
Boundary Objects: Engaging and Bridging Needs of People in Participatory Research by Arts-Based Methods

Abstract
:1. Introduction
Boundary objects are objects which are both plastic enough to adapt to local needs and the constraints of the several parties employing them, yet robust enough to maintain a common identity across sites. They are weakly structured in common use, and become strongly structured in individual site use. These objects may be abstract or concrete. They have different meanings in different social worlds, but their structure is common enough in more than one world to make them recognizable, used as a means of translation. The creation and management of boundary objects is a key process in developing and maintaining coherence across intersecting social worlds.([11], p. 393)
2. Materials and Methods
3. Results
3.1. DebTalk
“What wonderful, powerful presentations. But complex and intricate. The presentation touched me. They were moving. How much we learn from this meeting. The most important thing is to ‘really’ see each other, to be attentively curious about each other, person to person.”
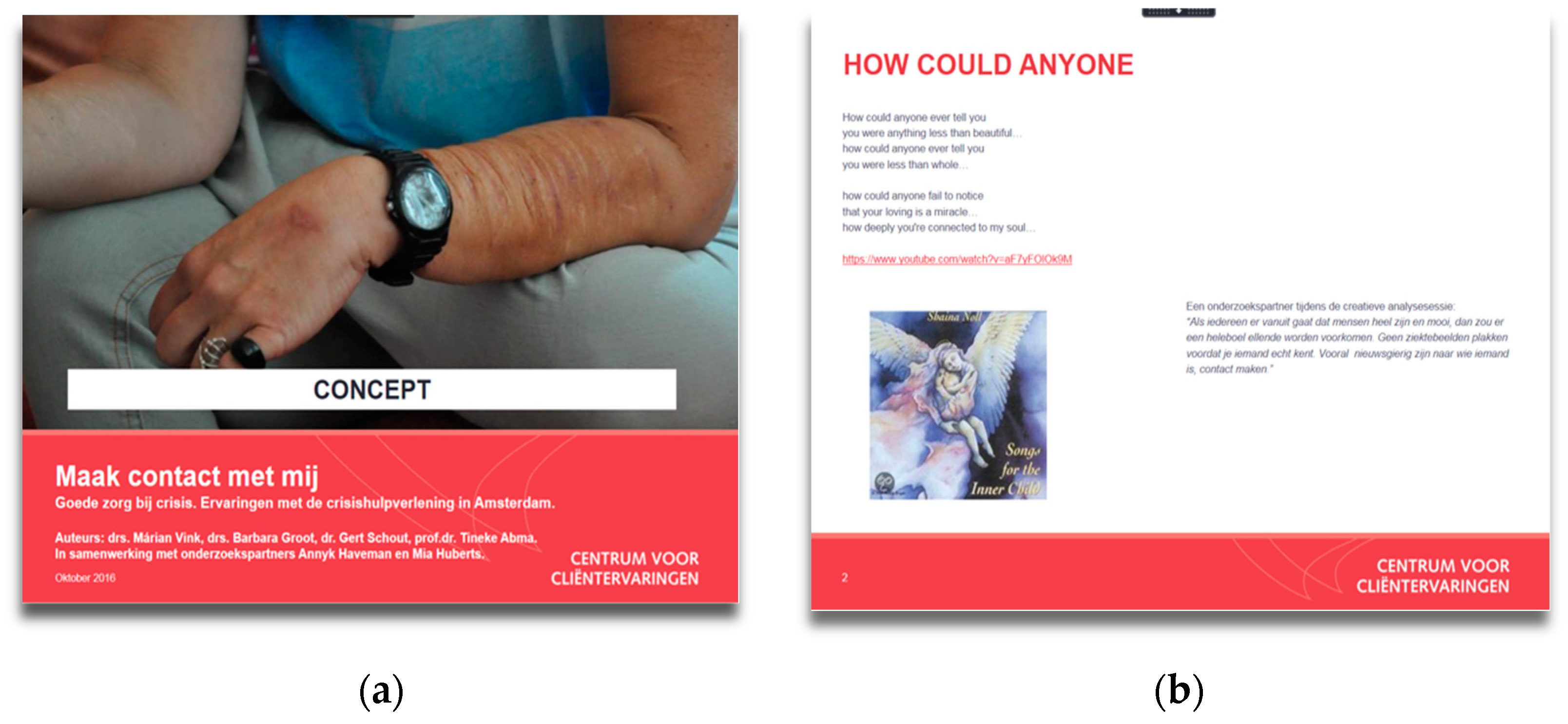
3.2. Make Contact with Me
“If everyone assumes that people are whole and beautiful, a lot of misery would be avoided. No pasting labels before you really know someone. Especially being curious about who someone is, making contact.”
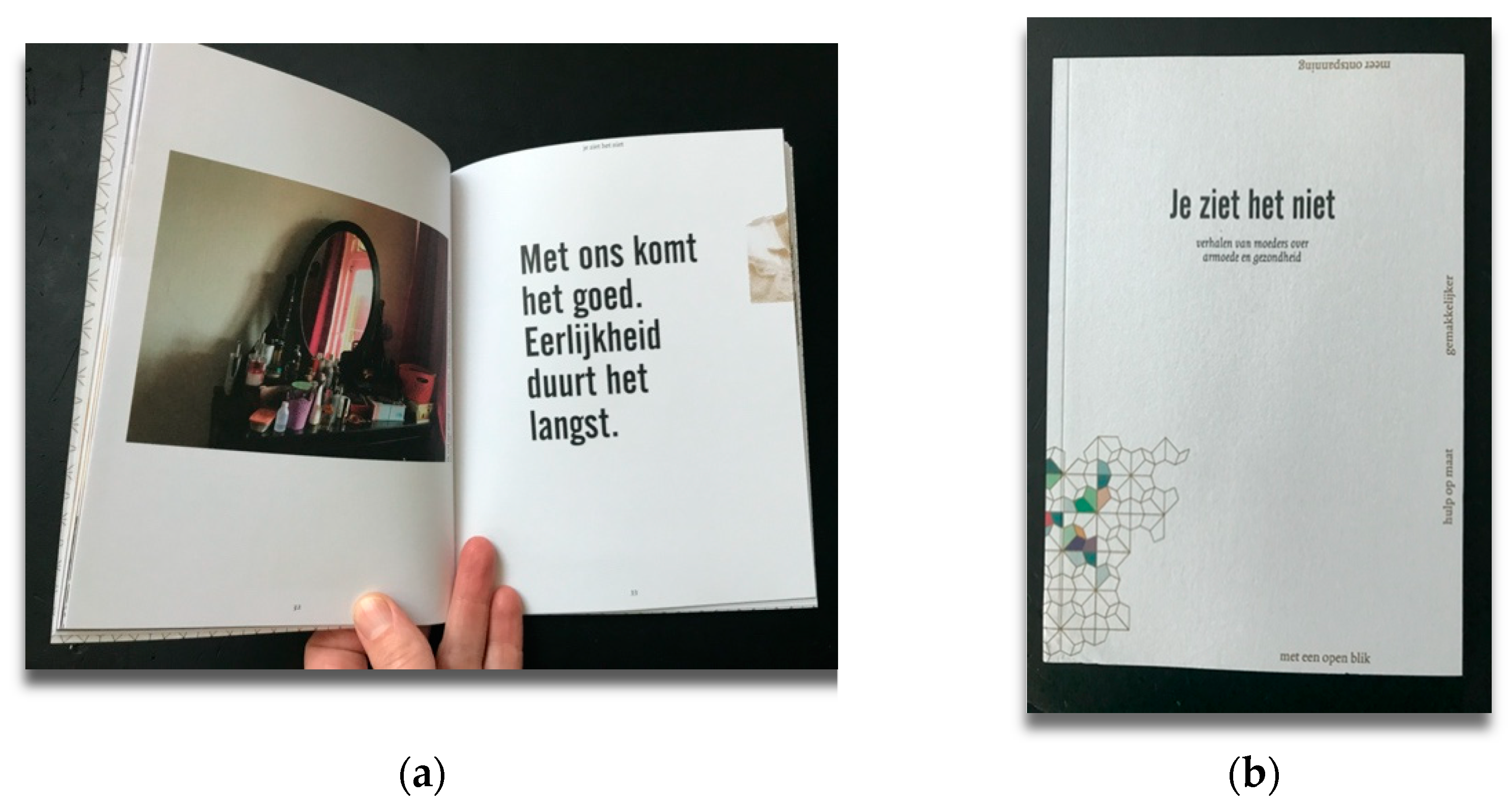
3.3. You Do Not See It
“This conversation made it clear again that sometimes we are not on the right route... Excellent feedback, professional, judgment-free, and positively worded yet not misunderstood. It has put us over the top to change things.”
“Clarifying. It gave me confidence that we are doing a good job in the schools with the children and that that is enough for now. It doesn’t always have to be even grander and more; sometimes we just want too much and too fast.”
“Very nice to talk with this group about our project. They looked at it from a different perspective, and that gave interesting insights. Through such a conversation, you focus consciously on the target group and get more understanding.”
4. Discussion
“Working the hyphen means creating occasions to discuss what is, and is not, “happening between,” within the negotiated relations of whose story is being told, why, to whom, with what interpretation, and whose story is shadowed, why, for whom, and with what consequence. …Self and Other are knottily entangled we inscribe the Other, strain to white our Self, and refuse to engage in contradictions [44].”
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Abma, T.; Banks, S.; Cook, T.; Dias, S.; Madsen, W.; Springett, J.; Wright, M.T. Participatory Research for Health and Social Well-Being; Springer: Berlin/Heidelberg, Germany, 2019; ISBN 978-3-319-93192-0. [Google Scholar]
- Wright, M.T.; Kongats, K. Participatory Health Research: Voices from Around the World; Springer: Berlin/Heidelberg, Germany, 2018; ISBN1 978-3-319-92176-1. ISBN2 978-3-319-92177-8. [Google Scholar]
- Groot, B.; Abma, T. Participatory Health Research with Older People in the Netherlands: Navigating Power Imbalances towards Mutually Transforming Power. In Participatory Health Research; Wright, M.T., Kongats, K., Eds.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 165–178. ISBN1 978-3-319-92176-1. ISBN2 978-3-319-92177-8. [Google Scholar]
- Foucault, M. Power/Knowledge; Routledge: London, UK, 2020; ISBN 978-039-473-954-0. [Google Scholar]
- Leavy, P. Handbook of Arts-Based Research; Guilford Publications: New York, NY, USA, 2017; ISBN 978-146-254-038-9. [Google Scholar]
- McNiff, S. Art-Based Research. In Handbook of the Arts in Qualitative Research: Perspectives, Methodologies, Examples, and Issues; SAGE Publications: New York, NY, USA, 2008; pp. 29–40. [Google Scholar] [CrossRef] [Green Version]
- Heron, J.; Reason, P. Extending Epistemology within a Co-Operative Inquiry. In The Sage Handbook of Action Research: Participative Inquiry and Practice; SAGE Publications: New York, NY, USA, 2008; pp. 366–380. [Google Scholar] [CrossRef]
- Bradbury, H. The Sage Handbook of Action Research; SAGE Publications: New York, NY, USA, 2015. [Google Scholar] [CrossRef] [Green Version]
- Reason, P.; Bradbury, H. Handbook of Action Research: Participative Inquiry and Practice; SAGE Publications: New York, NY, USA, 2001; ISBN 978-1-4129-2029-2. [Google Scholar]
- Leigh Star, S. This is not a boundary object: Reflections on the origin of a concept. Sci. Technol. Hum. Values 2010, 35, 601–617. [Google Scholar] [CrossRef]
- Star, S.L.; Griesemer, J.R. Institutional ecology, ‘translations’ and boundary objects: Amateurs and professionals in Berkeley’s Museum of Vertebrate Zoology, 1907-39. Soc. Stud. Sci. 1989, 19, 387–420. [Google Scholar] [CrossRef]
- Melo, S.; Bishop, S. Translating healthcare research evidence into practice: The role of linked boundary objects. Soc. Sci. Med. 2020, 246, 112731. [Google Scholar] [CrossRef]
- Green, M. Making development agents: Participation as boundary object in international development. J. Dev. Stud. 2010, 46, 1240–1263. [Google Scholar] [CrossRef]
- Yakura, E.K. Charting time: Timelines as temporal boundary objects. Acad. Manag. J. 2002, 45, 956–970. [Google Scholar] [CrossRef]
- Brand, F.S.; Jax, K. Focusing the Meaning (s) of Resilience: Resilience as a Descriptive Concept and a Boundary Object. Ecol. Soc. 2007, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- Amundsen, H.; Hermansen, E.A. Green transformation is a boundary object: An analysis of conceptualisation of transformation in Norwegian primary industries. Environ. Plan. E Nat. Space 2020, 2514848620934337. [Google Scholar] [CrossRef]
- Aalders, J.T.; Moraa, A.; Oluoch-Olunya, N.A.; Muli, D. Drawing together: Making marginal futures visible through collaborative comic creation (CCC). Geogr. Helv. 2020, 75, 415–430. [Google Scholar] [CrossRef]
- Zurba, M.; Berkes, F. Caring for country through participatory art: Creating a boundary object for communicating Indigenous knowledge and values. Local Environ. 2014, 19, 821–836. [Google Scholar] [CrossRef]
- Woodgate, R.L.; Zurba, M.; Tennent, P. A day in the life of a young person with anxiety: Arts-based boundary objects used to communicate the results of health research. Forum Qual. Soz. Forum Qual. Soc. Res. 2017, 18, 3. [Google Scholar] [CrossRef]
- Woodgate, R.L.; Tennent, P.; Legras, N. Understanding Youth’s Lived Experience of Anxiety through Metaphors: A Qualitative, Arts-Based Study. Int. J. Environ. Res. Public Health 2017, 18, 4315. [Google Scholar] [CrossRef] [PubMed]
- Minkler, M.; Wallerstein, N. Community-Based Participatory Research for Health: From Process to Outcomes; John Wiley & Sons: Hoboken, NJ, USA, 2011; ISBN 978-047-026-043-2. [Google Scholar]
- Mitchell, C.; De Lange, N.; Moletsane, R. Participatory Visual Methodologies: Social Change, Community and Policy; SAGE Publications: New York, NY, USA, 2017; ISBN 9781526416117. [Google Scholar]
- Hsiao, R.L.; Tsai, D.H.; Lee, C.F. Collaborative knowing: The adaptive nature of cross-boundary spanning. J. Manag. Stud. 2012, 49, 463–491. [Google Scholar] [CrossRef]
- Akkerman, S.F.; Bakker, A. Boundary crossing and boundary objects. Rev. Educ. Res. 2011, 81, 132–169. [Google Scholar] [CrossRef] [Green Version]
- Daykin, N. Social movements and boundary work in arts, health and wellbeing: A research agenda. Nord. J. Arts Cult. Health 2019, 1, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research; SAGE Publications: New York, NY, USA, 2018; ISBN 978-147-399-711-0. [Google Scholar]
- Abma, T.; Stake, R. Stake’s responsive evaluation: Core ideas and evolution. New Dir. Eval. 2001, 2001, 7–22. [Google Scholar] [CrossRef]
- Stake, R.E. The Art of Case Study Research; SAGE Publications: New York, NY, USA, 1995; ISBN 978-080-395-767-1. [Google Scholar]
- Groot-Sluijsmans, B.C. Ethics of Participatory Health Research: Insights from a Reflective Journey. Ridderprint. 2021. Available online: https://research.vu.nl/en/publications/ethics-of-participatory-health-research-insights-from-a-reflectiv (accessed on 14 July 2021).
- Groot, B.C.; Weerman, A.; Overbeek, F.; Abma, T.A. Making a Difference: Participatory Health Research With Unemployed Citizens and Policymakers. Int. Rev. Qual. Res. 2020, 13, 200–218. [Google Scholar] [CrossRef]
- Groot, B.; Abma, T.; Weerman, A. Het onzegbare uiten. Een creatieve vorm van participatief actieonderzoek. Particip. Herstel 2019, 28, 17–26. [Google Scholar]
- Groot, B.; Haveman, A.; Abma, T. Relational, ethically sound co-production in mental health care research: Epistemic injustice and the need for an ethics of care. Crit. Public Health 2020, 1–11. [Google Scholar] [CrossRef]
- Groot, B.C.; Vink, M.; Haveman, A.; Huberts, M.; Schout, G.; Abma, T.A. Ethics of care in participatory health research: Mutual responsibility in collaboration with co-researchers. Educ. Action Res. 2019, 27, 286–302. [Google Scholar] [CrossRef] [Green Version]
- Groot, B.; Vink, M.; Hubert, M.; Schout, G.; Abma, T. Pathways for improvement of care in psychiatric crisis: A plea for the co-creation with service users and ethics of care. Arch. Psychol. 2019, 3. [Google Scholar] [CrossRef]
- Groot, B.; Abma, T. Participatory health research with mothers living in poverty in the Netherlands: Pathways and challenges to strengthen empowerment. Forum Qual. Soz. Forum Qual. Soc. Res. 2020, 21, 1. [Google Scholar] [CrossRef]
- Banks, S. Everyday ethics in professional life: Social work as ethics work. Ethics Soc. Welf. 2016, 10, 35–52. [Google Scholar] [CrossRef] [Green Version]
- Aldrich, H. Organizational boundaries and inter-organizational conflict. Hum. Relat. 1971, 24, 279–293. [Google Scholar] [CrossRef]
- Aldricht, H.; Herker, D. Boundary spanning roles and organization structure. Acad. Manag. Rev. 1977, 2, 217–230. [Google Scholar] [CrossRef]
- Collien, I. Concepts of power in boundary spanning research: A review and research agenda. Int. J. Manag. Rev. 2021. [Google Scholar] [CrossRef]
- Neal, J.W.; Neal, Z.P.; Brutzman, B. Defining brokers, intermediaries, and boundary spanners: A systematic review. Evid. Policy 2021. [Google Scholar] [CrossRef]
- Hawkins, M.A. Knowledge boundary spanning process: Synthesizing four spanning mechanisms. Manag. Decis. 2012. [Google Scholar] [CrossRef] [Green Version]
- Boler, M. Feeling Power: Emotions and Education; Psychology Press: Hove, UK, 1999; ISBN 978-041-592-104-6. [Google Scholar]
- Zembylas, M. ‘Pedagogy of discomfort’and its ethical implications: The tensions of ethical violence in social justice education. Ethics Educ. 2015, 10, 163–174. [Google Scholar] [CrossRef]
- Fine, M. Working the Hyphens. In Handbook of Qualitative Research; SAGE Publications: New York, NY, USA, 1994; p. 2. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| List of Pathways | Field | Authors |
|---|---|---|
| Healthcare (with professionals) | Melo and Bishop [12] |
| Management studies | Hsiao, Tsai and Lee [23] |
| Learning theory | Akkerman and Bakker [24] |
| Title of Boundary Object | Format of the Objects | Creators of the Objects (Hidden Population) | Period of Creation | Background of Stakeholders | Setting of Sharing the Objects |
|---|---|---|---|---|---|
| DebTalk | Spoken word (on-/offline) | People without a job | 2018 | Service for employment | Theater and Festival of Participation |
| Make contact with me | Report with a song | People with psychiatric vulnerability | 2018 | Psychiatric emergency care | Psychiatric hospital |
| You do not see it | Narrative and photo story | Mothers in poverty | 2019 | Municipality, care, welfare | Different workshops |
| List of Pathways | Field | Authors |
|---|---|---|
| Healthcare (with professionals) | Melo and Bishop [12] |
| Management studies | Hsiao, Tsai and Lee [23] |
| Learning theory | Akkerman and Bakker [24] |
| Participatory health research | Groot and Abma |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Groot, B.; Abma, T. Boundary Objects: Engaging and Bridging Needs of People in Participatory Research by Arts-Based Methods. Int. J. Environ. Res. Public Health 2021, 18, 7903. https://doi.org/10.3390/ijerph18157903
Groot B, Abma T. Boundary Objects: Engaging and Bridging Needs of People in Participatory Research by Arts-Based Methods. International Journal of Environmental Research and Public Health. 2021; 18(15):7903. https://doi.org/10.3390/ijerph18157903
Chicago/Turabian StyleGroot, Barbara, and Tineke Abma. 2021. "Boundary Objects: Engaging and Bridging Needs of People in Participatory Research by Arts-Based Methods" International Journal of Environmental Research and Public Health 18, no. 15: 7903. https://doi.org/10.3390/ijerph18157903
APA StyleGroot, B., & Abma, T. (2021). Boundary Objects: Engaging and Bridging Needs of People in Participatory Research by Arts-Based Methods. International Journal of Environmental Research and Public Health, 18(15), 7903. https://doi.org/10.3390/ijerph18157903