
Recovery and Fatigue Behavior of Forearm Muscles during a Repetitive Power Grip Gesture in Racing Motorcycle Riders


Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Procedures
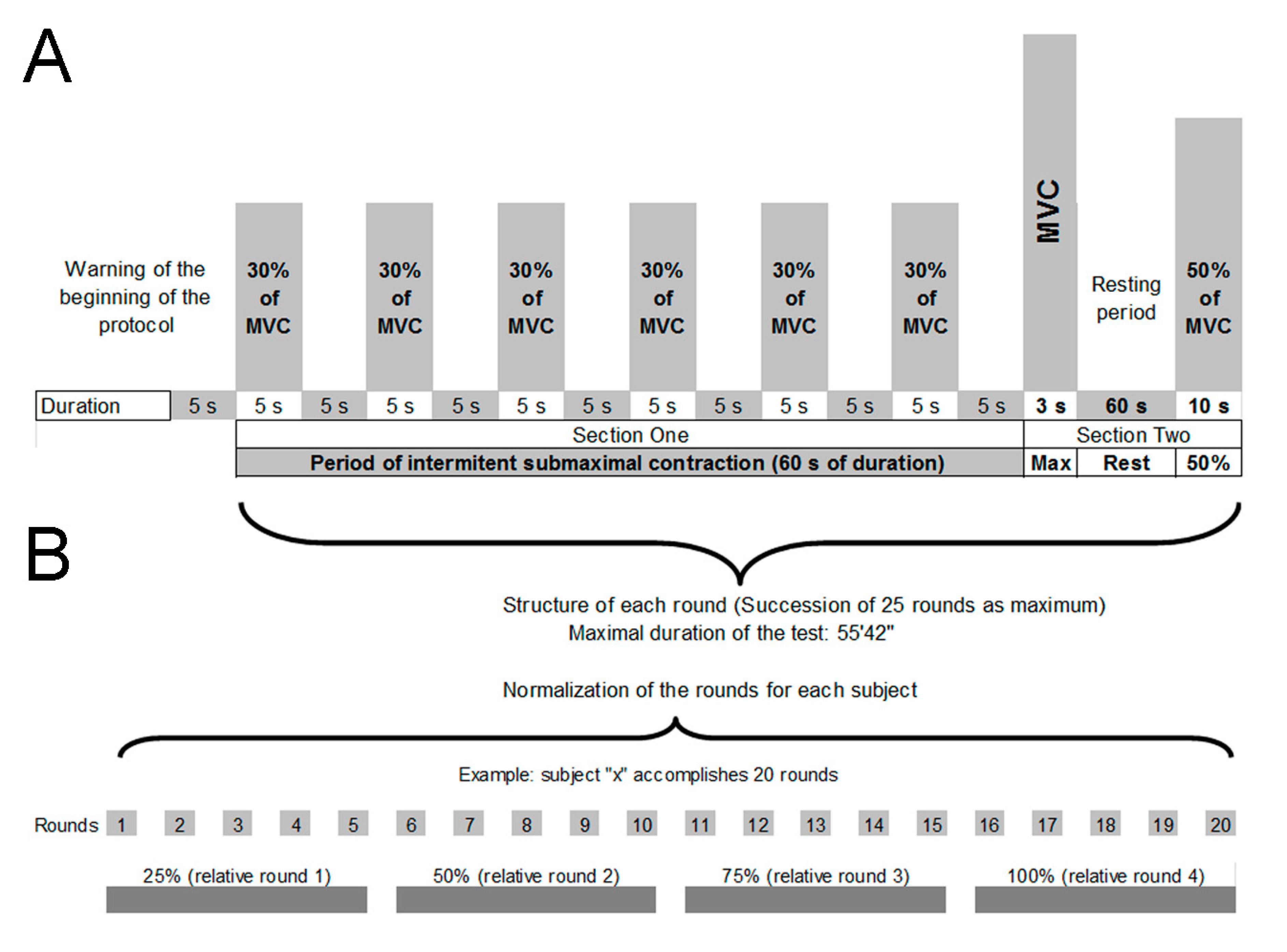
2.3. Sequence and Structure of the IFP
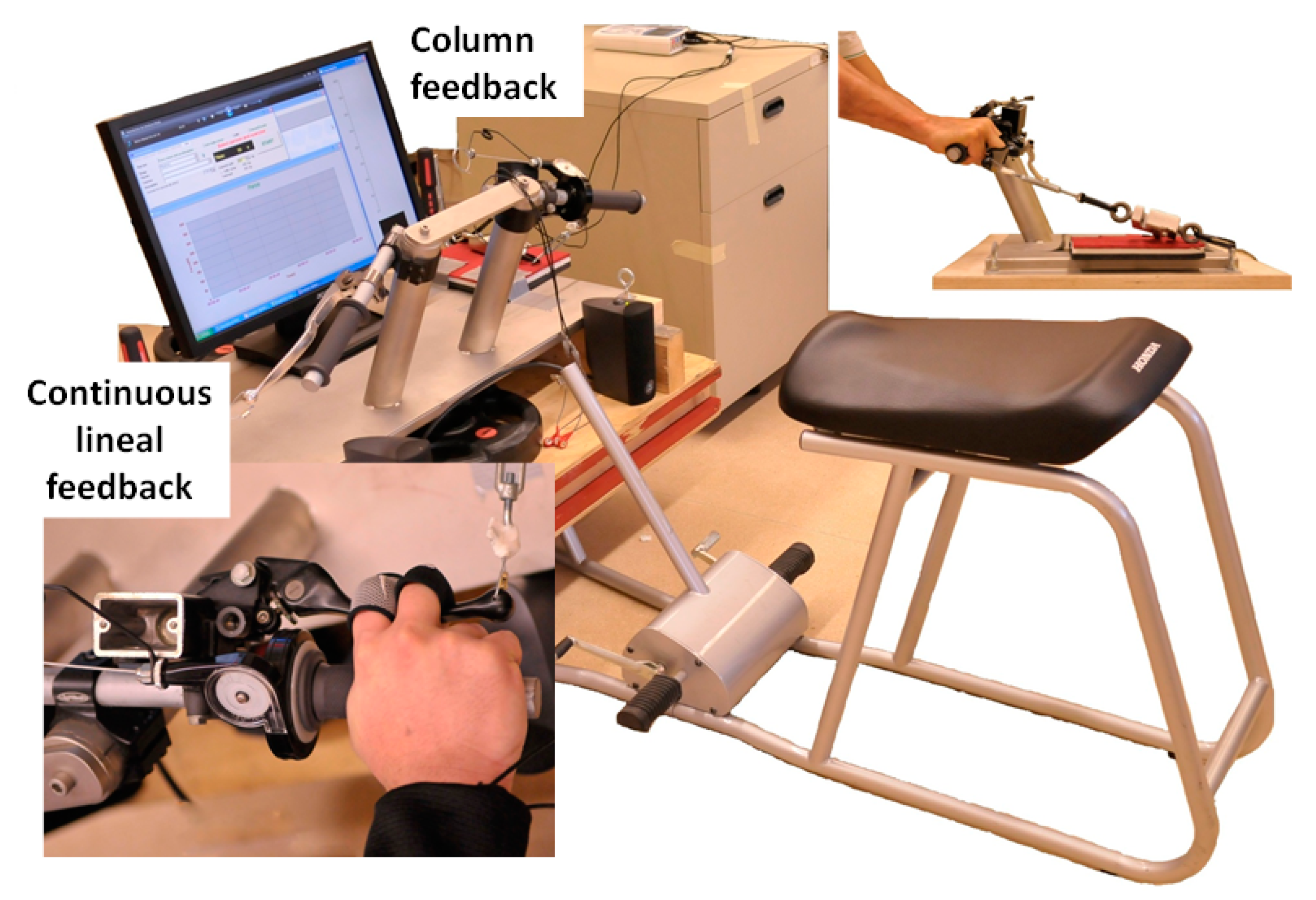
2.4. Dynamometric Assessment
2.5. Electromyography
2.6. Statistics
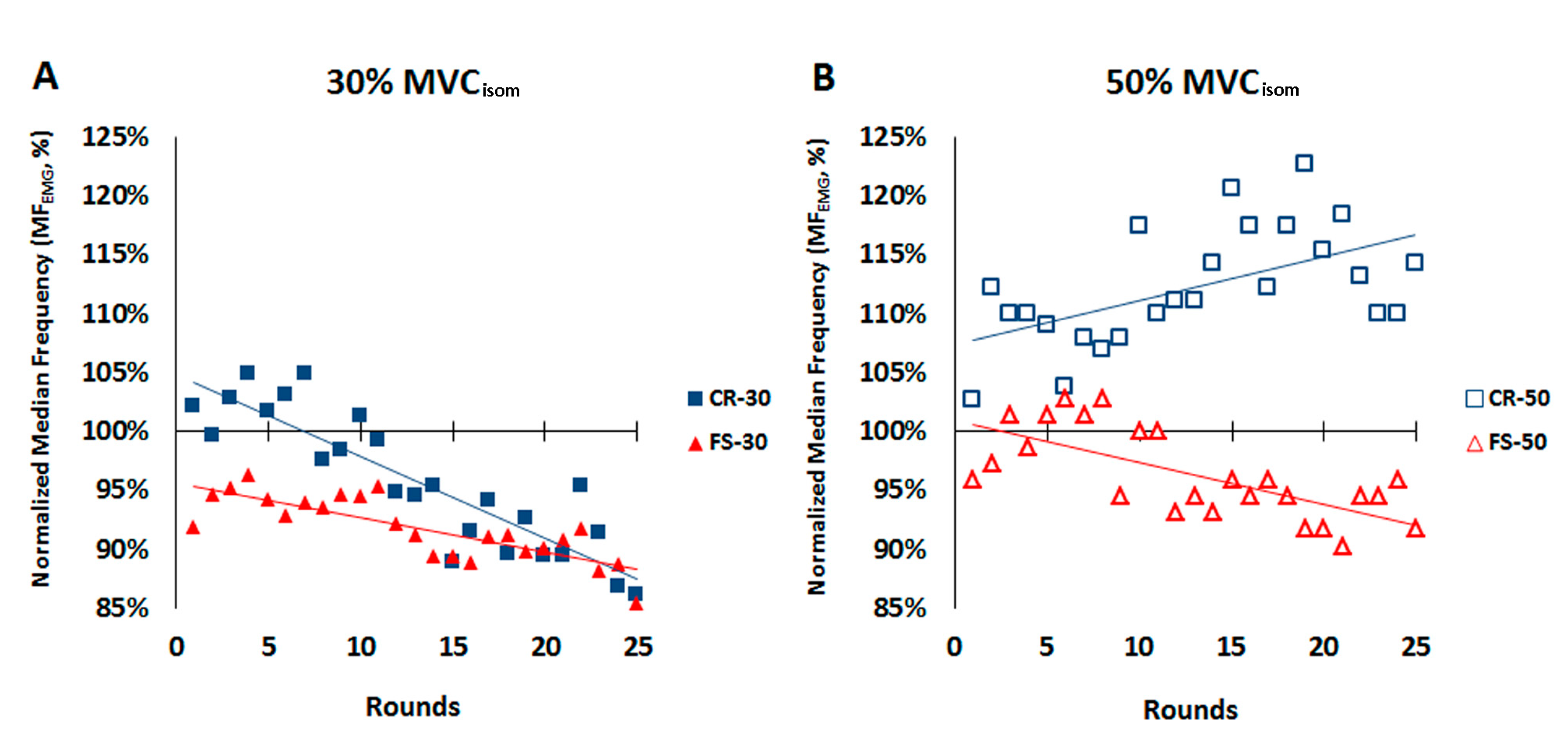
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barrera-Ochoa, S.; Haddad, S.; Correa-Vazquez, E.; Segura, J.F.; Gil, E.; Lluch, A.; Soldado, F.; Mir-Bullo, X. Surgical Decompression of Exertional Compartment Syndrome of the Forearm in Professional Motorcycling Racers: Comparative Long-term Results of Wide-Open Versus Mini-Open Fasciotomy. Clin. J. Sport Med. 2016, 26, 108–114. [Google Scholar] [CrossRef]
- Brown, J.S.; Wheeler, P.C.; Boyd, K.T.; Barnes, M.R.; Allen, M.J. Chronic exertional compartment syndrome of the forearm: A case series of 12 patients treated with fasciotomy. J. Hand Surg. Eur. Vol. 2011, 36, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Gondolini, G.; Schiavi, P.; Pogliacomi, F.; Ceccarelli, F.; Antonetti, T.; Zasa, M. Long-Term Outcome of Mini-Open Surgical Decompression for Chronic Exertional Compartment Syndrome of the Forearm in Professional Motorcycling Riders. Clin. J. Sport Med. 2019, 29, 476–481. [Google Scholar] [CrossRef]
- Goubier, J.N.; Saillant, G. Chronic compartment syndrome of the forearm in competitive motor cyclists: A report of two cases. Br. J. Sports Med. 2003, 37, 452–454. [Google Scholar] [CrossRef] [Green Version]
- Marina, M.; Porta, J.; Vallejo, L.; Angulo, R. Monitoring hand flexor fatigue in a 24-h motorcycle endurance race. J. Electromyogr. Kinesiol. 2011, 21, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, B.A.; Fine, L.J.; Armstrong, T.J. Occupational factors and carpal tunnel syndrome. Am. J. Ind. Med. 1987, 11, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Bystrom, S.; Sjogaard, G. Potassium homeostasis during and following exhaustive submaximal static handgrip contractions. Acta Physiol. Scand. 1991, 142, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Torrado, P.; Cabib, C.; Morales, M.; Valls-Sole, J.; Marina, M. Neuromuscular Fatigue after Submaximal Intermittent Contractions in Motorcycle Riders. Int. J. Sports Med. 2015, 36, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Marina, M.; Torrado, P.; Busquets, A.; Ríos, J.G.; Angulo-Barroso, R. Comparison of an intermittent and continuous forearm muscles fatigue protocol with motorcycle riders and control group. J. Electromyogr. Kinesiol. 2013, 23, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Dousset, E.; Jammes, Y. Reliability of burst superimposed technique to assess central activation failure during fatiguing contraction. J. Electromyogr. Kinesiol. 2003, 13, 103–111. [Google Scholar] [CrossRef]
- Liu, J.Z.; Shan, Z.Y.; Zhang, L.D.; Sahgal, V.; Brown, R.W.; Yue, G.H. Human brain activation during sustained and intermittent submaximal fatigue muscle contractions: An FMRI study. J. Neurophysiol. 2003, 90, 300–312. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.J. Myoelectrical manifestations of localized muscular fatigue in humans. CRC Crit. Rev. Biomed. Eng. 1984, 11, 251–279. [Google Scholar]
- Merletti, R.; LoConte, L.R. Surface EMG signal processing during isometric contractions. J. Electromyogr. Kinesiol. 1997, 7, 241–250. [Google Scholar] [CrossRef]
- Mamaghani, N.K.; Shimomura, Y.; Iwanaga, K.; Katsuura, T. Mechanomyogram and electromyogram responses of upper limb during sustained isometric fatigue with varying shoulder and elbow postures. J. Physiol. Anthr. Appl. Hum. Sci. 2002, 21, 29–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuglevand, A.J.; Zackowski, K.M.; Huey, K.A.; Enoka, R.M. Impairment of neuromuscular propagation during human fatiguing contractions at submaximal forces. J. Physiol. 1993, 460, 549–572. [Google Scholar] [CrossRef] [PubMed]
- Gamet, D.; Maton, B. The fatigability of two agonistic muscles in human isometric voluntary submaximal contraction: An EMG study - I. Assessment of muscular fatigue by means of surface EMG. Eur. J. Appl. Physiol. Occup. Physiol. 1989, 58, 361–368. [Google Scholar] [CrossRef]
- Mathiassen, S.E.; Winkel, J. Quantifying variation in physical load using exposure-vs-time data. Ergonomics 1991, 34, 1455–1468. [Google Scholar] [CrossRef]
- Bystrom, S.E.; Mathiassen, S.E.; Fransson-Hall, C. Physiological effects of micropauses in isometric handgrip exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1991, 63, 405–411. [Google Scholar] [CrossRef]
- Hunter, S.K. Sex differences in human fatigability: Mechanisms and insight to physiological responses. Acta Physiol. 2014, 210, 768–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, S.K.; Enoka, R.M. Changes in muscle activation can prolong the endurance time of a submaximal isometric contraction in humans. J. Appl. Physiol. 2003, 94, 108–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krogh-Lund, C. Myo-electric fatigue and force failure from submaximal static elbow flexion sustained to exhaustion. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 67, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Bystrom, S.E.; Kilbom, A. Physiological response in the forearm during and after isometric intermittent handgrip. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Krogh-Lund, C.; Jorgensen, K. Changes in conduction velocity, median frequency, and root mean square-amplitude of the electromyogram during 25% maximal voluntary contraction of the triceps brachii muscle, to limit of endurance. Eur. J. Appl. Physiol. Occup. Physiol. 1991, 63, 60–69. [Google Scholar] [CrossRef]
- Petrofsky, J.S.; Lind, A.R. Frequency analysis of the surface electromyogram during sustained isometric contractions. Eur. J. Appl. Physiol. Occup. Physiol. 1980, 43, 173–182. [Google Scholar] [CrossRef]
- Nagata, S.; Arsenault, A.B.; Gagnon, D.; Smyth, G.; Mathieu, P.A. EMG Power spectrum as a measure of muscular fatigue at different levels of contraction. Med. Biol. Eng. Comput. 1990, 28, 374–378. [Google Scholar] [CrossRef]
- Ratkevicius, A.; Skurvydas, A.; Povilonis, E.; Quistorff, B.; Lexell, J. Effects of contraction duration on low-frequency fatigue in voluntary and electrically induced exercise of quadriceps muscle in humans. Eur. J. Appl. Physiol. Occup. Physiol. 1998, 77, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Krogh-Lund, C.; Jorgensen, K. Myo-electric fatigue manifestations revisited: Power spectrum, conduction velocity, and amplitude of human elbow flexor muscles during isolated and repetitive endurance contractions at 30 percent maximal voluntary contraction. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 66, 161–173. [Google Scholar] [CrossRef]
- Mundale, M.O. The relationship of intermittent isometric exercise to fatigue of hand grip. Arch. Phys. Med. Rehabil. 1970, 51, 532–539. [Google Scholar]
- Eksioglu, M. Optimal work-rest cycles for an isometric intermittent gripping task as a function of force, posture and grip span. Ergonomics 2006, 49, 180–201. [Google Scholar] [CrossRef] [PubMed]
- Clancy, E.A.; Bertolina, M.V.; Merletti, R.; Farina, D. Time- and frequency-domain monitoring of the myoelectric signal during a long-duration, cyclic, force-varying, fatiguing hand-grip task. J. Electromyogr. Kinesiol. 2008, 18, 789–797. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Katsuura, T.; Harada, H.; Kikuchi, Y. Localized muscular load to different work patterns and heat loads during handgrip. Ann. Physiol. Anthr. 1994, 13, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Quaine, F.; Vigouroux, L.; Martin, L. Finger flexors fatigue in trained rock climbers and untrained sedentary subjects. Int. J. Sports Med. 2003, 24, 424–427. [Google Scholar] [CrossRef]
- De Luca, C.J. The use of surface electromyography in biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef] [Green Version]
- Merletti, R.; Sabbahi, M.A.; De Luca, C.J. Median Frequency of the myoelectric signal: Effects of muscle ischemia and cooling. Eur. J. Appl. Physiol. 1984, 52, 258–265. [Google Scholar] [CrossRef]
- Stulen, F.B.; De Luca, C.J. Frequency parameters of the myoelectric signal as a measure of muscle conduction velocity. IEEE Trans. Biomed. Eng. 1981, 28, 515–523. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.S.; Goncalves, M. Neuromuscular recovery of the biceps brachii muscle after resistance exercise. Res. Sports Med. 2008, 16, 244–256. [Google Scholar] [CrossRef]
- Vøllestad, N.K. Measurement of human muscle fatigue. J. Neurosci. Methods 1997, 74, 219–227. [Google Scholar] [CrossRef]
- Mathiassen, S.E. The influence of exercise/rest schedule on the physiological and psychophysical response to isometric shoulder-neck exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 67, 528–539. [Google Scholar] [CrossRef] [PubMed]
- Christensen, H.; Fuglsangfrederiksen, A. Quantitative surface EMG during sustained and intermittent submaximal contractions. Electroencephalogr. Clin. Neurophysiol. 1988, 70, 239–247. [Google Scholar] [CrossRef]
- Hagg, G.M.; Milerad, E. Forearm extensor and flexor muscle exertion during simulated gripping work - An electromyographic study. Clin. Biomech. 1997, 12, 39–43. [Google Scholar] [CrossRef]
- Luttmann, A.; Matthias, J.; Laurig, W. Electromyographical indication of muscular fatigue in occupational field studies. Int. J. Ind. Ergon. 2000, 25, 645–660. [Google Scholar] [CrossRef]
- Seghers, J.; Spaepen, A. Muscle fatigue of the elbow flexor muscles during two intermittent exercise protocols with equal mean muscle loading. Clin. Biomech. 2004, 19, 24–30. [Google Scholar] [CrossRef]
- Kamimura, T.; Ikuta, Y. Evaluation of grip strength with a sustained maximal isometric contraction for 6 and 10 seconds. J. Rehabil. Med. 2001, 33, 225–229. [Google Scholar]
- Kleine, B.U.; Schumann, N.P.; Stegeman, D.F.; Scholle, H.C. Surface EMG mapping of the human trapezius muscle: The topography of monopolar and bipolar surface EMG amplitude and spectrum parameters at varied forces and in fatigue. Clin. Neurophysiol. 2000, 111, 686–693. [Google Scholar] [CrossRef]
- Green, J.G.; Stannard, S.R. Active recovery strategies and handgrip performance in trained vs. untrained climbers. J. Strength Cond. Res. 2010, 24, 494–501. [Google Scholar] [CrossRef]
- Keir, P.J.; Mogk, J.P. The development and validation of equations to predict grip force in the workplace: Contributions of muscle activity and posture. Ergonomics 2005, 48, 1243–1259. [Google Scholar] [CrossRef] [PubMed]
- Duque, J.; Masset, D.; Malchaire, J. Evaluation of handgrip force from EMG measurements. Appl. Erg. 1995, 26, 61–66. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. SENIAM Projecte: European Recommendations for Surface electroMyoGraphy; Roessingh Research and Development: Enschede, The Netherlands, 1999. [Google Scholar]
- Bigland-Ritchie, B.; Cafarelli, E.; Vøllestad, N.K. Fatigue of submaximal static contractions. Acta Physiol. Scand. Suppl. 1986, 556, 137–148. [Google Scholar]
- Allen, D.G.; Lamb, G.D.; Westerblad, H. Skeletal muscle fatigue: Cellular mechanisms. Physiol. Rev. 2008, 88, 287–332. [Google Scholar] [CrossRef] [Green Version]
- Solomonow, M.; Baten, C.; Smit, J.; Baratta, R.; Hermens, H.; D’Ambrosia, R.; Shoji, H. Electromyogram power spectra frequencies associated with motor unit recruitment strategies. J. Appl. Physiol. 1990, 68, 1177–1185. [Google Scholar] [CrossRef]
- Moritani, T.; Gaffney, F.; Carmichael, T.; Hargis, J. Interrelationships among muscle fiber types, electromyogram, and blood pressure during fatiguing isometric contraction. In Biomechanics IX-A; Winter, D.A., Norman, R., Well, R., Hayes, K., Patla, A., Eds.; Human Kinetics: Champaign, IL, USA, 1985; Volume 5A, pp. 287–292. [Google Scholar]
- Komi, P.V.; Tesch, P. EMG frequency spectrum, muscle structure, and fatigue during dynamic contractions in man. Eur. J. Appl. Physiol. Occup. Physiol. 1979, 42, 41–50. [Google Scholar] [CrossRef]
- Klass, M.; Guissard, N.; Duchateau, J. Limiting mechanisms of force production after repetitive dynamic contractions in human triceps surae. J. Appl. Physiol. 2004, 96, 1516–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peixoto, L.R.; da Rocha, A.F.; de Carvalho, J.L.; Goncalves, C.A. Electromyographic evaluation of muscle recovery after isometric fatigue. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2010, 2010, 4922–4925. [Google Scholar] [CrossRef]
- West, W.; Hicks, A.; Clements, L.; Dowling, J. The relationship between voluntary electromyogram, endurance time and intensity of effort in isometric handgrip exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1995, 71, 301–305. [Google Scholar] [CrossRef]
- Vigouroux, L.; Quaine, F. Fingertip force and electromyography of finger flexor muscles during a prolonged intermittent exercise in elite climbers and sedentary individuals. J. Sports Sci. 2006, 24, 181–186. [Google Scholar] [CrossRef]
- Mills, K.R. Power spectral analysis of electromyogram and compound muscle action potential during muscle fatigue and recovery. J. Physiol. 1982, 326, 401–409. [Google Scholar] [CrossRef]
- Kroon, G.W.; Naeije, M.; Hansson, T.L. Electromyographic power-spectrum changes during repeated fatiguing contractions of the human masseter muscle. Arch. Oral Biol. 1986, 31, 603–608. [Google Scholar] [CrossRef]
- Elfving, B.; Liljequist, D.; Dedering, A.; Németh, G. Recovery of electromyograph median frequency after lumbar muscle fatigue analysed using an exponential time dependence model. Eur. J. Appl. Physiol. 2002, 88, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I. Restitution of EMG spectrum after muscular fatigue. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 57, 311–315. [Google Scholar] [CrossRef]
- Broman, H.; Bilotto, G.; De Luca, C.J. Myoelectric signal conduction velocity and spectral parameters: Influence of force and time. J. Appl. Physiol. 1985, 58, 1428–1437. [Google Scholar] [CrossRef] [PubMed]
- Hara, Y.; Findley, T.W.; Sugimoto, A.; Hanayama, K. Muscle fiber conduction velocity (MFCV) after fatigue in elderly subjects. Electromyogr. Clin. Neurophysiol. 1998, 38, 427–435. [Google Scholar] [PubMed]
- Kadefors, R.; Kaiser, E.; Petersén, I. Dynamic spectrum analysis of myo-potentials and with special reference to muscle fatigue. Electromyography 1968, 8, 39–74. [Google Scholar] [PubMed]
- Petrofsky, J.S. Quantification through the surface EMG of muscle fatigue and recovery during successive isometric contractions. Aviat. Space Environ. Med. 1981, 52, 545–550. [Google Scholar]
- Van der Hoeven, J.H.; Van Weerden, T.W.; Zwarts, M.J. Long-lasting supernormal conduction velocity after sustained maximal isometric contraction in human muscle. Muscle Nerve 1993, 16, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Enoka, R.M.; Duchateau, J. Muscle fatigue: What, why and how it influences muscle function. J. Physiol. 2008, 586, 11–23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| n = 21 | r | r2 | Error of Estimate | F | p | |
|---|---|---|---|---|---|---|
| CR30 | Mean sd | −0.756 ± 0.176 | 0.580 ± 0.266 | 0.026 ± 0.012 | 54.163 ± 57.827 | 0.005 ± 0.009 |
| CI sup CI inf | 0.758 0.753 | 0.583 0.576 | 0.027 0.026 | 54.954 53.372 | 0.006 0.005 | |
| CR50 | Mean sd | 0.594 ± 0.284 | 0.397 ± 0.302 | 0.045 ± 0.019 | 28.046 ± 43.913 | 0.133 ± 0.295 |
| CI sup CI inf | 0.598 0.590 | 0.401 0.393 | 0.045 0.045 | 28.647 27.445 | 0.137 0.129 | |
| FS30 | Mean sd | −0.711 ± 0.152 | 0.504 ± 0.214 | 0.022 ± 0.008 | 27.659 ± 23.267 | 0.005 ± 0.007 |
| CI sup CI inf | 0.713 0.709 | 0.507 0.501 | 0.022 0.002 | 27.977 27.341 | 0.005 0.004 | |
| FS50 | Mean sd | −0.542 ± 0.283 | 0.338 ± 0.290 | 0.033 ± 0.016 | 20.524 ± 31.906 | 0.158 ± 0.288 |
| CI sup CI inf | 0.546 0.539 | 0.342 0.334 | 0.033 0.033 | 20.960 20.087 | 0.161 0.154 | |
| n = 21 | r | p | ||||
|---|---|---|---|---|---|---|
| >0.70 | 0.40–0.69 | <0.39 | <0.001 | 0.001–0.05 | ns | |
| CR30 | 13 | 8 | 0 | 14 | 7 | 0 |
| CR50 | 10 | 7 | 4 | 10 | 7 | 4 |
| FS30 | 13 | 8 | 0 | 12 | 9 | 0 |
| FS50 | 7 | 7 | 7 | 9 | 5 | 7 |
| Effect | F | df | p | η2p | Paired Comparisons | p |
|---|---|---|---|---|---|---|
| T × In × M | 20.04 | 1, 20 | <0.001 | 0.5 | T1 & T2: FS30 < CR30; FS50 < CR50 | <0.001 |
| T1: CR30 > CR50; T2: CR30 < CR50 | <0.002 | |||||
| CR30: T1 > T2; CR50: T1 < T2 | <0.001 | |||||
| T × In | 33.6 | 1, 20 | <0.001 | 0.63 | In30: T1 > T2 | <0.001 |
| In50: T1 < T2 | <0.024 | |||||
| T × M | 0.74 | 1, 20 | ns | 0.04 | ||
| In × M | 3.02 | 1, 20 | ns | 0.13 | ||
| T | 1.43 | 1, 20 | ns | 0.07 | ||
| In | 28.58 | 1, 20 | <0.001 | 0.59 | ||
| M | 42.43 | 1, 20 | <0.001 | 0.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marina, M.; Torrado, P.; Bescós, R. Recovery and Fatigue Behavior of Forearm Muscles during a Repetitive Power Grip Gesture in Racing Motorcycle Riders. Int. J. Environ. Res. Public Health 2021, 18, 7926. https://doi.org/10.3390/ijerph18157926
Marina M, Torrado P, Bescós R. Recovery and Fatigue Behavior of Forearm Muscles during a Repetitive Power Grip Gesture in Racing Motorcycle Riders. International Journal of Environmental Research and Public Health. 2021; 18(15):7926. https://doi.org/10.3390/ijerph18157926
Chicago/Turabian StyleMarina, Michel, Priscila Torrado, and Raul Bescós. 2021. "Recovery and Fatigue Behavior of Forearm Muscles during a Repetitive Power Grip Gesture in Racing Motorcycle Riders" International Journal of Environmental Research and Public Health 18, no. 15: 7926. https://doi.org/10.3390/ijerph18157926
APA StyleMarina, M., Torrado, P., & Bescós, R. (2021). Recovery and Fatigue Behavior of Forearm Muscles during a Repetitive Power Grip Gesture in Racing Motorcycle Riders. International Journal of Environmental Research and Public Health, 18(15), 7926. https://doi.org/10.3390/ijerph18157926