
ECOCAPTURE@HOME: Protocol for the Remote Assessment of Apathy and Its Everyday-Life Consequences



Abstract
:1. Introduction
1.1. Assessment Limits and the Potential of Information and Communication Technologies
1.2. Actigraphy and Its Limitations
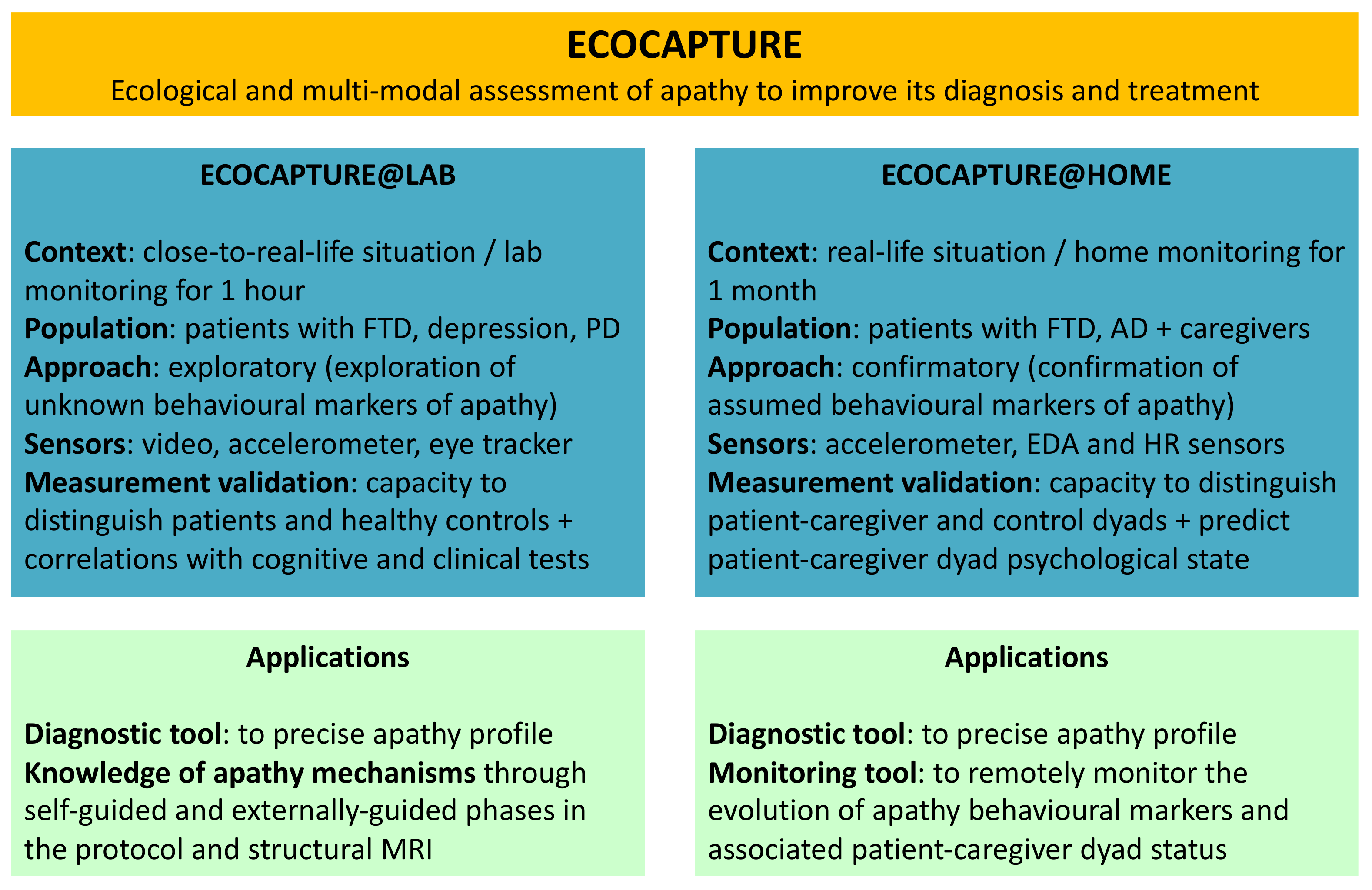
1.3. The ECOCAPTURE Programme
2. Materials and Methods
2.1. Objectives and Hypotheses of the Study
2.1.1. Primary Objectives and Hypotheses
2.1.2. Secondary Objectives
- To investigate the links between the extracted behavioural markers of apathy in real-life conditions and the self-reported measures of apathy
- To investigate the impact of the caregiver’s perception of the dyad’s psychological health status on the subsequent behavioural markers of apathy.
- To investigate the relationships between the caregiver’s and patient’s respective passive behavioural data to test the hypothesis of a dynamic causal relationship between their physiological status.
- To show the capacity of passive behavioural data to predict active behavioural data, as a prerequisite for the future development of a machine learning system able to automatically infer active data from passive ones after a training period.
2.2. Population and Design of the Study
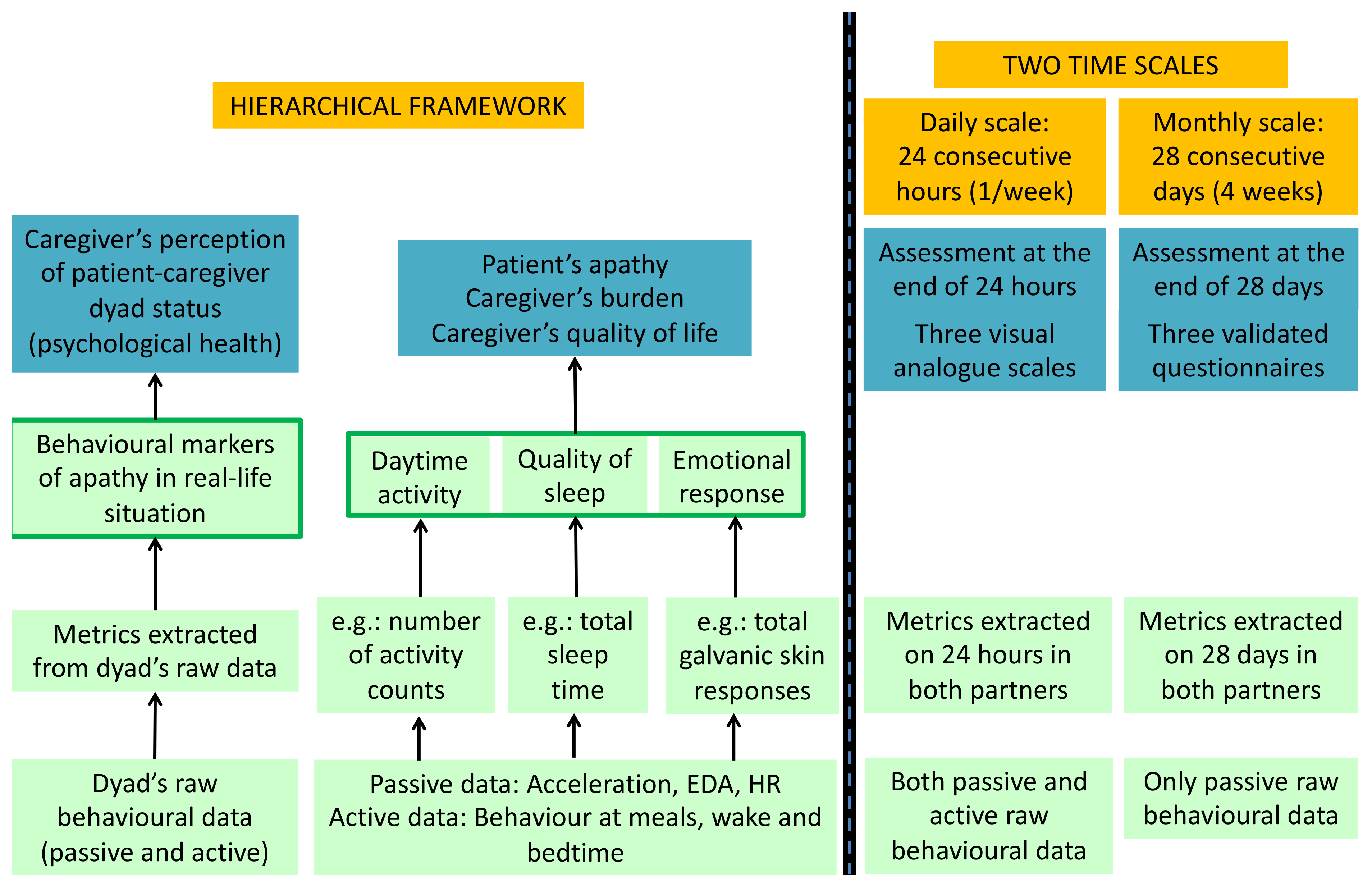
- In all the dyads, the three theoretical behavioural markers of apathy: daytime activity level, quality of sleep, and emotional arousal, will be assessed using a pool of metrics extracted from the dyad’s raw passive and active behavioural data according to a hierarchical framework with three levels (raw data < metrics < markers considered as latent concepts);
- In patient-caregiver dyads only, the caregiver’s perception of the dyad’s psychological state is assessed by the following variables through questionnaires: (1) the patient’s level of apathy, as perceived by the caregiver; (2) the caregiver’s perceived burden; (3) the caregiver’s perceived quality of life.
2.3. Characteristics of Participants
2.3.1. Selected Conditions
2.3.2. Recruitment and Inclusion Criteria
- No evidence of any other cerebral pathology;
- A Mini-Mental State Evaluation (MMSE) score superior or equal to 10 (to minimise the effect of confounding factors related to very severe cognitive impairment);
- Aged between 40 and 85;
- No evidence of any psychiatric condition and a Montgomery-Åsberg Depression Rating Scale (MADRS) score inferior to 20 (to avoid confusion between depression and apathy);
- No evidence of excessive consumption of psychotropic drugs—for instance benzodiazepines, sleeping pills, etc. (due to their tranquilising effect);
- No major physical disability disrupting mobility;
- No heart pacemaker (which would compromise heart rate measuring).
- Aged between 40 and 85;
- No evidence of any psychiatric condition;
- A MADRS score inferior to 20;
- No evidence of excessive consumption of psychotropic drugs;
- No major physical disability disrupting mobility;
- No heart pacemaker.
2.4. Measure of the Behavioural Markers of Apathy
2.4.1. Processing of Passive Behavioural Data from Sensors
- Acceleration signal: We will use a validated signal processing algorithm based on aggregation methods to extract «activity counts» from the raw data of acceleration. Using the validated Cole-Kripke algorithm (an automatic scoring method to distinguish sleep from wakefulness based on wrist actigraphy), we can also detect falling asleep and waking times from the acceleration signal.
- Skin conductance signal: Skin conductance data are traditionally interpreted using validated algorithms that extract two metrics: phasic skin conductance and tonic skin conductance. Phasic changes usually appear as abrupt increases (“peaks”) in the skin conductance. These are generally referred to as Galvanic Skin Responses (GSRs). Tonic skin conductance corresponds to the raw level of conductance of the skin and is usually referred to as Galvanic Skin Level (GSL). Further metrics such as storms (minimum of 5 GSRs/min for at least 10 consecutive minutes) can subsequently be derived from skin conductance data.
- BVP signal: The heart rate is computed by detecting peaks (beats) from the BVP data and computing the lengths of the intervals between adjacent beats. The inter-beat-interval (IBI) timing is used to estimate the instantaneous heart rate (HR), the average HR over multiple beats, and the heart rate variability (HRV) spectrum.
2.4.2. Processing of Active Behavioural Data from Questionnaires
2.4.3. Metrics for Daytime Activity, Quality of Sleep, and Emotional Arousal
2.5. Measure of Caregiver’s Perception of the Dyad’s Psychological State
2.6. Procedure
2.6.1. Visit 1 and Visit 2
2.6.2. Planning of Remote 28-Day Follow-Up
2.6.3. Wearable Sensor System
- A 3-axis accelerometer, which measures acceleration on three orthogonal spatial directions;
- A Galvanic Skin Response (GSR) sensor, which measures the electrical conductance of the skin;
- A photoplethysmography (PPG) sensor, which continuously measures Blood Volume Pulse (BVP, i.e., volumetric variations of blood circulation) using a light source and a photodetector at the surface of skin;
- A thermopile infrared sensor, which reads peripheral skin temperature.
2.6.4. Questionnaire Interfaces on Smartphone Application
- −
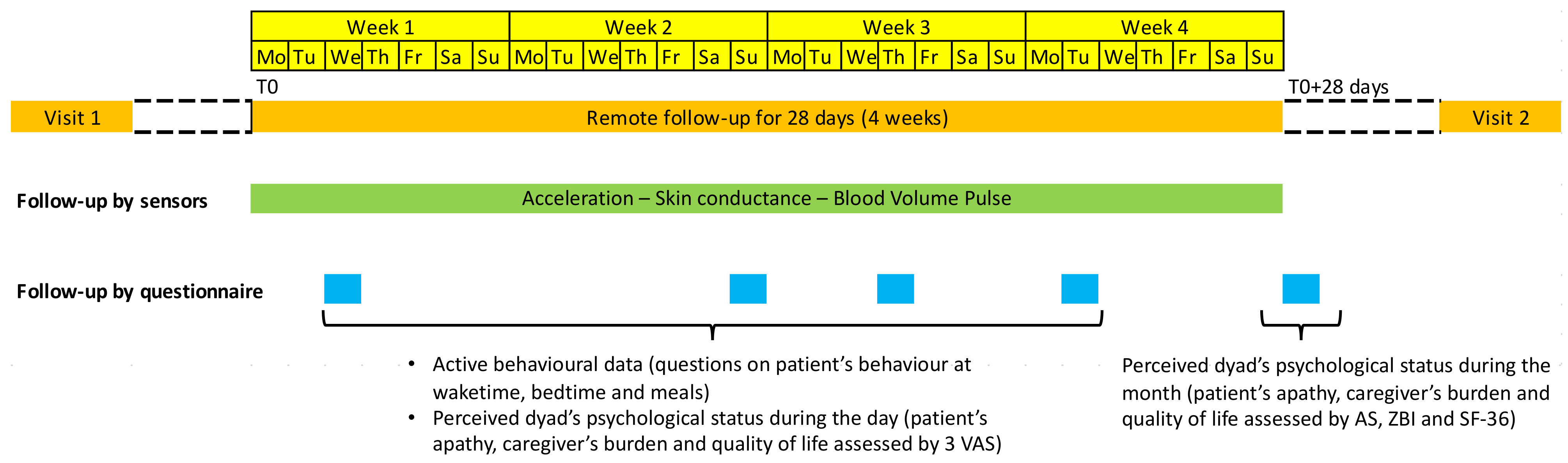
- The day questionnaire interface will be used by one partner (caregiver in patient-caregiver dyads) one day per week to provide information on their partner’s behaviour at: (1) Bedtime (the day before); (2) Wake time; (3) Breakfast; (4) Lunch; (5) Dinner. This interface will also be used at the end of the day by the caregiver (only in patient-caregiver dyads) to provide their perception of the dyad’s psychological status (i.e., patient’s apathy, perceived burden and quality of life) during the day.
- −
- The month questionnaire interface will be used by the caregiver (only in patient-caregiver dyads) at T0 + 28 days to complete the three validated questionnaires (AS, ZBI, SF-36) on their global perception of the dyad’s psychological status (i.e., patient’s apathy, perceived burden, and quality of life) during the 28 days of follow-up.
2.7. Data Flow
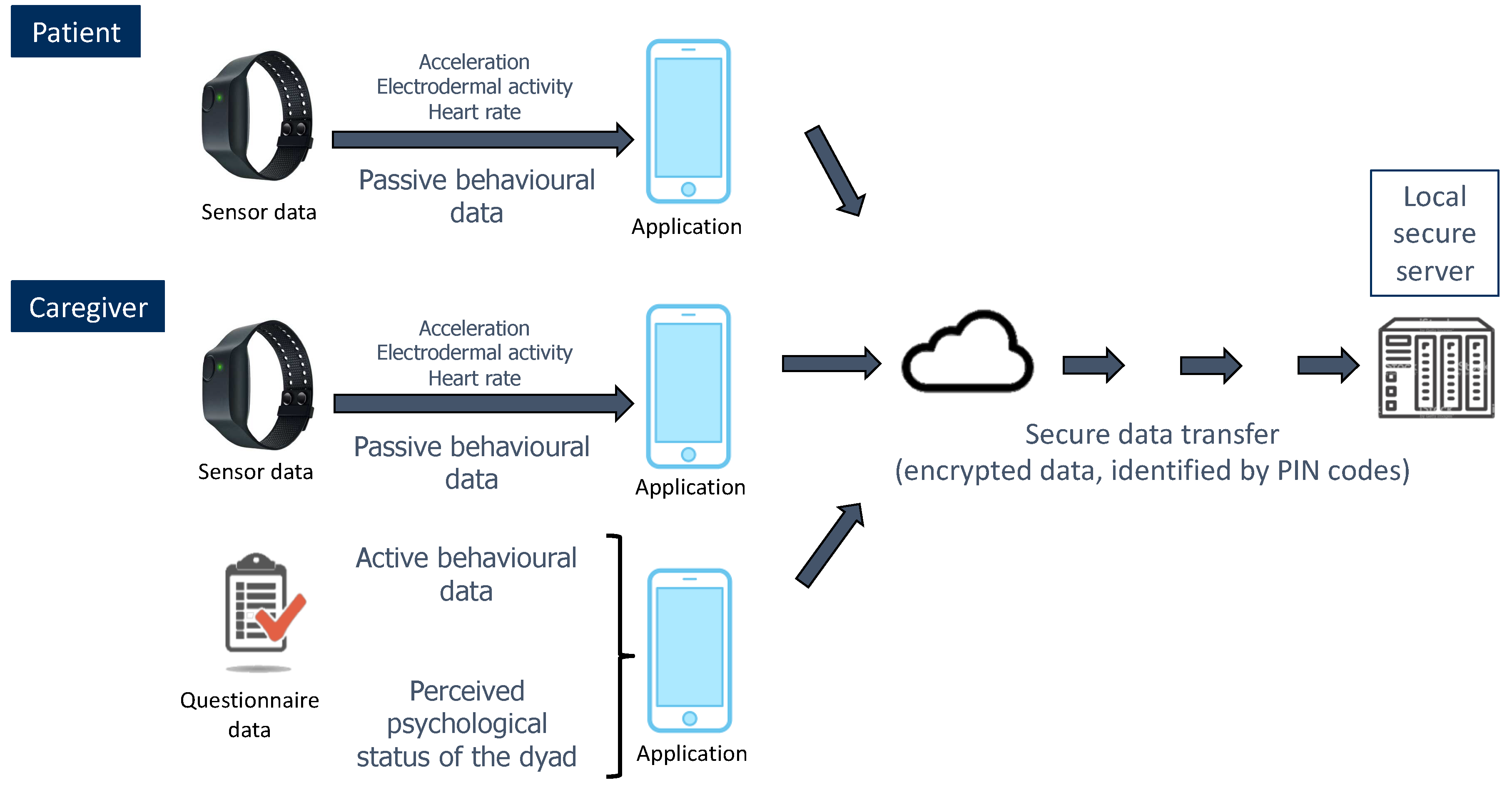
- Collection of two types of data through an application installed (by the investigators) on patients’ and caregivers’ smartphones: data from sensors (passive behavioural data), and data from questionnaires (active behavioural data + caregiver’s perception of the dyad’s psychological state);
- Transfer of these data to a remote server application hosted by a local secure server (of the Paris Brain Institute).
2.8. Statistical Analyses
2.8.1. Sample Size
2.8.2. Analysis Plan for Primary Objective
2.8.3. Analysis Plan for Secondary Objectives
- A.
- We will investigate the links between the extracted behavioural markers of apathy in real-life conditions and the self-reported measures of apathy using a linear regression. We may also compare the clusters of individuals with dementia identified based on the behavioural markers with those based on the self-reported measures of apathy (DAS subscales in particular).
- B.
- We will analyse the impact of caregiver’s perception of the dyad’s psychological status on the subsequent behavioural markers of apathy using a linear regression to show that the caregiver’s perception at day N predicts the three behavioural markers of apathy at day N + 1 (i.e., one week later) above and beyond the markers of apathy at day N.
- C.
- We also will study the relationships between the patient’s and his/her caregiver’s passive behavioural data using Granger causality test (to investigate causality between two variables in a time series) applied to the different sensor signals collected for 28 days in patient-caregiver dyads.
- D.
- We will attempt to show that passive behavioural data can predict active behavioural data collected on a daily scale. For this purpose, we will create categories derived from the active behavioural data (for instance, good–medium–bad day from the caregiver’s point of view) and use different supervised clustering methods (Linear Discriminant Analysis, Random Forest, Support Vector Machine, Artificial Neural Networks, K-Nearest Neighbours) to investigate their capacity to predict the correct category from the set of passive behavioural data.
3. Expected Results and Discussion
3.1. Expected Results
3.2. Potential Limitations of the Project
3.3. Potential Impacts of the Project
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Robert, P.H.; Clairet, S.; Benoit, M.; Koutaich, J.; Bertogliati, C.; Tible, O.; Caci, H.; Borg, M.; Brocker, P.; Bedoucha, P. The Apathy Inventory: Assessment of Apathy and Awareness in Alzheimer’s Disease, Parkinson’s Disease and Mild Cognitive Impairment. Int. J. Geriatr. Psychiatry 2002, 17, 1099–1105. [Google Scholar] [CrossRef]
- Pasquier, F.; Lebert, F.; Lavenu, I.; Guillaume, B. The Clinical Picture of Frontotemporal Dementia: Diagnosis and Follow-Up. DEM 1999, 10, 10–14. [Google Scholar] [CrossRef]
- Aalten, P.; Verhey, F.R.; Boziki, M.; Bullock, R.; Byrne, E.J.; Camus, V.; Caputo, M.; Collins, D.; de Deyn, P.P.; Elina, K. Neuropsychiatric Syndromes in Dementia. Dement. Geriatr. Cogn. Disord. 2007, 24, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Hurt, C.; Bhattacharyya, S.; Burns, A.; Camus, V.; Liperoti, R.; Marriott, A.; Nobili, F.; Robert, P.; Tsolaki, M.; Vellas, B. Patient and Caregiver Perspectives of Quality of Life in Dementia. Dement. Geriatr. Cogn. Disord. 2008, 26, 138–146. [Google Scholar] [CrossRef]
- Wadsworth, L.P.; Lorius, N.; Donovan, N.J.; Locascio, J.J.; Rentz, D.M.; Johnson, K.A.; Sperling, R.A.; Marshall, G.A. Neuropsychiatric Symptoms and Global Functional Impairment along the Alzheimer’s Continuum. Dement. Geriatr. Cogn. Disord. 2012, 34, 96–111. [Google Scholar] [CrossRef] [PubMed]
- Starkstein, S.E.; Jorge, R.; Mizrahi, R.; Robinson, R.G. A Prospective Longitudinal Study of Apathy in Alzheimer’s Disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 8–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lechowski, L.; Benoit, M.; Chassagne, P.; Vedel, I.; Tortrat, D.; Teillet, L.; Vellas, B. Persistent Apathy in Alzheimer’s Disease as an Independent Factor of Rapid Functional Decline: The REAL Longitudinal Cohort Study. Int. J. Geriatr. Psychiatry 2009, 24, 341–346. [Google Scholar] [CrossRef]
- Drijgers, R.L.; Aalten, P.; Winogrodzka, A.; Verhey, F.R.J.; Leentjens, A.F.G. Pharmacological Treatment of Apathy in Neurodegenerative Diseases: A Systematic Review. Dement. Geriatr. Cogn. Disord. 2009, 28, 13–22. [Google Scholar] [CrossRef]
- Brodaty, H.; Burns, K. Nonpharmacological Management of Apathy in Dementia: A Systematic Review. Am. J. Geriatr. Psychiatry 2012, 20, 549–564. [Google Scholar] [CrossRef]
- Marin, R.S. Apathy: A Neuropsychiatric Syndrome. J. Neuropsychiatry Clin. Neurosci. 1991. [Google Scholar] [CrossRef]
- Marin, R.S. Apathy: Concept, Syndrome, Neural Mechanisms, and Treatment. Semin. Clin. Neuropsychiatry 1996, 1, 304–314. [Google Scholar] [PubMed]
- Levy, R.; Dubois, B. Apathy and the Functional Anatomy of the Prefrontal Cortex–Basal Ganglia Circuits. Cerebr. Cortex 2006, 16, 916–928. [Google Scholar] [CrossRef] [Green Version]
- Robert, P.; Lanctôt, K.L.; Agüera-Ortiz, L.; Aalten, P.; Bremond, F.; Defrancesco, M.; Hanon, C.; David, R.; Dubois, B.; Dujardin, K.; et al. Is It Time to Revise the Diagnostic Criteria for Apathy in Brain Disorders? The 2018 International Consensus Group. Eur. Psychiatry 2018, 54, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogullari, S. Reliability and Validity of the Apathy Evaluation Scale. Psychiatry Res. 1991, 38, 143–162. [Google Scholar] [CrossRef]
- Levy, R. Apathy: A Pathology of Goal-Directed Behaviour. A New Concept of the Clinic and Pathophysiology of Apathy. Rev. Neurol. 2012, 168, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Massimo, L.; Powers, J.P.; Evans, L.K.; McMillan, C.T.; Rascovsky, K.; Eslinger, P.; Ersek, M.; Irwin, D.J.; Grossman, M. Apathy in Frontotemporal Degeneration: Neuroanatomical Evidence of Impaired Goal-Directed Behavior. Front. Hum. Neurosci. 2015, 9. [Google Scholar] [CrossRef] [Green Version]
- Wei, G.; Irish, M.; Hodges, J.R.; Piguet, O.; Kumfor, F. Disease-Specific Profiles of Apathy in Alzheimer’s Disease and Behavioural-Variant Frontotemporal Dementia Differ across the Disease Course. J. Neurol. 2019, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Radakovic, R.; Colville, S.; Cranley, D.; Starr, J.M.; Pal, S.; Abrahams, S. Multidimensional Apathy in Behavioral Variant Frontotemporal Dementia, Primary Progressive Aphasia, and Alzheimer Disease. J. Geriatr. Psychiatry Neurol. 2020, 33, 1–8. [Google Scholar] [CrossRef]
- Massimo, L.; Evans, L.K.; Grossman, M. Differentiating Subtypes of Apathy to Improve Person-Centered Care in Frontotemporal Degeneration. J. Gerontol. Nurs. 2014, 40, 58–65. [Google Scholar] [CrossRef] [Green Version]
- DelliFraine, J.L.; Dansky, K.H. Home-Based Telehealth: A Review and Meta-Analysis. J. Telemed. Telecare 2008, 14, 62–66. [Google Scholar] [CrossRef]
- Korman, M.; Weiss, P.L.; Kizony, R. Living Labs: Overview of Ecological Approaches for Health Promotion and Rehabilitation. Disabil. Rehabil. 2016, 38, 613–619. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Glidden, A.M.; Holloway, M.R.; Birbeck, G.L.; Schwamm, L.H. Teleneurology and Mobile Technologies: The Future of Neurological Care. Nat. Rev. Neurol. 2018, 14, 285–297. [Google Scholar] [CrossRef]
- König, A.; Aalten, P.; Verhey, F.; Bensadoun, G.; Petit, P.-D.; Robert, P.; David, R. A Review of Current Information and Communication Technologies: Can They Be Used to Assess Apathy?: Current and New Methods for the Assessment of Apathy. Int. J. Geriatr. Psychiatry 2014, 29, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Manera, V.; Abrahams, S.; Agüera-Ortiz, L.; Bremond, F.; David, R.; Fairchild, K.; Gros, A.; Hanon, C.; Husain, M.; König, A. Recommendations for the Nonpharmacological Treatment of Apathy in Brain Disorders. Am. J. Geriatr. Psychiatry 2020, 28, 410–420. [Google Scholar] [CrossRef]
- Chi, N.-C.; Demiris, G. A Systematic Review of Telehealth Tools and Interventions to Support Family Caregivers. J. Telemed. Telecare 2015, 21, 37–44. [Google Scholar] [CrossRef] [PubMed]
- David, R.; Rivet, A.; Robert, P.H.; Mailland, V.; Friedman, L.; Zeitzer, J.M.; Yesavage, J. Ambulatory Actigraphy Correlates with Apathy in Mild Alzheimer’s Disease. Dementia 2010, 9, 509–516. [Google Scholar] [CrossRef] [Green Version]
- David, R.; Mulin, E.; Friedman, L.; Le Duff, F.; Cygankiewicz, E.; Deschaux, O.; Garcia, R.; Yesavage, J.A.; Robert, P.H.; Zeitzer, J.M. Decreased Daytime Motor Activity Associated With Apathy in Alzheimer Disease: An Actigraphic Study. Am. J. Geriatr. Psychiatry 2012, 20, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Mulin, E.; Zeitzer, J.M.; Friedman, L.; Le Duff, F.; Yesavage, J.; Robert, P.H.; David, R. Relationship between Apathy and Sleep Disturbance in Mild and Moderate Alzheimer’s Disease: An Actigraphic Study. J. Alzheimer’s Dis. 2011, 25, 85–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeitzer, J.M.; David, R.; Friedman, L.; Mulin, E.; Garcia, R.; Wang, J.; Yesavage, J.A.; Robert, P.H.; Shannon, W. Phenotyping Apathy in Individuals With Alzheimer Disease Using Functional Principal Component Analysis. Am. J. Geriatr. Psychiatry 2013, 21, 391–397. [Google Scholar] [CrossRef] [Green Version]
- Valembois, L.; Oasi, C.; Pariel, S.; Jarzebowski, W.; Lafuente-Lafuente, C.; Belmin, J. Wrist Actigraphy: A Simple Way to Record Motor Activity in Elderly Patients with Dementia and Apathy or Aberrant Motor Behavior. J. Nutr. Health Aging 2015, 19, 759–764. [Google Scholar] [CrossRef]
- Merrilees, J.; Dowling, G.A.; Hubbard, E.; Mastick, J.; Ketelle, R.; Miller, B.L. Characterization of Apathy in Persons With Frontotemporal Dementia and the Impact on Family Caregivers. Alzheimer Dis. Assoc. Disord. 2013, 27, 62–67. [Google Scholar] [CrossRef]
- Mohr, D.C.; Zhang, M.; Schueller, S.M. Personal Sensing: Understanding Mental Health Using Ubiquitous Sensors and Machine Learning. Annu. Rev. Clin. Psychol. 2017, 13, 23–47. [Google Scholar] [CrossRef] [Green Version]
- Batrancourt, B.M.; Lecouturier, K.; Ferrand-Verdejo, J.; Guillemot, V.; Azuar, C.; Bendetowicz, D.; Migliaccio, R.; Rametti-Lacroux, A.; Dubois, B.; Levy, R. Exploration Deficits under Ecological Conditions as a Marker of Apathy in Frontotemporal Dementia. Front. Neurol. 2019, 10, 941. [Google Scholar] [CrossRef] [PubMed]
- Bouldin, E.D.; Winter, K.H.; Andresen, E.M. Lack of Choice in Caregiving Decision and Caregiver Risk of Stress, North Carolina, 2005. Prev. Chronic Dis. 2010, 7, A41. [Google Scholar]
- Radakovic, R.; Abrahams, S. Developing a New Apathy Measurement Scale: Dimensional Apathy Scale. Psychiatry Res. 2014, 219, 658–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, J.; Bradley, M.M.; Jones, J.; Okun, M.S.; Perlstein, W.M.; Bowers, D. The Late Positive Potential, Emotion and Apathy in Parkinson’s Disease. Neuropsychologia 2013, 51, 960–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sano, A.; Picard, R.W. Toward a Taxonomy of Autonomic Sleep Patterns with Electrodermal Activity. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2011, 2011, 777–780. [Google Scholar] [CrossRef] [Green Version]
- Stein, P.K.; Pu, Y. Heart Rate Variability, Sleep and Sleep Disorders. Sleep Med. Rev. 2012, 16, 47–66. [Google Scholar] [CrossRef]
- Grapperon, J.; Pignol, A.-C.; Vion-Dury, J. La mesure de la réaction électrodermale. L’Encéphale 2012, 38, 149–155. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Luecken, L.J. Heart Rate Variability as an Index of Regulated Emotional Responding. Rev. Gen. Psychol. 2006, 10, 229–240. [Google Scholar] [CrossRef] [Green Version]
- Chase, T.N. Apathy in Neuropsychiatric Disease: Diagnosis, Pathophysiology, and Treatment. Neurotox. Res. 2011, 19, 266–278. [Google Scholar] [CrossRef]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; van Swieten, J.C.; Seelaar, H.; Dopper, E.G.P.; Onyike, C.U.; et al. Sensitivity of Revised Diagnostic Criteria for the Behavioural Variant of Frontotemporal Dementia. Brain 2011, 134, 2456–2477. [Google Scholar] [CrossRef]
- Benoit, M.; Staccini, P.; Brocker, P.; Benhamidat, T.; Bertogliati, C.; Lechowski, L.; Tortrat, D.; Robert, P.H. Symptômes Comportementaux et Psychologiques Dans La Maladied’Alzheimer: Résultats de l’étude REAL.FR. Rev. Méd. Interne 2003, 24, 319s–324s. [Google Scholar] [CrossRef]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing Research Diagnostic Criteria for Alzheimer’s Disease: The IWG-2 Criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.; Andrezejewski, P.; Leiguarda, R.; Robinson, R.G. Reliability, Validity, and Clinical Correlates of Apathy in Parkinson’s Disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar]
- Bédard, M.; Pedlar, D.; Martin, N.J.; Malott, O.; Stones, M.J. Burden in Caregivers of Cognitively Impaired Older Adults Living in the Community: Methodological Issues and Determinants. Int. Psychogeriatr. 2000, 12, 307–332. [Google Scholar] [CrossRef] [PubMed]
- Stewart, M. The Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36). Aust. J. Physiother. 2007, 53, 208. [Google Scholar] [CrossRef] [Green Version]
- Cunny, K.A.; Perri, M. Single-item vs multiple-item measures of health-related quality of life. Psychol. Rep. 1991, 69, 127–130. [Google Scholar] [CrossRef]
- Westland, J.C. Lower Bounds on Sample Size in Structural Equation Modeling. Electron. Commer. Res. Appl. 2010, 9, 476–487. [Google Scholar] [CrossRef]
- Picard, R.W.; Fedor, S.; Ayzenberg, Y. Multiple Arousal Theory and Daily-Life Electrodermal Activity Asymmetry. Emot. Rev. 2016, 8, 62–75. [Google Scholar] [CrossRef] [Green Version]
- Can, Y.S.; Chalabianloo, N.; Ekiz, D.; Ersoy, C. Continuous Stress Detection Using Wearable Sensors in Real Life: Algorithmic Programming Contest Case Study. Sensors 2019, 19, 1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion (35 min) | |
|---|---|
| 5 min | After giving further information to the recruited couple on the objectives/conditions of the protocol and making sure that all is clearly understood, the investigator gives to both partners an information notice and collects their non-opposition to participate in the study. If a patient has a legal guardian, non-opposition is provided by the guardian and if a patient is under curatorship, non-opposition is provided by the patient with the help of their curator. |
| 5 min | For all the participants, the collection of demographics (age, sex, and education level), medical history (in particular, date of first symptoms and diagnosis for patients) and treatments. |
| 25 min | Verification of inclusion criteria including two tests:
|
| Assessment of the Severity of Dementia and of Clinical Symptoms of Interest (1 h) | |
| 30 min | For patients, Clinical Dementia Rating (CDR): severity of dementia symptoms in three domains (cognition, autonomy, behaviour). |
| 30 min | For all the participants,
|
| Handing over of the Equipment and Training (15 min) | |
| 15 min |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Godefroy, V.; Levy, R.; Bouzigues, A.; Rametti-Lacroux, A.; Migliaccio, R.; Batrancourt, B. ECOCAPTURE@HOME: Protocol for the Remote Assessment of Apathy and Its Everyday-Life Consequences. Int. J. Environ. Res. Public Health 2021, 18, 7824. https://doi.org/10.3390/ijerph18157824
Godefroy V, Levy R, Bouzigues A, Rametti-Lacroux A, Migliaccio R, Batrancourt B. ECOCAPTURE@HOME: Protocol for the Remote Assessment of Apathy and Its Everyday-Life Consequences. International Journal of Environmental Research and Public Health. 2021; 18(15):7824. https://doi.org/10.3390/ijerph18157824
Chicago/Turabian StyleGodefroy, Valérie, Richard Levy, Arabella Bouzigues, Armelle Rametti-Lacroux, Raffaella Migliaccio, and Bénédicte Batrancourt. 2021. "ECOCAPTURE@HOME: Protocol for the Remote Assessment of Apathy and Its Everyday-Life Consequences" International Journal of Environmental Research and Public Health 18, no. 15: 7824. https://doi.org/10.3390/ijerph18157824
APA StyleGodefroy, V., Levy, R., Bouzigues, A., Rametti-Lacroux, A., Migliaccio, R., & Batrancourt, B. (2021). ECOCAPTURE@HOME: Protocol for the Remote Assessment of Apathy and Its Everyday-Life Consequences. International Journal of Environmental Research and Public Health, 18(15), 7824. https://doi.org/10.3390/ijerph18157824