
Cardiorespiratory Fitness, Blood Pressure and Ethnicity Are Related to Salivary Cortisol Responses after an Exercise Test in Children: The ExAMIN Youth SA Study



Abstract
:1. Introduction
2. Methods
2.1. Study Setting
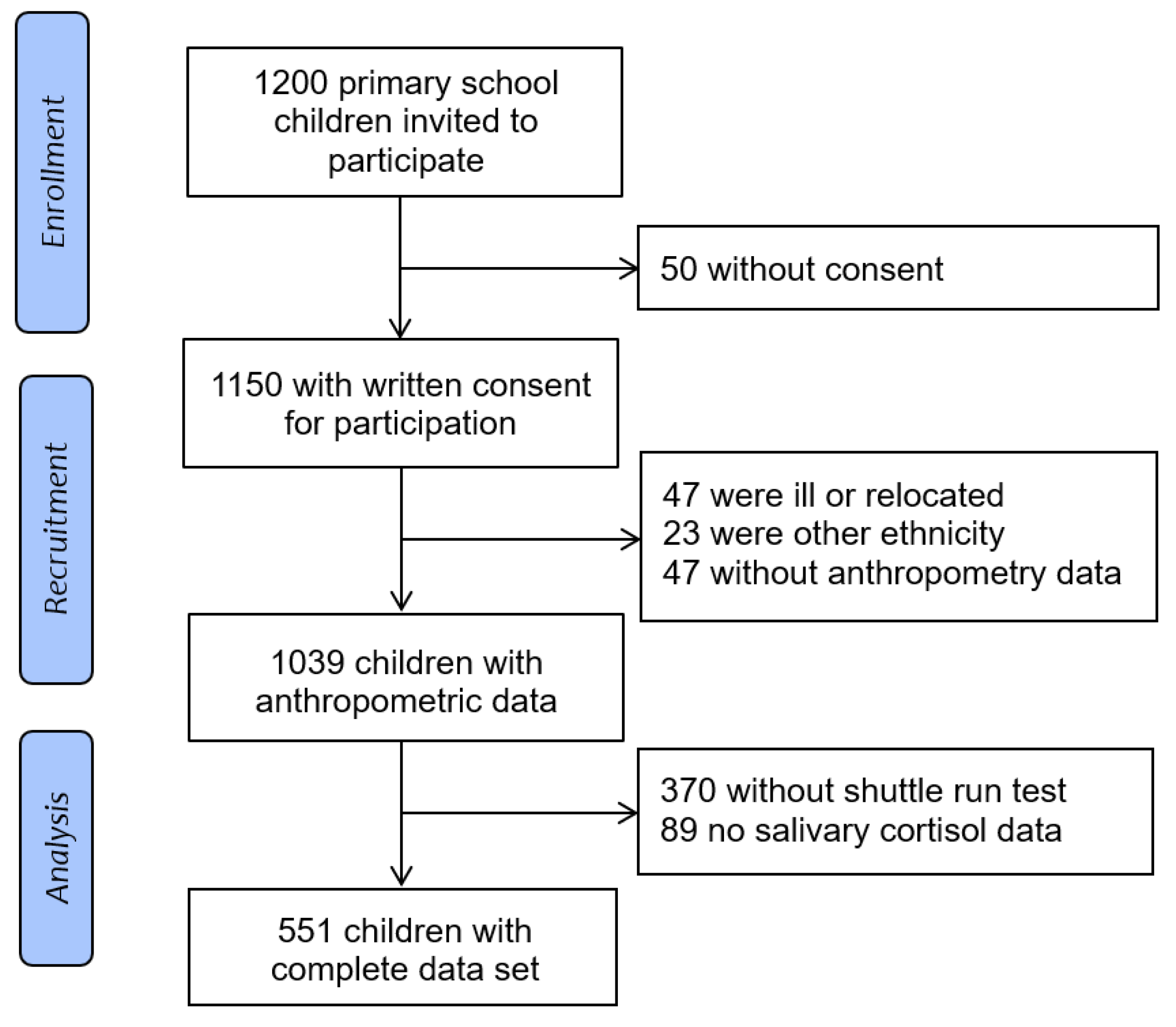
2.2. Participants
2.3. Measurements
2.3.1. Salivary Cortisol
2.3.2. Sociodemographic Data and Anthropometry
2.3.3. Blood Pressure
2.3.4. Cardiorespiratory Fitness
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics and Prevalence
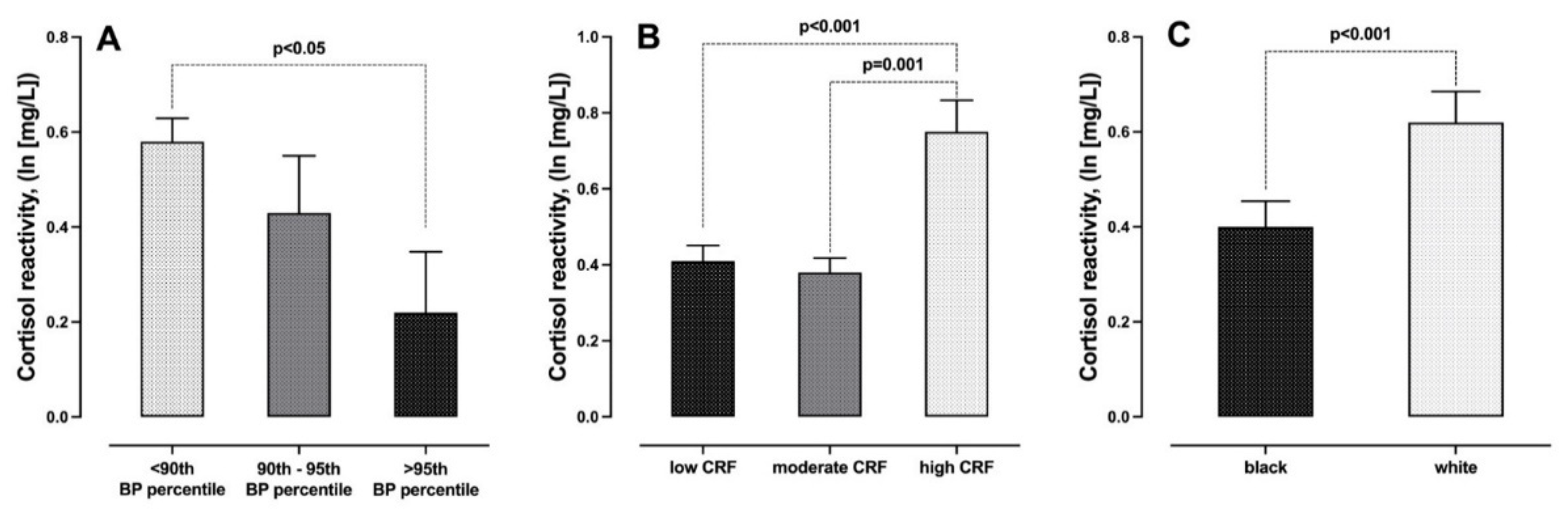
3.2. Group Differences
4. Discussion
4.1. Physical Fitness and Cortisol
4.2. Obesity and Cortisol
4.3. Blood Pressure and Cortisol
4.4. Ethnicity and Cortisol
4.5. Potential Mechanisms
4.6. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vrijkotte, T.G.; van Doornen, L.J.; de Geus, E.J. Effects of Work Stress on Ambulatory Blood Pressure, Heart Rate, and Heart Rate Variability. Hypertension (Dallas Tex 1979) 2000, 35, 880–886. [Google Scholar] [CrossRef]
- Tomiyama, A.J. Stress and Obesity. Annu. Rev. Psychol. 2019, 70, 703–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charmandari, E.; Tsigos, C.; Chrousos, G. Endocrinology of the Stress Response. Annu. Rev. Physiol. 2005, 67, 259–284. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The Impact of Stress on Body Function: A Review. EXCLI J. 2017, 16, 1057–1072. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Wingfield, J.C. The Concept of Allostasis in Biology and Biomedicine. Horm. Behav. 2003, 43, 2–15. [Google Scholar] [CrossRef]
- Charmandari, E.; Kino, T.; Souvatzoglou, E.; Chrousos, G.P. Pediatric Stress: Hormonal Mediators and Human Development. Horm. Res. 2003, 59, 161–179. [Google Scholar] [CrossRef] [Green Version]
- Pervanidou, P.; Chrousos, G.P. Metabolic Consequences of Stress during Childhood and Adolescence. Metabolism 2012, 61, 611–619. [Google Scholar] [CrossRef]
- Teicher, M.H.; Andersen, S.L.; Polcari, A.; Anderson, C.M.; Navalta, C.P. Developmental Neurobiology of Childhood Stress and Trauma. Psychiatr. Clin. N. Am. 2002, 25, 397–426, vii–viii. [Google Scholar] [CrossRef]
- McEwen, B.S. Understanding the Potency of Stressful Early Life Experiences on Brain and Body Function. Metabolism 2008, 57, S11–S15. [Google Scholar] [CrossRef] [Green Version]
- Jessop, D.S.; Turner-Cobb, J.M. Measurement and Meaning of Salivary Cortisol: A Focus on Health and Disease in Children. Stress 2008, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Chrousos, G.P. The Role of Stress and the Hypothalamic-Pituitary-Adrenal Axis in the Pathogenesis of the Metabolic Syndrome: Neuro-Endocrine and Target Tissue-Related Causes. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2000, 24 (Suppl. 2), S50–S55. [Google Scholar] [CrossRef] [Green Version]
- Wirix, A.J.; Finken, M.J.; von Rosenstiel-Jadoul, I.A.; Heijboer, A.C.; Nauta, J.; Groothoff, J.W.; Chinapaw, M.J.; Kist-van Holthe, J.E. Is There an Association Between Cortisol and Hypertension in Overweight or Obese Children? J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Zhou, W.; Wu, S.; Liu, Q.; Li, X. Evidence for Disruption of Diurnal Salivary Cortisol Rhythm in Childhood Obesity: Relationships with Anthropometry, Puberty and Physical Activity. BMC Pediatr. 2020, 20, 381. [Google Scholar] [CrossRef]
- Wood, C.J.; Clow, A.; Hucklebridge, F.; Law, R.; Smyth, N. Physical Fitness and Prior Physical Activity Are Both Associated with Less Cortisol Secretion during Psychosocial Stress. Anxiety Stress Coping 2018, 31, 135–145. [Google Scholar] [CrossRef]
- Heijsman, S.M.; Koers, N.F.; Bocca, G.; van der Veen, B.S.; Appelhof, M.; Kamps, A.W.A. Non-Invasive Measurement of Adrenal Response after Standardized Exercise Tests in Prepubertal Children. J. Pediatr. Endocrinol. Metab. JPEM 2012, 25, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, A.; Hawken, S.; Ounpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N.; Sitthi-amorn, C.; Sato, H.; Yusuf, S.; et al. Association of Psychosocial Risk Factors with Risk of Acute Myocardial Infarction in 11119 Cases and 13648 Controls from 52 Countries (the INTERHEART Study): Case-Control Study. Lancet Lond. Engl. 2004, 364, 953–962. [Google Scholar] [CrossRef]
- Malan, L.; Hamer, M.; Schlaich, M.P.; Lambert, G.W.; Harvey, B.H.; Reimann, M.; Ziemssen, T.; de Geus, E.J.C.N.; Huisman, H.W.; van Rooyen, J.M.; et al. Facilitated Defensive Coping, Silent Ischaemia and ECG Left-Ventricular Hypertrophy: The SABPA Study. J. Hypertens. 2012, 30, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Kruger, R.; Monyeki, M.A.; Schutte, A.E.; Smith, W.; Mels, C.M.C.; Kruger, H.S.; Pienaar, A.E.; Gafane-Matemane, L.F.; Breet, Y.; Lammertyn, L.; et al. The Exercise, Arterial Modulation and Nutrition in Youth South Africa Study (ExAMIN Youth SA). Front. Pediatr. 2020, 8, 212. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet Lond. Engl. 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Flynn, J.T.; Kaelber, D.C.; Baker-Smith, C.M.; Blowey, D.; Carroll, A.E.; Daniels, S.R.; de Ferranti, S.D.; Dionne, J.M.; Falkner, B.; Flinn, S.K.; et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics 2017, 140, e20171904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blair, J.; Adaway, J.; Keevil, B.; Ross, R. Salivary Cortisol and Cortisone in the Clinical Setting. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 161–168. [Google Scholar] [CrossRef]
- Da Silva, V.S.; Vieira, M.F.S.; da Silva, V.S.; Vieira, M.F.S. International Society for the Advancement of Kinanthropometry (ISAK) Global: International Accreditation Scheme of the Competent Anthropometrist. Rev. Bras. Cineantropometria Desempenho Hum. 2020, 22. [Google Scholar] [CrossRef]
- Kelishadi, R.; Mirmoghtadaee, P.; Najafi, H.; Keikha, M. Systematic Review on the Association of Abdominal Obesity in Children and Adolescents with Cardio-Metabolic Risk Factors. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2015, 20, 294–307. [Google Scholar]
- Ashwell, M.; Hsieh, S.D. Six Reasons Why the Waist-to-Height Ratio Is a Rapid and Effective Global Indicator for Health Risks of Obesity and How Its Use Could Simplify the International Public Health Message on Obesity. Int. J. Food Sci. Nutr. 2005, 56, 303–307. [Google Scholar] [CrossRef]
- Bös, K.; Wohlmann, R. Allgemeiner Sportmotorischer Test <AST 6-11> zur Diagnose der konditionellen und koordinativen Leistungsfaehigket. Sportunterricht 1987, 36, S145–S156. [Google Scholar]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C. Validation of Two Running Tests as Estimates of Maximal Aerobic Power in Children. Eur. J. Appl. Physiol. 1986, 55, 503–506. [Google Scholar] [CrossRef]
- Nilsson, P. Early vascular aging (EVA): Consequences and prevention. Vasc. Health Risk Manag. 2008, 4, 547–552. [Google Scholar] [CrossRef] [Green Version]
- Lissak, G. Adverse Physiological and Psychological Effects of Screen Time on Children and Adolescents: Literature Review and Case Study. Environ. Res. 2018, 164, 149–157. [Google Scholar] [CrossRef]
- Wallenius, M.; Hirvonen, A.; Lindholm, H.; Rimpela, A.; Nygard, C.-H.; Saarni, L.; Punamaki, R.-L. Salivary Cortisol in Relation to the Use of Information and Communication Technology (ICT) in School-Aged Children. Psychology 2010, 1, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Nguyen-Michel, S.T.; Unger, J.B.; Hamilton, J.; Spruijt-Metz, D. Associations between Physical Activity and Perceived Stress/Hassles in College Students. Stress Health 2006, 22, 179–188. [Google Scholar] [CrossRef]
- Papafotiou, C.; Christaki, E.; van den Akker, E.L.T.; Wester, V.L.; Apostolakou, F.; Papassotiriou, I.; Chrousos, G.P.; Pervanidou, P. Hair Cortisol Concentrations Exhibit a Positive Association with Salivary Cortisol Profiles and Are Increased in Obese Prepubertal Girls. Stress (Amst. Neth.) 2017, 20, 217–222. [Google Scholar] [CrossRef]
- Köchli, S.; Endes, K.; Steiner, R.; Engler, L.; Infanger, D.; Schmidt-Trucksäss, A.; Zahner, L.; Hanssen, H. Obesity, High Blood Pressure, and Physical Activity Determine Vascular Phenotype in Young Children. Hypertension (Dallas Tex 1979) 2019, 73, 153–161. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Verheyden, B.; Aubert, A.E.; Fagard, R.H. Effects of Aerobic Training Intensity on Resting, Exercise and Post-Exercise Blood Pressure, Heart Rate and Heart-Rate Variability. J. Hum. Hypertens. 2010, 24, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. (Auckl. NZ) 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Hamer, M.; Steptoe, A. Cortisol Responses to Mental Stress and Incident Hypertension in Healthy Men and Women. J. Clin. Endocrinol. Metab. 2012, 97, E29–E34. [Google Scholar] [CrossRef] [Green Version]
- Wright, B.J.; O’Brien, S.; Hazi, A.; Kent, S. Increased Systolic Blood Pressure Reactivity to Acute Stress Is Related with Better Self-Reported Health. Sci. Rep. 2014, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Carroll, D.; Phillips, A.C.; Der, G. Body Mass Index, Abdominal Adiposity, Obesity, and Cardiovascular Reactions to Psychological Stress in a Large Community Sample. Psychosom. Med. 2008, 70, 653–660. [Google Scholar] [CrossRef] [Green Version]
- Mokwatsi, G.G.; Schutte, A.E.; Kruger, R. Ethnic Differences Regarding Arterial Stiffness of 6–8-Year-Old Black and White Boys. J. Hypertens. 2017, 35, 960–967. [Google Scholar] [CrossRef]
- Ramamoorthy, S.; Cidlowski, J. Corticosteroids-Mechanisms of Action in Health and Disease. Rheum. Dis. Clin. N. Am. 2016, 42, 15–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sergio, G. Exploring the complex relations between inflammation and aging (inflamm-aging): Anti-inflamm-aging remodelling of inflamm—Aging, from robustness to frailty. Inflamm. Res. 2008, 57, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Blum, A.; Maser, E. Enzymology and molecular biology of glucocorticoid metabolism in humans. Porg. Nucleic Res. Mol. Biol. 2003, 75, 173–216. [Google Scholar]
- Brydon, L.; O’Donnell, K.; Wright, C.E.; Wawrzyniak, A.J.; Wardle, J.; Steptoe, A. Circulating Leptin and Stress-Induced Cardiovascular Activity in Humans. Obesity 2008, 16, 2642–2647. [Google Scholar] [CrossRef]
- Nina, E.; Markus, S.; Anuradha, A.; David, K.; Murray, E. Interactions Between Leptin and the Human Sympathetic Nervous System. Hypertension 2003, 41, 1072–1079. [Google Scholar] [CrossRef] [Green Version]
- Gubelmann, C.; Kuehner, C.; Vollenweider, P.; Marques-Vidal, P. Association of Activity Status and Patterns with Salivary Cortisol: The Population-Based CoLaus Study. Eur. J. Appl. Physiol. 2018, 118, 1507–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karstoft, K.; Pedersen, B.K. Exercise and Type 2 Diabetes: Focus on Metabolism and Inflammation. Immunol. Cell Biol. 2016, 94, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Mücke, M.; Ludyga, S.; Colledge, F.; Gerber, M. Influence of Regular Physical Activity and Fitness on Stress Reactivity as Measured with the Trier Social Stress Test Protocol: A Systematic Review. Sports Med. (Auckl. NZ) 2018, 48, 2607–2622. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, G.S.; Ioanna, B.; Christina, A.; Andriani, V.; Anastasios, K.; Angeliki, N. Reproducibility of Office and Out-of-Office Blood Pressure Measurements in Children. Hypertension 2021, 77, 993–1000. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Total (n = 551) | Cortisol Groups | p Value | |
|---|---|---|---|---|
| <P25 (n = 137) | ≥P25 (n = 414) | |||
| Age | 7.4 ± 1.0 | 7.2 ± 0.9 | 7.4 ± 1.0 | 0.118 |
| Sex, boys (n, %) | 242; 43.9 | 66; 12.0 | 176; 31.9 | 0.248 |
| Ethnicity, black (n,%) | 324; 58.8 | 94; 17.1 | 230; 41.7 | 0.007 |
| Height (cm) | 122.0 ± 8.2 | 121.1 ± 7.8 | 122.2 ± 8.3 | 0.152 |
| Weight (kg) | 24.3 ± 6.4 | 23.7 ± 5.8 | 24.4 ± 6.6 | 0.261 |
| Body mass index (kg/m2) | 16.1 ± 2.6 | 16.0 ± 2.5 | 16.1 ± 2.7 | 0.582 |
| Body mass index (z-score) | −0.07 ± 1.14 | −0.12 ± 1.24 | −0.06 ± 1.10 | 0.554 |
| Waist circumference (cm) | 54.5 ± 7.0 | 53.9 ± 6.3 | 54.7 ± 7.2 | 0.214 |
| Waist/height ratio | 0.45 ± 0.04 | 0.45 ± 0.04 | 0.45 ± 0.04 | 0.532 |
| Percentage body fat (%) | 24.7 ± 7.9 | 23.9 ± 8.2 | 24.9 ± 7.7 | 0.170 |
| Office systolic BP (mmHg) | 103.9 ± 10.6 | 105.4 ± 11.5 | 103.4 ± 10.2 | 0.062 |
| Office diastolic BP (mmHg) | 64.4 ± 7.9 | 64.8 ± 7.1 | 64.3 ± 8.1 | 0.511 |
| Office heart rate (bpm) | 87.0 ± 12.9 | 89.3 ± 13.1 | 86.2 ± 11.5 | 0.009 |
| Shuttle run (stages) | 3.4 ± 1.6 | 3.1 ± 1.3 | 3.5 ± 1.7 | 0.041 |
| Cortisol at baseline (mg/L) | 0.18 ± 0.22 | 0.24 ± 0.20 | 0.15 ± 0.22 | <0.001 |
| Cortisol at pre (mg/L) | 0.17 ± 0.19 | 0.28 ± 0.18 | 0.13 ± 0.18 | <0.001 |
| Cortisol at post (mg/L) | 0.27 ± 0.27 | 0.13 ± 0.08 | 0.32 ± 0.30 | <0.001 |
| Parameter | n | Cortisol (ln [mg/L]) | |||
|---|---|---|---|---|---|
| Baseline | Pre Sample | Post Sample | Change from Pre to Post | ||
| Body mass index | |||||
| normal weight | 467 | −1.99 (−2.05;−1.92) * | −2.08 (−2.1;−2.01) | −1.60 (−1.67;−1.53) | 0.48 (0.49;0.57) |
| overweight | 44 | −2.04 (−2.23;−1.84) | −2.11 (−2.33;−1.89) | −1.52 (−1.75;−1.30) | 0.59 (0.30;0.88) |
| obesity | 40 | −2.28 (−2.48;−2.07) | −2.18 (−2.41;−1.95) | −1.69 (−1.93;−1.45) | 0.49 (0.19;0.80) |
| Body mass index a | |||||
| normal weight | 467 | −2.00 (−2.06;−1.94) | −2.07 (−2.14;−2.00) | −1.61 (−1.67;−1.54) | 0.47 (0.38;0.56) |
| overweight | 44 | −1.99 (−2.18;−1.80) | −2.14 (−2.36;−1.91) | −1.50 (−1.72;−1.28) | 0.64 (0.35;0.93) |
| obesity | 40 | −2.13 (−2.33;−1.92) | −2.24 (−2.48;−2.00) | −1.67 (−1.91;−1.43) | 0.57 (0.26;0.88) |
| Waist/height ratio | |||||
| <0.5 | 508 | −1.98 (−2.03;−1.92) *** | −2.08 (2.15;−2.02) | −1.60 (−1.67;−1.54) | 0.48 (0.40;0.57) |
| >0.5 | 43 | −2.42 (−2.62;−2.22) | −2.18 (−2.41;−1.96) | −1.60 (−1.83;−1.37) | 0.57 (0.28;0.86) |
| Waist/height ratio a | |||||
| <0.5 | 508 | −1.99 (−2.04;−1.94) * | −2.08 (−2.15;−2.02) | −1.60 (−1.67;−1.54) | 0.48 (0.40;0.56) |
| >0.5 | 43 | −2.25 (−2.45;−2.05) | −2.19 (−2.42;−1.95) | −1.59 (−1.82;−1.36) | 0.60 (0.30;0.90) |
| Systolic BP | |||||
| normal BP | 381 | −2.01 (−2.07;−1.94) | −2.13 (−2.21;−2.06) | −1.58 (−1.66;−1.50) | 0.56 (0.46;0.65) |
| elevated BP | 60 | −1.95 (−2.12;−1.78) | −2.01 (−2.20;−1.82) | −1.53 (−1.72;−1.34) | 0.48 (0.24;0.73) |
| hypertension | 110 | −2.06 (−2.19;−1.94) | −1.99 (−2.13;−1.85) | −1.73 (−1.87;−1.58) | 0.27 (0.08;0.45) * |
| Systolic BP b | |||||
| normal BP | 381 | −2.03 (−2.09;−1.96) | −2.14 (−2.21;−2.07) | −1.56 (−1.64;−1.49) | 0.58 (0.48;0.67) |
| elevated BP | 60 | −1.88 (−2.05;−1.72) | −2.01 (−2.20;−1.82) | −1.59 (−1.77;−1.40) | 0.43 (0.18;0.67) |
| hypertension | 110 | −2.02 (−2.14;−1.90) | −1.96 (−2.11;−1.82) | −1.74 (−1.88;−1.60) | 0.22 (0.04;0.40) ** |
| Diastolic BP | |||||
| normal BP | 429 | −2.01 (−2.08;−1.95) | −2.10 (−2.17;−2.03) | −1.58 (−1.65;−1.51) | 0.52 (0.43;0.61) |
| elevated BP | 46 | −2.09 (−2.28;−1.89) | −2.00 (−2.22;−1.79) | −1.82 (−2.04;−1.60) | 0.18 (−0.10;0.46) |
| hypertension | 76 | −1.96 (−2.11;−1.81) | −2.10 (−2.27;−1.93) | −1.59 (−1.76; −1.41) | 0.51 (0.30;0.73) |
| Diastolic BP b | |||||
| normal BP | 429 | −2.01 (−2.07;−1.95) | −2.10 (−2.17;−2.03) | −1.59 (−1.65;−1.52) | 0.52 (0.43;0.61) |
| elevated BP | 46 | −2.11 (−2.29;−1.93) | −2.00 (−2.21;−1.78) | −1.80 (−2.01;−1.59) | 0.20 (−0.08;0.48) |
| hypertension | 76 | −1.97 (−2.11;−1.83) | −2.08 (−2.25;−1.92) | −1.58 (−1.75; −1.42) | 0.50 (0.28;0.72) |
| Physical fitness | |||||
| low | 209 | −2.09 (−2.18;−2.00) | −2.13 (−2.23;−2.03) | −1.76 (−1.87;−1.67) *** | 0.44 (0.30;0.57) *** |
| moderate | 196 | −1.92 (−2.01;−1.82) | −2.00 (−2.11;−1.90) | −1.62 (−1.73;−1.52) | 0.36 (0.22;0.49) |
| high | 146 | −2.02 (−2.13;−1.92) | −2.15 (−2.27;−2.03) | −1.34 (−1.47;−1.21) | 0.74 (0.58;0.90) |
| Physical fitness c | |||||
| low | 209 | −2.09 (−2.18;−2.00) | −2.17 (−2.28;−2.07) | −1.76 (−1.87;−1.66) *** | 0.41 (0.27;0.54) ** |
| moderate | 196 | −1.94 (−2.03;−1.85) | −1.99 (−2.09;−1.89) | −1.61 (−1.72;−1.51) | 0.38 (0.25;0.51) |
| high | 146 | −1.99 (−2.10;−1.88) | −2.11 (−2.23;−1.98) | −1.36 (−1.49;−1.23) | 0.75 (0.59;0.92) |
| Ethnicity | |||||
| black | 324 | −1.83 (−1.90;−1.76) *** | −2.12 (−2.20;−2.03) | −1.74 (−1.82;−1.66) *** | 0.38 (0.28;0.49) ** |
| white | 227 | −2.27 (−2.35;−2.19) | −2.05 (−2.15;−1.95) | −1.41 (−1.50;−1.31) | 0.64 (0.52;0.77) |
| Ethnicity d | |||||
| black | 324 | −1.84 (−1.91;−1.77) *** | −2.13 (−2.22;−2.05) | −1.74 (−1.82;−1.66) *** | 0.40 (0.29;0.50) ** |
| white | 227 | −2.26 (−2.34;−2.17) | −2.03 (−2.13;−1.93) | −1.41 (−1.51;−1.31) | 0.62 (0.49;0.75) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köchli, S.; Botha-Le Roux, S.; Uys, A.S.; Kruger, R. Cardiorespiratory Fitness, Blood Pressure and Ethnicity Are Related to Salivary Cortisol Responses after an Exercise Test in Children: The ExAMIN Youth SA Study. Int. J. Environ. Res. Public Health 2021, 18, 7898. https://doi.org/10.3390/ijerph18157898
Köchli S, Botha-Le Roux S, Uys AS, Kruger R. Cardiorespiratory Fitness, Blood Pressure and Ethnicity Are Related to Salivary Cortisol Responses after an Exercise Test in Children: The ExAMIN Youth SA Study. International Journal of Environmental Research and Public Health. 2021; 18(15):7898. https://doi.org/10.3390/ijerph18157898
Chicago/Turabian StyleKöchli, Sabrina, Shani Botha-Le Roux, Aletta Sophia Uys, and Ruan Kruger. 2021. "Cardiorespiratory Fitness, Blood Pressure and Ethnicity Are Related to Salivary Cortisol Responses after an Exercise Test in Children: The ExAMIN Youth SA Study" International Journal of Environmental Research and Public Health 18, no. 15: 7898. https://doi.org/10.3390/ijerph18157898
APA StyleKöchli, S., Botha-Le Roux, S., Uys, A. S., & Kruger, R. (2021). Cardiorespiratory Fitness, Blood Pressure and Ethnicity Are Related to Salivary Cortisol Responses after an Exercise Test in Children: The ExAMIN Youth SA Study. International Journal of Environmental Research and Public Health, 18(15), 7898. https://doi.org/10.3390/ijerph18157898