
Behavioural Improvements in Children with Autism Spectrum Disorder after Participation in an Adapted Judo Programme Followed by Deleterious Effects during the COVID-19 Lockdown


 ,
,  ,
,  and
and 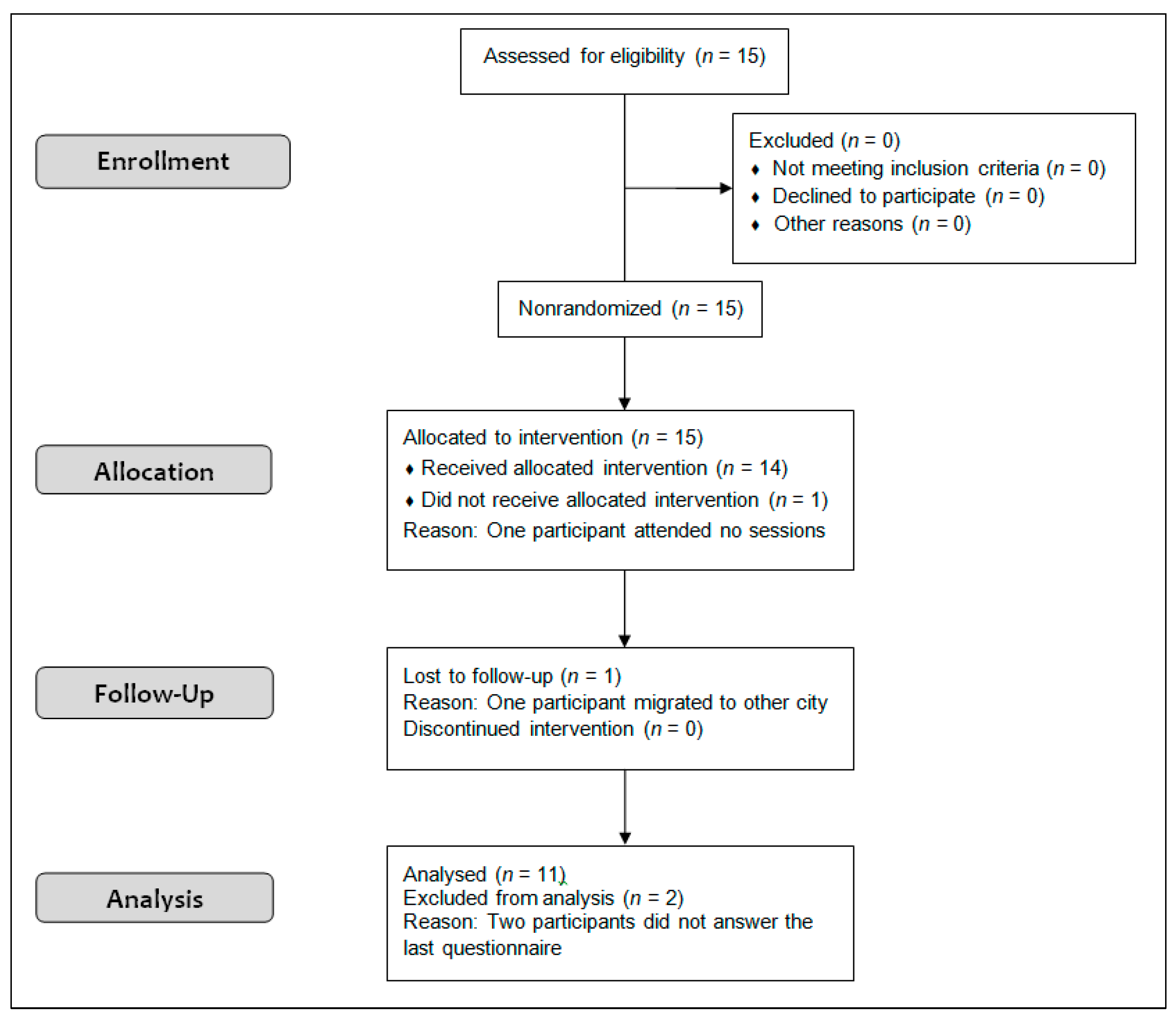{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
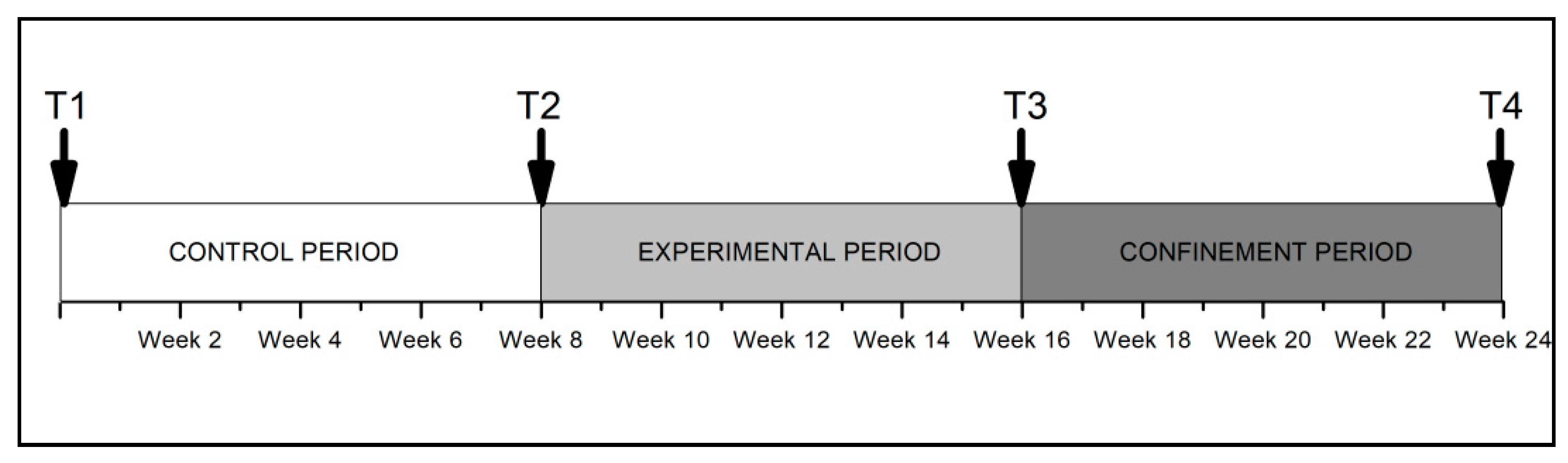
2.2. Procedure
2.3. Intervention
- Different types of movements and falling techniques (from walking in all directions to turning around, from stable movements to unstable movements).
- Judo techniques and opposition games (building up body contact with games, teaching simplified movements, basic judo movements).
- Ground control techniques and throws (gradually adding techniques to already known movements, scaffolding basic repetitive movements to assist in understanding those more relevant for judo).
- Repetition of different forms of foundational directional movements (pulling, pushing, holding, lifting).
2.4. Instruments
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bricout, V.-A.; Pace, M.; Dumortier, L.; Baillieul, F.; Favre-Juvin, A.; Guinot, M. Reduced Cardiorespiratory Capacity in Children with Autism Spectrum Disorders. J. Clin. Med. 2018, 7, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healy, S.; Haegele, J.A.; Grenier, M.; Garcia, J.M. Physical activity, screen-time behavior, and obesity among 13-year olds in Ireland with and without autism spectrum disorder. J. Autism Dev. Disord. 2017, 47, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.-Y. Motor proficiency and physical fitness in adolescent males with and without autism spectrum disorders. Autism 2014, 18, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Tyler, K.; MacDonald, M.; Menear, K. Physical activity and physical fitness of school-aged children and youth with autism spectrum disorders. Autism Res. Treat. 2014, 2014, 312163. [Google Scholar] [CrossRef]
- Sam, K.-L.; Chow, B.-C.; Tong, K.-K. Effectiveness of exercise-based interventions for children with autism: A systematic review and meta-analysis. Int. J. Learn. Teach. 2015, 1, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Sowa, M.; Meulenbroek, R. Effects of physical exercise on autism spectrum disorders: A meta-analysis. Res. Autism Spectr. Disord. 2012, 6, 46–57. [Google Scholar] [CrossRef]
- Howells, K.; Sivaratnam, C.; May, T.; Lindor, E.; McGillivray, J.; Rinehart, N. Efficacy of Group-Based Organised Physical Activity Participation for Social Outcomes in Children with Autism Spectrum Disorder: A Systematic Review and Meta-analysis. J. Autism Dev. Disord. 2019, 49, 3290–3308. [Google Scholar] [CrossRef] [PubMed]
- Healy, S.; Nacario, A.; Braithwaite, R.E.; Hopper, C. The effect of physical activity interventions on youth with autism spectrum disorder: A meta-analysis. Autism Res. 2018, 11, 818–833. [Google Scholar] [CrossRef]
- Bremer, E.; Crozier, M.; Lloyd, M. A systematic review of the behavioural outcomes following exercise interventions for children and youth with autism spectrum disorder. Autism 2016, 20, 899–915. [Google Scholar] [CrossRef]
- McCoy, S.M.; Jakicic, J.M.; Gibbs, B.B. Comparison of obesity, physical activity, and sedentary behaviors between adolescents with autism spectrum disorders and without. J. Autism Dev. Disord. 2016, 46, 2317–2326. [Google Scholar] [CrossRef]
- Stanish, H.; Curtin, C.; Must, A.; Phillips, S.; Maslin, M.; Bandini, L. Enjoyment, barriers, and beliefs about physical activity in adolescents with and without autism spectrum disorder. Adapt. Phys. Act. Q. 2015, 32, 302–317. [Google Scholar] [CrossRef] [PubMed]
- Duffy, L.; Baluch, B.; Welland, S.; Raman, E. Effects of physical activity on debilitating behaviours in 13-to 20-year-old males with severe autism spectrum disorder. J. Exerc. Rehabil. 2017, 13, 340. [Google Scholar] [CrossRef]
- Najafabadi, M.G.; Sheikh, M.; Hemayattalab, R.; Memari, A.-H.; Aderyani, M.R.; Hafizi, S. The effect of SPARK on social and motor skills of children with autism. Pediatr. Neonatol. 2018, 59, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Shanok, N.A.; Sotelo, M.; Hong, J. Brief Report: The Utility of a Golf Training Program for Individuals with Autism Spectrum Disorder. J. Autism Dev. Disord. 2019, 49, 4691–4697. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Chen, S. The effects of structured physical activity program on social interaction and communication for children with autism. Biomed Res. Int. 2018, 2018, 1825046. [Google Scholar] [CrossRef]
- Zanobini, M.; Solari, S. Effectiveness of the Program “Acqua Mediatrice di Comunicazione”(Water as a Mediator of Communication) on Social Skills, Autistic Behaviors and Aquatic Skills in ASD Children. J. Autism Dev. Disord. 2019, 49, 4134–4146. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Todd, T.; Fujii, T.; Lim, J.-C.; Vrongistinos, K.; Jung, T. Effects of Taekwondo intervention on balance in children with autism spectrum disorder. J. Exerc. Rehabil. 2016, 12, 314–319. [Google Scholar] [CrossRef]
- Sarabzadeh, M.; Azari, B.B.; Helalizadeh, M. The effect of six weeks of Tai Chi Chuan training on the motor skills of children with Autism Spectrum Disorder. J. Bodyw. Mov. Ther. 2019, 23, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Movahedi, A.; Bahrami, F.; Marandi, S.M.; Abedi, A. Improvement in social dysfunction of children with autism spectrum disorder following long term Kata techniques training. Res. Autism Spectr. Disord. 2013, 7, 1054–1061. [Google Scholar] [CrossRef]
- Bahrami, F.; Movahedi, A.; Marandi, S.M.; Abedi, A. Kata techniques training consistently decreases stereotypy in children with autism spectrum disorder. Res. Dev. Disabil. 2012, 33, 1183–1193. [Google Scholar] [CrossRef]
- Garcia, J.M.; Leahy, N.; Rivera, P.; Renziehausen, J.; Samuels, J.; Fukuda, D.H.; Stout, J.R. Brief Report: Preliminary Efficacy of a Judo Program to Promote Participation in Physical Activity in Youth with Autism Spectrum Disorder. J. Autism Dev. Disord. 2019, 50, 1418–1424. [Google Scholar] [CrossRef]
- Bell, A.; Allen, M. Using Martial Arts to Address Social and Behavioral Functioning in Children and Adolescents With Autism Spectrum Disorder. Ther. Recreat. J. 2016, 50, 176–181. [Google Scholar] [CrossRef]
- Polak, E.; Sikora, J.; Rachwał, M. An aikido-based intervention supporting the therapy of a child with autism spectrum disorders–a case study. Ido Mov. Cult. J. Martial Arts Anthropol. 2019, 19, 67–76. [Google Scholar]
- Rivera, P.; Renziehausen, J.; Garcia, J.M. Effects of an 8-Week Judo Program on Behaviors in Children with Autism Spectrum Disorder: A Mixed-Methods Approach. Child Psychiatry Hum. Dev. 2020, 51, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Geertz, W.; Dechow, A.-S.; Pohl, E.; Zyriax, B.-C.; Ganschow, R.; Schulz, K.-H. Physical and psychological well-being in overweight children participating in a long-term intervention based on judo practice. Adv. Phys. Educ. 2017, 7, 85. [Google Scholar] [CrossRef] [Green Version]
- Carratalá, V.; Marco-Ahulló, A.; Carratalá, I.; Carratalá, H.; Bermejo, J.-L. Judo as a tool for social integration in adolescents at risk of social exclusion: A pilot study. J. Hum. Sport Exerc. 2019, 15, 202–216. [Google Scholar] [CrossRef]
- Oblak, V.P.; Karpljuk, D.; Vodičar, J.; Šimenko, J. Inclusion of people with intellectual disabilities in judo: A systematic review of literature. Environment 2020, 5, 8. [Google Scholar]
- Srinivasan, S.M.; Pescatello, L.S.; Bhat, A.N. Current perspectives on physical activity and exercise recommendations for children and adolescents with autism spectrum disorders. Phys. Ther. 2014, 94, 875–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naves-Bittencourt, W.; Mendonça-de-Sousa, A.; Stults-Kolehmainen, M.; Fontes, E.; Córdova, C.; Demarzo, M.; Boullosa, D. Martial arts: Mindful exercise to combat stress. Eur. J. Hum. Mov. 2015, 34, 34–51. [Google Scholar]
- Baron, L.J.; Faubert, C. The role of Tai Chi Chuan in reducing state anxiety and enhancing mood of children with special needs. J. Bodyw. Mov. Ther. 2005, 9, 120–133. [Google Scholar] [CrossRef]
- Yukimoto, Y.; Akira, K. Psychological changes in anxiety, enjoyment, and value of learning in junior high school students learning judo. J. Phys. Educ. Sport 2021, 21, 1676–1681. [Google Scholar] [CrossRef]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet. Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Gilliam, J.E. GARS-3: Gilliam Autism Rating Scale, 3rd ed.; Pro-Ed Publishers: Austin, TX, USA, 2014. [Google Scholar]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Heal. Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Hattier, M.A.; Matson, J.L.; Macmillan, K.; Williams, L. Stereotyped behaviours in children with autism spectrum disorders and atypical development as measured by the BPI-01. Dev. Neurorehabil. 2013, 16, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.P.; Ghiarone, T.; Cabral Júnior, C.R.; Furtado, G.E.; Moreira Carvalho, H.; Machado-Rodrigues, A.M.; Toscano, A.; Vasconcelos, C. Effects of Physical Exercise on the Stereotyped Behavior of Children with Autism Spectrum Disorders. Medicina 2019, 55, 685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriels, R.L.; Agnew, J.A.; Holt, K.D.; Shoffner, A.; Zhaoxing, P.; Ruzzano, S.; Clayton, G.H.; Mesibov, G. Pilot study measuring the effects of therapeutic horseback riding on school-age children and adolescents with autism spectrum disorders. Res. Autism Spectr. Disord. 2012, 6, 578–588. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Tureck, K.; Schneiderman, R.L. Autism and exergaming: Effects on repetitive behaviors and cognition. Psychol. Res. Behav. Manag. 2011, 4, 129–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phung, J.N.; Goldberg, W.A. Promoting Executive Functioning in Children with Autism Spectrum Disorder Through Mixed Martial Arts Training. J. Autism Dev. Disord. 2019, 49, 3669–3684. [Google Scholar] [CrossRef]
- Critchley, H.D.; Wiens, S.; Rotshtein, P.; Öhman, A.; Dolan, R.J. Neural systems supporting interoceptive awareness. Nat. Neurosci. 2004, 7, 189–195. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, C.; Zarrett, N. Benefits of physical activity for adolescents with autism spectrum disorders: A comprehensive review. Rev. J. Autism Dev. Disord. 2014, 1, 344–353. [Google Scholar] [CrossRef]
- Pan, C.-Y.; Chu, C.-H.; Tsai, C.-L.; Sung, M.-C.; Huang, C.-Y.; Ma, W.-Y. The impacts of physical activity intervention on physical and cognitive outcomes in children with autism spectrum disorder. Autism 2017, 21, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Gabriels, R.L.; Pan, Z.; Dechant, B.; Agnew, J.A.; Brim, N.; Mesibov, G. Randomized controlled trial of therapeutic horseback riding in children and adolescents with autism spectrum disorder. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Yarımkaya, E.; Esentürk, O.K. Promoting physical activity for children with autism spectrum disorders during Coronavirus outbreak: Benefits, strategies, and examples. Int. J. Dev. Disabil. 2020, 1–6. [Google Scholar] [CrossRef]
- Narzisi, A. Handle the autism spectrum condition during Coronavirus (COVID-19) stay at home period: Ten tips for helping parents and caregivers of young children. Brain Sci. 2020, 10, 207. [Google Scholar] [CrossRef] [Green Version]
- Türkoğlu, S.; Uçar, H.N.; Çetin, F.H.; Güler, H.A.; Tezcan, M.E. The relationship between chronotype, sleep, and autism symptom severity in children with ASD in COVID-19 home confinement period. Chronobiol. Int. 2020, 37, 1207–1213. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales, J.; Fukuda, D.H.; Garcia, V.; Pierantozzi, E.; Curto, C.; Martínez-Ferrer, J.O.; Gómez, A.M.; Carballeira, E.; Guerra-Balic, M. Behavioural Improvements in Children with Autism Spectrum Disorder after Participation in an Adapted Judo Programme Followed by Deleterious Effects during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 8515. https://doi.org/10.3390/ijerph18168515
Morales J, Fukuda DH, Garcia V, Pierantozzi E, Curto C, Martínez-Ferrer JO, Gómez AM, Carballeira E, Guerra-Balic M. Behavioural Improvements in Children with Autism Spectrum Disorder after Participation in an Adapted Judo Programme Followed by Deleterious Effects during the COVID-19 Lockdown. International Journal of Environmental Research and Public Health. 2021; 18(16):8515. https://doi.org/10.3390/ijerph18168515
Chicago/Turabian StyleMorales, Jose, David H. Fukuda, Vanessa Garcia, Emanuela Pierantozzi, Cristina Curto, Josep O. Martínez-Ferrer, Antonia M. Gómez, Eduardo Carballeira, and Myriam Guerra-Balic. 2021. "Behavioural Improvements in Children with Autism Spectrum Disorder after Participation in an Adapted Judo Programme Followed by Deleterious Effects during the COVID-19 Lockdown" International Journal of Environmental Research and Public Health 18, no. 16: 8515. https://doi.org/10.3390/ijerph18168515
APA StyleMorales, J., Fukuda, D. H., Garcia, V., Pierantozzi, E., Curto, C., Martínez-Ferrer, J. O., Gómez, A. M., Carballeira, E., & Guerra-Balic, M. (2021). Behavioural Improvements in Children with Autism Spectrum Disorder after Participation in an Adapted Judo Programme Followed by Deleterious Effects during the COVID-19 Lockdown. International Journal of Environmental Research and Public Health, 18(16), 8515. https://doi.org/10.3390/ijerph18168515