
Patient Safety in the Eyes of Aspiring Healthcare Professionals: A Systematic Review of Their Attitudes

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search and Selection of Studies
2.2. Risk of Bias Assessment of the Included Studies
2.3. Data Extraction and Synthesis
- Tabular description of the included studies, presented as supplementary material;
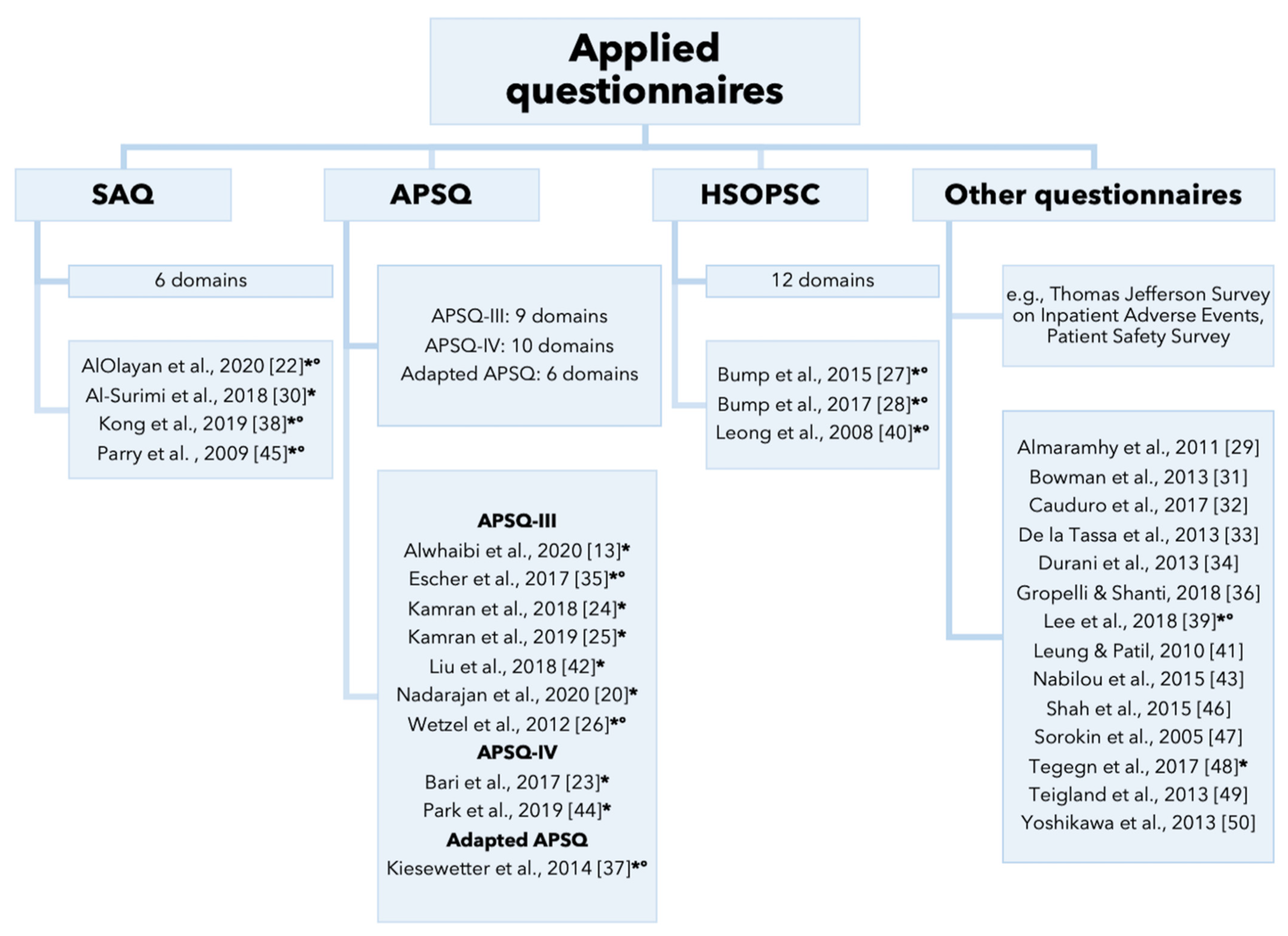
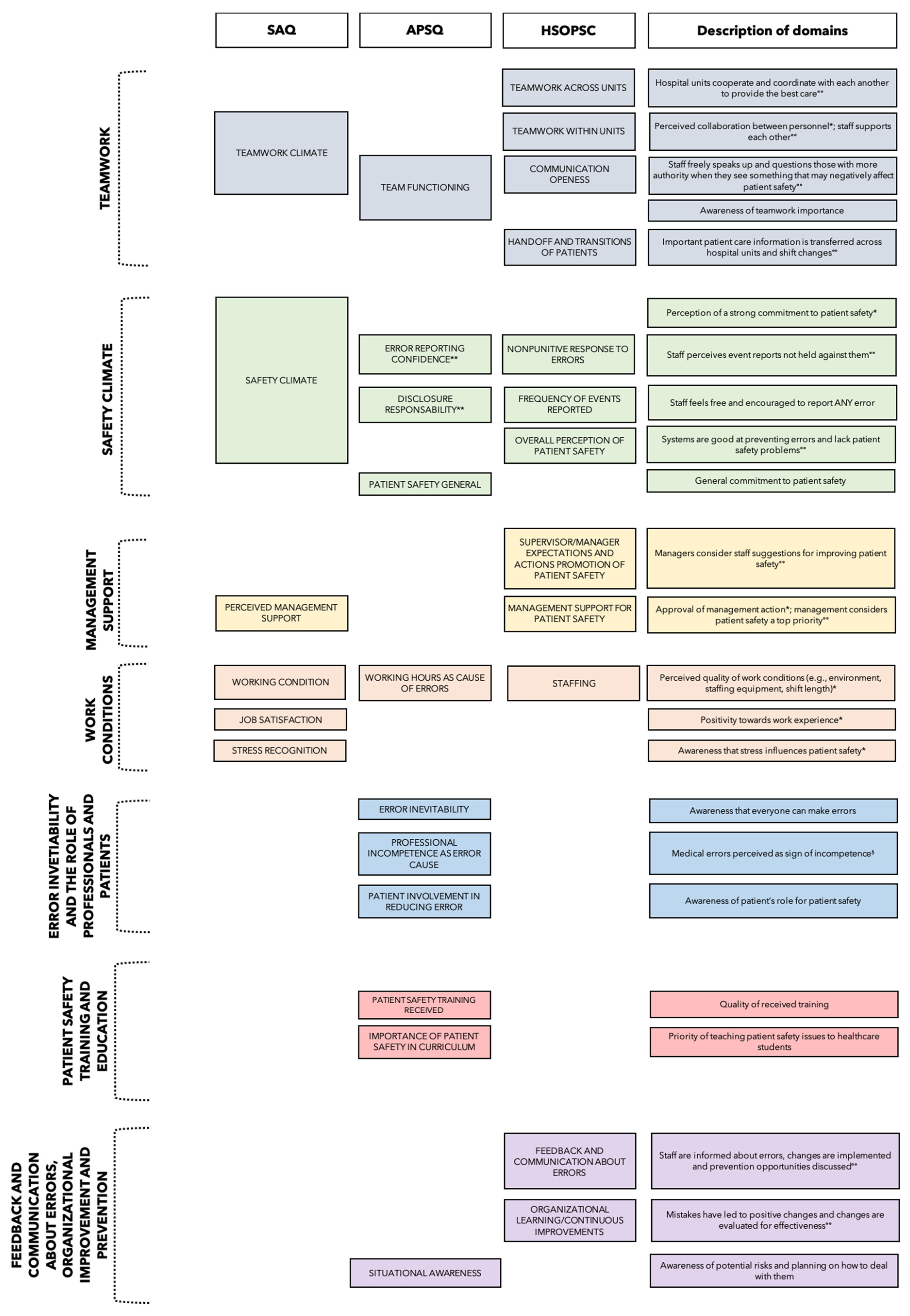
- Synthesis of students and young healthcare professionals’ attitudes assessed by (1) the Safety Attitudes Questionnaires (SAQ), (2) the Attitudes to Patient Safety Questionnaire (APSQ), (3) Hospital Survey on Patient Safety Culture (HSOPSC) by the Agency for Healthcare Research and Quality (AHRQ), (4) other questionnaires, structured around areas with regard to awareness/perception of patient safety culture, presented as figure, narrative text, and supplementary material;
- Synthesis of reported differences (1) across years of study, (2) across specialties, (3) between genders, presented as table and narrative text;
- When synthesizing the data, we followed some specific guidelines:
- For articles using the SAQ, APSQ, or HSOPSC, if only the mean item scores were given, we calculated the mean domain scores with Excel, taking into account reverse scored items. The same procedure was applied for percentages of positive answers.
- For the articles applying the APSQ, we did not compare the reported mean scores of the domains across but only within studies since different types of Likert scales (e.g., 5 or 7 points) were used across studies. Based on the indications in the literature [23,24,25,26], responses to individual items rated with 7-point Likert scales were considered as a positive/desired attitude if the response was “strongly agree”, “agree” or “somewhat agree” in positively worded questions and “strongly disagree”, “disagree” and “somewhat disagree” in negatively worded questions and mean scores of 5-point Likert scales were considered as a positive/desired response if the response was “strongly agree” or “agree” in positively worded questions and “strongly disagree” or “disagree” in negatively worded questions. Consequently, mean scores of domains assessed by a 7-point Likert scale reflect a more positive/desired attitude if >4, while mean scores measured by a 5-point Likert scale point to a more positive/desired attitude if >3.
3. Results
3.1. Risk of Bias Assessment of the Included Studies
3.2. Characteristics of the Included Studies
3.3. Overall Attitudes of Students and Young Health Professionals
3.3.1. Teamwork
3.3.2. Safety Climate
3.3.3. Management Support
3.3.4. Work Conditions
3.3.5. Error Inevitability and the Role of Professionals and Patients
3.3.6. Patient Safety Training and Education
3.3.7. Feedback and Communication about Errors, Organizational Improvement, and Prevention
3.3.8. Differences in Patient Safety Attitudes between Subgroups
3.3.9. Differences across Years of Study
3.3.10. Differences between Genders
3.3.11. Differences across Specialties
4. Discussion
4.1. Recommendations for Medical Education and Clinical Practice
4.2. Limitations of Our Study
4.3. Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Makary, M.A.; Daniel, M. Medical error-the third leading cause of death in the US. BMJ 2016, 353, i2139. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe. Data and Statistics. Available online: https://www.euro.who.int/en/health-topics/Health-systems/patient-safety/data-and-statistics#:~:text=European%20data%2C%20mostly%20from%20European,%25%20to%2012%25%20of%20hospitalizations (accessed on 26 March 2021).
- Institute of Medicine (US) Committee on Quality of Health Care in America. Errors in Health Care: A Leading Cause of Death and Injury. In To Err Is Human: Building a Safer Health System; Kohn, L.T., Corrigan, J.M., Donaldson, M.S., Eds.; The National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Busch, I.M.; Moretti, F.; Purgato, M.; Barbui, C.; Wu, A.W.; Rimondini, M. Psychological and Psychosomatic Symptoms of Second Victims of Adverse Events: A Systematic Review and Meta-Analysis. J. Patient. Saf. 2020, 16, e61–e74. [Google Scholar] [CrossRef]
- Busch, I.M.; Saxena, A.; Wu, A.W. Putting the Patient in Patient Safety Investigations: Barriers and Strategies for Involvement. J. Patient. Saf. 2020. [Google Scholar] [CrossRef]
- Busch, I.M.; Moretti, F.; Purgato, M.; Barbui, C.; Wu, A.W.; Rimondini, M. Dealing with Adverse Events: A Meta-analysis on Second Victims’ Coping Strategies. J. Patient. Saf. 2020, 16, e51–e60. [Google Scholar] [CrossRef]
- Rodziewicz, T.L.; Houseman, B.; Hipskind, J.E. Medical Error Reduction and Prevention; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Sammer, C.E.; Lykens, K.; Singh, K.P.; Mains, D.A.; Lackan, N.A. What is patient safety culture? A review of the literature. J. Nurs. Scholarsh. 2010, 42, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.J.; Lubomksi, L.H.; Wilson, R.F.; Pfoh, E.R.; Martinez, K.A.; Dy, S.M. Promoting a culture of safety as a patient safety strategy: A systematic review. Ann. Intern. Med. 2013, 158, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Scott, L.D.; Dahinten, V.S.; Vincent, C.; Lopez, K.D.; Park, C.G. Safety Culture, Patient Safety, and Quality of Care Outcomes: A Literature Review. West. J. Nurs. Res. 2019, 41, 279–304. [Google Scholar] [CrossRef]
- López-Hernández, L.B.; Díaz, B.G.; González, E.O.Z.; Montes-Hernández, K.I.; Díaz, S.S.T.; Toledo-Lozano, C.G.; Bustamante-Montes, L.P.; Vázquez-Cárdenas, N.A. Quality and Safety in Healthcare for Medical Students: Challenges and the Road Ahead. Healthcare 2020, 8, 540. [Google Scholar] [CrossRef]
- Wu, A.W.; Busch, I.M. Patient safety: A new basic science for professional education. GMS J. Med. Educ. 2019, 36, Doc21. [Google Scholar] [CrossRef] [PubMed]
- Alwhaibi, M.; AlRuthia, Y.; Almalag, H.; Alkofide, H.; Balkhi, B.; Almejel, A.; Alshammari, F. Pharmacy students’ attitudes toward patient safety in Saudi Arabia: A cross-sectional study. BMC Med. Educ. 2020, 20, 275. [Google Scholar] [CrossRef]
- Auzoult, L.; Ngueutsa, R. Attitude to safety rules and reflexivity as determinants of safety climate. J. Saf. Res. 2019, 71, 95–102. [Google Scholar] [CrossRef]
- Walton, M.; Woodward, H.; Van Staalduinen, S.; Lemer, C.; Greaves, F.; Noble, D.; Ellis, B.; Donaldson, L.; Barraclough, B. Expert Group convened by the World Alliance of Patient Safety, as Expert Lead for the Sub-Programme. The WHO patient safety curriculum guide for medical schools. Qual. Saf. Health Care 2010, 19, 542–546. [Google Scholar]
- World Health Organization. WHO Patient Safety Curriculum Guide for Medical Schools; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan Nha, H.; Pierre, P.; Sergi, F.; Gillian, B.; Felicity, B.; Margaret, C.; Pierre, D.; Marie-Pierre, G.; Frances, G.; Belinda, N.; et al. Mixed Method Appraisal Tool (MMAT) Version 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 8 January 2021).
- Nadarajan, S.P.; Karuthan, S.R.; Rajasingam, J.; Chinna, K. Attitudes toward Patient Safety among Medical Students in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 7721. [Google Scholar] [CrossRef] [PubMed]
- Norden-Hägg, A.; Sextion, J.B.; Kälvemark-Sporrong, S.; Ring, L.; Kettis-Lindblad, Å. Assessing safety culture in pharmacies: The psychometric validation of the Safety Attitudes Questionnaire (SAQ) in a national sample of community pharmacies in Sweden. BMC Clin. Pharmacol. 2010, 10, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlOlayan, R.; Alahmad, A.; Buali, D.; Alonaizan, F.; Alhareky, M.; Alhumaid, J.; Nazir, M.A. Patient safety culture amongst dental students and interns in Dammam, Saudi Arabia. Eur. J. Dent. Educ. 2020, 25, 175–182. [Google Scholar] [CrossRef]
- Bari, A.; Jabeen, U.; Bano, I.; Rathore, A.W. Patient safety awareness among postgraduate students and nurses in a tertiary health care facility. Pak. J. Med. Sci. 2017, 33, 1059–1064. [Google Scholar] [CrossRef]
- Kamran, R.; Bari, A.; Khan, R.A.; Al-Eraky, M. Patient safety awareness among Undergraduate Medical Students in Pakistani Medical School. Pak. J. Med. Sci. 2018, 34, 305–309. [Google Scholar] [CrossRef]
- Kamran, R.; Bari, A.; Uddin, R.; Tauseef, A.; Ijaz, F.; Yasser, F.; Aftab, R.K. Patient Safety Awareness among Future Health Professionals in a Pakistani Medical College of Military Set-up. Int. J. Med. Res. Health Sci. 2019, 8, 118–123. [Google Scholar]
- Wetzel, A.P.; Dow, A.W.; Mazmanian, P.E. Patient safety attitudes and behaviors of graduating medical students. Eval. Health Prof. 2012, 35, 221–238. [Google Scholar] [CrossRef] [PubMed]
- Bump, G.M.; Calabria, J.; Gosman, G.; Eckart, C.; Metro, D.G.; Jasti, H.; McCausland, J.B.; Itri, J.N.; Patel, R.M.; Buchert, A. Evaluating the Clinical Learning Environment: Resident and Fellow Perceptions of Patient Safety Culture. J. Grad. Med. Educ. 2015, 7, 109–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bump, G.M.; Coots, N.; Liberi, C.A.; Minnier, T.E.; Phrampus, P.E.; Gosman, G.; Metro, D.G.; McCausland, J.B.; Buchert, A. Comparing Trainee and Staff Perceptions of Patient Safety Culture. Acad. Med. 2017, 92, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Almaramhy, H.; Al-Shobaili, H.; El-Hadary, K.; Dandash, K. Knowledge and attitude towards patient safety among a group of undergraduate medical students in saudi arabia. Int. J. Health Sci. 2011, 5, 59–67. [Google Scholar]
- Al-Surimi, K.; AlAyadi, H.; Salam, M. Female dental students’ perceptions of patient safety culture: A cross sectional study at a middle eastern setting. BMC Med. Educ. 2018, 18, 301. [Google Scholar] [CrossRef] [Green Version]
- Bowman, C.; Neeman, N.; Sehgal, N.L. Enculturation of unsafe attitudes and behaviors: Student perceptions of safety culture. Acad. Med. 2013, 88, 802–810. [Google Scholar] [CrossRef] [Green Version]
- Cauduro, G.M.R.; Magnago, T.S.B.S.; Andolhe, R.; Lanes, T.C.; Ongaro, J.D. Patient safety in the understanding of health care students. Rev. Gaucha. Enferm. 2017, 38, e64818. [Google Scholar]
- De la Tassa, J.M.; Martin, D.G.; Fernandez, E.L.; Castro, M.J.G.; Sanchez, G.S. Survey on the Culture of Patient Safety Among Spanish Health Care Residents. Am. J. Med. Qual. 2013, 28, 434–442. [Google Scholar] [CrossRef]
- Durani, P.; Dias, J.; Singh, H.P.; Taub, N. Junior doctors and patient safety: Evaluating knowledge, attitudes and perception of safety climate. BMJ Qual. Saf. 2013, 22, 65–71. [Google Scholar] [CrossRef]
- Escher, C.; Creuztfeldt, J.; Meurling, L.; Hedman, L.; Kjellin, A.; Felländer-Tsai, L. Medical students’ situational motivation to participate in simulation based team training is predicted by attitudes to patient safety. BMC Med. Educ. 2017, 17, 37. [Google Scholar] [CrossRef] [Green Version]
- Gropelli, T.; Shanty, J.A. Nursing Students’ Perceptions of Safety and Communication Issues in the Clinical Setting. J. Nurs. Educ. 2018, 57, 287–290. [Google Scholar] [CrossRef]
- Kiesewetter, J.; Kager, M.; Lux, R.; Zwissler, B.; Fischer, M.R.; Dietz, I. German undergraduate medical students’ attitudes and needs regarding medical errors and patient safety-a national survey in Germany. Med. Teach. 2014, 36, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.N.; Zhu, W.F.; He, S.; Chen, S.Z.; Yang, L.; Qi, L.; Peng, X. Attitudes towards patient safety culture among postgraduate nursing students in China: A cross-sectional study. Nurse Educ. Pract. 2019, 38, 1–6. [Google Scholar] [CrossRef]
- Lee, H.Y.; Hahm, M.I.; Lee, S.G. Undergraduate medical students’ perceptions and intentions regarding patient safety during clinical clerkship. BMC Med. Educ. 2018, 18, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leong, P.; Afrow, J.; Weber, H.P.; Howell, H. Attitudes toward patient safety standards in U.S. dental schools: A pilot study. J. Dent. Educ. 2008, 72, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.K.K.; Patil, N.G. Patient safety in the undergraduate curriculum: Medical students’ perception. Hong Kong Med. J. 2010, 16, 101–105. [Google Scholar] [PubMed]
- Liu, H.; Li, Y.; Zhao, S.; Jiao, M.; Lu, Y.; Liu, J.; Jiang, K.; Fang, H.; Sun, P.; Li, P.; et al. Perceptions of patient safety culture among medical students: A cross-sectional investigation in Heilongjiang Province, China. BMJ Open 2018, 8, e020200. [Google Scholar] [CrossRef]
- Nabilou, B.; Feizi, A.; Seyedin, H. Patient Safety in Medical Education: Students’ Perceptions, Knowledge and Attitudes. PLoS ONE 2015, 10, e0135610. [Google Scholar] [CrossRef]
- Park, K.H.; Park, K.H.; Kang, Y.; Kwon, O.Y. The attitudes of Korean medical students toward patient safety. Korean J. Med. Educ. 2019, 31, 363–369. [Google Scholar] [CrossRef]
- Parry, G.; Horowitz, L.; Goldmann, D. Patient safety attitudes of paediatric trainee physicians. Qual. Saf. Health Care 2009, 18, 462–466. [Google Scholar] [CrossRef]
- Shah, N.; Jawaid, M.; Shah, N.; Ali, S.M. Patient safety: Perceptions of Medical Students of Dow Medical College, Karachi. J. Pak. Med. Assoc. 2015, 65, 1261–1265. [Google Scholar]
- Sorokin, R.; Riggio, J.M.; Hwang, C. Attitudes about patient safety: A survey of physicians-in-training. Am. J. Med. Qual. 2005, 20, 70–77. [Google Scholar] [CrossRef]
- Tegegn, H.G.; Abebe, T.B.; Ayalew, M.B.; Bhagavathula, A.S. Patient safety attitudes of pharmacy students in an Ethiopian university: A cross-sectional study. Drug. Health Pat. Saf. 2017, 9, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Teigland, C.L.; Blasiak, R.C.; Wilson, L.A.; Hines, R.E.; Meyerhoff, K.L.; Viera, A.J. Patient safety and quality improvement education: A cross-sectional study of medical students’ preferences and attitudes. BMC Med. Educ. 2013, 13, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshikawa, J.M.; de Sousa, B.E.C.; Peterlini, M.A.S.; Kusahara, D.M.; Pedreira, M.D.G.; Avelar, A.F.M. Comprehension of undergraduate students in nursing and medicine on patient safety. Acta Paul. Enferm. 2013, 26, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Sexton, J.B.; Helmreich, R.L.; Neilands, T.B.; Rowan, K.; Vella, K.; Boyden, J.; Roberts, P.R.; Thomas, E.J. The Safety Attitudes Questionnaire: Psychometric properties, benchmarking data, and emerging research. BMC Health Serv. Res. 2006, 6, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorra, J.; Gray, L.; Streagle, S.; Famolaro, T.; Yount, N.; Behm, J. AHRQ Hospital Survey on Patient Safety Culture: User’s Guide. (Prepared by Westat, under Contract No. HHSA290201300003C); AHRQ Publication No. 15-0049-EF (Replaces 04-0041); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2016.
- Rosen, M.A.; DiazGranados, D.; Dietz, A.S.; Benishek, L.E.; Thompson, D.; Pronovost, P.J.; Weaver, S.J. Teamwork in healthcare: Key discoveries enabling safer, high-quality care. Am. Psychol. 2018, 73, 433–450. [Google Scholar] [CrossRef]
- Gaufberg, E.H.; Batalden, M.; Sands, R.; Bell, S.K. The hidden curriculum: What can we learn from third-year medical student narrative reflections? Acad. Med. 2010, 85, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Royal College; Patient Safety Institute Canada. Available online: https://www.patientsafetyinstitute.ca/en/toolsResources/Patient-Safety-and-the-Hidden-Curriculum/Documents/Patient%20Safety%20and%20the%20Hidden%20Curriculum.pdf (accessed on 19 May 2021).
- Kang, S.; Ho, T.T.T.; Lee, N.J. Comparative Studies on Patient Safety Culture to Strengthen Health Systems among Southeast Asian Countries. Front. Public Health 2021, 8, 600216. [Google Scholar] [CrossRef]
- Wagner, C.; Smits, M.; Sorra, J.; Huang, C.C. Assessing patient safety culture in hospitals across countries. IJQHC 2013, 25, 213–221. [Google Scholar] [CrossRef]
- Rajput, V.; Mookerjee, A.; Cagande, C. The Contemporary Hidden Curriculum in Medical Education. MedEdPublish 2017. [Google Scholar] [CrossRef] [Green Version]
- Fischer, M.A.; Mazor, K.M.; Baril, J.; Alper, E.; DeMarco, D.; Pugnaire, M. Learning from mistakes. Factors that influence how students and residents learn from medical errors. J. Gen. Intern. Med. 2006, 21, 419–423. [Google Scholar] [CrossRef]
- Lawton, R.; Parker, D. Barriers to incident reporting in a healthcare system. Qual. Saf. Health Care 2002, 11, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, T.H.; Waterman, A.D.; Garbutt, J.M.; Kapp, J.M.; Chan, D.K.; Dunagan, W.C.; Fraser, V.J.; Levinson, W. US and Canadian physicians’ attitudes and experiences regarding disclosing errors to patients. Arch. Intern. Med. 2006, 166, 1605–1611. [Google Scholar] [CrossRef] [Green Version]
- White, A.A.; Gallagher, T.H. Medical error and disclosure. Handb. Clin. Neurol. 2013, 118, 107–117. [Google Scholar]
- Leone, D.; Lamiani, G.; Vegni, E.; Larson, S.; Roter, D.L. Error disclosure and family members’ reactions: Does the type of error really matter? Patient. Educ. Couns. 2015, 98, 446–452. [Google Scholar] [CrossRef]
- Benn, J.; Koutantji, M.; Wallace, L.; Spurgeon, P.; Rejman, M.; Healey, A.; Vincent, C. Feedback from incident reporting: Information and action to improve patient safety. Qual. Saf. Health Care 2009, 18, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Moeller, A.D.; Rasmussen, K.; Nielsen, K.J. Learning and feedback from the Danish patient safety incident reporting system can be improved. Dan. Med. J. 2016, 63, A5242. [Google Scholar]
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsugawa, Y.; Jena, A.B.; Figueroa, J.F.; Orav, E.J.; Blumenthal, D.M.; Jha, A.K. Comparison of Hospital Mortality and Readmission Rates for Medicare Patients Treated by Male vs Female Physicians. JAMA Intern. Med. 2017, 177, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Baumhäkel, M.; Müller, U.; Böhm, M. Influence of gender of physicians and patients on guideline-recommended treatment of chronic heart failure in a cross-sectional study. Eur. J. Heart. Fail. 2009, 11, 299–303. [Google Scholar] [CrossRef]
- Berthold, H.K.; Gouni-Berthold, I.; Bestehorn, K.P.; Böhm, M.; Krone, W. Physician gender is associated with the quality of type 2 diabetes care. J. Intern. Med. 2008, 264, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Roter, D.L.; Hall, J.A.; Aoki, Y. Physician gender effects in medical communication: A meta-analytic review. JAMA 2002, 288, 756–764. [Google Scholar] [CrossRef]
- Roter, D.L.; Hall, J.A. Physician gender and patient-centered communication: A critical review of empirical research. Annu. Rev. Public Health 2004, 25, 497–519. [Google Scholar] [CrossRef]
- Lurie, N.; Slater, J.; McGovern, P.; Ekstrum, J.; Quam, L.; Margolis, K. Preventive care for women. Does the sex of the physician matter? N. Engl. J. Med. 1993, 329, 478–482. [Google Scholar] [CrossRef]
- Franks, P.; Bertakis, K.D. Physician gender, patient gender, and primary care. J. Women’s Health 2003, 12, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Lucian Leape Institute. Unmet Needs: Teaching Physicians to Provide Safe Patient Care; Lucian Leape Institute at the National Patient Safety Foundation: Boston, MA, USA, 2010. [Google Scholar]
- Lochner, L.; Girardi, S.; Pavcovich, A.; Meier, H.; Mantovan, F.; Ausserhofer, D. Applying interprofessional Team-Based Learning in patient safety: A pilot evaluation study. BMC Med. Educ. 2018, 18, 48. [Google Scholar] [CrossRef] [PubMed]
- Peterson-Graziose, V.; Bryer, J. Assessing Student Perceptions of Quality and Safety Education for Nurses Competencies in a Baccalaureate Curriculum. J. Nurs. Educ. 2017, 56, 435–438. [Google Scholar] [CrossRef]
- Berry, J.C.; Davis, J.T.; Bartman, T.; Hafer, C.C.; Lieb, L.M.; Khan, N.; Brilli, R.J. Improved Safety Culture and Teamwork Climate Are Associated With Decreases in Patient Harm and Hospital Mortality Across a Hospital System. J. Patient. Saf. 2020, 16, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.L.; Abreu, L.C.; Ramos, J.L.S.; Castro, C.F.D.; Smiderle, F.R.N.; Santos, J.A.D.; Bezerra, I.M.P. Influence of Burnout on Patient Safety: Systematic Review and Meta-Analysis. Medicina 2019, 55, 553. [Google Scholar] [CrossRef] [Green Version]
- Habibzadeh, H.; Baghaei, R.; Ajoudani, F. Relationship between patient safety culture and job burnout in Iranian nurses: Assessing the mediating role of second victim experience using structural equation modelling. J. Nurs. Manag. 2020, 28, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Busch, I.M.; Moretti, F.; Mazzi, M.; Wu, A.W.; Rimondini, M. What We Have Learned from Two Decades of Epidemics and Pandemics: A Systematic Review and Meta-Analysis of the Psychological Burden of Frontline HealthcareWorkers. Psychother. Psychosom. 2021, 90, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Baumann, N. How to use the medical subject headings (MeSH). Int. J. Clin. Pract. 2016, 70, 171–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| DIFFERENCES ACROSS YEARS OF STUDIES | ||
| Less Advanced Students | More Advanced Students | |
| AlOlayan et al. [22] | SAQ domains Teamwork climate, Safety climate, Perception of management, Work condition (p < 0.01 for all) | |
| Al-Surimi et al. [30] | SAQ domain Teamwork climate (p = 0.001) | |
| Bari et al., 2017 [25] | Positively worded questions on patient safety attitudes (p = 0.006) | |
| De la Tassa et al. [33] | Perception of importance of improvements in techniques and procedures and of involvement in group for patient safety improvement (p < 0.05 for all) | |
| Durani et al. [34] | Individual items “Medical error is a sign of incompetence” (p < 0.001), “It is only important to disclose errors to patients if they have resulted in harm” (p = 0.008) | Individual items “Management is more interested in meeting performance targets than focusing on patient safety issues” (p < 0.001), “My suggestions about patient safety would be acted upon if I expressed them to management” (p < 0.001), “I know the proper channels to direct questions regarding patient safety” (p < 0.001), “The senior managers in my hospital listen to me and care about my patient safety concerns” (p < 0.001), “The senior doctors in my department listen to me and care about my patient safety concerns” (p = 0.002), “I would feel safe here being treated as an inpatient” (p = 0.004) |
| Gropelli and Shanti [36] | Individual items “As a student, I have a safety focus for my patient” (p < 0.020), “My patient has a safety focus for my shift” (p < 0.028), “My clinical instructor focuses on safety issues” (p < 0.039), “Students are informed about errors that happened during the semester” (p < 0.021) | |
| Kiesewetter et al. [37] | APSQ scale Error reporting confidence (p < 0.000) | |
| Liu et al. [42] | APSQ domains Working hours as an error cause and Teamwork (p < 0.05) | APSQ domain Error inevitability (p < 0.05) |
| Nadarajan et al. [20] | APSQ domain Disclosure responsibility (p = 0.002) | APSQ domain Error reporting confidence (p = 0.001), Professional incompetence (p < 0.001) |
| Shah et al. [46] | Individual items “There is no need to report a near miss event” (p = 0.01), “Only physicians can determine the cause of medical errors” (p < 0.001), “Most errors are not related to physicians” (p = 0.04) | |
| Sorokin et al. [47] | Work efficiency (Reduction of adverse events by establishing 80-h workweek) (p = 0.03) Comfort in disclosure discussions (p < 0.01) | |
| DIFFERENCES BETWEEN GENDERS | ||
| Women | Men | |
| AlOlayan et al. [22] | SAQ domain Stress recognition (p = 0.004) | |
| Alwhaibi et al. [13] | APSQ domains Patient safety training received, Error reporting confidence, Working hours as error cause, Error inevitability, Team functioning, Patient involvement in reducing errors (p < 0.05) | APSQ domain Professional incompetence as error (p < 0.05) |
| Escher et al. [35] | APSQ domains Disclosure responsibility (p < 0.001); Team functioning (p = 0.029) | |
| Nadarajan et al. [20] | APSQ domain Professional incompetence as error (p = 0.012) | APSQ domain Error reporting confidence (p = 0.002) |
| Nabilou et al. [40] | Interest in patient safety education (p = 0.001) | |
| DIFFERENCES ACROSS SPECIALTIES | ||
| Dentistry Students | Dental Hygiene Students | |
| Al-Surimi et al. [30] | SAQ domains Teamwork climate, Safety climate, Job satisfaction, Stress recognition, Perceived management support, Working conditions (p < 0.04) | |
| Surgical Students/Trainees | Medical Students/Trainees | |
| Bowman et al. [31] | Teamwork (p < 0.05) | |
| Durani et al. [34] | Individual items “The number of hours doctors work increases the likelihood of making errors” (p = 0.035), “Medical error is a sign of incompetence” (p < 0.00), “Learning about patient safety is not as important as learning other more skill-based aspects of being a doctor” (p < 0.001), “It is only important to disclose errors to patients if they have resulted in harm”, (p < 0.00) | |
| Nursing/Midwifery Students | Medical Students | |
| Nabilou et al. [43] | Interest in patient safety education (p = 0.0017) Attitude towards patient safety (p = 0.001) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tocco Tussardi, I.; Benoni, R.; Moretti, F.; Tardivo, S.; Poli, A.; Wu, A.W.; Rimondini, M.; Busch, I.M. Patient Safety in the Eyes of Aspiring Healthcare Professionals: A Systematic Review of Their Attitudes. Int. J. Environ. Res. Public Health 2021, 18, 7524. https://doi.org/10.3390/ijerph18147524
Tocco Tussardi I, Benoni R, Moretti F, Tardivo S, Poli A, Wu AW, Rimondini M, Busch IM. Patient Safety in the Eyes of Aspiring Healthcare Professionals: A Systematic Review of Their Attitudes. International Journal of Environmental Research and Public Health. 2021; 18(14):7524. https://doi.org/10.3390/ijerph18147524
Chicago/Turabian StyleTocco Tussardi, Ilaria, Roberto Benoni, Francesca Moretti, Stefano Tardivo, Albino Poli, Albert W. Wu, Michela Rimondini, and Isolde Martina Busch. 2021. "Patient Safety in the Eyes of Aspiring Healthcare Professionals: A Systematic Review of Their Attitudes" International Journal of Environmental Research and Public Health 18, no. 14: 7524. https://doi.org/10.3390/ijerph18147524
APA StyleTocco Tussardi, I., Benoni, R., Moretti, F., Tardivo, S., Poli, A., Wu, A. W., Rimondini, M., & Busch, I. M. (2021). Patient Safety in the Eyes of Aspiring Healthcare Professionals: A Systematic Review of Their Attitudes. International Journal of Environmental Research and Public Health, 18(14), 7524. https://doi.org/10.3390/ijerph18147524