
The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes


Abstract
:1. Introduction
2. High-Altitude Physiology
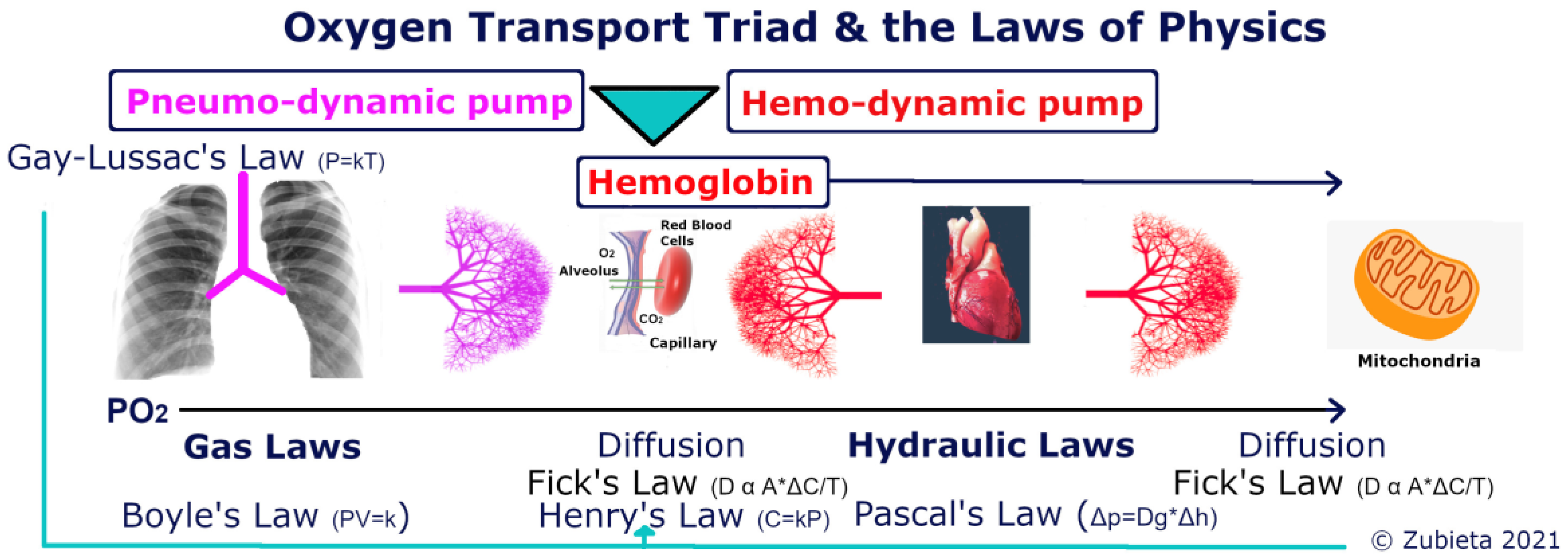
3. The Oxygen Transport Triad
4. The Arterial Oxygen Content (CaO2) at High Altitude
5. The Ferromagnetism of Iron in Hemoglobin and the Paramagnetic Property of Oxygen
6. The High-Altitude Adaptation Formula
7. Acid-Base Balance at High Altitude
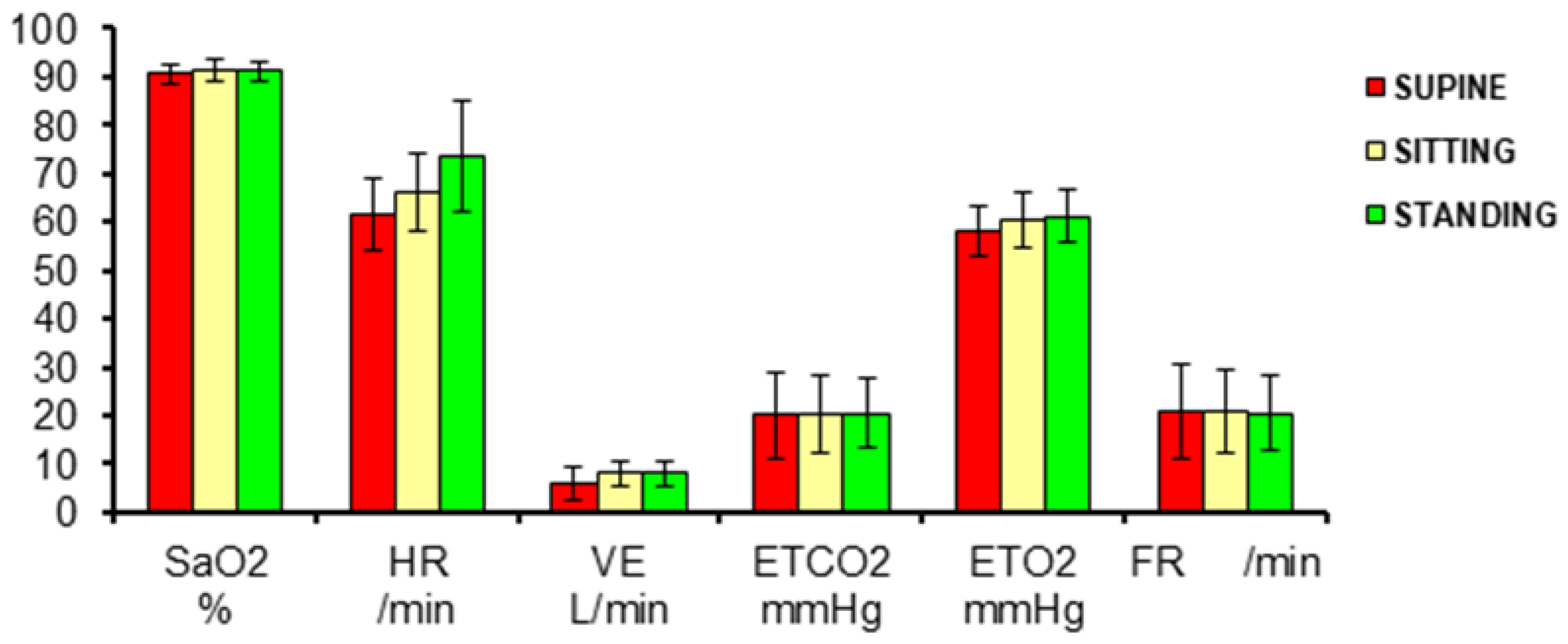
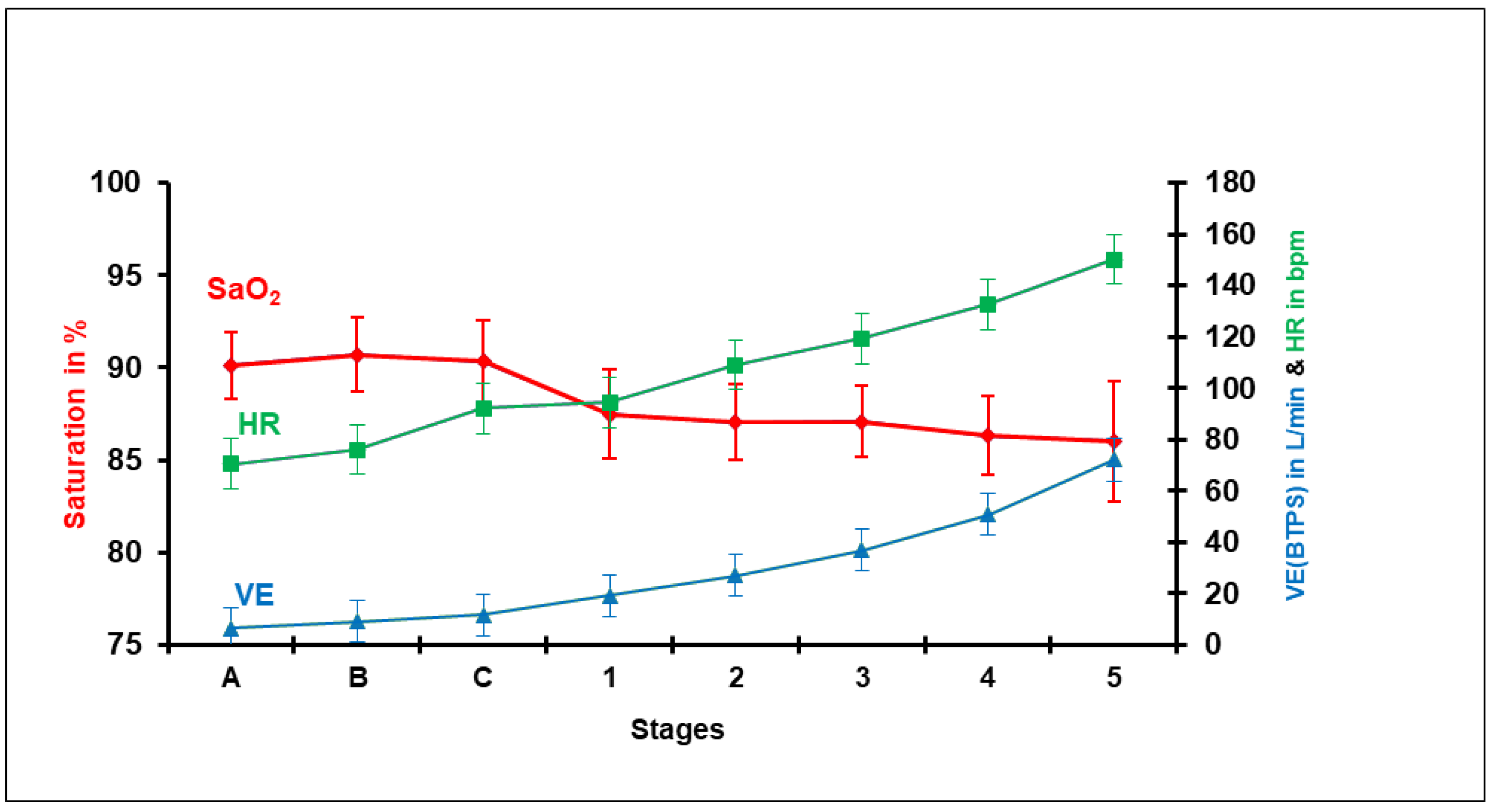
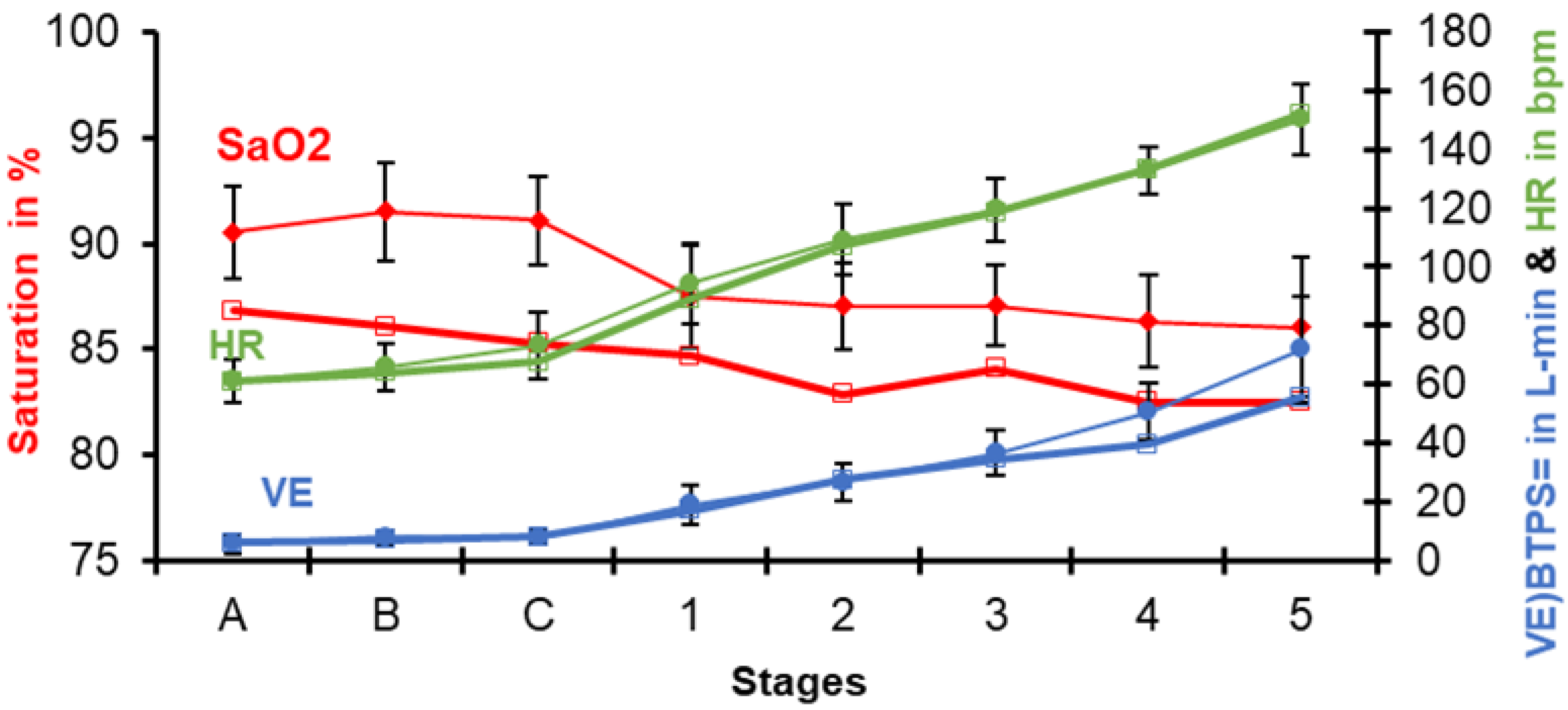
8. Variations of Pulse-Oximetry at High Altitude
9. The Expansion of Gases at High Altitude
10. The Tolerance to Hypoxia Formula
11. The Oxygen Levels in the Summit of Mt. Everest and Fetuses
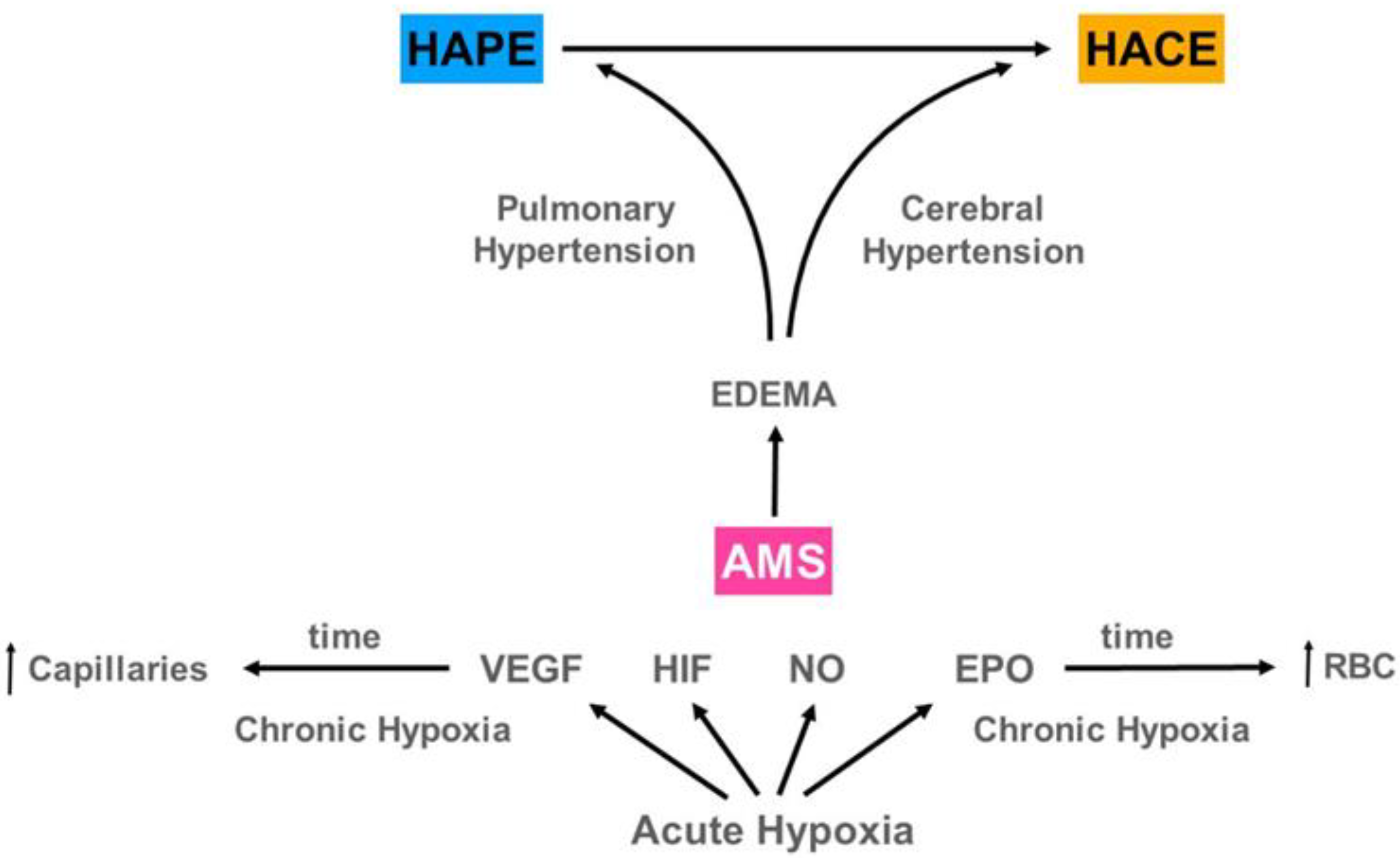
12. AMS Evolving to HAPE and/or HACE
13. Treatment of HAPE and HACE at High Altitude
14. Pulmonary Hypertension and a Dilated Right Ventricle in (HAPE)
15. Benefits of Life under Chronic Hypoxia
16. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Zubieta-Calleja, G.; Zubieta-DeUrioste, N. Acute Mountain Sickness, High Altitude Pulmonary Edema, and High Altitude Cerebral Edema: A view from the High Andes. Respir Physiol. Neurobiol. 2021, 287, 103628. [Google Scholar] [CrossRef]
- Rosenblatt, A.E.; Schmitz, O.J. Interactive effects of multiple climate change variables on trophic interactions: A meta-analysis. Clim Chang. Responses 2014, 1, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Frisancho, A.R. Developmental functional adaptation to high altitude: Review. Am. J. Hum. Biol. 2013, 25, 151–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storz, J.F.; Scott, G.R. Life Ascending: Mechanism and Process in Physiological Adaptation to High-Altitude Hypoxia. Annu. Rev. Ecol. Evol. Syst. 2019, 50, 503–526. [Google Scholar] [CrossRef] [Green Version]
- Blix, A.S. Adaptations to deep and prolonged diving in phocid seals. J. Exp. Biol. 2018, 221, jeb182972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corante, N.; Anza-Ramírez, C.; Figueroa-Mujíca, R.; MacArlupú, J.L.; Vizcardo-Galindo, G.; Bilo, G.; Parati, G.; Gamboa, J.L.; León-Velarde, F.; Villafuerte, F.C. Excessive Erythrocytosis and Cardiovascular Risk in Andean Highlanders. High Alt. Med. Biol. 2018, 19, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villafuerte, F.C.; Corante, N. Chronic Mountain Sickness: Clinical Aspects, Etiology, Management, and Treatment. High Alt. Med. Biol. 2016, 17, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Zubieta-Calleja, G.; Zubieta-Castillo, G.; Zubieta-Calleja, L.; Ardaya-Zubieta, G.; Paulev, P.E. Do over 200 million healthy altitude residents really suffer from chronic acid-base disorders? Indian J. Clin. Biochem. 2011, 26, 62–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zubieta-Calleja, G.; Zubieta-DeUrioste, N. Extended longevity at high altitude: Benefits of exposure to chronic hypoxia. BLDE Uni. J. Health Sci. 2017, 2, 80–90. [Google Scholar] [CrossRef]
- Xing, G.; Qualls, C.; Huicho, L.; River-Ch, M.; Stobdan, T.; Slessarev, M.; Prisman, E.; Ito, S.; Wu, H.; Norboo, A.; et al. Adaptation and mal-adaptation to ambient hypoxia; Andean, Ethiopian and Himalayan patterns. PLoS ONE 2008. [Google Scholar] [CrossRef]
- Maignan, M.; Rivera-Ch, M.; Privat, C.; León-Velarde, F.; Richalet, J.P.; Pham, I. Pulmonary pressure and cardiac function in chronic mountain sickness patients. Chest 2009, 135, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Appenzeller, O.; Minko, T.; Qualls, C.; Pozharov, V.; Gamboa, J.; Gamboa, A.; Pakunlu, R.I. Chronic hypoxia in Andeans are there lessons for neurology at sea level? J. Neurol. Sci. 2006, 247, 93–99. [Google Scholar]
- Richalet, J.P. Adaption to chronic hypoxaemia by populations living at high altitude. In Revue des Maladies Respiratoires; Elsevier Masson s.r.l. Issy-les-Moulineaux: Paris, France, 2021; pp. 395–403. [Google Scholar]
- Gazal, S.; Espinoza, J.R.; Austerlitz, F.; Marchant, D.; Macarlupu, J.L.; Rodriguez, J.; Ju-Preciado, H.; Rivera-Chira, M.; Hermine, O.; Leon-Velarde, F.; et al. The genetic architecture of chronic mountain sickness in Peru. Front Genet. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azad, P.; Stobdan, T.; Zhou, D.; Hartley, I.; Akbari, A.; Bafna, V.; Haddad, G.G. High-altitude adaptation in humans: From genomics to integrative physiology. J. Mol. Med. 2017, 95, 1269–1282. [Google Scholar] [CrossRef]
- Zubieta-Castillo, G.R.; Zubieta-Calleja, G.R.; Zubieta-Calleja, L. Chronic mountain sickness: The reaction of physical disorders to chronic hypoxia. J. Physiol. Pharmacol. 2006, 57, 431–442. [Google Scholar] [PubMed]
- Zubieta-Castillo, G. Forever: Loss of Adaptation Does Not Exist. Available online: http://altitudeclinic.com/blog/2010/07/forever-loss-of-adaptation-does-not-exist/ (accessed on 12 July 2021).
- Zubieta-Castillo, G. Variations in Pulse Oximetry in Natives at High Altitude (3510 m) and After Exposure to Simulated Sea Level. Acta Andin. Available online: https://www.altitudeclinic.com/oxivariations.html (accessed on 12 July 2021).
- Frey, M.A.B.; Tomaselli, C.M.; Hoffler, W.G. Cardiovascular responses to postural changes: Differences with age for women and men. J. Clin. Pharm. 1994, 34, 394–402. [Google Scholar] [CrossRef]
- Zubieta-Calleja, G. Human Adaptation to High Altitude and to Sea Level: Acid-Base equilibrium, ventilation and circulation in chronic hypoxia. J. Appl. Physiol. 1985, 58, 978–988. [Google Scholar]
- Zubieta-Calleja, G.; Zubieta-DeUrioste, N. Space travel in a high altitude environment: Biology by-passing the pressure laws of physics and BioSpaceForming. Rev. Cuba. Investig. Biomed. 2019, 38, 1–14. [Google Scholar]
- Zubieta-Calleja, G.R.; Zubieta-DeUrioste, N. Space travel in a high-altitude environment. One more step in human BioSpace Forming. J. Health Sci. 2018, 3, 97–103. [Google Scholar]
- Naeije, R.; Vanderpool, R. Pulmonary hypertension and chronic mountain sickness. High Alt. Med. Biol. 2013. [Google Scholar] [CrossRef]
- Zubieta-Calleja, G.R.; Zubieta-Castillo, G.; Zubieta-Calleja, L.; Zubieta-Calleja, N. Exercise performance in chronic mountain sickness (C.M.S.). patients at 3510 m. High Alt. Med. Biol. 2002, 3, 114–115. [Google Scholar]
- Zubieta-Calleja, G.R.; Zubieta-DeUrioste, N.; Venkatesh, T.; Das, K.; Soliz, J. COVID-19 and Pneumolysis Simulating Extreme High-altitude Exposure with Altered Oxygen Transport Physiology; Multiple Diseases, and Scarce Need of Ventilators: Andean Condor’s-eye-view. Rev. Recent Clin. Trials 2020, 15, 347–359. [Google Scholar] [CrossRef]
- Schmidt-Nielsen, B. August & Marie Krogh Lives in Science; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Zubieta-Calleja, G.R.; Paulev, P.E.; Zubieta-Calleja, L.; Zubieta-Castillo, G. Altitude adaptation through hematocrit changes. J. Physiol. Pharmacol. 2007, 58, 811–818. [Google Scholar]
- Bren, K.L.; Eisenberg, R.; Gray, H.B. Discovery of the magnetic behavior of hemoglobin: A beginning of bioinorganic chemistry. Proc. Natl. Acad. Sci. USA 2015, 112, 13123–13127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zubieta-Calleja, G.R.; Paulev, P.E.; Zubieta-Calleja, L.; Zubieta-Calleja, N.; Zubieta-Castillo, G. Hypoventilation in Chronic Mountain Sickness: A mechanism to preserve energy. J. Physiol. Pharmacol. 2006, 57, 425–430. [Google Scholar] [PubMed]
- Wagner, P.D.; Araoz, M.; Boushel, R.; Calbet, J.A.L.; Jessen, B.; Rådegran, G.; Spielvogel, H.; Søndegaard, H.; Wagner, H.; Saltin, B. Pulmonary gas exchange and acid-base state at 5260 m in high-altitude Bolivians and acclimatized lowlanders. J. Appl. Physiol. 2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulev, P.E.; Zubieta-Calleja, G.R. Essentials in the diagnosis of acid-base disorders and their high altitude application. J. Physiol. Pharmacol. 2005, 56, 155–170. [Google Scholar]
- Grogono, A.W.; Solarte, I. Correcting Acid Base Interpretation for High Altitudes. Anesthesiology 2020. [Google Scholar] [CrossRef]
- Apráez, J.I.L. Interpretación de los gases arteriales en Bogotá (2.640 msnm) basada en el nomograma de Siggaard-Andersen. Una propuesta para facilitar y unificar la lectura. Rev. Colomb. Neumol. 2014. [Google Scholar] [CrossRef] [Green Version]
- Grocott, M.P.W.; Martin, D.S.; Levett, D.Z.H.; McMorrow, R.; Windsor, J.; Montgomery, H.E. Arterial blood gases and oxygen content in climbers on Mount Everest. N. Engl. J. Med. 2009, 360, 140–149. [Google Scholar] [CrossRef] [Green Version]
- Zubieta-Calleja, G., Jr. Extremely high altitude hypoxic conditions during Mount Everest expeditions, residence at South Pole stations, in Tibet and among the Andes: Van Slyke equation modification is crucially important for acid–base measurements. J. Biol. Phys. Chem. 2012, 12, 103–112. [Google Scholar] [CrossRef]
- Zubieta-Calleja, G.; Zubieta-Castillo, G. Changes in Oximetry during Breath Holding in Normal Residents of High Altitude (3510m). Progress in Mountain Medicine and H.I.gh Altitude Physiology. In Proceedings of the Press Committee of the 3rd World Congress on Mountain Medicine and High Altitude Physiology, Matsumoto, Japan, 20 May 1998; pp. 343–348. [Google Scholar]
- Auerbach, P.; Miller, Y.E. High Altitude Flatus Expulsion (H.A.F.E.). West. J. Med. 1981, 134, 173–174. [Google Scholar] [PubMed]
- Mansoulié, B. The Ideal Gas Law. In All of Physics (Almost) in 15 Equations; World Scientific Publishing Company: Singapore, 2019. [Google Scholar]
- Frisancho, O. Dolicomegacolon andino y vólvulos intestinales de altura. Rev. Gastroenterol. Perú 2008, 28, 248–257. [Google Scholar]
- Borda, L.; Kcam Mayorca, E.; Alarcon Aguilar, P.; Miranda Rosales, L. Megacolon andino y vólvulo del sigmoides de la altura: Presentación de 418 casos entre 2008–2012 en el hospital C. Monge—Puno, Perú. Rev. Gastroenterol. Perú 2017, 37, 317–322. [Google Scholar]
- Savourey, G.; Launay, J.C.; Besnard, Y.; Guinet, A.; Travers, S. Normo- and hypobaric hypoxia: Are there any physiological differences? Eur. J. Appl. Physiol. 2003. [Google Scholar] [CrossRef] [PubMed]
- Coppel, J.; Hennis, P.; Gilbert-Kawai, E.; Grocott, M.P.W. The physiological effects of hypobaric hypoxia versus normobaric hypoxia: A systematic review of crossover trials. Extrem. Physiol. Med. 2015. [Google Scholar] [CrossRef] [Green Version]
- Zubieta-Calleja, G.R.; Ardaya, G.; Zubieta-DeUrioste, N.; Paulev, P.E. Zubieta-Calleja, G. Tolerance to Hypoxia. J. Fisiol. 2013, 59, 65–71. [Google Scholar]
- Zubieta-Calleja, G.; Zubieta-Castillo, G. Tolerance to Hypoxia: A High Altitude Paradox. Wilderness Environ. Med 2015. [Google Scholar] [CrossRef]
- Zubieta-Calleja, G.; Zubieta-DeUrioste, N. Low Altitude Peripheral Edema (L.A.P.E.): The Opposite of H.A.P.E. or H.A.C.E. Wilderness Environ. Med. 2017, 28, e3. [Google Scholar]
- Zubieta-Castillo, G.; Zubieta-Calleja, G. Triple Hypoxia Syndrome. 1989. Available online: https://www.altitudeclinic.com/thsart.htm (accessed on 12 July 2021).
- Szymczak, R.K.; Marosz, M.; Grzywacz, T.; Sawicka, M.; Naczyk, M. Death Zone Weather Extremes Mountaineers Have Experienced in Successful Ascents. Front. Physiol 2021, 12, 998. [Google Scholar] [CrossRef]
- Marticorena, E.; Hultgren, H.N. Evaluation of therapeutic methods in high altitude pulmonary edema. Am. J. Cardiol. 1979. [Google Scholar] [CrossRef]
- Hultgren, H.N.; Marticorena, E.A. High altitude pulmonary edema. Epidemiologic observations in Peru. Chest 1978. [Google Scholar] [CrossRef]
- Suresh, K.; Shimoda, L.A. Lung circulation. Compr. Physiol. 2016. [Google Scholar] [CrossRef]
- Zubieta-Calleja, G.; Zubieta-DeUrioste, N. Pneumolysis and “Silent Hypoxemia” in COVID-19. Indian J. Clin. Biochem. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bärtsch, P.; Gibbs, J.S.R. Effect of altitude on the heart and the lungs Circulation. Lippincott Williams Wilkins 2007, 116, 2191–2202. [Google Scholar]
- Hultgren, H.N.; Grover, R.F.; Hartley, L.H. Abnormal circulatory responses to high altitude in subjects with a previous history of high-altitude pulmonary edema. Circulation 1971, 44, 759–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luks, A.M.; Swenson, E.R. COVID-19 Lung Injury and High Altitude Pulmonary Edema: A False Equation with Dangerous Implications. Ann. Am. Thorac. Soc. 2020. [Google Scholar] [CrossRef]
- Strapazzon, G.; Hilty, M.P.; Bouzat, P.; Pratali, L.; Brugger, H.; Rauch, S. To compare the incomparable: COVID-19 pneumonia and high-altitude disease. Eur. Respir. J. 2020. [Google Scholar] [CrossRef]
- Archer, S.L.; Sharp, W.W.; Weir, E.K. Differentiating COVID-19 Pneumonia from Acute Respiratory Distress Syndrome and High Altitude Pulmonary Edema: Therapeutic Implications. Circulation 2020. [Google Scholar] [CrossRef]
- Bärtsch, P.; Mairbäurl, H.; Maggiorini, M.; Swenson, E.R. Physiological aspects of high-altitude pulmonary edema. J. Appl. Physiol. 2005. [Google Scholar] [CrossRef] [Green Version]
- Maggiorini, M.; Mélot, C.; Pierre, S.; Pfeiffer, F.; Greve, I.; Sartori, C.; Lepori, M.; Hauser, M.; Scherrer, U.; Naeije, R. High-altitude pulmonary edema is initially caused by an increase in capillary pressure. Circulation 2001, 103, 2078–2083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarenbach, C.F.; Senn, O.; Christ, A.L.; Fischler, M.; Maggiorini, M.; Bloch, K.E. Lung function and breathing pattern in subjects developing high altitude pulmonary edema. PLoS ONE 2012, 7, e41188. [Google Scholar] [CrossRef]
- Herrmann, J.; Mori, V.; Bates, J.H.T.; Suki, B. Modeling lung perfusion abnormalities to explain early COVID-19 hypoxemia. Nat. Commun. 2020, 11, 1–9. [Google Scholar] [CrossRef]
- Schwensen, H.F.; Borreschmidt, L.K.; Storgaard, M.; Redsted, S.; Christensen, S.; Madsen, L.B. Fatal pulmonary fibrosis: A post-COVID-19 autopsy case. J. Clin. Pathol. 2020. [Google Scholar] [CrossRef]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Coudert, J. High-Altitude Pulmonary Edema. Med. Sport. Sci. 1985, 19, 99–102. [Google Scholar]
- Dempsey, J.A.; Morgan, B.J. Humans in hypoxia: A conspiracy of maladaptation?! Physiology 2015, 30, 304–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulloa, N.A.; Cook, J. Altitude Induced Pulmonary Hypertension; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Antezana, G.; Barragán, L.; Coudert, J.; Coudkowicz, L.; Durand, J.; Lockhart, A.; Mensch-Dechene, J.; Zamora, M.P.; Spielvogel, H.; Vargas, E.; et al. The Pulmonary Circulation of High Altitude Natives. In High Altitude Physiology and Medicine; Springer: New York, NY, USA, 1982; pp. 142–149. [Google Scholar]
- Penaloza, D.; Arias-Stella, J.; Sime, F.; Recavarren, S.; Marticorena, E. The heart and pulmonary circulation in children at high altitudes: Physiological, anatomical and clinical observations. Pediatrics 1964, 34, 568–582. [Google Scholar]
- Burtscher, M. Effects of living at higher altitudes on mortality: A narrative review. Aging Disease 2014, 5, 274–280. [Google Scholar] [PubMed]
- Burtscher, J.; Millet, G.P.; Burtscher, M. Does living at moderate altitudes in Austria affect mortality rates of various causes? An ecological study. BMJ Open 2021, 11, e048520. [Google Scholar] [CrossRef]
- Honigman, B. Study Shows Living at High Altitude Reduces Risk of Dying From Heart Disease 2011. Available online: https://www.eurekalert.org/pub_releases/2011-03/uocd-ssl032511.php (accessed on 10 July 2021).
- Saxer, S.; Schneider, S.R.; Appenzeller, P.; Bader, P.R.; Lichtblau, M.; Furian, M.; Sheraliev, U.; Estebesova, B.; Emilov, B.; Sooronbaev, T.; et al. Asthma rehabilitation at high vs. low altitude: Randomized parallel-group trial. BMC Pulm. Med. 2019. [Google Scholar] [CrossRef] [Green Version]
- Narvaez-Guerra, O.; Herrera-Enriquez, K.; Medina-Lezama, J.; Chirinos, J.A. Systemic Hypertension at High Altitude. Hypertension 2018, 72, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Aryal, N.; Weatherall, M.; Bhatta, Y.K.D.; Mann, S. Blood Pressure and Hypertension in Adults Permanently Living at High Altitude: A Systematic Review and Meta-Analysis. High Alt. Med. Biol. 2016, 17, 185–193. [Google Scholar] [CrossRef]
- Simeonov, K.P.; Himmelstein, D.S. Lung cancer incidence decreases with elevation: Evidence for oxygen as an inhaled carcinogen. PeerJ 2015. [Google Scholar] [CrossRef] [Green Version]
- Merrill, R.M.; Frutos, A. Reduced Lung Cancer Mortality With Lower Atmospheric Pressure. Dose Response 2018, 16, 1559325818769484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zubieta-Calleja, G. The Advantages of Ultraviolet Radiation in Controlling the Coronavirus at High Altitude 2020. Available online: http://altitudeclinic.com/blog/2020/04/u_v-radiation-covid-2-at-high-altitude/ (accessed on 10 July 2021).
- Accinelli, R.A.; Leon-Abarca, J.A. At High Altitude COVID-19 Is Less Frequent: The Experience of Peru. Arch. Bronconeumol. 2020, 56, 760–761. [Google Scholar] [CrossRef] [PubMed]
- Cano-Perez, E.; Torres-Pacheco, J.; Fragozo-Ramos, M.C.; Garcia-Diaz, G.; Montalvo-Varela, E.; Pozo-Palacios, J.C. Negative correlation between altitude and COVID-19 pandemic in Colombia: A preliminary report. Am. J. Trop. Med. Hyg. 2020, 103, 2347–2349. [Google Scholar] [CrossRef] [PubMed]
- Bagali, S.; Hadimani, G.A.; Biradar, M.S. Introductory Chapter: Primary Concept of Hypoxia and Anoxia. In Hypoxia and Anoxia; Das, K.K., Ed.; IntechOpen: London, UK, 2018. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PB mmHg | SaO2 % | Hb gm/dL | PaO2 mmHg | CaO2 Vol% | Hb O2 % | Dissolved O2 % | |
|---|---|---|---|---|---|---|---|
| Sea-level | 760 | 99 | 15 | 100 | 20 | 98.45 | 1.55 |
| La Paz (3500 m) | 495 | 90 | 17 | 60 | 20.50 | 99.13 | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zubieta-Calleja, G.; Zubieta-DeUrioste, N. The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes. Int. J. Environ. Res. Public Health 2021, 18, 7619. https://doi.org/10.3390/ijerph18147619
Zubieta-Calleja G, Zubieta-DeUrioste N. The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes. International Journal of Environmental Research and Public Health. 2021; 18(14):7619. https://doi.org/10.3390/ijerph18147619
Chicago/Turabian StyleZubieta-Calleja, Gustavo, and Natalia Zubieta-DeUrioste. 2021. "The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes" International Journal of Environmental Research and Public Health 18, no. 14: 7619. https://doi.org/10.3390/ijerph18147619
APA StyleZubieta-Calleja, G., & Zubieta-DeUrioste, N. (2021). The Oxygen Transport Triad in High-Altitude Pulmonary Edema: A Perspective from the High Andes. International Journal of Environmental Research and Public Health, 18(14), 7619. https://doi.org/10.3390/ijerph18147619