
Breastfeeding after Returning to Work: A Systematic Review and Meta-Analysis


 ,
,
Abstract
:1. Introduction
2. Methods
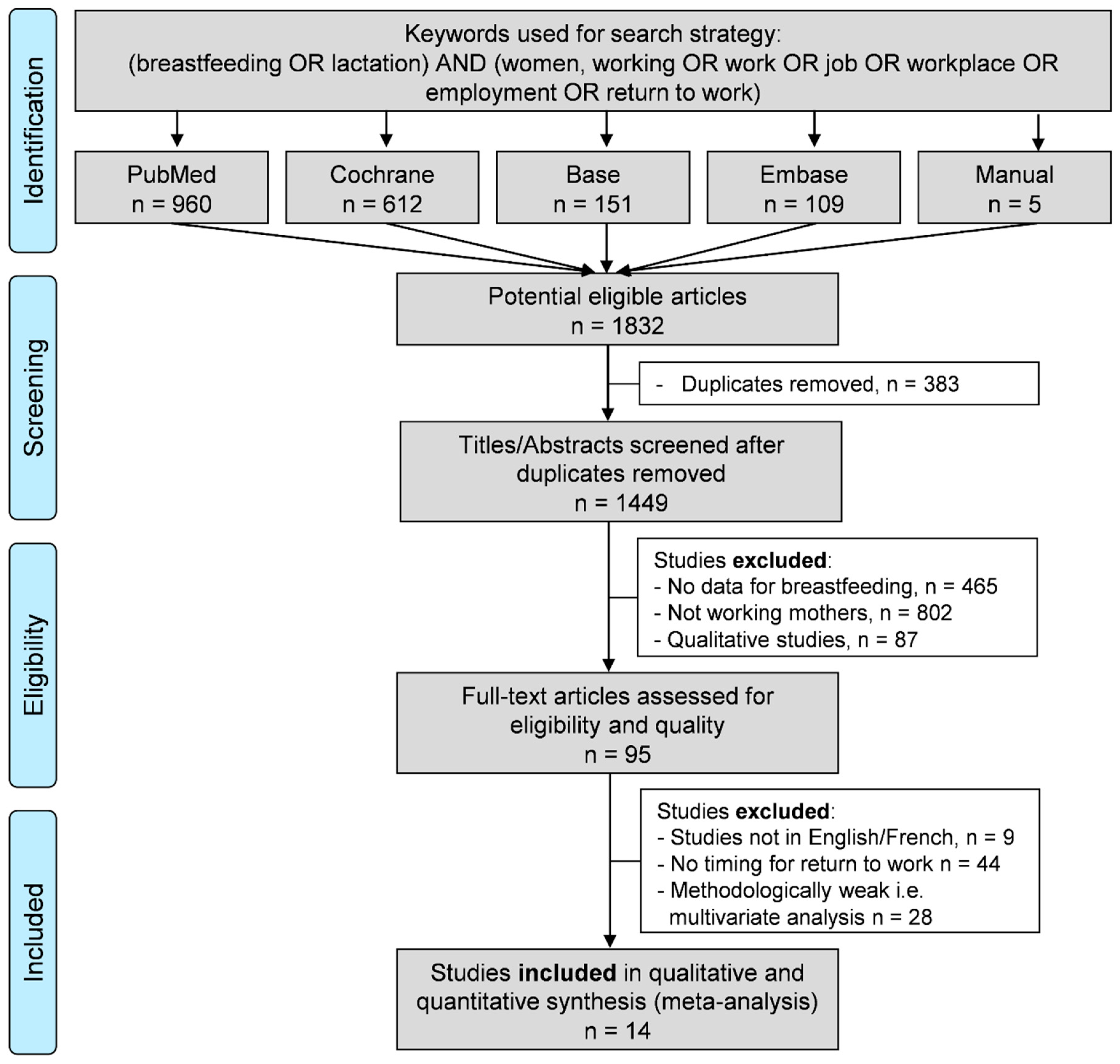
2.1. Literature Search
2.2. Data Collection
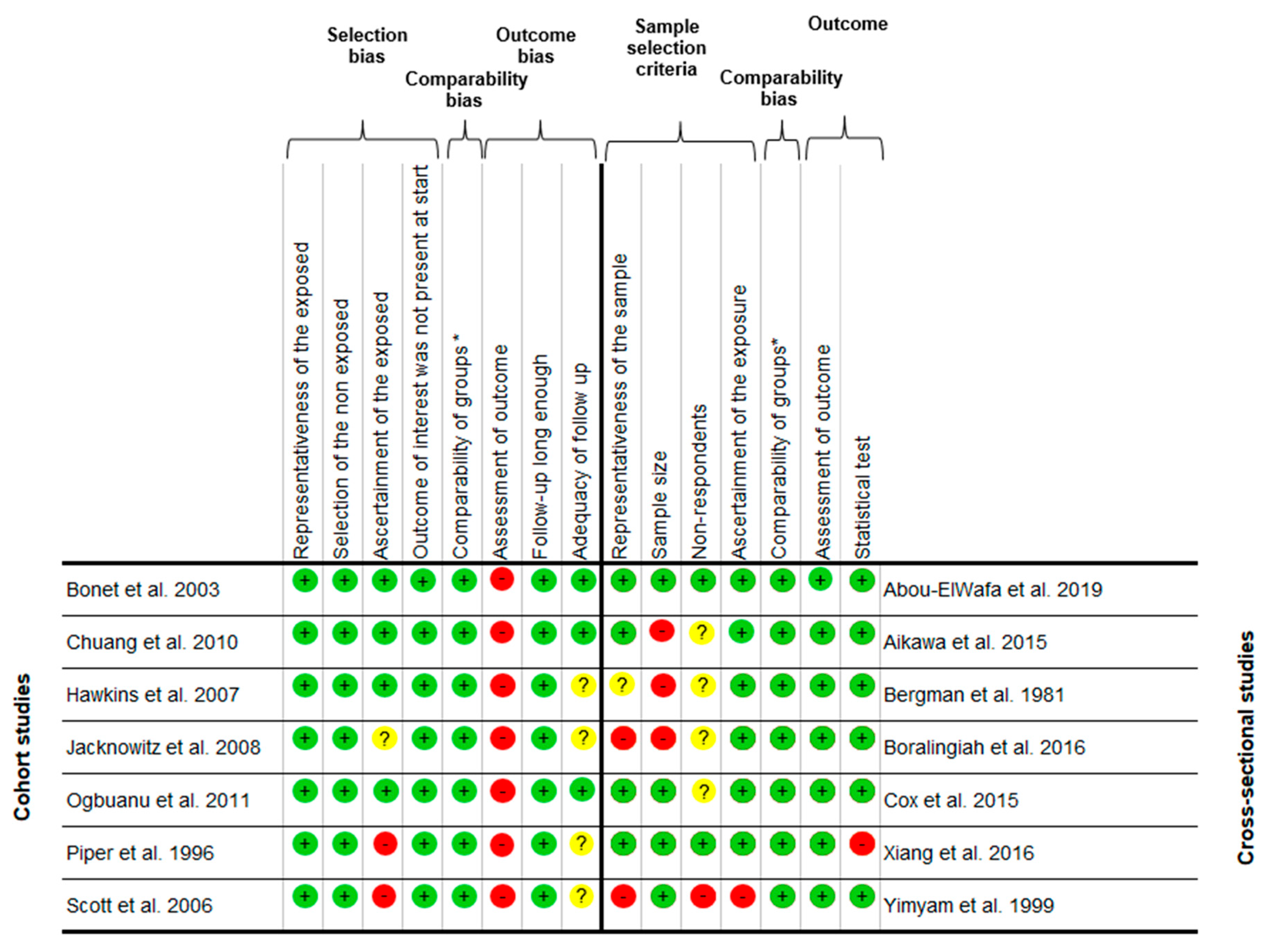
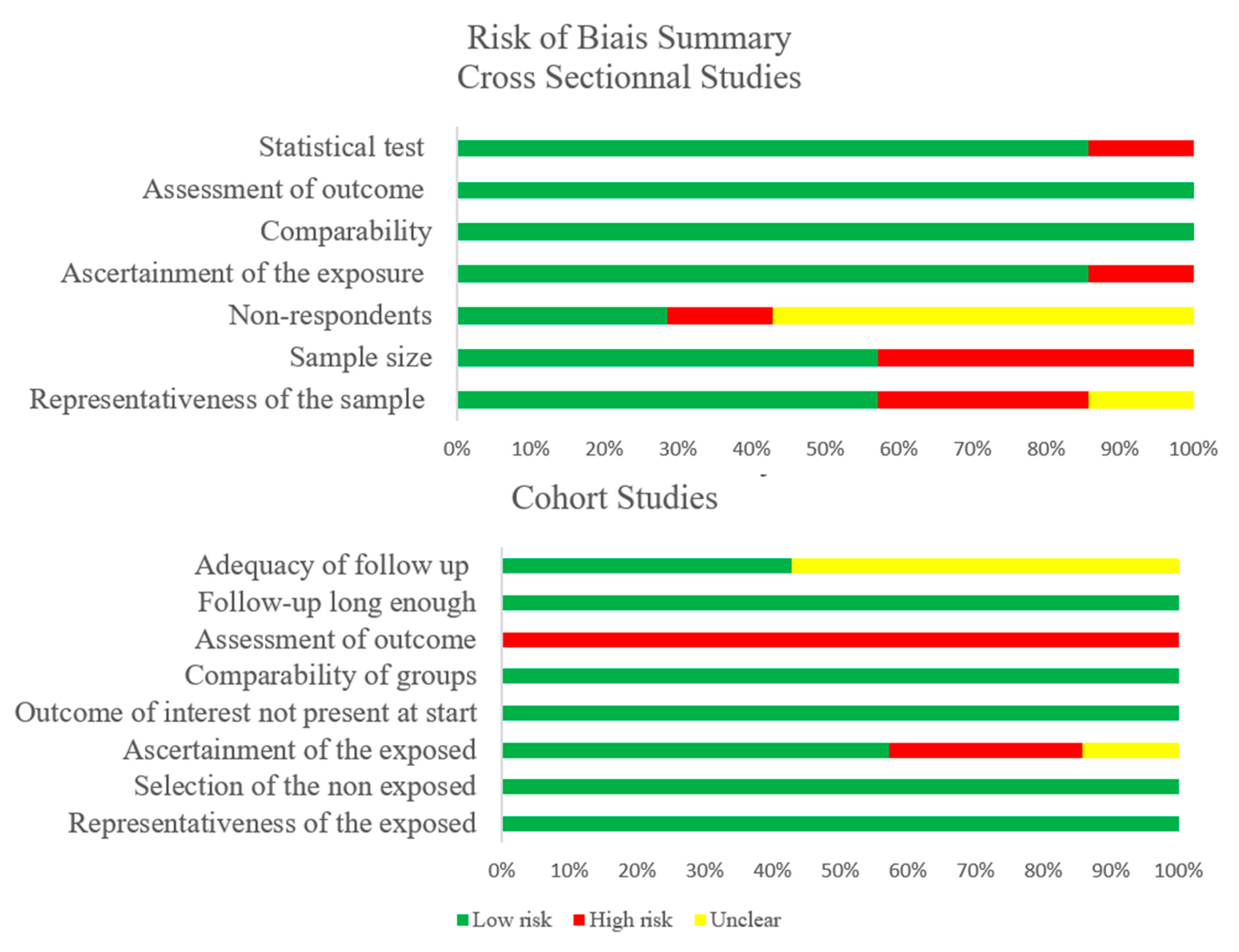
2.3. Quality of Assessment
2.4. Statistical Considerations
3. Results
3.1. Quality of the Articles
3.2. Population
3.3. Inclusion and Exclusion Criteria within the Included Articles
3.4. Outcome and Aim of the Studies
3.5. Study Designs
3.6. Breastfeeding and Return to Work
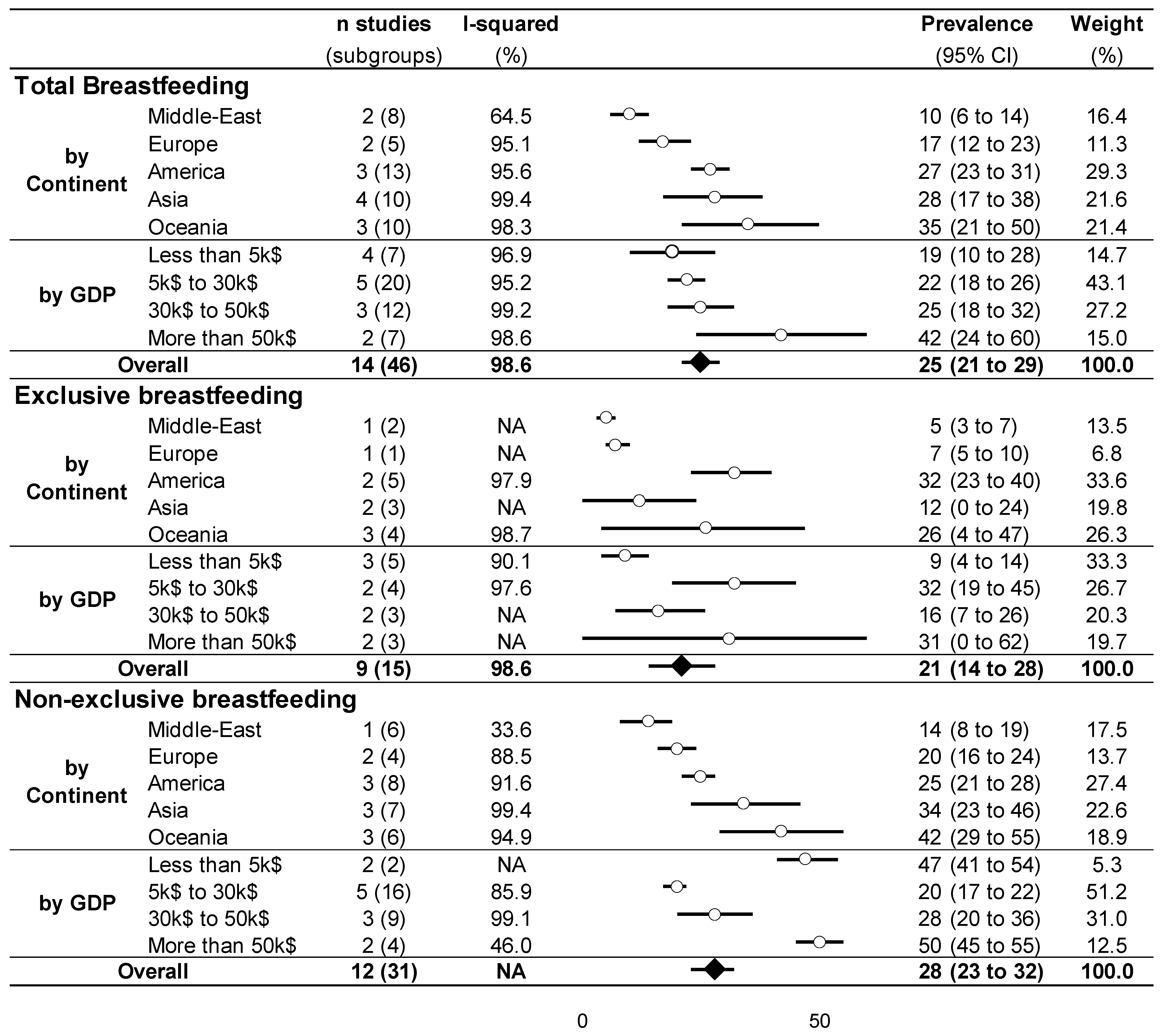
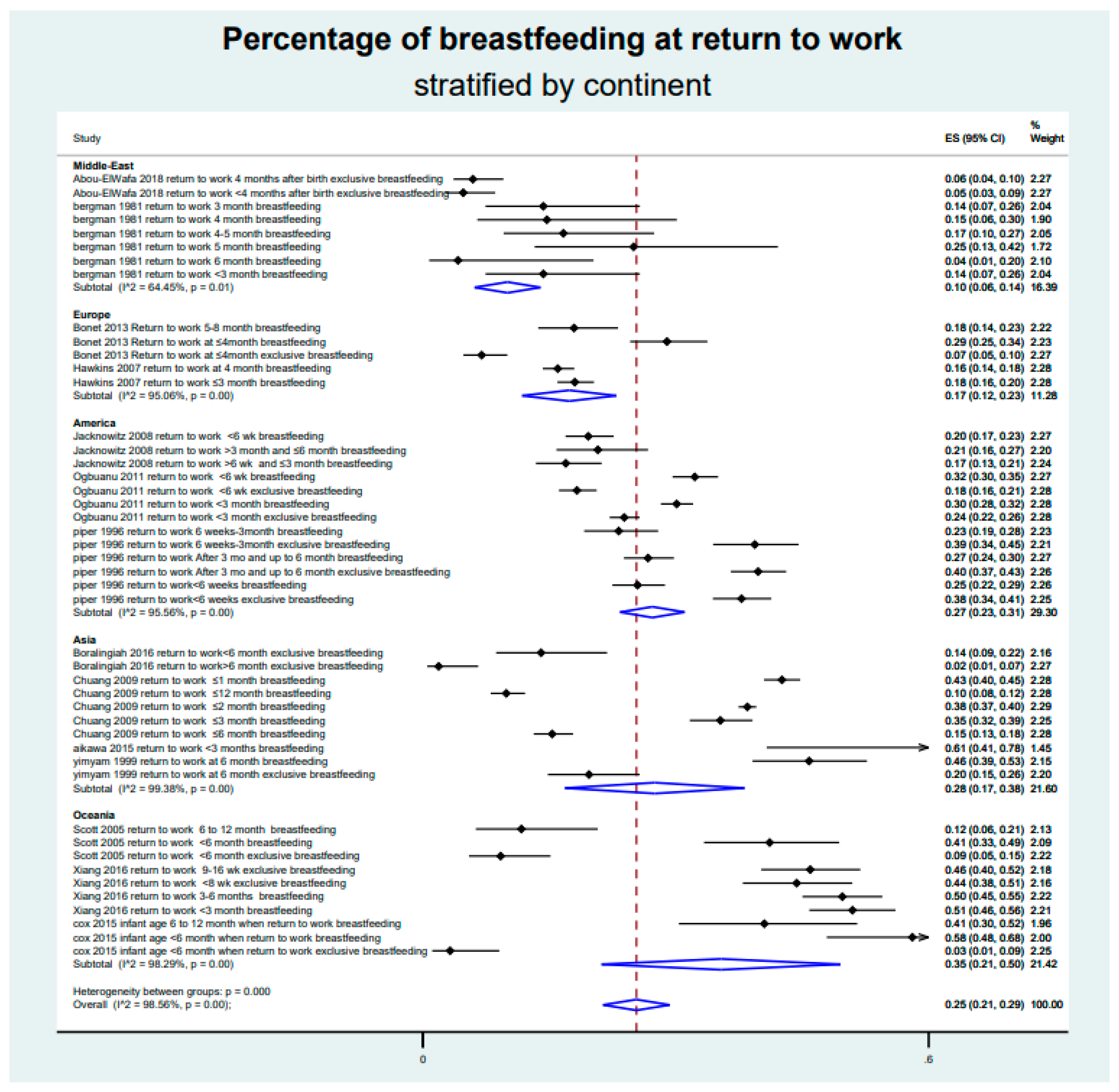
3.7. Meta-Analysis on the Prevalence of Breastfeeding after Returning to Work
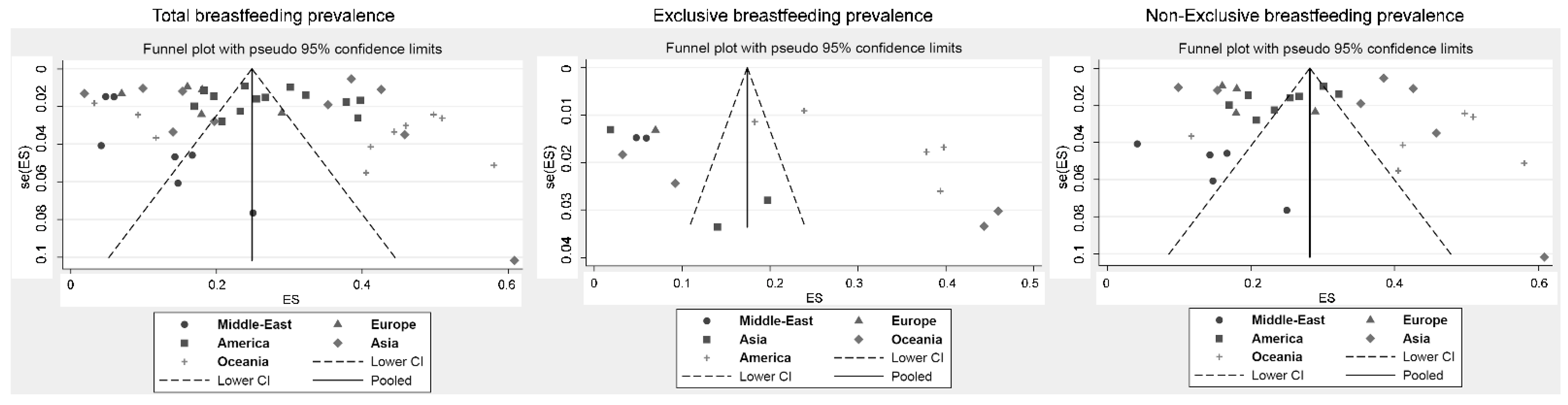
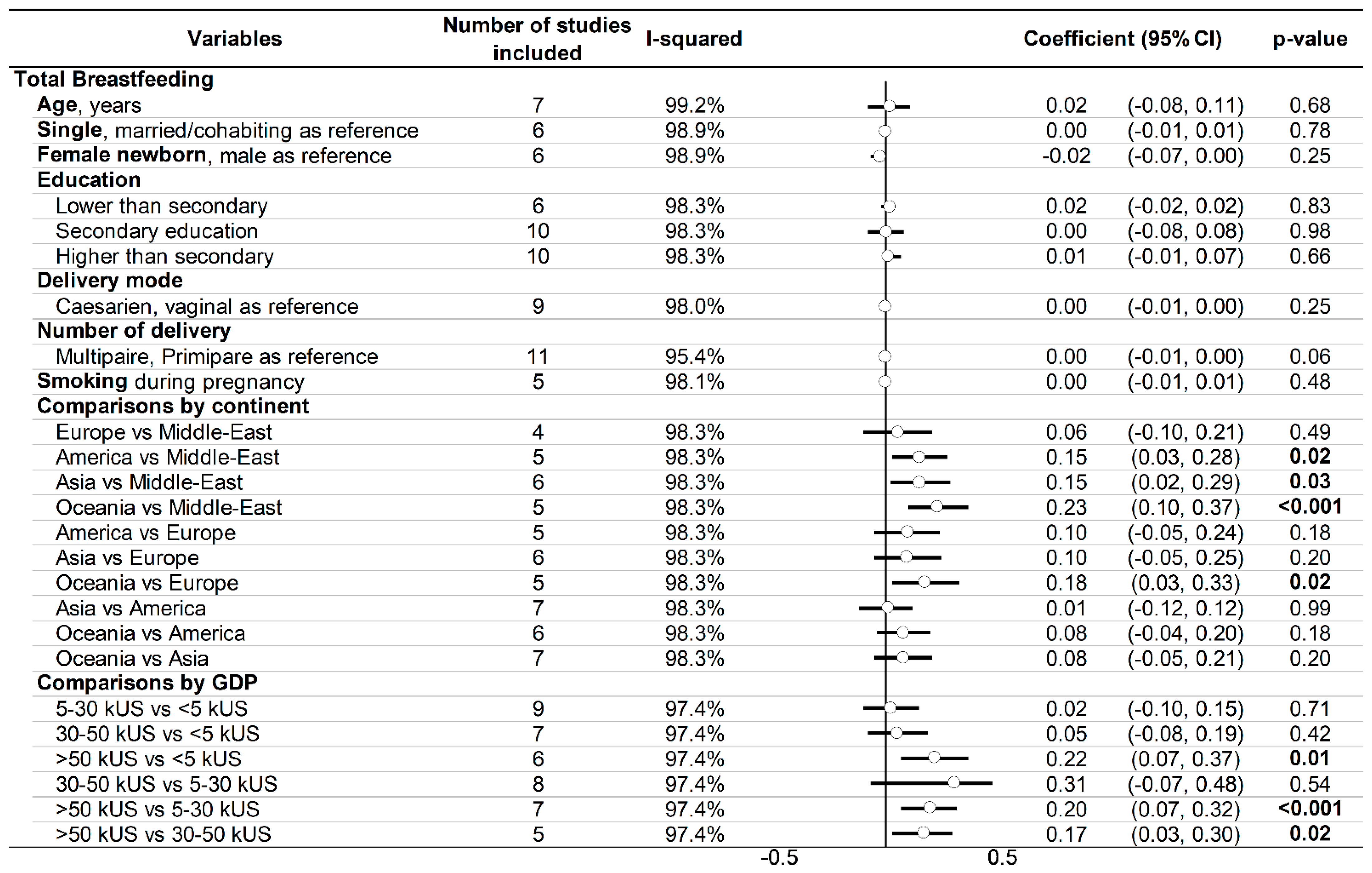
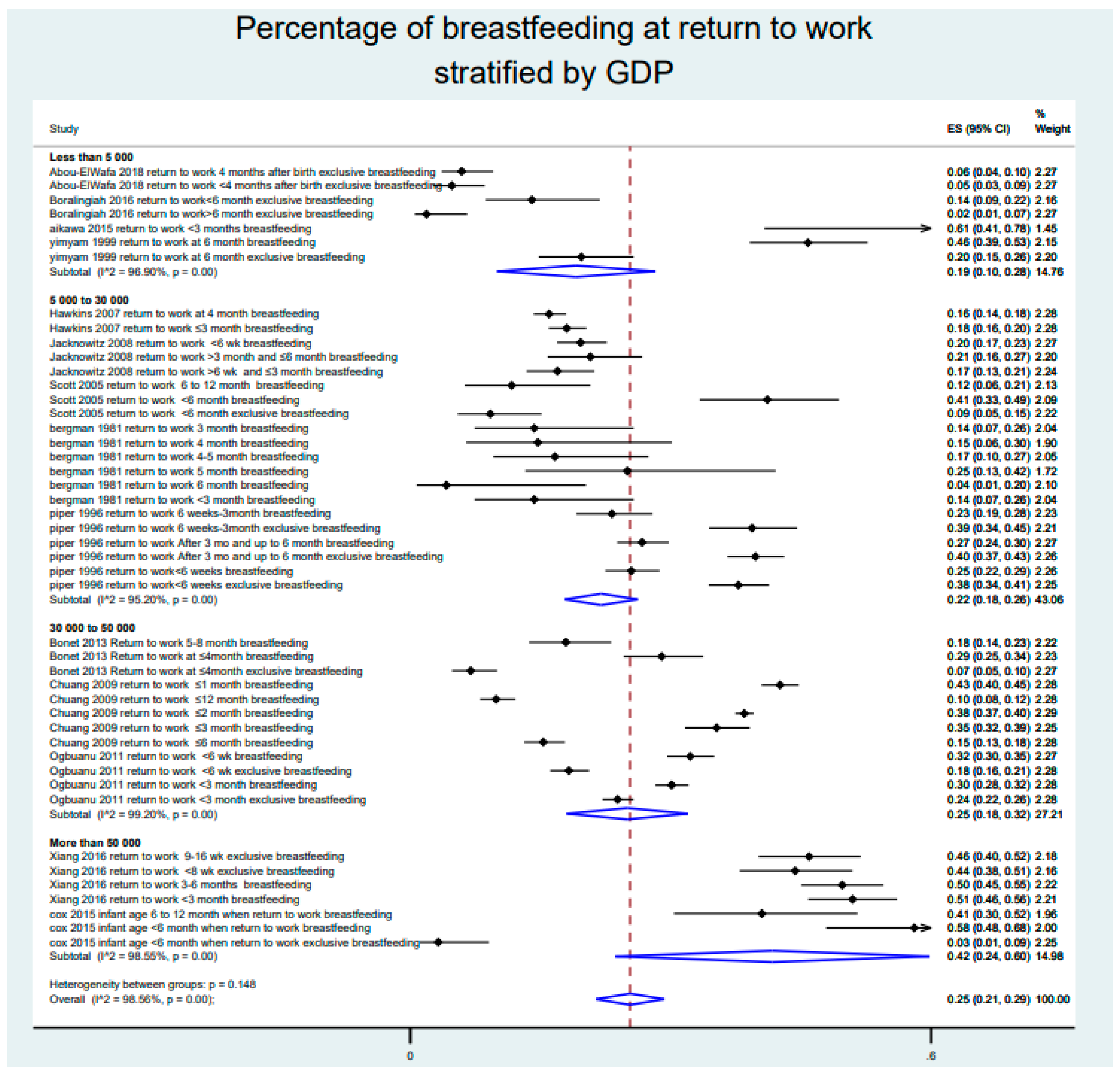
3.8. Sensitivity Analysis and Other Meta-Regressions
4. Discussion
4.1. Breastfeeding around the World
4.2. Cultural Aspect in Breastfeeding
4.3. Other Factors Influencing Breastfeeding after Returning to Work
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Details for the Search Strategy Used within Each Database
Appendix A.2. PRISMA Checklist
| Section/Topic | # | Checklist Item | Reported on Page # |
| TITLE | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | 2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 3 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 3 |
| METHODS | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. | 3–6 |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 3–6 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 3–6 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 3–6 and Figure |
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 3–6 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 3–6 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 3–6 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 3–6 |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | 3–6 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | 3–6 |
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | 3–6 |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | 3–6 |
| RESULTS | |||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 6–10 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 6–10 and Figures |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 6–10 and Figures |
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | 6–10 and Figures |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | 6–10 and Figures |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | 6–10 and Figures |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | 6–10 |
| DISCUSSION | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 10–13 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 14 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 14 |
| FUNDING | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | 15–16 |
Appendix A.3. Quality of the Articles—Newcastle–Ottawa Scale

Appendix A.4. Risk of Bias of the Included Articles Using the Newcastle–Ottawa Quality Assessment Scale

Appendix A.5. Meta-Analysis of the Prevalence of Breastfeeding after Return to Work, Stratified by Continent

Appendix A.6. Meta-Analysis of the Prevalence of Breastfeeding after Return to Work, Stratified by GDP per Capita

References
- Horta, B.L.; de Mola, C.L.; Victora, C.G. Breastfeeding and Intelligence: A Systematic Review and Meta-Analysis. Acta Paediatr. Oslo Nor. 1992 2015, 104, 14–19. [Google Scholar] [CrossRef]
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and Maternal Health Outcomes: A Systematic Review and Meta-Analysis. Acta Paediatr. Oslo Nor. 1992 2015, 104, 96–113. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st Century: Epidemiology, Mechanisms, and Lifelong Effect. Lancet Lond. Engl. 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Turck, D.; Vidailhet, M.; Bocquet, A.; Bresson, J.-L.; Briend, A.; Chouraqui, J.-P.; Darmaun, D.; Dupont, C.; Frelut, M.-L.; Girardet, J.-P.; et al. Breastfeeding: Health benefits for child and mother. Arch. Pediatr. Organe Off. Soc. Francaise Pediatr. 2013, 20 (Suppl. 2), S29–S48. [Google Scholar]
- Ball, T.M.; Bennett, D.M. The Economic Impact of Breastfeeding. Pediatr. Clin. North Am. 2001, 48, 253–262. [Google Scholar] [CrossRef]
- Kendall-Tackett, K.A.; Sugarman, M. The Social Consequences of Long-Term Breastfeeding. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 1995, 11, 179–183. [Google Scholar] [CrossRef]
- Krol, K.M.; Grossmann, T. Psychological Effects of Breastfeeding on Children and Mothers. Bundesgesundh. Gesundh. Gesundh. 2018, 61, 977–985. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report. 2005: Make Every Mother and Child Count; World Health Organization: Geneva, Switzerland, 2005; ISBN 978-92-4-156290-4. [Google Scholar]
- Chatterji, P.; Frick, K.D. Does Returning to Work After Childbirth AffectBreastfeeding Practices? Rev. Econ. Househ. 2005, 3, 315–335. [Google Scholar] [CrossRef]
- Fein, S.B.; Roe, B. The Effect of Work Status on Initiation and Duration of Breast-Feeding. Am. J. Public Health 1998, 88, 1042–1046. [Google Scholar] [CrossRef]
- Ong, G.; Yap, M.; Li, F.L.; Choo, T.B. Impact of Working Status on Breastfeeding in Singapore: Evidence from the National Breastfeeding Survey 2001. Eur. J. Public Health 2005, 15, 424–430. [Google Scholar] [CrossRef]
- Visness, C.M.; Kennedy, K.I. Maternal Employment and Breast-Feeding: Findings from the 1988 National Maternal and Infant Health Survey. Am. J. Public Health 1997, 87, 945–950. [Google Scholar] [CrossRef]
- Lakati, A.; Binns, C.; Stevenson, M. The Effect of Work Status on Exclusive Breastfeeding in Nairobi. Asia. Pac. J. Public Health 2002, 14, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Wang, S. The Role of Gender Role Attitudes and Immigrant Generation in Ethnic Minority Women’s Labor Force Participation in Britain. Sex Roles 2019, 80, 234–245. [Google Scholar] [CrossRef]
- Paul, M. Breastfeeding Practices in Indonesia. Zhonghua Minguo Xiao Er Ke Yi Xue Hui Za Zhi J. 1997, 38, 338–344. [Google Scholar]
- Sriraman, N.K.; Kellams, A. Breastfeeding: What Are the Barriers? Why Women Struggle to Achieve Their Goals. J. Womens Health 2002 2016, 25, 714–722. [Google Scholar] [CrossRef]
- Chen, Y.C.; Wu, Y.-C.; Chie, W.-C. Effects of Work-Related Factors on the Breastfeeding Behavior of Working Mothers in a Taiwanese Semiconductor Manufacturer: A Cross-Sectional Survey. BMC Public Health 2006, 6, 160. [Google Scholar] [CrossRef]
- Lubold, A.M. The Effect of Family Policies and Public Health Initiatives on Breastfeeding Initiation among 18 High-Income Countries: A Qualitative Comparative Analysis Research Design. Int. Breastfeed. J. 2017, 12, 34. [Google Scholar] [CrossRef]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G. Lancet Breastfeeding Series Group Why Invest, and What It Will Take to Improve Breastfeeding Practices? Lancet Lond. Engl. 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Kimbro, R.T. On-the-Job Moms: Work and Breastfeeding Initiation and Duration for a Sample of Low-Income Women. Matern. Child Health J. 2006, 10, 19–26. [Google Scholar] [CrossRef]
- Bonet, M.; L’hélias, L.F.; Blondel, B. Exclusive and mixed breastfeeding in a maternity unit in France, 2003. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2008, 15, 1407–1415. [Google Scholar] [CrossRef]
- Acharya, P.; Khanal, V. The Effect of Mother’s Educational Status on Early Initiation of Breastfeeding: Further Analysis of Three Consecutive Nepal Demographic and Health Surveys. BMC Public Health 2015, 15, 1069. [Google Scholar] [CrossRef] [PubMed]
- Hackman, N.M.; Schaefer, E.W.; Beiler, J.S.; Rose, C.M.; Paul, I.M. Breastfeeding Outcome Comparison by Parity. Breastfeed. Med. 2015, 10, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Kosmala-Anderson, J.; Wallace, L.M. Breastfeeding Works: The Role of Employers in Supporting Women Who Wish to Breastfeed and Work in Four Organizations in England. J. Public Health Oxf. Engl. 2006, 28, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Capra, A.M.; Braveman, P.A.; Jensvold, N.G.; Escobar, G.J.; Lieu, T.A. Clinician Support and Psychosocial Risk Factors Associated with Breastfeeding Discontinuation. Pediatrics 2003, 112, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.; Janson, A.; Nolan, M.; Wen, L.M.; Rissel, C. Female Employees’ Perceptions of Organisational Support for Breastfeeding at Work: Findings from an Australian Health Service Workplace. Int. Breastfeed. J. 2011, 6, 19. [Google Scholar] [CrossRef]
- Scott, J.A.; Binns, C.W. Factors Associated with the Initiation and Duration of Breastfeeding: A Review of the Literature. Breastfeed. Rev. Prof. Publ. Nurs. Mothers Assoc. Aust. 1999, 7, 5–16. [Google Scholar]
- Smith, J.; McIntyre, E.; Craig, L.; Javanparast, S.; Strazdins, L.; Mortensen, K. Workplace Support Breastfeeding and Health. Fam. Matters 2013, 93, 58–73. [Google Scholar]
- Tsai, S.-Y. Impact of a Breastfeeding-Friendly Workplace on an Employed Mother’s Intention to Continue Breastfeeding after Returning to Work. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2013, 8, 210–216. [Google Scholar] [CrossRef]
- Mirkovic, K.R.; Perrine, C.G.; Scanlon, K.S.; Grummer-Strawn, L.M. Maternity Leave Duration and Full-Time/Part-Time Work Status Are Associated with US Mothers’ Ability to Meet Breastfeeding Intentions. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2014, 30, 416–419. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 3 September 2020).
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G. ESH Working Group on CV Risk in Low Resource Settings Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar]
- Ollier, M.; Chamoux, A.; Naughton, G.; Pereira, B.; Dutheil, F. Chest CT Scan Screening for Lung Cancer in Asbestos Occupational Exposure: A Systematic Review and Meta-Analysis. Chest 2014, 145, 1339–1346. [Google Scholar] [CrossRef]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.-X.; Dutheil, F. Creatine Supplementation and Lower Limb Strength Performance: A Systematic Review and Meta-Analyses. Sports Med. Auckl. NZ 2015, 45, 1285–1294. [Google Scholar] [CrossRef]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.-X.; Dutheil, F. Creatine Supplementation and Upper Limb Strength Performance: A Systematic Review and Meta-Analysis. Sports Med. Auckl. NZ 2017, 47, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Navel, V.; Mulliez, A.; Benoist d’Azy, C.; Baker, J.S.; Malecaze, J.; Chiambaretta, F.; Dutheil, F. Efficacy of Treatments for Demodex Blepharitis: A Systematic Review and Meta-Analysis. Ocul. Surf. 2019, 17, 655–669. [Google Scholar] [CrossRef]
- d’Azy, C.B.; Pereira, B.; Naughton, G.; Chiambaretta, F.; Dutheil, F. Antibioprophylaxis in Prevention of Endophthalmitis in Intravitreal Injection: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0156431. [Google Scholar]
- Benichou, T.; Pereira, B.; Mermillod, M.; Tauveron, I.; Pfabigan, D.; Maqdasy, S.; Dutheil, F. Heart Rate Variability in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. PLoS ONE 2018, 13, e0195166. [Google Scholar] [CrossRef] [PubMed]
- Benoist d’Azy, C.; Pereira, B.; Chiambaretta, F.; Dutheil, F. Oxidative and Anti-Oxidative Stress Markers in Chronic Glaucoma: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0166915. [Google Scholar]
- Courtin, R.; Pereira, B.; Naughton, G.; Chamoux, A.; Chiambaretta, F.; Lanhers, C.; Dutheil, F. Prevalence of Dry Eye Disease in Visual Display Terminal Workers: A Systematic Review and Meta-Analysis. BMJ Open 2016, 6, e009675. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Russo, M.W. How to Review a Meta-Analysis. Gastroenterol. Hepatol. 2007, 3, 637–642. [Google Scholar]
- Abou-ElWafa, H.S.; El-Gilany, A.-H. Maternal Work and Exclusive Breastfeeding in Mansoura, Egypt. Fam. Pract. 2019, 36, 568–572. [Google Scholar] [CrossRef]
- Aikawa, T.; Pavadhgul, P.; Chongsuwat, R.; Sawasdivorn, S.; Boonshuyar, C. Maternal Return to Paid Work and Breastfeeding Practices in Bangkok, Thailand. Asia. Pac. J. Public Health 2015, 27, NP1253–NP1262. [Google Scholar] [CrossRef]
- Bergman, R.; Feinberg, D. Working Women and Breastfeeding in Israel. J. Adv. Nurs. 1981, 6, 305–309. [Google Scholar] [CrossRef]
- Bonet, M.; Marchand, L.; Kaminski, M.; Fohran, A.; Betoko, A.; Charles, M.-A.; Blondel, B. “EDEN Mother–Child Cohort Study Group” Breastfeeding Duration, Social and Occupational Characteristics of Mothers in the French “EDEN Mother-Child” Cohort. Matern. Child Health J. 2013, 17, 714–722. [Google Scholar] [CrossRef]
- Boralingiah, P.; Polineni, V.; Kulkarni, P.; Manjunath, R. Study of Breastfeeding Practices among Working Women Attending a Tertiary Care Hospital, Mysore, Karnataka, India. Int. J. Community Med. Public Health 2016, 3, 1178–1182. [Google Scholar] [CrossRef]
- Chuang, C.-H.; Chang, P.-J.; Chen, Y.-C.; Hsieh, W.-S.; Hurng, B.-S.; Lin, S.-J.; Chen, P.-C. Maternal Return to Work and Breastfeeding: A Population-Based Cohort Study. Int. J. Nurs. Stud. 2010, 47, 461–474. [Google Scholar] [CrossRef]
- Cox, K.; Binns, C.W.; Giglia, R. Predictors of Breastfeeding Duration for Rural Women in a High-Income Country: Evidence from a Cohort Study. Acta Paediatr. Oslo Nor. 1992 2015, 104, e350–e359. [Google Scholar] [CrossRef]
- Hawkins, S.S.; Griffiths, L.J.; Dezateux, C.; Law, C. Millennium Cohort Study Child Health Group The Impact of Maternal Employment on Breast-Feeding Duration in the UK Millennium Cohort Study. Public Health Nutr. 2007, 10, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Jacknowitz, A. The Role of Workplace Characteristics in Breastfeeding Practices. Women Health 2008, 47, 87–111. [Google Scholar] [CrossRef] [PubMed]
- Ogbuanu, C.; Glover, S.; Probst, J.; Liu, J.; Hussey, J. The Effect of Maternity Leave Length and Time of Return to Work on Breastfeeding. Pediatrics 2011, 127, e1414–e1427. [Google Scholar] [CrossRef]
- Piper, S.; Parks, P.L. Predicting the Duration of Lactation: Evidence from a National Survey. Birth 1996, 23, 7–12. [Google Scholar] [CrossRef]
- Scott, J.A.; Binns, C.W.; Oddy, W.H.; Graham, K.I. Predictors of Breastfeeding Duration: Evidence from a Cohort Study. Pediatrics 2006, 117, e646–e655. [Google Scholar] [CrossRef]
- Xiang, N.; Zadoroznyj, M.; Tomaszewski, W.; Martin, B. Timing of Return to Work and Breastfeeding in Australia. Pediatrics 2016, 137, e20153883. [Google Scholar] [CrossRef]
- Yimyam, S.; Morrow, M.; Srisuphan, W. Role Conflict and Rapid Socio-Economic Change: Breastfeeding among Employed Women in Thailand. Soc. Sci. Med. 1982 1999, 49, 957–965. [Google Scholar] [CrossRef]
- World Development Indicators | DataBank. Available online: https://databank.worldbank.org/source/world-development-indicators (accessed on 10 September 2020).
- WHO Technical Staff Continued Breastfeeding for Healthy Growth and Development of Children. Available online: http://www.who.int/elena/titles/bbc/continued_breastfeeding/en/ (accessed on 13 September 2020).
- Brown, C.R.L.; Dodds, L.; Legge, A.; Bryanton, J.; Semenic, S. Factors Influencing the Reasons Why Mothers Stop Breastfeeding. Can. J. Public Health Rev. Can. Sante Publique 2014, 105, e179–e185. [Google Scholar] [CrossRef] [PubMed]
- Thomas-Jackson, S.C.; Bentley, G.E.; Keyton, K.; Reifman, A.; Boylan, M.; Hart, S.L. In-Hospital Breastfeeding and Intention to Return to Work Influence Mothers’ Breastfeeding Intentions. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2016, 32, NP76–NP83. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, G.; Martin, N.; Denantes, M.; Saurel-Cubizolles, M.-J.; Ringa, V.; Magnier, A.-M. Prevalence of Breastfeeding in Industrialized Countries. Rev. Epidemiol. Sante Publique 2012, 60, 305–320. [Google Scholar] [CrossRef] [PubMed]
- Walters, D.; Horton, S.; Siregar, A.Y.M.; Pitriyan, P.; Hajeebhoy, N.; Mathisen, R.; Phan, L.T.H.; Rudert, C. The Cost of Not Breastfeeding in Southeast Asia. Health Policy Plan. 2016, 31, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- COAG Health Council Australian National Breastfeeding Strategy 2019 and Beyond. Available online: http://www.coaghealthcouncil.gov.au/Publications/Reports (accessed on 13 September 2020).
- Alzaheb, R.A. A Review of the Factors Associated with the Timely Initiation of Breastfeeding and Exclusive Breastfeeding in the Middle East. Clin. Med. Insights Pediatr. 2017, 11, 1–15. [Google Scholar] [CrossRef]
- Wagner, S.; Kersuzan, C.; Gojard, S.; Tichit, C.; Nicklaus, S.; Thierry, X.; Charles, M.A.; Lioret, S.; de Lauzon-Guillain, B. Breastfeeding Initiation and Duration in France: The Importance of Intergenerational and Previous Maternal Breastfeeding Experiences—Results from the Nationwide ELFE Study. Midwifery 2019, 69, 67–75. [Google Scholar] [CrossRef]
- Negin, J.; Coffman, J.; Vizintin, P.; Raynes-Greenow, C. The Influence of Grandmothers on Breastfeeding Rates: A Systematic Review. BMC Pregnancy Childbirth 2016, 16, 91. [Google Scholar] [CrossRef]
- Knight, C.R.; Brinton, M.C. One Egalitarianism or Several? Two Decades of Gender-Role Attitude Change in Europe. Am. J. Sociol. 2017, 122, 1485–1532. [Google Scholar] [CrossRef]
- McIntyre, E.; Pisaniello, D.; Gun, R.; Sanders, C.; Frith, D. Balancing Breastfeeding and Paid Employment: A Project Targeting Employers, Women and Workplaces. Health Promot. Int. 2002, 17, 215–222. [Google Scholar] [CrossRef]
- Sydney Local Health District Breastfeeding Guidelines. Available online: https://www.cesphn.org.au/images/SLHD_BF_guidelines_2014.pdf (accessed on 13 September 2020).
- South Western Sydney Local Health District a Research Strategy for South Western Sydney Local Health District. Available online: https://www.swslhd.health.nsw.gov.au/planning/content/pdf/researchissuespaper.pdf (accessed on 13 September 2020).
- South Western Sydney Local Health District the Maternal Early Childhood Sustained Home-Visiting (MECSH) Program. Available online: https://www.earlychildhoodconnect.edu.au/home-visiting-programs/mecsh-public/about-mecsh (accessed on 14 September 2020).
- Guendelman, S.; Kosa, J.L.; Pearl, M.; Graham, S.; Goodman, J.; Kharrazi, M. Juggling Work and Breastfeeding: Effects of Maternity Leave and Occupational Characteristics. Pediatrics 2009, 123, e38–e46. [Google Scholar] [CrossRef]
- Ryan, A.S.; Zhou, W.; Arensberg, M.B. The Effect of Employment Status on Breastfeeding in the United States. Womens Health Issues Off. Publ. Jacobs Inst. Womens Health 2006, 16, 243–251. [Google Scholar] [CrossRef]
- Navarro-Rosenblatt, D.; Garmendia, M.-L. Maternity Leave and Its Impact on Breastfeeding: A Review of the Literature. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2018, 13, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Mandal, B.; Roe, B.E.; Fein, S.B. The Differential Effects of Full-Time and Part-Time Work Status on Breastfeeding. Health Policy Amst. Neth. 2010, 97, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Ayton, J.E.; Tesch, L.; Hansen, E. Women’s Experiences of Ceasing to Breastfeed: Australian Qualitative Study. BMJ Open 2019, 9, e026234. [Google Scholar] [CrossRef] [PubMed]
- Hangchaovanich, Y.; Voramongkol, N. Breastfeeding Promotion in Thailand. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2006, 89 (Suppl. 4), S173–S177. [Google Scholar]
- Hmone, M.P.; Li, M.; Alam, A.; Dibley, M.J. Mobile Phone Short Messages to Improve Exclusive Breastfeeding and Reduce Adverse Infant Feeding Practices: Protocol for a Randomized Controlled Trial in Yangon, Myanmar. JMIR Res. Protoc. 2017, 6, e126. [Google Scholar] [CrossRef] [PubMed]
- Health and Human Services Letter. Available online: https://media.washingtonpost.com/wp-srv/health/documents/yeutterletters.pdf (accessed on 14 September 2020).
- Murtagh, L.; Moulton, A.D. Working Mothers, Breastfeeding, and the Law. Am. J. Public Health 2011, 101, 217–223. [Google Scholar] [CrossRef] [PubMed]
- USBC: Healthy People 2020: Breastfeeding Objectives. Available online: http://www.usbreastfeeding.org/p/cm/ld/fid=221 (accessed on 24 September 2020).
- Garvin, C.C.; Sriraman, N.K.; Paulson, A.; Wallace, E.; Martin, C.E.; Marshall, L. The Business Case for Breastfeeding: A Successful Regional Implementation, Evaluation, and Follow-Up. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2013, 8, 413–417. [Google Scholar]
- Noble, S. Maternal Employment and the Initiation of Breastfeeding. Acta Paediatr. 2001, 90, 423–428. [Google Scholar] [CrossRef]
- Skafida, V. Juggling Work and Motherhood: The Impact of Employment and Maternity Leave on Breastfeeding Duration: A Survival Analysis on Growing Up in Scotland Data. Matern. Child Health J. 2012, 16, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Nardi, A.L.; von Frankenberg, A.D.; Franzosi, O.S.; do Espirito Santo, L.C. Impact of institutional aspects on breastfeeding for working women: A systematic review. Cienc. Saude Coletiva 2020, 25, 1445–1462. [Google Scholar] [CrossRef]
- Johnston, M.L.; Esposito, N. Barriers and Facilitators for Breastfeeding among Working Women in the United States. J. Obstet. Gynecol. Neonatal Nurs. Jognn 2007, 36, 9–20. [Google Scholar] [CrossRef]
- Vilar-Compte, M.; Hernández-Cordero, S.; Ancira-Moreno, M.; Burrola-Méndez, S.; Ferre-Eguiluz, I.; Omaña, I.; Pérez Navarro, C. Breastfeeding at the Workplace: A Systematic Review of Interventions to Improve Workplace Environments to Facilitate Breastfeeding among Working Women. Int. J. Equity Health 2021, 20, 110. [Google Scholar] [CrossRef]
- Morilla-Luchena, A.; Muñoz-Moreno, R.; Chaves-Montero, A.; Vázquez-Aguado, O. Telework and Social Services in Spain during the COVID-19 Pandemic. Int. J. Environ. Res. Public. Health 2021, 18, 725. [Google Scholar] [CrossRef]
- Heymann, J.; Raub, A.; Earle, A. Breastfeeding Policy: A Globally Comparative Analysis. Bull. World Health Organ. 2013, 91, 398–406. [Google Scholar] [CrossRef]
- Scott, V.C.; Taylor, Y.J.; Basquin, C.; Venkitsubramanian, K. Impact of Key Workplace Breastfeeding Support Characteristics on Job Satisfaction, Breastfeeding Duration, and Exclusive Breastfeeding Among Health Care Employees. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2019, 14, 416–423. [Google Scholar] [CrossRef]
- Zhuang, J.; Bresnahan, M.J.; Yan, X.; Zhu, Y.; Goldbort, J.; Bogdan-Lovis, E. Keep Doing the Good Work: Impact of Coworker and Community Support on Continuation of Breastfeeding. Health Commun. 2019, 34, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.M.; Said, Z.M.; Sutan, R.; Shah, S.A.; Darus, A.; Shamsuddin, K. Work Related Determinants of Breastfeeding Discontinuation among Employed Mothers in Malaysia. Int. Breastfeed. J. 2011, 6, 4. [Google Scholar] [CrossRef]
- Forster, D.A.; McLachlan, H.L.; Lumley, J. Factors Associated with Breastfeeding at Six Months Postpartum in a Group of Australian Women. Int. Breastfeed. J. 2006, 1, 18. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.L.; Leathers, S.J.; Kelley, M.A. Family Characteristics Associated with Duration of Breastfeeding during Early Infancy among Primiparas. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2004, 20, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Ludvigsson, J. Socio-Economic Determinants, Maternal Smoking and Coffee Consumption, and Exclusive Breastfeeding in 10,205 Children. Acta Paediatr. Oslo Nor. 1992 2005, 94, 1310–1319. [Google Scholar]
- Cohen, S.S.; Alexander, D.D.; Krebs, N.F.; Young, B.E.; Cabana, M.D.; Erdmann, P.; Hays, N.P.; Bezold, C.P.; Levin-Sparenberg, E.; Turini, M.; et al. Factors Associated with Breastfeeding Initiation and Continuation: A Meta-Analysis. J. Pediatr. 2018, 203, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, A.J.; Mannion, C.A.; McDonald, S.W.; Brockway, M.; Tough, S.C. The Impact of Caesarean Section on Breastfeeding Initiation, Duration and Difficulties in the First Four Months Postpartum. BMC Pregnancy Childbirth 2016, 16, 90. [Google Scholar] [CrossRef]
- Li, R.; Darling, N.; Maurice, E.; Barker, L.; Grummer-Strawn, L.M. Breastfeeding Rates in the United States by Characteristics of the Child, Mother, or Family: The 2002 National Immunization Survey. Pediatrics 2005, 115, e31–e37. [Google Scholar] [CrossRef] [PubMed]
- Chimoriya, R.; Scott, J.A.; John, J.R.; Bhole, S.; Hayen, A.; Kolt, G.S.; Arora, A. Determinants of Full Breastfeeding at 6 Months and Any Breastfeeding at 12 and 24 Months among Women in Sydney: Findings from the HSHK Birth Cohort Study. Int. J. Environ. Res. Public. Health 2020, 17, 5384. [Google Scholar] [CrossRef]
- Mangrio, E.; Persson, K.; Bramhagen, A.-C. Sociodemographic, Physical, Mental and Social Factors in the Cessation of Breastfeeding before 6 Months: A Systematic Review. Scand. J. Caring Sci. 2018, 32, 451–465. [Google Scholar] [CrossRef] [PubMed]
- LeLorier, J.; Grégoire, G.; Benhaddad, A.; Lapierre, J.; Derderian, F. Discrepancies between Meta-Analyses and Subsequent Large Randomized, Controlled Trials. N. Engl. J. Med. 1997, 337, 536–542. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Type of Study | Follow-Up | Population | Recruitment Procedures | Occupation | GDP per Capita * (in $) | Type of Breastfeeding | Timing of Returning to Work | Other Parameters Measured |
|---|---|---|---|---|---|---|---|---|---|---|
| Abou-ElWafa 2019 [44] | Egypt | Cross-sectional study | July–December 2017 | 633 | All working mothers attending healthcare facilities | Professional/semi-professional; manual; business worker | 2413 | Exclusive | <4 months; 4 months | Maternal sociodemographics, employment patterns, and birth characteristics |
| Aikawa 2015 [45] | Thailand | Cross-sectional study | February 2008 | 84 | Mothers who visited the breastfeeding mobile clinic at a nursery goods exhibition in Bangkok | Government and semi-government; private company employee; self-employed or family business owner | 4379 | Non-exclusive | <3 months | Maternal sociodemographics, employment patterns, and birth characteristics |
| Bergman 1981 [46] | Israel | Cross-sectional study | 1979 | 291 | Working women interviewed 7–9 months after delivery | All workers | 5674 | Non-exclusive | <3 months; 3 months; 4 months; 4–5 months; 5 months; 6 months | Maternal sociodemographics and employment patterns |
| Bonet 2013 [47] | France | Cohort study | 2003–2006 | 979 | From EDEN mother–child cohort; pregnant women were recruited from the maternity wards of the Poitiers and Nancy University hospitals | All workers | 34,760 | Exclusive and non-exclusive | ≤4 months; 5–8 months | Maternal sociodemographics and employment patterns |
| Boralingiah 2016 [48] | India | Cross-sectional study | January–December 2014 | 107 | Working mothers of the children attending the immunization center at JSS Hospital, Mysuru | All workers | 1576 | Exclusive | <6 months; >6 months | Maternal sociodemographics, employment patterns, and hospital breastfeeding practice |
| Chuang 2010 [49] | Taiwan | Cohort study | 2006–2007 | 20,172 | From the Taiwan Birth Cohort Study | All workers | 30,100 | Non-exclusive | ≤1 month; ≤2 months; ≤3 months; ≤6 months; ≤12 months | Maternal sociodemographics, employment patterns, birth characteristics, and hospital feeding practices |
| Cox 2015 [50] | Australia | Cross-sectional study | 2010–2011 | 427 | Mothers recruited from maternity services in rural western Australia | All workers | 51,937 | Exclusive and non-exclusive | <6 months; 6–12 months | Maternal sociodemographics, employment patterns, birth characteristics, hospital feeding practices, and psychosocial factors |
| Hawkins 2007 [51] | U.K. | Cohort study | September 2000–January 2002 | 6917 | From the Millennium Cohort Study | Employed workers in the formal or informal sector | 27,427 | Non-exclusive | <3 months; 4 months | Maternal sociodemographics and employment patterns |
| Jacknowitz 2008 [52] | USA | Cohort study | 1989–1999 | 1506 | From the National Longitudinal Survey of Youth and the Children of the National Longitudinal Survey | All workers | 24,405 | Non-exclusive | <6 weeks; >6 weeks and ≤3 months; >3 months and ≤6 months | Maternal sociodemographics, employment patterns, and birth characteristics |
| Ogbuanu 2011 [53] | USA | Cohort study | 2001–2003 | 6150 | Data drawn from the Early Childhood Longitudinal Study–Birth Cohort | All workers | 39,677 | Exclusive and non-exclusive | <6 weeks; <3 months | Maternal sociodemographics, employment patterns, birth characteristics, and hospital feeding practices |
| Piper 1996 [54] | USA | Cohort study | January 1989–June 1991 | 2372 | Data from the 1988 National Maternal-Infant Health Survey | All workers | 24,405 | Exclusive and non-exclusive | <6 weeks; 6 weeks–3 months; after 3 months and up to 6 months | Maternal sociodemographics and employment patterns |
| Scott 2006 [55] | Australia | Cohort study | September 2002–July 2003 | 587 | Mothers contacted within the 3 days after birth from 2 maternity hospitals in Perth | All workers | 23,437 | Exclusive and non-exclusive | <6 months; 6–12 month | Maternal sociodemographics, employment patterns, birth characteristics, hospital feeding practices, and psychosocial factors |
| Xiang 2016 [56] | Australia | Cross-sectional study | November 2010–February 2011 | 2300 | Data from the BaselineMothers Survey | Paid employment | 51,937 | Exclusive and non-exclusive | <3 months; 3–6 months; <8 weeks; 9–16 weeks | Maternal sociodemographics and employment patterns |
| Yimyam 1999 [57] | Thailand | Cross-sectional study | July–August 1994 and April–November 1995 | 295 | Women approached in the growth monitoring clinic at Chiang Mai University Hospital or at Chiang Mai University’s Child Care Centre | Formal sector (public and private employee) and informal sector (pieceworker at home and self/family employed) | 2845 | Exclusive and non-exclusive | 6 months | Maternal sociodemographics and employment patterns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dutheil, F.; Méchin, G.; Vorilhon, P.; Benson, A.C.; Bottet, A.; Clinchamps, M.; Barasinski, C.; Navel, V. Breastfeeding after Returning to Work: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8631. https://doi.org/10.3390/ijerph18168631
Dutheil F, Méchin G, Vorilhon P, Benson AC, Bottet A, Clinchamps M, Barasinski C, Navel V. Breastfeeding after Returning to Work: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(16):8631. https://doi.org/10.3390/ijerph18168631
Chicago/Turabian StyleDutheil, Frédéric, Grégory Méchin, Philippe Vorilhon, Amanda C. Benson, Anne Bottet, Maëlys Clinchamps, Chloé Barasinski, and Valentin Navel. 2021. "Breastfeeding after Returning to Work: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 16: 8631. https://doi.org/10.3390/ijerph18168631
APA StyleDutheil, F., Méchin, G., Vorilhon, P., Benson, A. C., Bottet, A., Clinchamps, M., Barasinski, C., & Navel, V. (2021). Breastfeeding after Returning to Work: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(16), 8631. https://doi.org/10.3390/ijerph18168631