. | - Increase in the number of glucometers in the units; - Reduction of unnecessary total executions from 13% to 4%; - Reduction of failed executions from 14% to 7% and reduction of the quality control/patient ratio from 24/76 to 19/81; - Decrease in the total number of strips used in quality control runs by 18.6% and increase in the total number of strips used in patient tests by 10.4%. |
| 2016 [41]. United States. Mil Med. | Six. | Improve the mass immunization process. | - VSM; - SIPOC; - 5S. | - Decrease in lead time spent by aspirants on their immunization by 79%; - Reduction of the work team to carry out the immunization process by 10%. |
| 2017 [22]. United States. Med Care. | Not rated. | Evaluate the current process and the efficiency standards of the Veterans Choice Program. | - VSM; - 5S; - DMAIC. | - Waste identification; - Recommendations for improvements. |
| 2017 [57] United States. J Pediatr Surg, | Not rated. | Determine whether Lean Six Sigma contributes to process improvement when applied simultaneously to all services in an academic hospital. | - SIPOC; - Ishikawa Diagram; - Pareto Diagram; - DMAIC. | - Reduction of the patient’s turnover time from 41 to 32 min; - Decrease in the time between the incision and the application of the surgical dressing from 81.5 to 71 min. |
| 2017 [38] Italy. J Eval Clin Pract, | Not rated. | Demonstrate the efficiency of Lean Six Sigma and DMAIC for solutions that allow quality improvement and cost reduction. | - DMAIC; - Gantt Diagram; - Brainstorming; - VSM. | - Reduction of the patient’s residence time by 42%; - Cost reduction of € 260,000/year. |
| 2017 [45] United States. J Perianesth Nurs. | Six. | Discuss the implementation of new practices in the preoperative period, along with the benefits and obstacles. | - DMAIC. | - Improved communication between staff, patients and family. |
| 2017 [21] Brazil. Int J Health Plann Manage. | Six. | Investigate the history of implementation of Lean Healthcare in Brazil, present particularities of lean implementation in the health sector, especially in developing countries, and suggest relevant topics for future research. | - DMAIC; - VSM; - Kaizen; - 5S; - Kanban; - Gemba; - Spaghetti diagram; - Matrix exchange tool. | - Improved financial performance; - Increased capacity and productivity; - Decrease in lead time. |
| 2017 [51] United States. J Am Coll Radiol. | Not rated. | Use the Lean Six Sigma methodology to assess and decrease the waiting time from the outpatient scheduling process to the scheduled procedure. | - VSM; - DMAIC; - FMEA; - Brainstorming; - SIPOC. | - Lead time was not influenced by the day of the week or by the nurse. |
| 2017 [55] Italy. J Eval Clin Pract, | Not rated. | Reduce the number of patients affected by bacterial infections. | - DMAIC; - Critical to Quality Tree (CTQ); - SIPOC; - Ishikawa Diagram. | - Reduction in the number of colonized patients from 0.37% to 0.21%; - Decrease in the average number of days of hospitalization. |
| 2017 [49] United States. Nurs Econ. | Six. | Examine the impact of Heijunka on the distribution of consultations and decreased waiting times. | - Heijunka. | - Increase in the number of patients treated from 3385 to 3738; - Reduction of waiting time; - Increase in revenue. |
| 2017 [39] United States. Anesth. Analg. | Not rated. | Resolve deficiencies in the pediatric anesthesia supply chain. | - DMAIC; - VSM; - Spaghetti diagram; - VOC. | - Reduction of the distance covered by the anesthesia technician by 28%. |
| 2018 [52] United States. Jt Comm J Qual Patient Saf, | Not rated. | Increase discharge prescriptions to 40% by 10 am and 12% effective patient departures by 12 noon. | - DMAIC; - Flowchart; - Ishikawa Diagram; - Pareto Diagram. | - Increase in discharge prescriptions up to 10:00 from 15.6% to 47.1%; - Increase of the patient’s effective departure until 12:00 from 10.5% to 20.6%. |
| 2018 [30] Brazil. Einstein. | Not rated. | Verify the impact of Lean Six Sigma in reducing incorrect entries of inappropriate income and expenses. | - DMAIC; - CTQ; - VOC; - SIPOC; - Ishikawa Diagram; - Pareto Diagram. | - Sigma level increased from 3.44 to 5.92; - Reduction to 0% of inappropriate revenues and expenses, generating savings of R $ 1.8 million. |
| 2018 [53] United States. Qual. Manag. Health Care | Not rated. | Reduce expenses by improving the registration process for patient insurance data. | - DMAIC; - SIPOC; - Pareto Diagram; - Brainstorming. | - Reduction in the number of occurrences due to billing errors, non-insurance coverage and incorrect information of 99.6%. |
| 2018 [63] Italy. J Eval Clin Pract. | Not rated. | Reduce the risk of healthcare-associated infections through Lean Six Sigma. | - DMAIC; - Ishikawa Diagram. | - Reduction in the percentage of colonized patients from 0.36% to 0.19%. |
| 2018 [24] United States. Qual Manag Health Care. | Six. | Identify the root cause of repeated Computed Tomography (CT) losses and implement a solution to increase adherence to the departmental guideline. | - DMAIC; - Ishikawa Diagram. - 5 whys; - FMEA. | - Reduction in the rate of routine repeated CT scans unnecessarily from 15% to 4%. |
| 2018 [29] Brazil. Leadersh Health Serv. | Not rated. | Address problems in the flow of patients and identify the causes of waiting time through Lean Healthcare. | - A3; - VSM; - Gemba. | - Reduced waiting time by 4.5 h. - Increase by 50% of the complete and correct percentage. |
| 2018 [60] United States. Int J Health Care Qual Assur. | Not rated. | Describe the process used to standardize a Program for the Prevention of Violence at Work in a health system. | - Current State Map; - Poka Yoke; - VOC; - Just-in-time. | - Increase of requests to appeal the mitigation plan by 500%; - Reduction of the average cycle time from 30 to 10 days; - Increase in the number of trained professionals from 29 to 72. |
| 2019 [20] Brazil. Qual Manag Health Care. | Not rated. | Integrate systematic architectural planning techniques with “Lean Healthcare” practices. | - VSM; - Analytic Hierarchy Process (AHP); - First in, first out; - Brainstorming. | - 75% reduction in overtime; - Increased productivity. |
| 2019 [56] Ireland. Int J Qual Health Care. | Six. | Optimize nursing time, improve personalized patient care and staff satisfaction. | - SIPOC; - DMAIC; - Spaghetti diagram; - VSM; - 5S. | - Reduction of lead time in 15 min; - Increased patient flow; - Reduction of the admission process to 5 min; - Reduction of patient stay and nursing time. |
| 2019 [25] Ireland. Clin Radiol. | Not rated. | To evaluate the use of the Lean Six Sigma methodology to improve the response time for peripherally inserted central catheters. | - VSM. | - Reduction of the time between the request and insertion of the catheter from 3.74 to 1.89 days; - 13.8% increase in radiological activity. |
| 2019 [59] Spain. Int J Health Plann Manage. | Six. | Improve work organization, reduce physical effort and obtain greater worker satisfaction. | - VSM; - Spaghetti diagram; - 5S; - Gemba; - Kaizen week; - PDCA. | - Reduction of the physical space necessary for the performance of work by 44%; - Reduced distance traveled from 318 to 50 m; - Increased professional satisfaction. |
| 2019 [32] United States. Quality Management in Healthcare. | Not rated. | Reduce the patient’s cycle time. | - DMAIC; - SIPOC; - FMEA; - Brainstorming. | - Cycle time reduction by 22% (15 min); - Increase in the number of assistance by 27%. |
| 2019 [33] Ireland. Int J Qual Health Care. | Six. | Increase the number of diagnoses of Low Grade Mucinous Neoplasms. | - DMAIC; - Specific, Measurable, Achieveable, Realistic, Time frame (SMART); - SIPOC; - Responsible, Accountable, Consulted and Informed (RACI); - CTQ; - VOC; - Ishikawa diagram; - 5 whys; - FMEA; -Possible, Implement, Challenge and Kill (PICK). | - Increase in patients with correct annual access for screening from 61% to 78%; - Increase of patients who received information by 90%, with the creation of the leaflet. |
References
- Arruda, N.M.; Maia, A.G.; Alves, L.C. Inequality in access to health services between urban and rural areas in Brazil: A disaggregation of factors from 1998 to 2008. Cad. Saude Publica 2018, 34. [Google Scholar] [CrossRef] [Green Version]
- Malta, D.C.; Bernal, R.T.I.; Lima, M.G.; de Araújo, S.S.C.; da Silva, M.M.A.; de Freitas, M.I.F.; de Barros, M.B.A. Noncommunicable diseases and the use of health services: Analysis of the National Health Survey in Brazil. Rev. Saude Publica 2017, 51, 1S–10S. [Google Scholar] [CrossRef] [Green Version]
- Radnor, Z.J.; Holweg, M.; Waring, J. Lean in healthcare: The unfilled promise? Soc. Sci. Med. 2012, 74, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Henrique, D.B.; Godinho Filho, M. A systematic literature review of empirical research in Lean and Six Sigma in healthcare. Total Qual. Manag. Bus. Excell. 2020, 31, 429–449. [Google Scholar] [CrossRef]
- Marodin, G.; Frank, A.G.; Tortorella, G.L.; Netland, T. Lean product development and lean manufacturing: Testing moderation effects. Int. J. Prod. Econ. 2018, 203, 301–310. [Google Scholar] [CrossRef]
- Raweewan, M.; Kojima, F. Digital lean manufacturing Collaborative university-industry education in systems design for lean transformation. In Proceedings of the Procedia Manufacturing; Elsevier B.V.: Amsterdam, The Netherlands, 2020; Volume 45, pp. 183–188. [Google Scholar]
- Kafuku, J.M. Factors for effective implementation of lean manufacturing practice in selected industries in Tanzania. In Proceedings of the Procedia Manufacturing; Elsevier B.V.: Amsterdam, The Netherlands, 2019; Volume 33, pp. 351–358. [Google Scholar]
- Toussaint, J.S.; Berry, L.L. The promise of lean in health care. Mayo Clin. Proc. 2013, 88, 74–82. [Google Scholar] [CrossRef] [Green Version]
- Mousavi Isfahani, H.; Tourani, S.; Seyedin, H. Features and Results of Conducted Studies Using a Lean Management Approach in Emergency Department in Hospital: A Systematic Review. Bull. Emerg. Trauma 2019, 7, 9–20. [Google Scholar] [CrossRef]
- Belhadi, A.; Sha’ri, Y.B.M.; Touriki, F.E.; El Fezazi, S. Lean production in SMEs: Literature review and reflection on future challenges. J. Ind. Prod. Eng. 2018, 35, 368–382. [Google Scholar] [CrossRef]
- Cohen, R.I. Lean Methodology in Health Care. Chest 2018, 154, 1448–1454. [Google Scholar] [CrossRef]
- Womack, J.P.; Jones, D.T.; Roos, D. The Machine That Changed the World; Rawson Associates: New York, NY, USA, 1990; ISBN 0743299795. [Google Scholar]
- Mendes, K.D.S.; de Silveira, R.C.C.P.; Galvão, C.M. Revisão integrativa: Método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto Context. Enferm. 2008, 17, 758–764. [Google Scholar] [CrossRef] [Green Version]
- Marinho, A.M.; Sabino, F.H.O.; Monteiro, D.A.T.; da Filgueira, V.S.A.; de Azevedo, G.N.; Toffano, S.E.M. Difficult peripheral venous puncture in adults: Integrative review. Rev. Enferm. Uerj 2019, 27, 42567. [Google Scholar] [CrossRef]
- da Santos, C.M.C.; de Pimenta, C.A.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Galvão, T.F.; Pansani, T.S.A.; Harrad, D. Principais itens para relatar Revisões sistemáticas e Meta-análises: A recomendação PRISMA. Epidemiol. e Serviços Saúde 2015, 24, 335–342. [Google Scholar] [CrossRef]
- Ursi, E.S.; Galvão, C.M. Prevenção de lesões de pele no perioperatório: Revisão integrativa da literatura. Rev. Lat. Am. Enferm. 2006, 14, 124–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 1–6. [Google Scholar]
- Fernández Aranda, M.I. Aplicación del método Lean Healthcare en un servicio de Ginecología y Obstetricia. Metas de Enfermería 2016, 19, 21–26. [Google Scholar]
- Fogliatto, F.S.; Tortorella, G.L.; Anzanello, M.J.; Tonetto, L.M. Lean-oriented layout design of a health care facility. Qual. Manag. Health Care 2019, 28, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.B.M.; Filho, M.G.; Rentes, A.F.; Bertani, T.M.; Mardegan, R. Lean healthcare in developing countries: Evidence from Brazilian hospitals. Int. J. Health Plann. Manag. 2017, 32, 99–120. [Google Scholar] [CrossRef] [PubMed]
- Ball, S.; Stevenson, L.; Ladebue, A.; McCreight, M.; Lawrence, E.; Oestreich, T. Adaptation of Lean Six Sigma Methodologies for the Evaluation of Veterans Choice Program at 3 Urban Veterans Affairs Medical Centers. Med. Care 2017, 55, 76–83. [Google Scholar] [CrossRef]
- Granata, R.L.; Hamilton, K. Exploring the effect of at-risk case management compensation on hospital pay-for-performance outcomes: Tools for change. Prof. Case Manag. 2015, 20, 14–27. [Google Scholar] [CrossRef] [Green Version]
- Birmingham, L.E.; Sedorovich, A.; Mann, N.; George, R.L. Using Lean Six Sigma to Improve Delayed Intracranial Hemorrhage Screening in a Geriatric Trauma Population. Qual. Manag. Health Care 2018, 27, 199–203. [Google Scholar] [CrossRef]
- Hynes, J.P.; Murray, A.S.; Murray, O.M.; Eustace, S.K.; Gilchrist, S.; Dolan, A.; Lawler, L.P. Use of Lean Six Sigma methodology shows reduction of inpatient waiting time for peripherally inserted central catheter placement. Clin. Radiol. 2019, 74, 733–735. [Google Scholar] [CrossRef] [PubMed]
- Womack, J.P.; Jones, D.T.; Roos, D. A Máquina Que Mudou o Mundo, 5th ed.; Campus: Rio de Janeiro, Brazil, 2004; ISBN 1847370551. [Google Scholar]
- Buzzi, D.; Plytiuk, C.F. Pensamento enxuto e sistemas de saúde: Um estudo da aplicabilidade de conceitos e ferramentas lean em contexto hospitalar. Rev. Qual. Emerg. 2011, 2, 18–38. [Google Scholar] [CrossRef] [Green Version]
- Garre, P.; Nikhil Bharadwaj, V.V.S.; Shiva Shashank, P.; Harish, M.; Sai Dheeraj, M. Applying lean in aerospace manufacturing. In Proceedings of the Materials Today: Proceedings; Elsevier: Amsterdam, The Netherlands, 2017; Volume 4, pp. 8439–8446. [Google Scholar]
- Lot, L.T.; Sarantopoulos, A.; Min, L.L.; Perales, S.R.; de Boin, I.F.S.F.; de Ataide, E.C. Using Lean tools to reduce patient waiting time. Leadersh. Health Serv. 2018, 31, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Pavão, D.N.; Buttignol, M.; Pereira, A.J.; Tanjoni, R.; de Almeida, E.H.P.; Leisnock, P.; Sato, G.; Silva, E. Efficiency in the operational process: Reduction of incorrect entries and guarantee of compliance in the rendering of accounts. Einstein 2018, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Henrique, D.B.; Rentes, A.F.; Filho, M.G.; Esposto, K.F. A new value stream mapping approach for healthcare environments. Prod. Plan. Control 2016, 27, 24–48. [Google Scholar] [CrossRef]
- Kovach, J.V.; Ingle, D. Using Lean Six Sigma to Reduce Patient Cycle Time in a Nonprofit Community Clinic. Qual. Manag. Health Care 2019, 28, 169–175. [Google Scholar] [CrossRef] [PubMed]
- McGrath, K.; Casserly, M.; O’mara, F.; Mulsow, J.; Shields, C.; Staunton, O.; Teeling, S.P.; Ward, M. Zap it track it: The application of Lean Six Sigma methods to improve the screening system of low-grade mucinous neoplasms of the appendix in an acute hospital setting. Int. J. Qual. Health Care 2019, 31, 35–44. [Google Scholar] [CrossRef]
- Moyano-Fuentes, J.; Bruque-Cámara, S.; Maqueira-Marín, J.M. Development and validation of a lean supply chain management measurement instrument. Prod. Plan. Control 2019, 30, 20–32. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Essentials of Nursing Research Seventh Edition Appraising Evidence for Nursing Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; ISBN 9788578110796. [Google Scholar]
- Rodrigues, F.W.A.; Ramos, A.B.B. Metodologia científica: Análise e reflexão sobre a percepção dos graduandos. Int. J. Educ. Teach. 2019, 2, 47–60. [Google Scholar] [CrossRef] [Green Version]
- Guimarães, C.A. Normas para manuscritos submetidos às revistas biomédicas: Escrita e edição da publicação biomédica (tradução integral do texto). Rev. Col. Bras. Cir. 2008, 35, 425–441. [Google Scholar] [CrossRef] [Green Version]
- Improta, G.; Balato, G.; Romano, M.; Ponsiglione, A.M.; Raiola, E.; Russo, M.A.; Cuccaro, P.; Santillo, L.C.; Cesarelli, M. Improving performances of the knee replacement surgery process by applying DMAIC principles. J. Eval. Clin. Pract. 2017, 23, 1401–1407. [Google Scholar] [CrossRef]
- Roberts, R.J.; Wilson, A.E.; Quezado, Z. Using Lean Six Sigma Methodology to Improve Quality of the Anesthesia Supply Chain in a Pediatric Hospital. Anesth. Analg. 2017, 124, 922–924. [Google Scholar] [CrossRef]
- Liker, J.K. O Modelo Toyota: 14 Princípios de Gestão do Maior Fabricante do Mundo, 1st ed.; Bookman Editora: New York, NY, USA, 2005; ISBN 8536304952. [Google Scholar]
- Ha, C.; McCoy, D.A.; Taylor, C.B.; Kirk, K.D.; Fry, R.S.; Modi, J.R. Using lean six sigma methodology to improve a mass immunizations process at the United States naval academy. Mil. Med. 2016, 181, 582–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, N.N.; Casella, E.; Capozzi, D.; McGettigan, S.; Gangadhar, T.C.; Schuchter, L.; Myers, J.S. Improving the safety of oral chemotherapy at an academic medical center. J. Oncol. Pract. 2016, 12, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva, A.L.; da Oliveira, E.S.; Borges, J.A.; Maia, P.H.M.; Fructuozo, R.A.; Torricelli, T.A.; Pereira, L.C. Implantação do Diagrama de Ishikawa no sistema de gestão da qualidade de uma empresa de fabricação termoplástica, para resolução e devolutiva de relatórios de não conformidade enviados pelo cliente. Rev. Gestão em Foco 2018, 387–397. [Google Scholar]
- Kanamori, S.; Sow, S.; Castro, M.C.; Matsuno, R.; Tsuru, A.; Jimba, M. Implementation of 5S management method for lean healthcare at a health center in Senegal: A qualitative study of staff perception. Glob. Health Action 2015, 8. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.; Franklin, T. Improving Preoperative Throughput. J. Perianesthesia Nurs. 2017, 32, 38–44. [Google Scholar] [CrossRef]
- Agarwal, S.; Gallo, J.J.; Parashar, A.; Agarwal, K.K.; Ellis, S.G.; Khot, U.N.; Spooner, R.; Murat Tuzcu, E.; Kapadia, S.R. Impact of lean six sigma process improvement methodology on cardiac catheterization laboratory efficiency. Cardiovasc. Revascularization Med. 2016, 17, 95–101. [Google Scholar] [CrossRef]
- Rico, F.; Yalcin, A.; Eikman, E.A. Technology Integration Performance Assessment Using Lean Principles in Health Care. Am. J. Med. Qual. 2015, 30, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Hultman, C.S.; Kim, S.; Lee, C.N.; Wu, C.; Dodge, B.; Hultman, C.E.; Tanner Roach, S.; Halvorson, E.G. Implementation and analysis of a lean six sigma program in microsurgery to improve operative throughput in perforator flap breast reconstruction. Ann. Plast. Surg. 2016, 76, 352–356. [Google Scholar] [CrossRef]
- Gavriloff, C.; Ostrowski-Delahanty, S.; Oldfield, K. The impact of lean six sigma methodology on patient scheduling. Nurs. Econ. 2017, 35, 189–193. [Google Scholar]
- Yuri, N.E.; Silveira, A.T.-J. Comparative study: TQ and Lean Production ownership models in health services. Rev. Lat. Am. Enfermagem 2015, 23, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Dowell, J.D.; Makary, M.S.; Brocone, M.; Sarbinoff, J.G.; Vargas, I.G.; Gadkari, M. Lean Six Sigma Approach to Improving Interventional Radiology Scheduling. J. Am. Coll. Radiol. 2017, 1316–1321. [Google Scholar] [CrossRef] [PubMed]
- Molla, M.; Warren, D.S.; Stewart, S.L.; Stocking, J.; Johl, H.; Sinigayan, V. A Lean Six Sigma Quality Improvement Project Improves Timeliness of Discharge from the Hospital. Jt. Comm. J. Qual. Patient Saf. 2018, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kovach, J.V.; Borikar, S. Enhancing Financial Performance: An Application of Lean Six Sigma to Reduce Insurance Claim Denials. Qual. Manag. Health Care 2018, 27, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Almorsy, L.; Khalifa, M. Lean six sigma in health care: Improving utilization and reducing waste. Stud. Health Technol. Inform. 2016, 194–197. [Google Scholar] [CrossRef]
- Montella, E.; Di Cicco, M.V.; Ferraro, A.; Centobelli, P.; Raiola, E.; Triassi, M.; Improta, G. The application of Lean Six Sigma methodology to reduce the risk of healthcare–associated infections in surgery departments. J. Eval. Clin. Pract. 2017, 23, 530–539. [Google Scholar] [CrossRef]
- Davies, C.; Lyons, C.; Whyte, R. Optimizing nursing time in a day care unit: Quality improvement using Lean Six Sigma methodology. Int. J. Qual. Health Care 2019, 31, 22–28. [Google Scholar] [CrossRef]
- Tagge, E.P.; Thirumoorthi, A.S.; Lenart, J.; Garberoglio, C.; Mitchell, K.W. Improving operating room efficiency in academic children’s hospital using Lean Six Sigma methodology. J. Pediatr. Surg. 2017, 55, 1040–1044. [Google Scholar] [CrossRef]
- Krishnaiyer, K.; Chen, F.F.; Burgess, B.; Bouzary, H. D3S Model for Sustainable Process Excellence. In Proceedings of the Procedia Manufacturing; Elsevier B.V.: Amsterdam, The Netherlands, 2018; pp. 1441–1447. [Google Scholar]
- Damián Sanz, M.; Yagüe-Fabra, J.A.; Gracia Matilla, R. Use of Lean techniques in health care in Spain to improve involvement and satisfaction of workers. Int. J. Health Plann. Manag. 2019, 34, 274–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutton, S.A.; Vance, K.; Burgard, J.; Grace, S.; Van Male, L. Workplace violence prevention standardization using lean principles across a healthcare network. Int. J. Health Care Qual. Assur. 2018, 31, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Pinto, C.F. Em Busca do Cuidado Perfeito. Lean Institute Brasil: São Paulo, Brazil, 2014; ISBN 9788588874169. [Google Scholar]
- Dorval, M.; Jobin, M.H.; Benomar, N. Lean culture: A comprehensive systematic literature review. Int. J. Product. Perform. Manag. 2019, 68, 920–937. [Google Scholar] [CrossRef]
- Improta, G.; Cesarelli, M.; Montuori, P.; Santillo, L.C.; Triassi, M. Reducing the risk of healthcare-associated infections through Lean Six Sigma: The case of the medicine areas at the Federico II University Hospital in Naples (Italy). J. Eval. Clin. Pract. 2018, 24, 338–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melnyk, B.M.; Fineout-Overholt, E. Evidence-Based Practice in Nursing & Healthcare: A Guide to Best Practice, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; ISBN 1605477788. [Google Scholar]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Barros, L.B.; Bassi, L.d.C.; Caldas, L.P.; Sarantopoulos, A.; Zeferino, E.B.B.; Minatogawa, V.; Gasparino, R.C. Lean Healthcare Tools for Processes Evaluation: An Integrative Review. Int. J. Environ. Res. Public Health 2021, 18, 7389. https://doi.org/10.3390/ijerph18147389
de Barros LB, Bassi LdC, Caldas LP, Sarantopoulos A, Zeferino EBB, Minatogawa V, Gasparino RC. Lean Healthcare Tools for Processes Evaluation: An Integrative Review. International Journal of Environmental Research and Public Health. 2021; 18(14):7389. https://doi.org/10.3390/ijerph18147389
Chicago/Turabian Stylede Barros, Letícia Bianchini, Letícia de Camargo Bassi, Laura Passos Caldas, Alice Sarantopoulos, Eliete Boaventura Bargas Zeferino, Vinicius Minatogawa, and Renata Cristina Gasparino. 2021. "Lean Healthcare Tools for Processes Evaluation: An Integrative Review" International Journal of Environmental Research and Public Health 18, no. 14: 7389. https://doi.org/10.3390/ijerph18147389
APA Stylede Barros, L. B., Bassi, L. d. C., Caldas, L. P., Sarantopoulos, A., Zeferino, E. B. B., Minatogawa, V., & Gasparino, R. C. (2021). Lean Healthcare Tools for Processes Evaluation: An Integrative Review. International Journal of Environmental Research and Public Health, 18(14), 7389. https://doi.org/10.3390/ijerph18147389