
Effectiveness of Swimming Program in Adolescents with Down Syndrome



Abstract
:1. Introduction
2. Materials and Methods
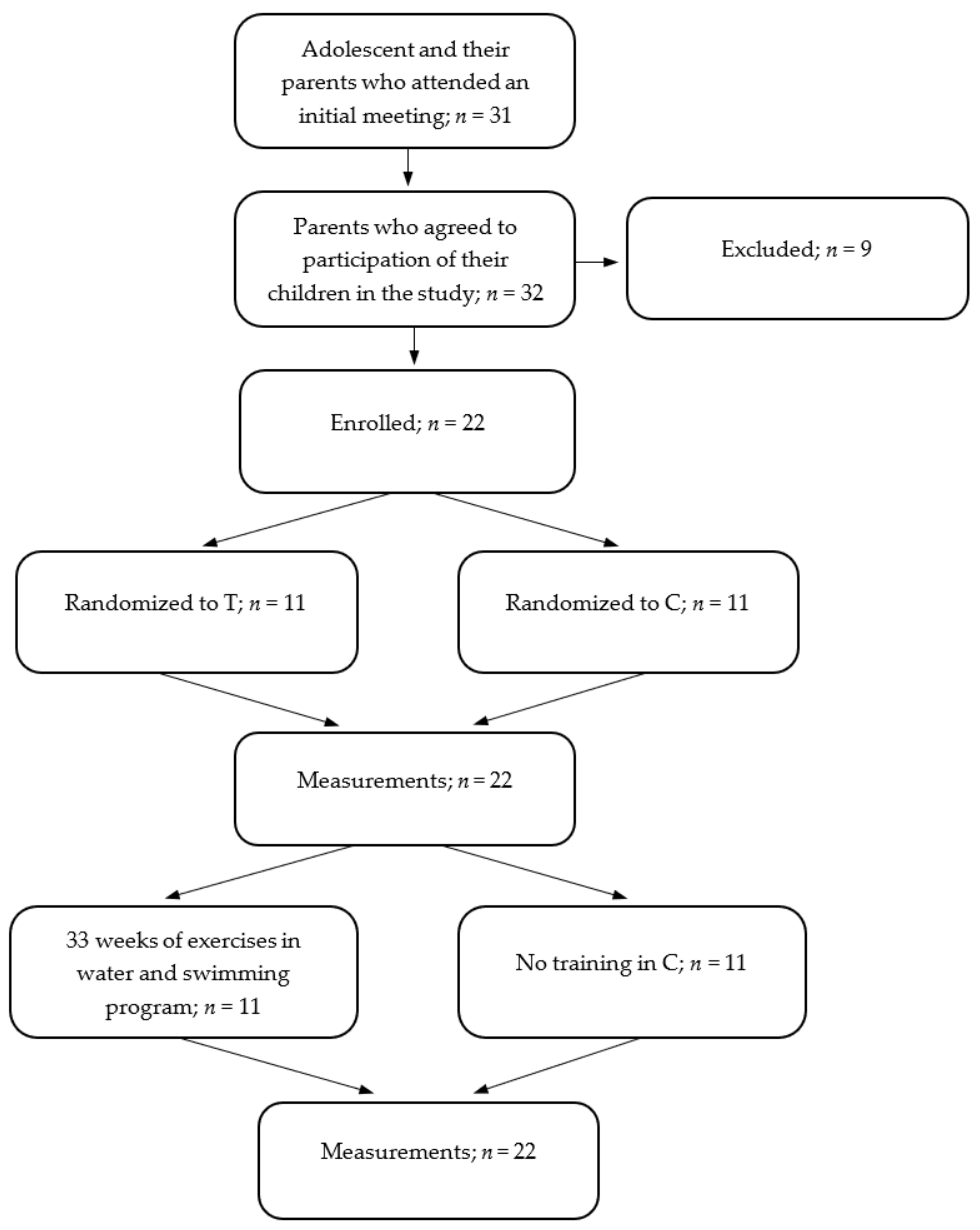
2.1. Participants
2.2. Testing
2.3. Eurofit Test
- plate tapping-tests which measure the speed of limb movement
- handgrip test which measures static arm strength (using Takei 5401 dynamometer, Takei, Niigata, Japan)
- flamingo balance test which is a single leg balance test
- sit-and-reach flexibility test
- sit-ups in 30 s which measure trunk strength
- bent arm hang which measures muscular endurance/functional strength
2.4. Aerobic Capacity
2.5. Water Orientation Test Alyn 2 (WOTA2)
2.6. Training Program
- At the first stage, which lasted 4 weeks, the adolescents were getting used to the aquatic environment, and mainly water games were used to that effect. During this stage the participants learned how to submerge their heads under water, open their eyes under water, and lie in the water on their chests and backs. After this stage, the adolescents were visibly happy when they were entering the water, they showed no fear of the aquatic environment. At this stage swimming session lasted 70 min.
- At the second stage, which also lasted 4 weeks, water games were still carried out and the participants were taught to exhale into the water, slide on the chest and back, and make simple jumps into the water, at the end of this stage the participants had the ability to float on the water. At this stage swimming session lasted 80 min.
- At the third stage, lasting 15 weeks, the adolescents learned to swim in the four swimming styles: backstroke, crawl, breaststroke and butterfly, water games constituted 30% of the main part of the training session, learning to swim constituted 70% of the main part of the training session. At this stage swimming session lasted 90 min.
- The last 10-week stage was aimed at improving swimming skills. The exercises performed with and without the swimming equipment were focused on improving the swimming technique. During these training sessions, the adolescents usually swam 700 to 1000 m. At this stage swimming session lasted 90 min.
2.7. Training Session
- the warm-up outside the pool—10 min; and warm-up in water—10 min;
- the main part of the training session for the first 4 weeks lasted 30 min, the next 4 weeks—40 min; and in the following weeks—50 min;
- the recovery part (games in the water) lasted 20 min.
2.8. Statistical Analysis
3. Results
4. Discussion
5. Limitations and Strengths of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bertapelli, F.; Pitetti, K.; Agiovlasitis, S.; Guerra-Junior, G. Overweight and obesity in children and adolescents with Down syndrome-prevalence, determinants, consequences, and interventions: A literature review. Res. Dev. Disabil. 2016, 57, 181–192. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Risks Mortality and Burden of Disease Attributable to Selected Major Risks; WHO Library Cataloguing-in-Publication Data; World Health Organization: Geneva, Switzerland, 2009; pp. 1–62. [Google Scholar]
- Vis, J.C.; Duffels, M.G.J.; Winter, M.M.; Weijerman, M.E.; Cobben, J.M.; Huisman, S.A.; Mulder, B.J.M. Down syndrome: A cardiovascular perspective. J. Intellect. Disabil. Res. 2009, 53, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Heller, T.; Hsieh, K.; Rimmer, J. Barriers and support for exercise participation among adults with Down syndrome. J. Gerontol. Soc. Work 2008, 38, 161–178. [Google Scholar] [CrossRef]
- Castro-Piñero, J.; Carbonell-Baeza, A.; Martinez-Gomez, D.; Gómez-Martínez, S.; Cabanas-Sánchez, V.; Santiago, C.; Veses, A.N.; Bandrés, F.; Gonzalez-Galo, A.; Gomez-Gallego, F.; et al. Follow-up in healthyschoolchildren and in adolescents with DOWN syndrome: Psycho-environmental and genetic determinants of physical activity andits impact on fitness, cardiovascular diseases, inflammatory biomarkersand mental health; the UP&DOWN Study. BMC Public Health 2014, 14, 400. [Google Scholar]
- Fernhall, B.; McCubbin, J.A.; Pitetti, K.H.; Rintala, P.; Rimmer, J.H.; Millar, A.L.; De Silva, A. Prediction of maximal heart rate in individuals with mental retardation. J. Sci. Med. Sports 2001, 33, 1655–1660. [Google Scholar] [CrossRef] [PubMed]
- Wee, S.O.; Pitetti, K.H.; Goulopoulou, S.; Collier, S.R.; Guerra, M.; Baynard, M. Impact of obesity and Down syndrome on peak heart rate and aerobic capacity in youth and adults. Res. Dev. Disabil. 2015, 36C, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.F. Mortality among people with mental retardation living in the united states: Research review and policy application. Ment. Retard. 1998, 36, 345–359. [Google Scholar] [CrossRef]
- Izquierdo-Gomez, R.; Martinez-Gomez, D.; Villagra, A.; Fernhall, B.; Veiga, O.L. Associations of physical activity with fatness and fitness in adolescents with Down syndrome: The UP & DOWN study. Res. Dev. Disabil. 2015, 36, 428–436. [Google Scholar]
- Pitetti, K.; Baynard, T.; Agiovlasitis, S. Children and adolescents with Down syndrome, physical fitness and physical activity. J. Sports Health. Sci. 2013, 2, 47–57. [Google Scholar] [CrossRef] [Green Version]
- DHSC. UK Chief Medical Officers Physical Activity Guidelines; Department of Health and Social Care: London, UK, 2019; pp. 1–65. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 16 Million Participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Shields, N.; Plant, S.; Warren, C.; Wollersheim, D.; Peiris, C. Do adults with Down syndrome do the same amount of physical activity as adults without disability? A proof of principle study. J. Appl. Res. Intellect. Disabil. 2018, 31, 459–465. [Google Scholar] [CrossRef]
- Seron, B.B.; Modesto, E.L.; Stanganelli, L.C.R.; Oliveira de Carvalho, E.M.; Greguol, M. Effects of aerobic and resistance training on the cardiorespiratory fitness of young people with Down Syndrome. Rev. Bras. Cineantropom. Hum. 2017, 19, 385–394. [Google Scholar] [CrossRef] [Green Version]
- Paul, Y.; Ellapen, T.J.; Barnard, M.; Hammill, H.V.; Swanepoel, M. The health benefits of exercise therapy for patients with Down syndrome: A systematic review. Afr. J. Disabil. 2019, 8, a576. [Google Scholar] [CrossRef]
- Ilinca, I.; Roșulescu, E.; Cosma, G.; Danoiu, M. The influence of physiotherapy on functional fitness of adults with down syndrome. Phys. Ed. Sport Kin. J. 2019, 97–100. [Google Scholar] [CrossRef]
- Millar, A.L.; Fernhall, B.; Burkett, L.N. Effects of aerobic training in adolescents with Down syndrome. Med. Sci. Sports Exerc. 1993, 25, 270–274. [Google Scholar] [CrossRef]
- Pérez, C.A.; Carral, J.M.C.; Costas, A.A.; Martínez, S.V.; Martínez-Lemos, R.I. Water-based exercise for adults with Down syndrome: Findings from a preliminary study. Int. J. Ther. Rehabil. 2018, 25, 20–28. [Google Scholar] [CrossRef]
- Suarez-Villadat, B.; Veiga, O.L.; Villagraa, A.Z.; Izquierdo-Gomez, R.P.; UP&DOWN Study Group. Changes in Body Composition and Physical Fitness in Adolescents with Down Syndrome: The UP&DOWN Longitudinal Study. Child. Obes. 2019, 15, 397–405. [Google Scholar]
- MacDonncha, C.; Watson, A.S.; McSweeney, T.; O’Donovan, D. Reliability of Eurofit physical items for adolescent males with and without mental retardation. Adapt. Phys. Act. Q. 1999, 16, 86–95. [Google Scholar]
- Baynard, T.; Pitetti, K.H.; Guerra, M.; Unnithan, V.B.; Fernhall, B. Age-Related Changes in Aerobic Capacityin Individuals with Mental Retardation: A 20-yr Review. Med. Sci. Sports Exerc. 2008, 40, 1984–1989. [Google Scholar] [CrossRef]
- Fernhall, B.; Pitetti, K.H.; Rimmer, J.H.; McCubbin, J.A.; Rintala, P.; Millar, A.L.; Kittredge, J.; Burkett, L.N. Cardiorespiratory capacity of individuals with mental retardation including Down syndrome. Med. Sci. Sports Exerc. 1996, 28, 366–371. [Google Scholar]
- The American Academy for Cerebral Palsy and Developmental Medicine. Available online: https://www.aacpdm.org/UserFiles/file/BRK9c_Tirosh.pdf (accessed on 6 July 2021).
- Tirosh, R.; Katz-Leurer, M.; Getz, M.D. Halliwick-Based Aquatic Assessments: Reliability and Validity. Int. J. Aquat. Res. Educ. 2008, 3, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- González-Agüero, A.; Ara, I.; Moreno, L.A.; Vicente-Rodríguez, G.; Casajús, J.A. Fat and lean masses in youths with Down syndrome: Gender differences. Res. Dev. Disabil. 2011, 33, 1685–1693. [Google Scholar] [CrossRef]
- Murray, J.; Ryan-Krause, P. Obesity in children with down syndrome: Background and recommendations for management. Pediatr. Nurs. 2010, 36, 314–319. [Google Scholar]
- O’Shea, M.; O’Shea, C.; Gibson, L.; Leo, J.; Carty, C. The prevalence of obesity in children and young people with Down syndrome. J. Appl. Res. Intellect. Disabil. 2018, 31, 1225–1229. [Google Scholar] [CrossRef]
- Maffeis, C.; Tato, L. Long-term effects of childhood obesity on morbidity and mortality. Horm. Res. 2001, 55 (Suppl. 1), 42–45. [Google Scholar] [CrossRef]
- Suarez-Villadat, B.; Luna-Olivac, L.; Acebesa, C.; Villagraa, A. The effect of swimming program on body composition levels in adolescents with Down syndrome. Res. Dev. Disabil. 2020, 102, 1–8. [Google Scholar] [CrossRef]
- Farías-Valenzuela, C.; Cofré-Bolados, C.; Ferrari, G.; Espoz-Lazo, S.; Arenas-Sánchez, G.; Álvarez-Arangua, S.; Espinoza-Salinas, A.; Valdivia-Moral, P. Effects of Motor-Games-Based Concurrent Training Program on Body Composition Indicators of Chilean Adults with Down Syndrome. Sustainability 2021, 13, 5737. [Google Scholar] [CrossRef]
- González-Agüero, A.; Vicente-Rodríguez, G.; Gómez-Cabello, A.; Ara, I.; Moreno, L.A.; Casajús, J.A. A combined training intervention programme increases lean mass in youths with Down syndrome. Res. Dev. Disabil. 2011, 32, 2383–2388. [Google Scholar] [CrossRef]
- Paffenbarger, R.S.; Blair, S.N.; Lee, I.M. A history of physical activity, cardiovascular health and longevity: The scientific cbcontributions of Jeremy N Morris, DSc, DPH, FRCP. Int. J. Epidemiol. 2001, 30, 1184–1192. [Google Scholar] [CrossRef]
- González-Agüero, A.; Vicente-Rodriguez, G.; Moreno, L.A.; Guerra-Balic, M.; Ara, I.; Casajus, J.A. Health-related physical fitness in children and adolescents with Down syndrome and response to training. Scand. J. Med. Sci. Sports 2010, 20, 716–724. [Google Scholar] [CrossRef]
- Savucu, Y. Influence of 12-Week Training on Aerobic Capacity and Respiratory Functions of Adolescents with down Syndrome. World Appl. Sci. J. 2010, 11, 1292–1296. [Google Scholar]
- Lewis, C.L.; Fragala-Pinkham, M.A. Effects of aerobic conditioning and strength training on a child with Down syndrome: A case study. Pediatr. Phys. Ther. 2005, 17, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Silva, V.; Campos, C.; Sá, A.; Cavadas, M.; Pinto, J.; Simões, P.; Machado, S.; Murillo-Rodríguez, E.; Barbosa-Rocha, N. Wii-based exercise program to improve physical fitness, motor proficiency and functional mobility in adults with Down syndrome. J. Intellectx. Disabil. Res. 2017, 61, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Parab, S.; Bose, M.; Shayer, S.; Saini, R.K.; Salvi, M.; Ravi, P.; Sawant, P. Bharatnatyam-based dance therapy in Children and and Adolescents with Down Syndrome. Clin. Kinesiol. 2019, 73, 15–20. [Google Scholar]
- Varela, A.M.; Sardinha, L.B.; Pitetti, K.H. Effects of an aerobic rowing training regimen in young adults with Down syndrome. Am. J. Ment. Retard. 2001, 106, 135–144. [Google Scholar] [CrossRef]
- Çiğdem, E.; Hüzmeli, E.D.; Gökçek, Ö. Investigation of the Relationship between Physical Activity and Body Mass Index in Children with Down Syndrome. J. Pediatr. Res. 2020, 7, 92–96. [Google Scholar]
- Vaščáková, T.; Kudláček, M. Halliwick Concept of Swimming and its Influence on Motoric Competencies of Children with Severe Disabilities. Eur. J. Adapt. Phys. Act. 2015, 8, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Declerck, M.; Verheul, M.; Daly, D.; Sanders, R. Benefits and Enjoyment of a Swimming Intervention for Youth with Cerebral Palsy: An RCT Study. Pediatr. Phys. Ther. 2016, 28, 162–169. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Group/Parameter | Height (m) | Body Mass (kg) | BMI | Fat (%) | Fat (kg) | VO2max (L/min) | VO2max (mL/kg/min) | HRmax | |
|---|---|---|---|---|---|---|---|---|---|
| T | Before | 1.50 ± 0.09 | 56.8 ± 7.97 | 25.1 ± 2.37 | 26.1± 4.23 | 15.1 ± 4.47 | 1.56 ± 0.33 | 27.4 ± 3.86 | 167 ± 9.66 |
| After | 1.52 ± 0.08 * | 55.0 ± 7.11 * | 24.0 ± 2.05 * | 23.7 ± 4.19 * | 13.2 ± 3.92 * | 1.74 ± 0.34 * | 31.7 ± 4.05 * | 168 ± 8.25 | |
| C | Before | 1.50 ± 0.12 * | 57.3 ± 8.43 | 25.4 ± 2.46 | 25.4 ± 3.32 | 14.5 ± 2.76 | 1.57 ± 0.35 | 27.2 ± 3.13 | 169 ± 5.79 |
| After | 1.52 ± 0.11 | 59.7 ± 8.29 * | 26.0 ± 2.72 * | 26.8 ± 3.47 * | 16.0 ± 3.11 * | 1.55 ± 0.33 | 25.9 ± 3.08 * | 169 ± 5.37 |
| Group/Parameter | Height (m) | Body Mass (kg) | BMI | Fat (%) | Fat (kg) | VO2max (L/min) | VO2max (mL/kg/min) | HRmax (b/min) | |
|---|---|---|---|---|---|---|---|---|---|
| T | % change | 0.84 ± 0.61 | −3.03± 1.60 * | −4.63 ± 1.80 * | −9.21 ± 5.89 * | −11.9 ± 6.64 * | 12.9 ± 12.0 * | 16.3 ± 11.6 * | 0.16 ± 1.40 |
| 95% CI | 0.48 to 1.20 | −3.98 to −2.08 | −5.69 to −3.57 | −12.7 to −5.73 | −15.8 to −7.99 | 5.75 to 20.0 | 9.44 to 23.2 | −0.67 to 0.99 | |
| T vs. C | ES | 0.14 | 3.14 | 3.33 | 3.10 | 4.09 | 1.25 | 2.17 | 0.06 |
| C | % change | 0.98 ± 1.18 | 4.39 ± 2.79 | 2.38 ± 2.23 | 5.57 ± 2.70 | 10.2 ± 3.13 | −0.54 ± 8.45 | −4.80 ± 6.38 | 0.07 ± 1.55 |
| 95% CI | 0.28 to 1.68 | 2.74 to 6.04 | 1.06 to 3.70 | 3.97 to 7.17 | 8.35 to 12.0 | −5.50 to 4.42 | −8.57 to −1.03 | −0.85 to 0.99 |
| Group/Muscle | Speed of Limb (reps) | Handgrip (kg) | Balance (No of Contacts) | Flexibility (cm) | Sit-Ups (reps) | Arms Strength-Endurance (s) | |
|---|---|---|---|---|---|---|---|
| T | Before | 26.7± 9.91 | 17.1 ± 5.42 | 13.7 ± 2.00 | 11.0 ± 9.09 | 13.4 ± 2.90 | 2.79 ± 2.89 |
| After | 26.6 ± 9.18 | 22.3 ± 5.63 * | 10.6 ± 8.39 | 12.9 ± 8.39 | 16.3 ± 2.89 * | 5.77 ± 2.57 * | |
| C | Before | 29.0 ± 8.08 | 16.5 ± 3.54 | 14.8 ± 2.95 | 10.9 ± 6.12 | 14.0 ± 2.63 | 3.20 ± 3.06 |
| After | 28.8 ± 8.49 | 16.8 ± 4.41 | 14.0 ± 3.28 | 11.7 ± 8.51 | 14.2 ± 2.62 | 3.60 ± 2.40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naczk, A.; Gajewska, E.; Naczk, M. Effectiveness of Swimming Program in Adolescents with Down Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 7441. https://doi.org/10.3390/ijerph18147441
Naczk A, Gajewska E, Naczk M. Effectiveness of Swimming Program in Adolescents with Down Syndrome. International Journal of Environmental Research and Public Health. 2021; 18(14):7441. https://doi.org/10.3390/ijerph18147441
Chicago/Turabian StyleNaczk, Alicja, Ewa Gajewska, and Mariusz Naczk. 2021. "Effectiveness of Swimming Program in Adolescents with Down Syndrome" International Journal of Environmental Research and Public Health 18, no. 14: 7441. https://doi.org/10.3390/ijerph18147441
APA StyleNaczk, A., Gajewska, E., & Naczk, M. (2021). Effectiveness of Swimming Program in Adolescents with Down Syndrome. International Journal of Environmental Research and Public Health, 18(14), 7441. https://doi.org/10.3390/ijerph18147441