
States Transitions Inference of Postpartum Depression Based on Multi-State Markov Model

Abstract
:1. Introduction
2. Materials and Methods
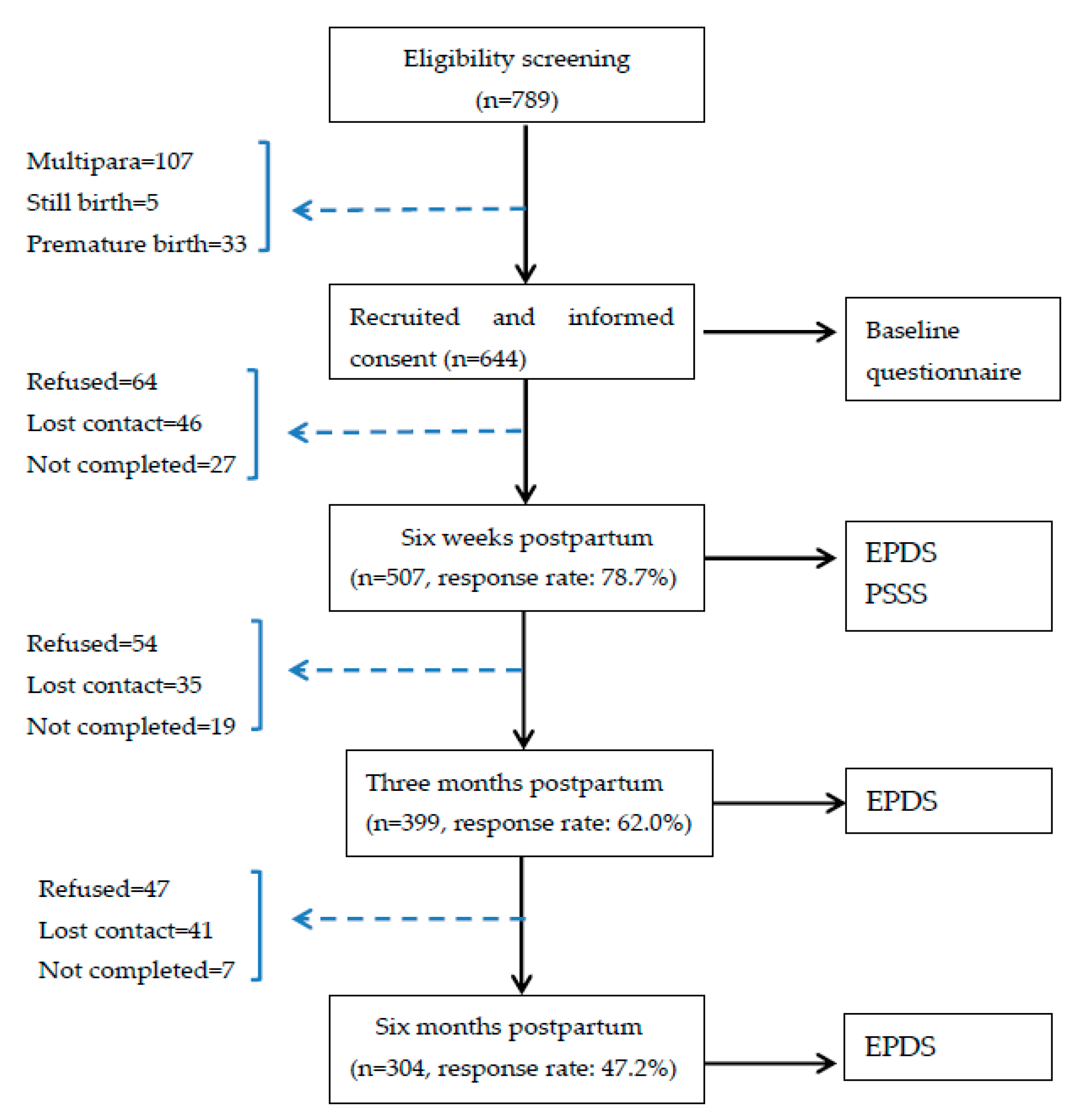
2.1. Study Design and Participants
2.2. Measurements
2.3. Data Collection Procedure
2.4. Data Analysis
3. Results
3.1. Social-Demographic and Clinical Characteristics of the Participants
3.2. Observed Numbers of PPD Status Transitions from One Visit to the Next Visit
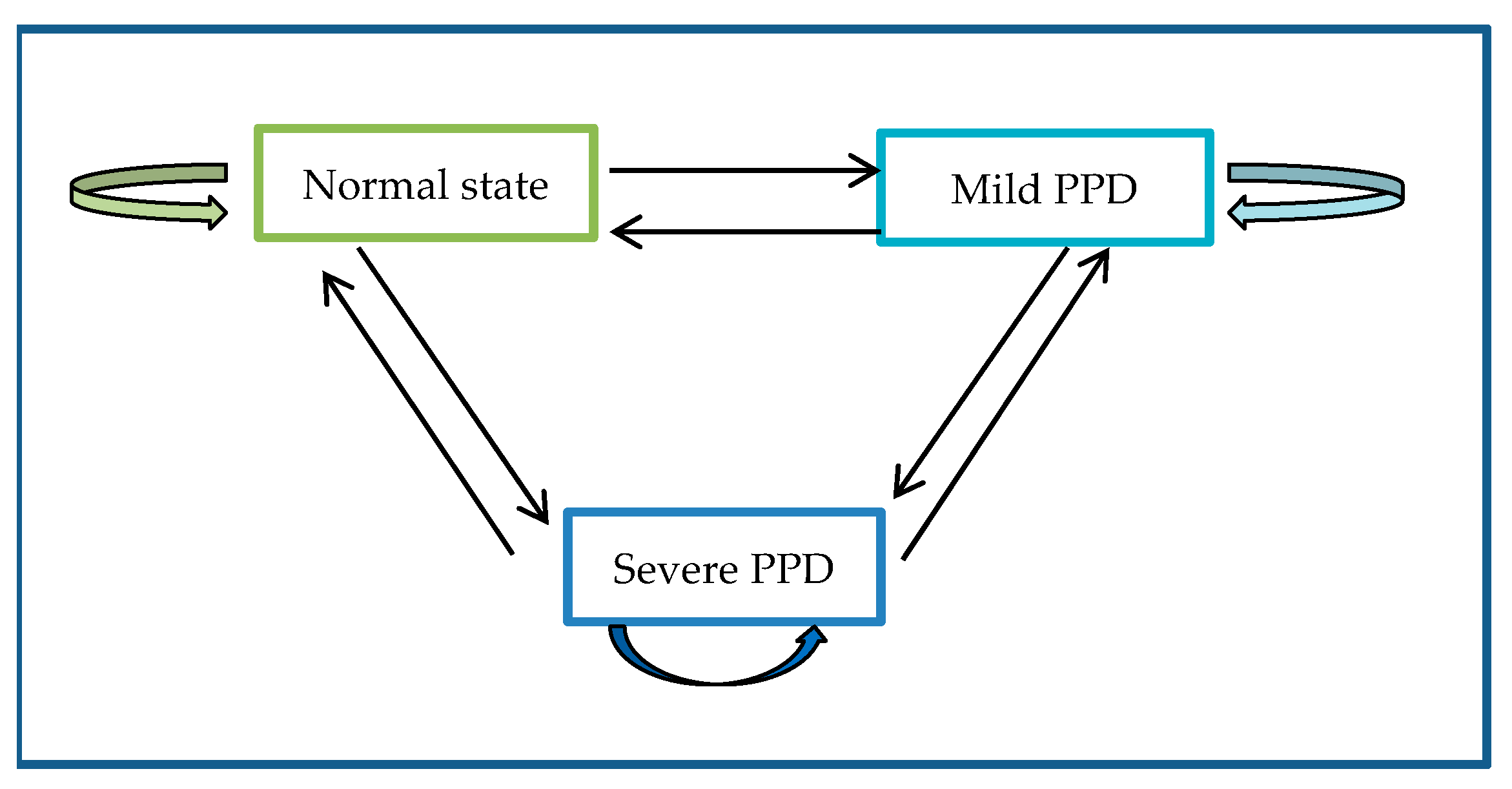
3.3. PPD State Transition Probabilities
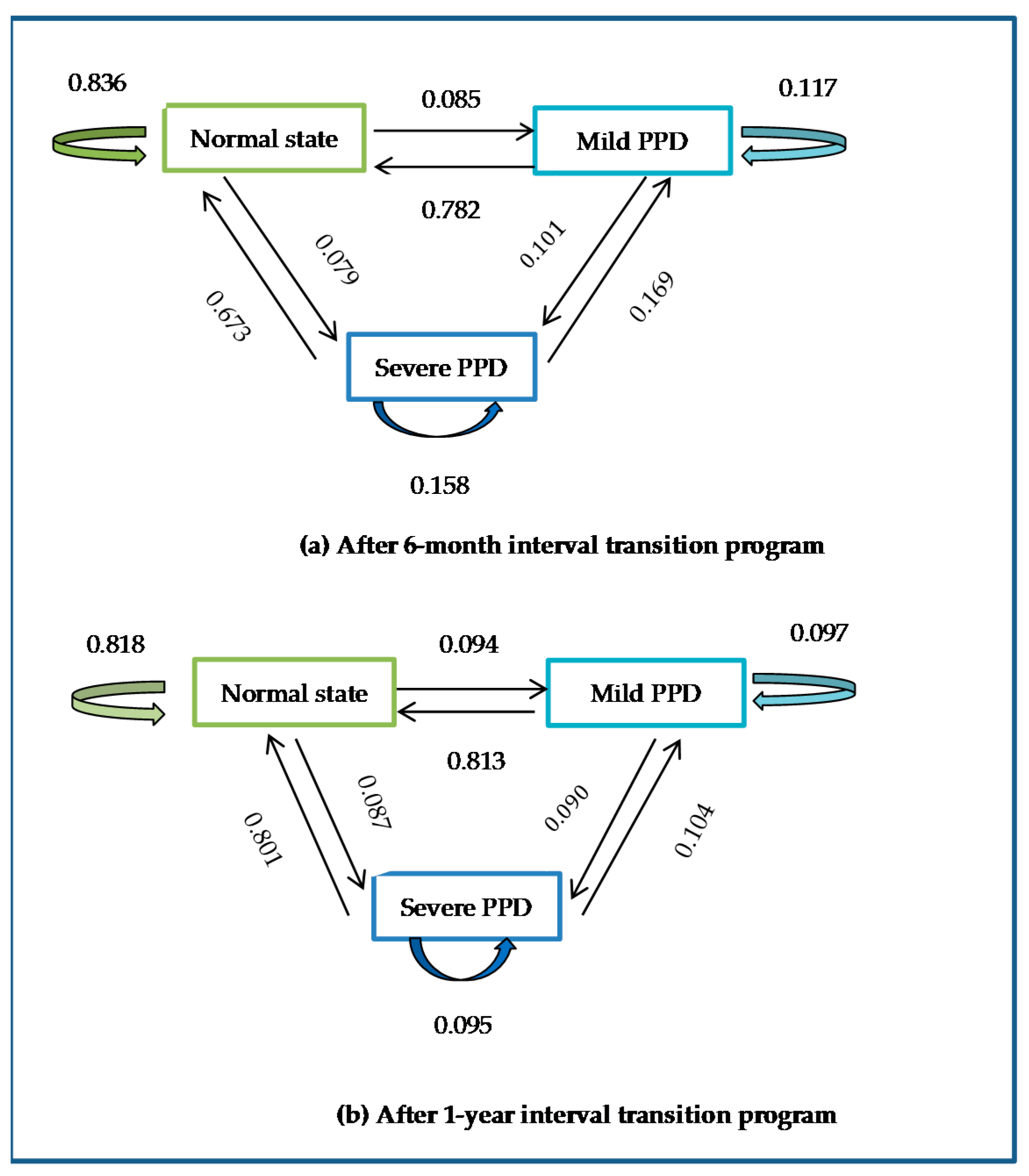
3.4. Model-Estimated Transition Probabilities over a Given Follow-Up Interval
3.5. Covariate Effects and Patient-Specific Risks
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cox, J.L.; Murray, D.; Chapman, G. A Controlled Study of the Onset, Duration and Prevalence of Postnatal Depression. Br. J. Psychiatry 1993, 163, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Craig, M.; Howar, L. Postnatal depression. Clin. Evid. 2009, 1, 1407. [Google Scholar]
- Radzi, W.M.; Jenatabadi, H.S.; Samsudin, N. Postpartum depression symptoms in survey-based research: A structural equation analysis. BMC Public Health 2021, 21, 27. [Google Scholar]
- El-Gilany, A.H.; Elkhawaga, G.O.; Sarraf, B.B. Depression and its associated factors among elderly: A community-based study in Egypt. Arch. Gerontol. Geriatr. 2018, 77, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Pope, Z.; Lee, J.; Gao, Z. Virtual reality exercise for anxiety and depression: A preliminary review of current re-search in an emerging field. J. Clin. Med. 2018, 7, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daley, A.; Jolly, K.; MacArthur, C. The effectiveness of exercise in the management of post-natal depression: Systematic re-view and meta-analysis. Fam. Prac. 2009, 26, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Zejnullahu, V.A.; Ukella-Lleshi, D.; Zejnullahu, V.A.; Miftari, E.; Govori, V. Prevalence of postpartum depression at the clinic for obstetrics and gynecology in Kosovo teaching hospital: Demographic, obstetric and psychosocial risk factors. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Goweda, R.; Metwally, T. Prevalence and associated risk factors of postpartum depression: A cross sectional study. Arch. Clin. Psychiatry 2020, 47, 106–109. [Google Scholar] [CrossRef]
- Zheng, X.; Morrell, J.; Watts, K. Changes in maternal self-efficacy, postnatal depression symptoms and social support among Chinese primiparous women during the initial postpartum period: A longitudinal study. Midwifery 2018, 62, 151–160. [Google Scholar] [CrossRef] [Green Version]
- Gavin, I.N.; Gaynes, N.B.; Lohr, N.K.; Meltzer-Brody, N.S.; Gartlehner, N.G.; Swinson, N.T. Perinatal depression a systematic review of prevalence and incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef]
- Dadi, A.F.; Miller, E.R.; Mwanri, L. Postnatal depression and its association with adverse infant health outcomes in low- and middle-income countries: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2020, 20, 1–15. [Google Scholar] [CrossRef]
- Chew-Graham, C.; Sharp, D.; Chamberlain, E.; Folkes, L.; Turner, K.M. Disclosure of symptoms of postnatal depression, the perspectives of health professionals and women: A qualitative study. BMC Fam. Prac. 2009, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Oates, M.R.; Cox, J.L.; Neema, S.; Asten, P.; Glangeaud-Freudenthal, N.; Figueiredo, B.; Gorman, L.L.; Hacking, S.; Hirst, E.; Kammerer, M.; et al. Postnatal depression across countries and cultures: A qualitative study. Br. J. Psychiatry 2004, 184, s10–s16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peñacoba Puente, C.; Suso-Ribera, C.; Blanco Rico, S.; Marín, D.; San Román Montero, J.; Catalá, P. Is the association between postpartum depression and early maternal–infant relationships contextually determined by avoidant coping in the Mother? Int. J. Environ. Res. Public Health 2021, 18, 562. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Morrell, J.; Watts, K. A quantitative longitudinal study to explore factors which influence maternal self-efficacy among Chinese primiparous women during the initial postpartum period. Midwifery 2018, 59, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Zhang, Y.; Li, X.L.; Ye, Z.W.; Huang, L.L.; Zhang, Y.; Zheng, X.J. Exploring maternal self-efficacy of first-time mothers among rural-to-urban floating women: A quantitative longitudinal study in China. Int. J. Environ. Res. Public Health 2021, 18, 2793. [Google Scholar] [CrossRef] [PubMed]
- Woldeyohannes, D.; Tekalegn, Y.; Sahiledengle, B.; Ermias, D.; Ejajo, T.; Mwanri, L. Effect of postpartum depression on exclusive breast-feeding practices in sub-Saharan Africa countries: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Adewuya, A.O.; Ola, B.O.; Aloba, O.O.; Mapayi, B.M.; Okeniyi, J.A. Impact of postnatal depression on infants’ growth in Nigeria. J. Affect. Disord. 2008, 108, 191–193. [Google Scholar] [CrossRef]
- Dennis, C.-L.; McQueen, K. Does maternal postpartum depressive symptomatology influence infant feeding outcomes? Acta Paediatr. 2007, 96, 590–594. [Google Scholar] [CrossRef]
- Wilkinson, R.B.; Mulcahy, R. Attachment and interpersonal relationships in postnatal depression. J. Reprod. Infant Psychol. 2010, 28, 252–265. [Google Scholar] [CrossRef]
- Shi, X.; Ying, Y.; Yu, Z.; Xing, M.; Zhu, J.; Feng, W.; Xu, D.; Zhang, W.; Zhou, M.; Wang, J.; et al. Risk factors for postpartum depression in Chinese women: A cross-sectional study at 6 weeks postpartum. J. Psychosom. Res. 2021, 140, 110295. [Google Scholar] [CrossRef] [PubMed]
- Ceriani Cernadas, J.M. Postpartum depression: Risks and early detection. Arch. Argent. Pediatr. 2020, 118, 154–155. [Google Scholar]
- Bloch, M.; Daly, R.C.; Rubinow, D.R. Endocrine factors in the etiology of postpartum depression. Compr. Psychiatry 2003, 44, 234–246. [Google Scholar] [CrossRef]
- Brummelte, S.; Galea, L.A. Depression during pregnancy and postpartum: Contribution of stress and ovarian hormones. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2010, 34, 766–776. [Google Scholar] [CrossRef]
- Corwin, E.J.; Kohen, R.; Jarrett, M.; Stafford, B. The heritability of postpartum depression. Biol. Res. Nurs. 2010, 12, 73–83. [Google Scholar] [CrossRef]
- Robertson, E.; Grace, S.; Wallington, T.; Stewart, D.E. Antenatal risk factors for postpartum depression: A synthesis of recent literature. Gen. Hosp. Psychiatry 2004, 26, 289–295. [Google Scholar] [CrossRef]
- Yim, I.S.; Tanner Stapleton, L.R.; Guardino, C.M.; Hahn-Holbrook, J.; Dunkel Schette, C. Biological and psychosocial predictors of postpartum depression: Systematic review and call for integration. Annu. Rev. Clin. Psychol. 2015, 11, 99–137. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Borba, V.; Suso-Ribera, C.; Osma, J.; Andreu-Pejó, L. Predicting Postpartum Depressive Symptoms from Pregnancy Biopsychosocial Factors: A Longitudinal Investigation Using Structural Equation Modeling. Int. J. Environ. Res. Public Health 2020, 17, 8445. [Google Scholar] [CrossRef]
- Yang, J.; Liu, F.; Wang, B.; Chen, C.; Church, T.; Dukes, L.; Smith, J.O. Blood Pressure States Transition Inference Based on MultiState Markov Model. IEEE J. Biomed. Health Inform. 2021, 25, 237–246. [Google Scholar] [CrossRef]
- Wong, L.Y.; Toh, M.P.H.S.; Tham, L.W.C. Projection of prediabetes and diabetes population size in singapore using a dynamicmarkovmodel. J. Diabetes 2017, 9, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Grover, G.; Sabharwal, A.; Kumar, S.; Thakur, A.K. A multi-state markov model for the progression of chronic kidney disease. Türkiye Klin. Biyoistatistik 2019, 11, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Srikanth, P. Using Markov Chains to predict the natural progression of diabetic retinopathy. Int. J. Ophthalmol. 2015, 8, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression: Development of the 10-Item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.; Holden, J. Perinatal Mental Health: A Guide to the Edinburgh Postnatal Depression Scale (EPDS); Gaskell: London, UK, 2003. [Google Scholar]
- Wang, Y.; Guo, X.; Lau, Y.; Chan, K.S.; Yin, L.; Chen, J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh Postnatal Depression Scale. Int. J. Nurs. Stud. 2009, 46, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of indi-vidual participant data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef]
- O’Connor, E.; Rossom, R.C.; Henninger, M.; Groom, H.C.; Burda, B.U. Primary care screening for and treatment of depression in pregnant and postpartum women: Evidence report and systematic review for the US Preventive Services Task Force. JAMA 2016, 315, 388–406. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.; Zheng, X.X. The relationship between social support and postnatal depression of primiparous women. Chin. J. Nurs. 2001, 36, 731–733. (In Chinese) [Google Scholar]
- Hewitt, C.; Gilbody, S.; Brealey, S.; Paulden, M.; Palmer, S.; Mann, R.; Green, J.; Morrell, J.; Barkham, M.; Light, K.; et al. Methods to identify postnatal depression in primary care: An integrated evidence synthesis and value of information analysis. Health Technol. Assess. 2009, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- National Collaborating Centre for Mental Health. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance, Updated ed.; British Psychological Society: Leicester, UK, 2014. [Google Scholar]
- Force, U.P.S.T. Screening for Depression in Adults: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2009, 151, 784–792. [Google Scholar] [CrossRef]
- Austin, M.-P.; Highet, N. Guidelines Expert Advisory Committee. Clinical Practice Guidelines for Depression and Related DisOrders—Anxiety, Bipolar Disorder and Puerperal Psychosis—In the Perinatal Period. In A Guideline for Primary Care Health Professionals; The National Depression Initiative; Beyondblue: Melbourne, Australia, 2013. [Google Scholar]
- National Institute of Child Health and Human Development (NICHD). Postpartum depression may persist three years after giving birth. JAMA 2020, 324, 2475. [Google Scholar]
- General Office of the National Health Commission. Notice of the General Office of the NationalHealth Commission on Exploring the Implementation of Special Services for the Prevention and Treatment of Depression and Senile Dementia. Available online: http://www.nhc.gov.cn/jkj/s7914/202009/a63d8f82eb53451f97217bef0962b98f.shtml (accessed on 3 March 2021).
- Zheng, X.J.; Morrell, J.; Watts, K. An Exploration of Factors which Influence Maternal Self-Efficacy in Primiparous Women in China during the Initial Postnatal Period. Ph.D. Thesis, The University of Nottingham, Nottingham, UK, 2015. [Google Scholar]
- Gong, W.; Jin, X.; Cheng, K.; Caine, E.; Lehman, R.; Xu, D. Chinese women’s acceptance and uptake of referral after screening for perinatal depression. Int. J. Environ. Res. Public Health 2020, 17, 8686. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 304) |
|---|---|
| Age, mean (SD) | 24.8 (2.89) |
| Marital status, n (%) | |
| Married | 304 (100.0%) |
| Divorced | 0 (0.0%) |
| Single | 0 (0.0%) |
| Education, n (%) | |
| Middle school or lower | 78 (25.6%) |
| High school or junior college | 123 (40.5%) |
| University or higher | 103 (33.9%) |
| Occupation, n (%) | |
| Professional | 10 (3.3%) |
| Skilled | 25 (8.2%) |
| Unskilled | 181 (59.5%) |
| Unemployed | 88 (29.0%) |
| Family income (per person, month), n (%) | |
| <3000 yuan (US$420) | 73 (24.0%) |
| 3001—5000 yuan (US$420–700) | 144 (47.4%) |
| >5000 yuan (US$700) | 87 (28.6%) |
| Delivery mode, n (%) | |
| Natural childbirth | 218 (71.7%) |
| Assisted childbirth | 46 (15.1%) |
| C-section | 40 (13.2%) |
| Whether attending parenting train, n (%) | |
| Yes | 157 (51.6%) |
| No | 147(48.4%) |
| Baby gender, n (%) | |
| Boy | 181 (59.5%) |
| Girl | 123 (40.5%) |
| Baby health, mean (SD) | 80.5 (15.49) |
| Baby fussiness, mean (SD) | 69.6 (19.89) |
| Emotional support, mean (SD) | 10.2 (2.72) |
| Material support, mean (SD) | 9.9 (3.43) |
| Informational support, mean (SD) | 6.8 (3.14) |
| Evaluation of support, mean (SD) | 8.4 (2.92) |
| From\To | Normal State n (%) | Mild PPD n (%) | Severe PPD n (%) |
|---|---|---|---|
| T1 Normal state | 155(25.5%) | 9 (1.5%) | 10 (1.6%) |
| T2 Mild PPD | 88 (14.5%) | 33 (5.4%) | 19 (3.1%) |
| T3 Severe PPD | 63 (10.3%) | 92 (15.1%) | 139 (22.9) |
| From\To | Normal PPD | Mild PPD | Severe PPD |
|---|---|---|---|
| Normal state | - | 0.498 | 0.502 |
| Mild PPD | 0.800 | - | 0.200 |
| Severe PPD | 0.064 | 0.936 | - |
| Sojourn Time (weeks) | 64.12 | 6.29 | 9.37 |
| Interval of Follow-Up | State 1 to State 3 Percent (95% CI) | State 2 to State 3 Percent (95% CI) | State 3 to State 1 Percent (95% CI) | State 2 to State 1 Percent (95% CI) |
|---|---|---|---|---|
| 1 month | 0.028 (0.015, 0.059) | 0.085 (0.050, 0.149) | 0.104 (0.086, 0.143) | 0.390 (0.332, 0.445) |
| 3 month | 0.060 (0.036, 0.108) | 0.114 (0.080, 0.171) | 0.407(0.351, 0.473) | 0.680 (0.600, 0.735) |
| 6 month | 0.079 (0.050, 0.144) | 0.101 (0.073, 0.157) | 0.673(0.601, 0.721) | 0.782 (0.700, 0.826) |
| 9 month | 0.085 (0.054, 0.150) | 0.093 (0.063, 0.152) | 0.769 (0.681, 0.818) | 0.806 (0.709, 0.859) |
| 1 year | 0.087 (0.057, 0.161) | 0.090 (0.059, 0.162) | 0.801 (0.694, 0.851) | 0.813 (0.700, 0.866) |
| 2 year | 0.088 (0.054, 0.149) | 0.088 (0.054, 0.149) | 0.816(0.712, 0.873) | 0.816 (0.712, 0.873) |
| 3 year | 0.088 (0.056, 0.147) | 0.088 (0.056, 0.147) | 0.816 (0.718, 0.871) | 0.816 (0.718, 0.871) |
| Worsening Transition | Hazard Ratio (95% CI) |
|---|---|
| State 1 to State 3 | |
| Emotional support | 0.48 (0.33, 0.70) |
| Material support | 0.65 (0.51, 0.82) |
| Informational support | 0.57 (0.42, 0.76) |
| Evaluation of support | 0.42 (0.22, 0.82) |
| Bettering Transition | Hazard Ratio (95% CI) |
|---|---|
| State 3 to State 1 | |
| Informational support | 1.59 (1.15, 2.19) |
| Evaluation of support | 2.27 (1.12, 4.58) |
| Maternal age | 1.46 (1.15, 1.86) |
| State 3 to State 2 | |
| Evaluation of support | 1.14 (1.04, 1.26) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, J.; Fang, Q.; Chen, J.; Li, Y.; Li, H.; Li, W.; Zheng, X. States Transitions Inference of Postpartum Depression Based on Multi-State Markov Model. Int. J. Environ. Res. Public Health 2021, 18, 7449. https://doi.org/10.3390/ijerph18147449
Xiong J, Fang Q, Chen J, Li Y, Li H, Li W, Zheng X. States Transitions Inference of Postpartum Depression Based on Multi-State Markov Model. International Journal of Environmental Research and Public Health. 2021; 18(14):7449. https://doi.org/10.3390/ijerph18147449
Chicago/Turabian StyleXiong, Juan, Qiyu Fang, Jialing Chen, Yingxin Li, Huiyi Li, Wenjie Li, and Xujuan Zheng. 2021. "States Transitions Inference of Postpartum Depression Based on Multi-State Markov Model" International Journal of Environmental Research and Public Health 18, no. 14: 7449. https://doi.org/10.3390/ijerph18147449
APA StyleXiong, J., Fang, Q., Chen, J., Li, Y., Li, H., Li, W., & Zheng, X. (2021). States Transitions Inference of Postpartum Depression Based on Multi-State Markov Model. International Journal of Environmental Research and Public Health, 18(14), 7449. https://doi.org/10.3390/ijerph18147449