
Longitudinal Associations between the Neighborhood Built Environment and Cognition in US Older Adults: The Multi-Ethnic Study of Atherosclerosis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
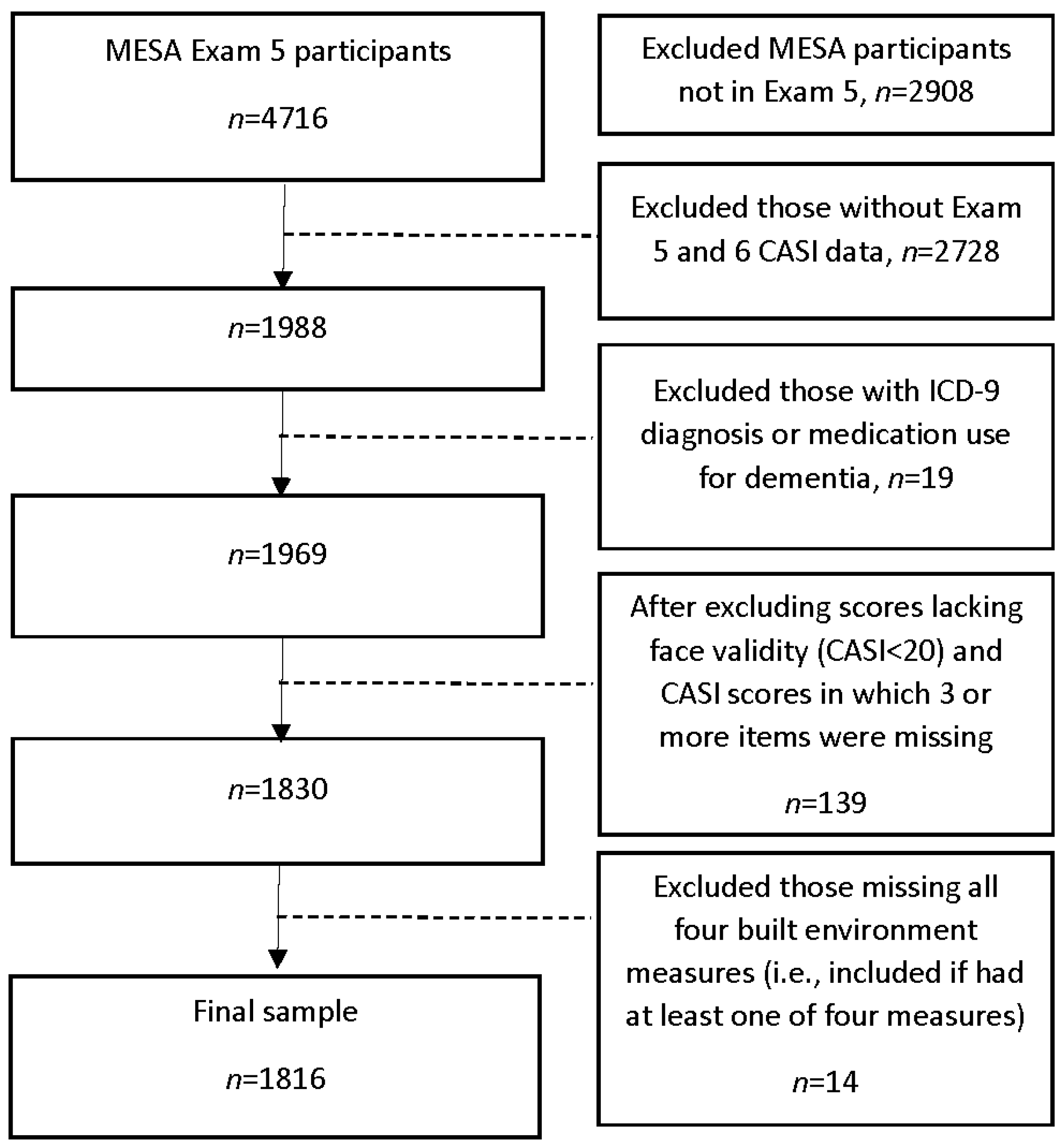
2.1. Sample
2.2. Measures
2.2.1. Cognitive Test Scores
2.2.2. Neighborhood Built Environment Measures
2.2.3. Other Neighborhood Measures
2.2.4. Other Measures
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roberts, R.; Knopman, D.S. Classification and Epidemiology of MCI. Clin. Geriatr. Med. 2013, 29, 753–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimer’s Dement. 2015, 11, 718–726. [Google Scholar] [CrossRef] [Green Version]
- Alzheimer’s Association. 2020 Alzheimer’s Disease Facts and Figures. Available online: https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf (accessed on 24 April 2021).
- Mayne, S.L.; Auchincloss, A.H.; Michael, Y.L. Impact of policy and built environment changes on obesity-related outcomes: A sys-tematic review of naturally occurring experiments. Obes. Rev. 2015, 16, 362–375. [Google Scholar] [CrossRef]
- Ferdinand, A.O.; Sen, B.; Rahurkar, S.; Engler, S.; Menachemi, N. The relationship between built environments and physical activity: A systematic re-view. Am. J. Public Health 2012, 102, e7–e13. [Google Scholar] [CrossRef] [PubMed]
- Mair, C.; Diez Roux, A.V.; Galea, S. Are neighbourhood characteristics associated with depressive symptoms? A review of evidence. J. Epidemiol. Community Health 2008, 62, 940–946. [Google Scholar]
- Badland, H.; Whitzman, C.; Lowe, M.; Davern, M.; Aye, L.; Butterworth, I.; Hes, D.; Giles-Corti, B. Urban liveability: Emerging lessons from Australia for exploring the potential for indicators to measure the social determinants of health. Soc. Sci. Med. 2014, 111, 64–73. [Google Scholar] [CrossRef]
- Wu, Y.T.; Prina, A.M.; Jones, A.; Matthews, F.E.; Brayne, C.; The Medical Research Council Cognitive Function and Ageing Study Collaboration. The Built Environment and Cognitive Disorders: Results from the Cognitive Function and Ageing Study II. Am. J. Prev. Med. 2017, 53, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Cherrie, M.P.C.; Shortt, N.K.; Mitchell, R.J.; Taylor, A.M.; Redmond, P.; Thompson, C.W.; Starr, J.M.; Deary, I.J.; Pearce, J.R. Green space and cognitive ageing: A retrospective life course analysis in the Lothian Birth Cohort 1936. Soc. Sci. Med. 2018, 196, 56–65. [Google Scholar] [CrossRef]
- Clarke, P.J.; Weuve, J.; Barnes, L.; Evans, D.A.; de Leon, C.F.M. Cognitive decline and the neighborhood environment. Ann. Epidemiology 2015, 25, 849–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watts, A.; Ferdous, F.; Moore, K.D.; Burns, J.M. Neighborhood Integration and Connectivity Predict Cognitive Performance and De-cline. Gerontol. Geriatr. Med. 2015, 1, 2333721415599141. [Google Scholar] [CrossRef] [Green Version]
- Groot, C.; Hooghiemstra, A.M.; Raijmakers, P.G.; van Berckel, B.N.; Scheltens, P.; Scherder, E.J.; van der Flier, W.M.; Ossenkoppele, R. The effect of physical activity on cognitive function in patients with de-mentia: A meta-analysis of randomized control trials. Aging Res. Rev. 2016, 25, 13–23. [Google Scholar] [CrossRef]
- Tan, Z.S.; Spartano, N.; Beiser, A.; DeCarli, C.; Auerbach, S.H.; Vasan, R.S.; Seshadri, S. Physical Activity, Brain Volume, and Dementia Risk: The Framingham Study. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2016, 72, 789–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Quervain, D.J.; Aerni, A.; Schelling, G.; Roozendaal, B. Glucocorticoids and the regulation of memory in health and disease. Front. Neuroendocrinol. 2009, 30, 358–370. [Google Scholar] [CrossRef]
- Lupien, S.; Maheu, F.; Tu, M.; Fiocco, A.; Schramek, T. The effects of stress and stress hormones on human cognition: Implications for the field of brain and cognition. Brain Cogn. 2007, 65, 209–237. [Google Scholar] [CrossRef] [Green Version]
- James, B.D. Social Engagement and Cognitive Decline in Older Adults: Pathways and Neighborhood Context; The Johns Hopkins University: Ann Arbor, MI, USA, 2009; p. 188. [Google Scholar]
- Marioni, R.E.; Proust-Lima, C.; Amieva, H.; Brayne, C.; Matthews, F.E.; Dartigues, J.F.; Jacqmin-Gadda, H. Social activity, cognitive decline and dementia risk: A 20-year prospective co-hort study. BMC Public Health 2015, 15, 1089. [Google Scholar] [CrossRef] [Green Version]
- Krueger, K.R.; Wilson, R.S.; Kamenetsky, J.M.; Barnes, L.L.; Bienias, J.L.; Bennett, D.A. Social Engagement and Cognitive Function in Old Age. Exp. Aging Res. 2009, 35, 45–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilker, E.H.; Preis, S.R.; Beiser, A.S.; Wolf, P.A.; Au, R.; Kloog, I.; Li, W.; Schwartz, J.; Koutrakis, P.; DeCarli, C.; et al. Long-term exposure to fine particulate matter, residential proximity to major roads and measures of brain structure. Stroke 2015, 46, 1161–1166. [Google Scholar] [CrossRef] [Green Version]
- Besser, L.M.; McDonald, N.C.; Song, Y.; Kukull, W.A.; Rodriguez, D.A. Neighborhood Environment and Cognition in Older Adults: A Systematic Review. Am. J. Prev. Med. 2017, 53, 241–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besser, L.M.; Rodriguez, D.A.; McDonald, N.; Kukull, W.A.; Fitzpatrick, A.L.; Rapp, S.R.; Seeman, T. Neighborhood built environment and cognition in non-demented older adults: The Multi-Ethnic Study of Atherosclerosis. Soc. Sci. Med. 2018, 200, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.P.; Nyunt, M.S.Z.; Shuvo, F.K.; Eng, J.Y.; Yap, K.B.; Hee, L.M.; Chan, S.P.; Scherer, S. The Neighborhood Built Environment and Cognitive Function of Older Persons: Results from the Singapore Longitudinal Ageing Study. Gerontology 2018, 64, 149–156. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Nakaya, T.; McCormack, G.R.; Shibata, A.; Ishii, K.; Yasunaga, A.; Oka, K. Cognitive Function of Elderly Persons in Japanese Neighborhoods: The Role of Street Layout. Am. J. Alzheimer’s Dis. Other Dement. 2019, 34, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-C.; Li, C.-Y.; Kung, S.-F.; Kuo, H.-W.; Huang, N.-C.; Sun, Y.; Hu, S.C. Association of Environmental Features and the Risk of Alzheimer’s Dementia in Older Adults: A Nationwide Longitudinal Case-Control Study. Int. J. Environ. Res. Public Health 2019, 16, 2828. [Google Scholar] [CrossRef] [Green Version]
- Tani, Y.; Suzuki, N.; Fujiwara, T.; Hanazato, M.; Kondo, K. Neighborhood Food Environment and Dementia Incidence: The Japan Gerontological Evaluation Study Cohort Survey. Am. J. Prev. Med. 2019, 56, 383–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Department of Health and Human Services. Social Determinants of Health. Available online: https://health.gov/healthypeople/objectives-and-data/social-determinants-health (accessed on 24 April 2021).
- Bild, D.E.; Bluemke, D.A.; Burke, G.L.; Detrano, R.; Roux, A.V.D.; Folsom, A.R.; Greenland, P.; Jacobs, D.R., Jr.; Kronmal, R.A.; Liu, K.; et al. Multi-Ethnic Study of Atherosclerosis: Objectives and Design. Am. J. Epidemiol. 2002, 156, 871–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiyoshi, A.; Jacobs, D.R.; Alonso, A.; Luchsinger, J.A.; Rapp, S.R.; Duprez, D.A. Validity of Death Certificate and Hospital Discharge ICD Codes for Dementia Diag-nosis: The Multi-Ethnic Study of Atherosclerosis. Alzheimer Dis. Assoc. Disord. 2016, 31, 168–172. [Google Scholar] [CrossRef]
- Jian, Z.-H.; Li, C.-P.; Chiu, E.-C. Ecological, convergent, and discriminative validities of the cognitive abilities screening instrument in people with dementia. Medicine 2021, 100, e25225. [Google Scholar] [CrossRef]
- Teng, E.L.; Hasegawa, K.; Homma, A.; Imai, Y.; Larson, E.; Graves, A.; Sugimoto, K.; Yamaguchi, T.; Sasaki, H.; Chiu, D.; et al. The Cognitive Abilities Screening Instrument (CASI): A Practical Test for Cross-Cultural Epidemiological Studies of Dementia. Int. Psychogeriatr. 1994, 6, 45–58. [Google Scholar] [CrossRef]
- González-Blanch, C.; Pérez-Iglesias, R.; Rodríguez-Sánchez, J.M.; Pardo-García, G.; Martínez-García, O.; Vázquez-Barquero, J.L.; Crespo-Facorro, B. A Digit Symbol Coding Task as a Screening Instrument for Cognitive Impairment in First-Episode Psychosis. Arch. Clin. Neuropsychol. 2010, 26, 48–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wechsler, D. Wechsler Adult Intelligence Scale; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Besser, L.; Galvin, J.E.; Rodriguez, D.; Seeman, T.; Kukull, W.; Rapp, S.R.; Smith, J. Associations between neighborhood built environment and cognition vary by apolipoprotein E genotype: Multi-Ethnic Study of Atherosclerosis. Health Place 2019, 60, 102188. [Google Scholar] [CrossRef] [PubMed]
- Diez Roux, A.V.; Mujahid, M.S.; Hirsch, J.A.; Moore, K.; Moore, L.V. The Impact of Neighborhoods on CV Risk. Glob. Heart 2016, 11, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, D.A.; Evenson, K.R.; Diez Roux, A.V.; Brines, S.J. Land use, residential density, and walking. The multi-ethnic study of ath-erosclerosis. Am. J. Prev. Med. 2009, 37, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talen, E. Visualizing Fairness: Equity Maps for Planners. J. Am. Plan. Assoc. 1998, 64, 22–38. [Google Scholar] [CrossRef]
- Unger, E.; Diez-Roux, A.V.; Lloyd-Jones, D.; Mujahid, M.S.; Nettleton, J.A.; Bertoni, A.; Badon, S.E.; Ning, H.; Allen, N.B. Association of Neighborhood Characteristics With Cardiovascular Health in the Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Albrecht, S.S.; Osypuk, T.; Kandula, N.R.; Gallo, L.C.; Scherban, F.L.-; Shrager, S.; Roux, A.V.D. Change in waist circumference with longer time in the United States among Hispanic and Chinese immigrants: The modifying role of the neighborhood built environment. Ann. Epidemiol. 2015, 25, 767–772.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoehner, C.M.; Schootman, M. Concordance of Commercial Data Sources for Neighborhood-Effects Studies. J. Hered. 2010, 87, 713–725. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; Cholerton, B.A.; et al. Effects of aerobic exercise on mild cognitive impairment: A controlled trial. Arch. Neurol. 2010, 67, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magaziner, J.; Cadigan, D.A. Community Resources and Mental Health of Older Women Living Alone. J. Aging Health 1989, 1, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.J.; Ailshire, J.A.; House, J.S.; Morenoff, J.D.; King, K.; Melendez, R.; Langa, K.M. Cognitive function in the community setting: The neighbourhood as a source of ’cogni-tive reserve’? J. Epidemiol. Community Health 2012, 66, 730–736. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic a | n = 1816 |
|---|---|
| Age at Exam 5, mean (SD) | |
| <60 years | 372 (20.5%) |
| 60–64 years | 430 (23.7%) |
| 65–69 years | 321 (17.7%) |
| 70–74 years | 283 (15.6%) |
| 75–79 years | 266 (14.7%) |
| 80 years or older | 144 (7.9%) |
| Female, n (%) | 957 (52.7%) |
| Education, n (%) | |
| <High school degree | 165 (9.1%) |
| High school degree | 280 (15.5%) |
| Some college, no bachelor’s degree | 550 (30.4%) |
| Bachelor’s degree or higher | 816 (45.1%) |
| Married, n (%) | 1172 (65.2%) |
| Race/ethnicity, n (%) | |
| White/Caucasian | 795 (43.8%) |
| Chinese-American | 192 (10.6%) |
| Black/African American | 521 (28.7%) |
| Hispanic | 308 (17.0%) |
| Family income ≥ $30,000/year, n (%) | 1392 (74.9%) |
| Own car, n (%) | 1578 (87.8%) |
| ≥1 APOE ε4 allele, n (%) | 466 (27.1%) |
| Depressive symptoms (CES-D score ≥ 16), n (%) | 224 (12.5%) |
| Current smoker, n (%) | 114 (6.3%) |
| Obese (body mass index ≥ 30 kg/m2), n (%) | 650 (35.8%) |
| Diabetes (self-reported), n (%) | 164 (9.09) |
| Hypertension (taking medication), n (%) | 905 (49.8%) |
| Taking depression medication, n (%) | 229 (12.6%) |
| Arthritis (self-reported), n (%) | 526 (29.3%) |
| Cardiovascular disease, n (%) | 104 (5.7%) |
| Cerebrovascular disease (stroke/TIA), n (%) | 38 (2.1%) |
| Frequently walk places (≥7 h/week), n (%) | 529 (29.2%) |
| MET-minutes moderate/vigorous physical activity/week, mean (SD) | 5783.6 (6564.3) |
| Number of moves, Exam 1 to Exam 5, mean (SD) | 0.47 (0.89) |
| None | 1269 (69.9%) |
| One | 369 (20.3%) |
| Two or more | 178 (9.8%) |
| Years between Exam 5 and Exam 6 | 6.3 (0.5) |
| Score Measure a | |
|---|---|
| Exam 5 cognitive test score, mean (SD) | |
| CASI (possible range: 0–100) | 90.0 (6.8) |
| DSC (possible range: 0–133) | 55.4 (16.8) |
| Change in cognitive test score, Exam 5 to 6, mean (SD) | |
| CASI | 0.027 (1.012) |
| DSC | −0.728 (1.823) |
| Categorical change in CASI score, Exam 5 to 6, n (%) | |
| No change or increase in score | 947 (52.2%) |
| Decrease in score | 869 (47.9%) |
| Categorical change in DSC score, Exam 5 to 6, n (%) | |
| No change or increase in score | 551 (30.3%) |
| Decrease in score | 1265 (69.7%) |
| Neighborhood Characteristic a | Mean (SD) | Range: Lowest, Highest |
|---|---|---|
| Measured at Exam 5 | ||
| Social destination density b | 132.5 (217.2) | 0, 1604.3 |
| Walking destination density b | 60.0 (101.4) | 0, 716.3 |
| Network ratio b | 0.426 (0.183) | 0.043, 0.801 |
| Proportion retail b | 0.04 (0.05) | 0.00, 0.30 |
| Neighborhood socioeconomic status c,d | −0.52 (1.20) | −4.22, 2.50 |
| Population density a | 6462 (9474) | 11, 54483 |
| Average annual change, Exam 1 to 5 | ||
| Social destination density a | 2.8 (10.4) | −121.7, 111.7 |
| Walking destination density a | −0.5 (4.8) | −83.0, 49.5 |
| Network ratio a | −0.001 (0.013) | −0.069, 0.061 |
| Proportion retail a | −0.002 (0.007) | −0.067, 0.0312 |
| At Exam 5 a | Maintained/Improved CASI Score b,c | Maintained/Improved DSC Score b,c | |||
|---|---|---|---|---|---|
| Buffer Size | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Social destination density (per 100) | ½-mile | 1.00 (0.99, 1.01) | 0.98 | 1.00 (1.00, 1.01) | 0.13 |
| Walking destination density (per 100) | ½-mile | 1.00 (0.98, 1.02) | 0.81 | 1.02 (1.00, 1.03) | 0.07 |
| Network ratio | ½-mile | 0.99 (0.83,1.17) | 0.89 | 0.95 (0.81,1.10) | 0.47 |
| Proportion retail | ½-mile | 1.19 (0.59,2.40) | 0.63 | 1.83 (0.98, 3.42) | 0.06 |
| Social destination density (per 100) | 1-mile | 1.00 (0.99, 1.01) | 0.96 | 1.01 (1.00, 1.02) | 0.09 |
| Walking destination density (per 100) | 1-mile | 1.00 (1.00, 1.03) | 0.83 | 1.03 (1.00, 1.05) | 0.02 |
| Network ratio | 1-mile | 1.05 (0.86, 1.26) | 0.64 | 0.95 (0.81, 1.13) | 0.56 |
| Proportion retail | 1-mile | 1.57 (0.55, 4.43) | 0.40 | 1.74 (0.69, 4.36) | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Besser, L.M.; Chang, L.-C.; Hirsch, J.A.; Rodriguez, D.A.; Renne, J.; Rapp, S.R.; Fitzpatrick, A.L.; Heckbert, S.R.; Kaufman, J.D.; Hughes, T.M. Longitudinal Associations between the Neighborhood Built Environment and Cognition in US Older Adults: The Multi-Ethnic Study of Atherosclerosis. Int. J. Environ. Res. Public Health 2021, 18, 7973. https://doi.org/10.3390/ijerph18157973
Besser LM, Chang L-C, Hirsch JA, Rodriguez DA, Renne J, Rapp SR, Fitzpatrick AL, Heckbert SR, Kaufman JD, Hughes TM. Longitudinal Associations between the Neighborhood Built Environment and Cognition in US Older Adults: The Multi-Ethnic Study of Atherosclerosis. International Journal of Environmental Research and Public Health. 2021; 18(15):7973. https://doi.org/10.3390/ijerph18157973
Chicago/Turabian StyleBesser, Lilah M., Lun-Ching Chang, Jana A. Hirsch, Daniel A. Rodriguez, John Renne, Stephen R. Rapp, Annette L. Fitzpatrick, Susan R. Heckbert, Joel D. Kaufman, and Timothy M. Hughes. 2021. "Longitudinal Associations between the Neighborhood Built Environment and Cognition in US Older Adults: The Multi-Ethnic Study of Atherosclerosis" International Journal of Environmental Research and Public Health 18, no. 15: 7973. https://doi.org/10.3390/ijerph18157973
APA StyleBesser, L. M., Chang, L. -C., Hirsch, J. A., Rodriguez, D. A., Renne, J., Rapp, S. R., Fitzpatrick, A. L., Heckbert, S. R., Kaufman, J. D., & Hughes, T. M. (2021). Longitudinal Associations between the Neighborhood Built Environment and Cognition in US Older Adults: The Multi-Ethnic Study of Atherosclerosis. International Journal of Environmental Research and Public Health, 18(15), 7973. https://doi.org/10.3390/ijerph18157973