
Use of a Spinal Traction Device during Work Shift in Assembly Line Workers

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcome Measures and Method of Measurement
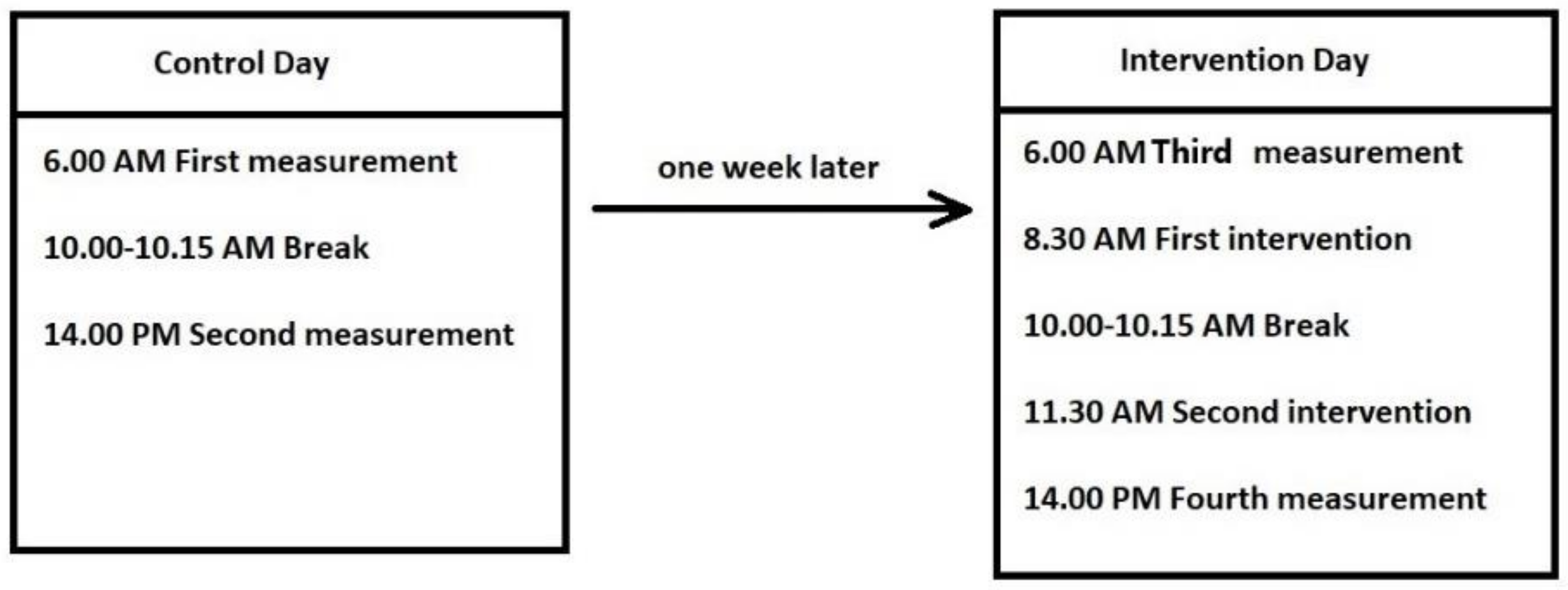
2.3. Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fujii, T.; Matsudaira, K. Prevalence of low back pain and factors associated with chronic disabling back pain in Japan. Eur. Spine J. 2013, 22, 432–438. [Google Scholar] [CrossRef] [Green Version]
- Dagenais, S.; Caro, J.; Haldeman, S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008, 8, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Waters, T.R.; Dick, R.B. Evidence of health risks associated with prolonged standing at work and intervention effectiveness. Rehabil. Nurs. 2015, 40, 148–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, G.; Uchida, K.; Miyagi, M.; Saito, W.; Nakazawa, T.; Imura, T.; Shirasawa, E.; Akazawa, T.; Orita, S.; Inage, K.; et al. Occupational Characteristics of Low Back Pain Among Standing Workers in a Japanese Manufacturing Company. Workplace Health Saf. 2019, 68, 13–23. [Google Scholar] [CrossRef]
- Gallagher, K.M.; Campbell, T.; Callaghan, J.P. The influence of a seated break on prolonged standing induced low back pain development. Ergonomics 2014, 57, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Leivseth, G.; Drerup, B. Spinal shrinkage during work in a sitting posture compared to work in a standing posture. Clin. Biomech. 1997, 12, 409–418. [Google Scholar] [CrossRef]
- Rabal-Pelay, J.; Cimarras-Otal, C.; Alcázar-Crevillén, A.; Planas-Barraguer, J.L.; Bataller-Cervero, A.V. Spinal shrinkage, sagittal alignment and back discomfort changes in manufacturing company workers during a working day. Ergonomics 2019, 62, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- van Deursen, L.L.; van Deursen, D.L.; Snijders, C.J.; Wilke, H.J. Relationship between everyday activities and spinal shrinkage. Clin. Biomech. 2005, 20, 547–550. [Google Scholar] [CrossRef] [PubMed]
- Sparrey, C.J.; Bailey, J.F.; Safaee, M.; Clark, A.J.; Lafage, V.; Schwab, F.; Smith, J.S.; Ames, C.P. Etiology of lumbar lordosis and its pathophysiology: A review of the evolution of lumbar lordosis, and the mechanics and biology of lumbar degeneration. Neurosurg. Focus 2014, 36, E1. [Google Scholar] [CrossRef]
- Sorensen, C.J.; Norton, B.J.; Callaghan, J.P.; Hwang, C.-T.; Van Dillen, L.R. Is lumbar lordosis related to low back pain development during prolonged standing? Man. Ther. 2015, 20, 553–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, S.-W.; Lim, C.-Y.; Kim, K.; Hwang, J.; Chung, S.G. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. Spine J. 2017, 17, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-D.; Oh, H.-K.; Lee, J.-H.; Cha, J.-Y.; Ko, I.-G.; Jee, Y.-S. The effect of inversion traction on pain sensation, lumbar flexibility and trunk muscles strength in patients with chronic low back pain. Isokinet. Exerc. Sci. 2013, 21, 237–246. [Google Scholar] [CrossRef]
- Diab, A.A.; Moustafa, I.M. The efficacy of lumbar extension traction for sagittal alignment in mechanical low back pain: A randomized trial. J. Back Musculoskelet. Rehabil. 2013, 26, 213–220. [Google Scholar] [CrossRef]
- Kamali, F.; Shirazi, S.A.; Ebrahimi, S.; Mirshamsi, M.; Ghanbari, A. Comparison of manual therapy and exercise therapy for postural hyperkyphosis: A randomized clinical trial. Physiother. Theory Pract. 2016, 32, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Steinmaus, C.; Harris-Adamson, C. Sit-stand workstations and impact on low back discomfort: A systematic review and meta-analysis. Ergonomics 2018, 61, 538–552. [Google Scholar] [CrossRef]
- Jakobsen, M.D.; Sundstrup, E.; Brandt, M.; Kristensen, A.Z.; Jay, K.; Stelter, R.; Lavendt, E.; Aagaard, P.; Andersen, L.L. Effect of workplace- versus home-based physical exercise on pain in healthcare workers: Study protocol for a single blinded cluster randomized controlled trial. BMC Musculoskelet. Disord. 2014, 15, 119. [Google Scholar] [CrossRef] [Green Version]
- Kang, T.-W.; Lee, J.-H.; Park, D.-H.; Cynn, H.-S. Effect of 6-week lumbar stabilization exercise performed on stable versus unstable surfaces in automobile assembly workers with mechanical chronic low back pain. Work 2018, 60, 445–454. [Google Scholar] [CrossRef]
- Muyor, J.; Lopez-Minarro, P.A.; Casimiro, A.J. Effect of stretching program in an industrial workplace on hamstring flexibility and sagittal spinal posture of adult women workers: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2012, 25, 161–169. [Google Scholar] [CrossRef]
- Smith, M.D.; Kwan, C.S.J.; Zhang, S.; Wheeler, J.; Sewell, T.; Johnston, V. The Influence of Using a Footstool during a Prolonged Standing Task on Low Back Pain in Office Workers. Int. J. Environ. Res. Public Health 2019, 16, 1405. [Google Scholar] [CrossRef] [Green Version]
- Waongenngarm, P.; Areerak, K.; Janwantanakul, P. The effects of breaks on low back pain, discomfort, and work productivity in office workers: A systematic review of randomized and non-randomized controlled trials. Appl. Ergon. 2018, 68, 230–239. [Google Scholar] [CrossRef]
- Mousavi, E.; Zamanian, Z.; Hadadi, M.; Sobhani, S. Investigating the effect of custom-made insoles and exercises on lower limb and back discomfort in assembly-line workers in a rubber tire factory: A randomized controlled trial. Hum. Factors Ergon. Manuf. Serv. Ind. 2019, 29, 478–484. [Google Scholar] [CrossRef]
- Alrwaily, M.; Almutiri, M.; Schneider, M. Assessment of variability in traction interventions for patients with low back pain: A systematic review. Chiropr. Man. Ther. 2018, 26, 35. [Google Scholar] [CrossRef]
- Chow, D.H.K.; Yuen, E.M.K.; Xiao, L.; Leung, M.C.P. Mechanical effects of traction on lumbar intervertebral discs: A magnetic resonance imaging study. Musculoskelet. Sci. Pract. 2017, 29, 78–83. [Google Scholar] [CrossRef]
- Prasad, K.S.M.; Gregson, B.A.; Hargreaves, G.; Byrnes, T.; Winburn, P.; Mendelow, A.D. Inversion therapy in patients with pure single level lumbar discogenic disease: A pilot randomized trial. Disabil. Rehabil. 2012, 34, 1473–1480. [Google Scholar] [CrossRef]
- Kane, M.D.; Karl, R.D.; Swain, J.H. Effects of Gravity-Facilitated Traction on lntervertebral Dimensions of the Lumbar Spine. J. Orthop. Sports Phys. Ther. 1985, 6, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Kisner, C.; Colby, L.A. The Spine: Traction Procedures. Therapeutic Exercise: Foundations and Techniques; FA Davis Co: Philadelphia, PA, USA, 1996; pp. 575–591. [Google Scholar]
- Ferrari, S.; Manni, T.; Bonetti, F.; Villafañe, J.H.; Vanti, C. A literature review of clinical tests for lumbar instability in low back pain: Validity and applicability in clinical practice. Chiropr. Man. Ther. 2015, 23, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabal-Pelay, J.; Cimarras-Otal, C.; Berzosa, C.; Bernal-Lafuente, M.; Ballestín-López, J.L.; Laguna-Miranda, C.; Planas-Barraguer, J.L.; Bataller-Cervero, A.V. Spinal sagittal alignment, spinal shrinkage, and back pain changes in office workers during a workday. Int. J. Occup. Saf. Ergon. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Carrasquero, E.E. Adaptación y validación española del instrumento cornell musculoskeletal discomfort questionnaires (CMDQ). Spanish adaptation and validation of Cornell musculoskeletal discomfort questionnaire (CDMQ). In Proceedings of the XV International Conference on Occupational Risk Prevention, Santiago de Chile, Chile, 23–26 November 2015. [Google Scholar]
- Adams, M.A.; Conway, T.L. Eta Squared. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 1965–1966. [Google Scholar] [CrossRef]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences; Routledge: London, UK, 2013; p. 735. [Google Scholar]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beynon, C.; Reilly, T. Spinal shrinkage during a seated break and standing break during simulated nursing tasks. Appl. Ergon. 2001, 32, 617–622. [Google Scholar] [CrossRef]
- McGill, S.M.; van Wijk, M.J.; Axler, C.T.; Gletsu, M. Studies of spinal shrinkage to evaluate low-back loading in the workplace. Ergonomics 1996, 39, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.K.; Kim, J.S.; Leven, D.M.; Kim, J.H.; Meaike, J.; Bronheim, R.S.; Suchman, K.I.; Nowacki, D.; Gidumal, S.S.; Cho, S.K. Differences in Fundamental Sagittal Pelvic Parameters Based on Age, Sex, and Race. Clin. Spine Surg. 2018, 31, E109–E114. [Google Scholar] [CrossRef] [PubMed]
- Murrie, V.; Dixon, A.; Hollingworth, W.; Wilson, H.; Doyle, T. Lumbar lordosis: Study of patients with and without low back pain. Clin. Anat. 2003, 16, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Xu, L.; Zhu, F.; Jiang, L.; Wang, Z.; Liu, Z.; Qian, B.P.; Qiu, Y. Sagittal alignment of spine and pelvis in asymptomatic adults: Norms in Chinese populations. Spine 2014, 39, E1–E6. [Google Scholar] [CrossRef]
- Zhou, S.; Li, W.; Wang, W.; Zou, D.; Sun, Z.; Xu, F.; Du, C.; Li, W. Sagittal Spinal and Pelvic Alignment in Middle-Aged and Older Men and Women in the Natural and Erect Sitting Positions: A Prospective Study in a Chinese Population. Med. Sci. Monit. 2020, 26, e919441. [Google Scholar] [CrossRef]
- Ozkunt, O.; Sariyilmaz, K.; Gemalmaz, H.C.; Kaya, O.; Dikici, F. Comparison of spinal sagittal parameters by time of day in a healthy working population: Do we bend during the day? J. Back Musculoskelet. Rehabil. 2018, 31, 381–388. [Google Scholar] [CrossRef]
- Lee, C.-H.; Heo, S.J.; Park, S.H.; Jeong, H.S.; Kim, S.-Y. Functional Changes in Patients and Morphological Changes in the Lumbar Intervertebral Disc after Applying Lordotic Curve-Controlled Traction: A Double-Blind Randomized Controlled Study. Medicina 2019, 56, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Gálvez, N.; Gea-García, G.M.; Marcos-Pardo, P.J. Effects of exercise programs on kyphosis and lordosis angle: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0216180. [Google Scholar] [CrossRef]
- Jang, H.-J.; Hughes, L.C.; Oh, D.-W.; Kim, S.-Y. Effects of Corrective Exercise for Thoracic Hyperkyphosis on Posture, Balance, and Well-Being in Older Women: A Double-Blind, Group-Matched Design. J. Geriatr. Phys. Ther. 2019, 42, E17–E27. [Google Scholar] [CrossRef] [PubMed]
- Seidi, F.; Rajabi, R.; Ebrahimi, I.; Alizadeh, M.H.; Minoonejad, H. The efficiency of corrective exercise interventions on thoracic hyper-kyphosis angle. J. Back Musculoskelet. Rehabil. 2014, 27, 7–16. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Outcome | Control Day | Intervention Day | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post–Pre | Pre | Post–Pre | F | p | η2 | |
| Height (cm), Mean (SD) | 175.93 (3.78) | −1.33 (0.72) a | 175.64 (3.77) | −0.99 (0.23) a | 1.34 | 0.263 | 0.073 |
| Body weight (kg), Mean (SD) | 80.4 (10.06) | −0.35 (0.58) a | 80.28 (10.1) | −0.46 (0.43) a | 1.11 | 0.307 | 0.061 |
| Thoracic angle (°), Mean (SD) | 50.46 (5.16) | +1.01 (2.39) | 49.66 (8.67) | −0.06 (1.7) | 6.35 | 0.022 | 0.272 |
| Lumbar angle (°), Mean (SD) | 21.86 (7.93) | +1.33 (3.08) | 22.86 (7.26) | +1.86 (2.53) a | 0.168 | 0.687 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabal-Pelay, J.; Cimarras-Otal, C.; Macia-Calvo, M.; Laguna-Miranda, C.; Bataller-Cervero, A.V. Use of a Spinal Traction Device during Work Shift in Assembly Line Workers. Int. J. Environ. Res. Public Health 2021, 18, 7708. https://doi.org/10.3390/ijerph18147708
Rabal-Pelay J, Cimarras-Otal C, Macia-Calvo M, Laguna-Miranda C, Bataller-Cervero AV. Use of a Spinal Traction Device during Work Shift in Assembly Line Workers. International Journal of Environmental Research and Public Health. 2021; 18(14):7708. https://doi.org/10.3390/ijerph18147708
Chicago/Turabian StyleRabal-Pelay, Juan, Cristina Cimarras-Otal, Mónica Macia-Calvo, Carmen Laguna-Miranda, and Ana Vanessa Bataller-Cervero. 2021. "Use of a Spinal Traction Device during Work Shift in Assembly Line Workers" International Journal of Environmental Research and Public Health 18, no. 14: 7708. https://doi.org/10.3390/ijerph18147708
APA StyleRabal-Pelay, J., Cimarras-Otal, C., Macia-Calvo, M., Laguna-Miranda, C., & Bataller-Cervero, A. V. (2021). Use of a Spinal Traction Device during Work Shift in Assembly Line Workers. International Journal of Environmental Research and Public Health, 18(14), 7708. https://doi.org/10.3390/ijerph18147708