
Objective Behavioral Measures in Children before, during, and after the COVID-19 Lockdown in Israel

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
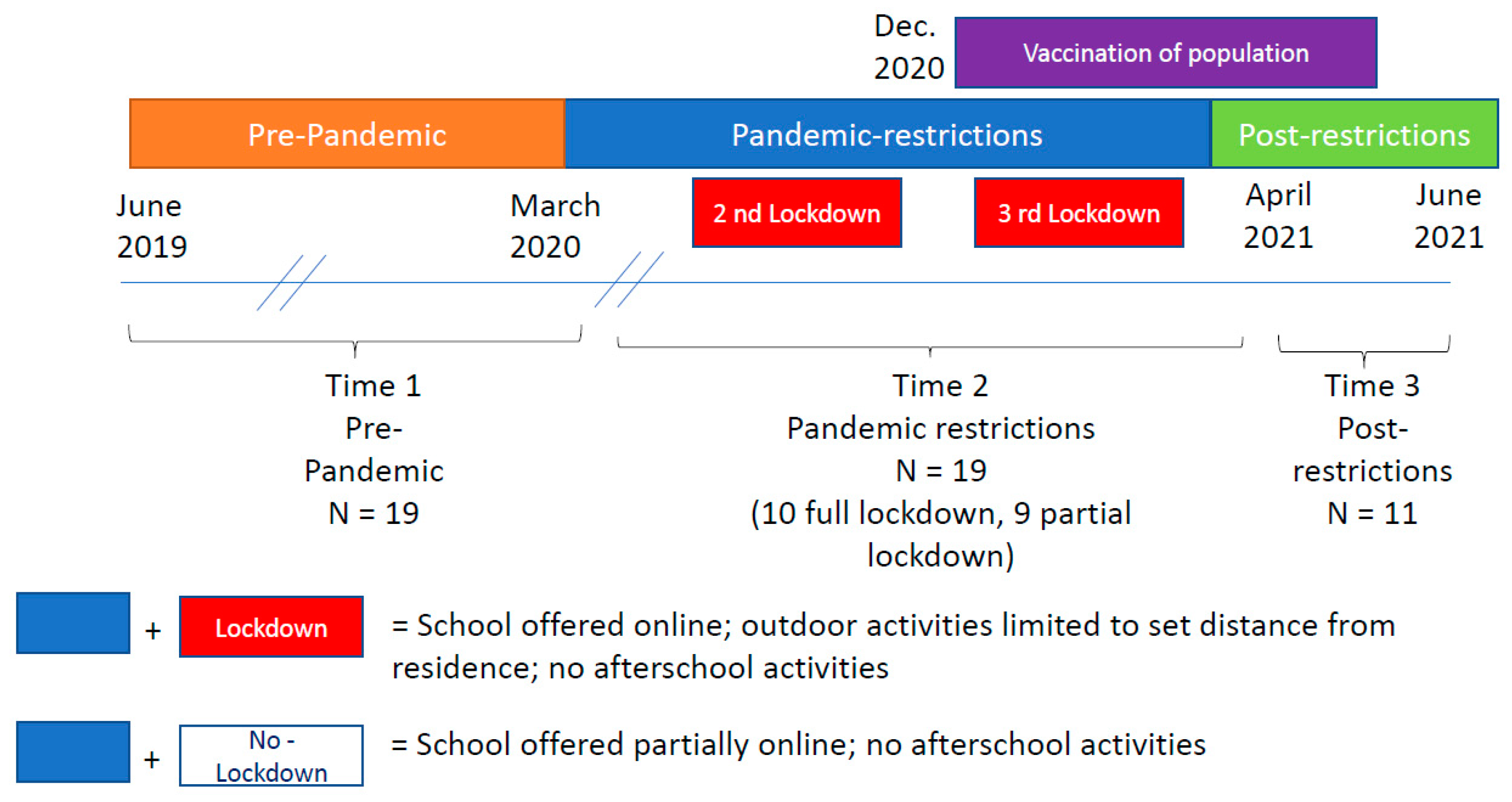
2.2. Setting
2.3. Measurements
2.4. Analysis
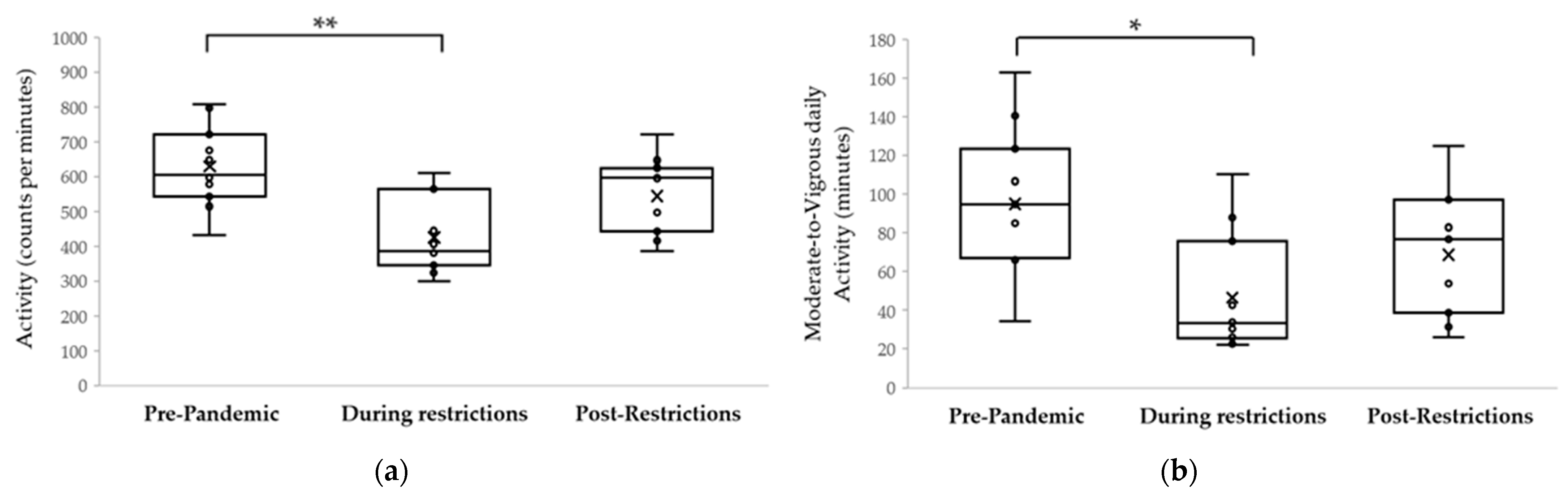
3. Results
4. Discussion
4.1. Physical Activity
4.2. Time Outdoors
4.3. Sleep
4.4. School and Children’s Health
4.5. Post-Restriction Behavior
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 17 July 2021).
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [Green Version]
- Haimi, M.; Kremer, R. Vitamin D deficiency/insufficiency from childhood to adulthood: Insights from a sunny country. World J. Clin. Pediatr. 2017, 6, 1–9. [Google Scholar] [CrossRef]
- Lingham, G.; Mackey, D.A.; Lucas, R.; Yazar, S. How does spending time outdoors protect against myopia? A review. Br. J. Ophthalmol. 2020, 104, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Kline, C.E.; Rebar, A.L.; Vandelanotte, C.; Short, C.E. Greater bed- and wake-time variability is associated with less healthy lifestyle behaviors: A cross-sectional study. Z Gesundh Wiss 2016, 24, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanamah, R.; Eghbaria-Ghanamah, H. Impact of COVID-19 Pandemic on Behavioral and Emotional Aspects and Daily Routines of Arab Israeli Children. Int. J. Environ. Res. Public Health 2021, 18, 2946. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef]
- Nathan, A.; George, P.; Ng, M.; Wenden, E.; Bai, P.; Phiri, Z.; Christian, H. Impact of COVID-19 Restrictions on Western Australian Children’s Physical Activity and Screen Time. Int. J. Environ. Res. Public Health 2021, 18, 2583. [Google Scholar] [CrossRef]
- Orgiles, M.; Morales, A.; Delvecchio, E.; Mazzeschi, C.; Espada, J.P. Immediate Psychological Effects of the COVID-19 Quarantine in Youth From Italy and Spain. Front. Psychol. 2020, 11, 579038. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity (Silver Spring) 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Xiang, M.; Zhang, Z.; Kuwahara, K. Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog. Cardiovasc. Dis. 2020, 63, 531–532. [Google Scholar] [CrossRef]
- Najman, J.M.; Williams, G.M.; Nikles, J.; Spence, S.; Bor, W.; O’Callaghan, M.; Le Brocque, R.; Andersen, M.J.; Shuttlewood, G.J. Bias influencing maternal reports of child behaviour and emotional state. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 186–194. [Google Scholar] [CrossRef]
- Whiteman, D.; Green, A. Wherein lies the truth? Assessment of agreement between parent proxy and child respondents. Int. J. Epidemiol. 1997, 26, 855–859. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F. Self-report measures of children’s physical activity. J. Sch. Health 1991, 61, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Sirard, J.R.; Pate, R.R. Physical activity assessment in children and adolescents. Sports Med. 2001, 31, 439–454. [Google Scholar] [CrossRef]
- Robbins, R.; Affouf, M.; Weaver, M.D.; Czeisler, M.E.; Barger, L.K.; Quan, S.F.; Czeisler, C.A. Estimated Sleep Duration Before and During the COVID-19 Pandemic in Major Metropolitan Areas on Different Continents: Observational Study of Smartphone App Data. J. Med. Internet Res. 2021, 23, e20546. [Google Scholar] [CrossRef]
- Sanudo, B.; Fennell, C.; Sánchez-Oliver, A.J. Objectively-Assessed Physical Activity, Sedentary Behavior, Smartphone Use, and Sleep Patterns Pre- and during-COVID-19 Quarantine in Young Adults from Spain. Sustainability 2020, 12, 5890. [Google Scholar] [CrossRef]
- Gordon-Shaag, A.; Shneor, E.; Doron, R.; Levine, J.; Ostrin, L.A. Environmental and Behavioral Factors with Refractive Error in Israeli Boys. Optom. Vis. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Emergency Regulations (New Corona Virus—Restrictions of Activity) Amendment No. 1, 5720-2020. Available online: https://www.gov.il/he/departments/policies/dec4919_2020 (accessed on 11 June 2021).
- Special Powers Regulations for Dealing with the New Corona Virus (Temporary Order) (Restriction of Stay) in Public Space and Restriction of Activity 5744-2020. Available online: https://www.nevo.co.il/law_word/law06/tak-8766.pdf (accessed on 11 June 2021).
- Special Powers Regulations for Dealing with the New Corona Virus (Temporary Order) (Restriction of Stay). In the Public Space and Restriction of Activity (5744-2020). Available online: https://www.nevo.co.il/law_word/law06/tak-9022.pdf (accessed on 11 June 2021).
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Ekblom, O.; Nyberg, G.; Bak, E.E.; Ekelund, U.; Marcus, C. Validity and comparability of a wrist-worn accelerometer in children. J. Phys. Act. Health 2012, 9, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, L.J.; Walsh, C.M.; Traylor, J.; Westin, A.M. Direct comparison of two new actigraphs and polysomnography in children and adolescents. Sleep 2012, 35, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Pesonen, A.K.; Kuula, L. The Validity of a New Consumer-Targeted Wrist Device in Sleep Measurement: An Overnight Comparison Against Polysomnography in Children and Adolescents. J. Clin. Sleep Med. 2018, 14, 585–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nystrom, C.; Mora-Gonzalez, J.; Lof, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Ward, T.M.; Lentz, M.; Kieckhefer, G.M.; Landis, C.A. Polysomnography and actigraphy concordance in juvenile idiopathic arthritis, asthma and healthy children. J. Sleep Res. 2012, 21, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Ostrin, L.A. Objectively measured light exposure in emmetropic and myopic adults. Optom. Vis. Sci. 2017, 94, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Ostrin, L.A.; Sajjadi, A.; Benoit, J.S. Objectively Measured Light Exposure During School and Summer in Children. Optom. Vis. Sci. 2018, 95, 332–342. [Google Scholar] [CrossRef]
- Read, S.A.; Collins, M.J.; Vincent, S.J. Light exposure and physical activity in myopic and emmetropic children. Optom. Vis. Sci. 2014, 91, 330–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, S.A.; Collins, M.J.; Vincent, S.J. Light exposure and eye growth in childhood. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6779–6787. [Google Scholar] [CrossRef]
- Read, S.A.; Vincent, S.J.; Tan, C.S.; Ngo, C.; Collins, M.J.; Saw, S.M. Patterns of Daily Outdoor Light Exposure in Australian and Singaporean Children. Transl. Vis. Sci. Technol. 2018, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Izmailova, E.S.; McLean, I.L.; Hather, G.; Merberg, D.; Homsy, J.; Cantor, M.; Volfson, D.; Bhatia, G.; Perakslis, E.D.; Benko, C.; et al. Continuous Monitoring Using a Wearable Device Detects Activity-Induced Heart Rate Changes After Administration of Amphetamine. Clin. Transl. Sci. 2019, 12, 677–686. [Google Scholar] [CrossRef] [Green Version]
- Ostrin, L.A.; Jnawali, A.; Carkeet, A.; Patel, N.B. Twenty-four hour ocular and systemic diurnal rhythms in children. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. 2019, 39, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Ostrin, L.A.; Read, S.A.; Vincent, S.J.; Collins, M.J. Sleep in Myopic and Non-Myopic Children. Transl. Vis. Sci. Technol. 2020, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Ulaganathan, S.; Read, S.A.; Collins, M.J.; Vincent, S.J. Measurement Duration and Frequency Impact Objective Light Exposure Measures. Optom. Vis. Sci. 2017, 94, 588–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donaldson, S.C.; Montoye, A.H.; Tuttle, M.S.; Kaminsky, L.A. Variability of Objectively Measured Sedentary Behavior. Med. Sci. Sports Exerc. 2016, 48, 755–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aadland, E.; Ylvisaker, E. Reliability of Objectively Measured Sedentary Time and Physical Activity in Adults. PLoS ONE 2015, 10, e0133296. [Google Scholar] [CrossRef] [Green Version]
- Flynn, J.I.; Coe, D.P.; Larsen, C.A.; Rider, B.C.; Conger, S.A.; Bassett, D.R., Jr. Detecting indoor and outdoor environments using the ActiGraph GT3X+ light sensor in children. Med. Sci. Sports Exerc. 2014, 46, 201–206. [Google Scholar] [CrossRef]
- Dharani, R.; Lee, C.F.; Theng, Z.X.; Drury, V.B.; Ngo, C.; Sandar, M.; Wong, T.Y.; Finkelstein, E.A.; Saw, S.M. Comparison of measurements of time outdoors and light levels as risk factors for myopia in young Singapore children. Eye 2012, 26, 911–918. [Google Scholar] [CrossRef] [Green Version]
- Jerusalem, Israel—Sunrise, Sunset and Daylength. Available online: https://www.timeanddate.com/sun/israel/jerusalem (accessed on 5 June 2021).
- Graham, P.; Jackson, R. A comparison of primary and proxy respondent reports of habitual physical activity, using kappa statistics and log-linear models. J. Epidemiol. Biostat. 2000, 5, 255–265. [Google Scholar]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Estevez-Lopez, F.; Munoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-Garcia, P.; Henriksson, H.; Mena-Molina, A.; Martinez-Vizcaino, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Abid, R.; Ammar, A.; Maaloul, R.; Souissi, N.; Hammouda, O. Effect of COVID-19-Related Home Confinement on Sleep Quality, Screen Time and Physical Activity in Tunisian Boys and Girls: A Survey. Int. J. Environ. Res. Public Health 2021, 18, 3065. [Google Scholar] [CrossRef]
- Guo, Y.F.; Liao, M.Q.; Cai, W.L.; Yu, X.X.; Li, S.N.; Ke, X.Y.; Tan, S.X.; Luo, Z.Y.; Cui, Y.F.; Wang, Q.; et al. Physical activity, screen exposure and sleep among students during the pandemic of COVID-19. Sci. Rep. 2021, 11, 8529. [Google Scholar] [CrossRef]
- Stavridou, A.; Kapsali, E.; Panagouli, E.; Thirios, A.; Polychronis, K.; Bacopoulou, F.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Obesity in Children and Adolescents during COVID-19 Pandemic. Children 2021, 8, 135. [Google Scholar] [CrossRef]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef]
- Antonucci, R.; Locci, C.; Clemente, M.G.; Chicconi, E.; Antonucci, L. Vitamin D deficiency in childhood: Old lessons and current challenges. J. Pediatr. Endocrinol. Metab. 2018, 31, 247–260. [Google Scholar] [CrossRef]
- Glabska, D.; Kolota, A.; Lachowicz, K.; Skolmowska, D.; Stachon, M.; Guzek, D. The Influence of Vitamin D Intake and Status on Mental Health in Children: A Systematic Review. Nutrients 2021, 13, 952. [Google Scholar] [CrossRef]
- Brenner, H. Vitamin D Supplementation to Prevent COVID-19 Infections and Deaths-Accumulating Evidence from Epidemiological and Intervention Studies Calls for Immediate Action. Nutrients 2021, 13, 411. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.L.; Wu, W.F.; Liou, Y.M. Dose-Response Relationship of Outdoor Exposure and Myopia Indicators: A Systematic Review and Meta-Analysis of Various Research Methods. Int. J. Environ. Res. Public Health 2019, 16, 2595. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Ma, Y.; Yuan, J.; Zhang, Y.; Wang, H.; Zhang, G.; Tu, C.; Lu, X.; Li, J.; Xiong, Y.; et al. COVID-19 Quarantine Reveals That Behavioral Changes Have an Effect on Myopia Progression. Ophthalmology 2021. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Y.; Musch, D.C.; Wei, N.; Qi, X.; Ding, G.; Li, X.; Li, J.; Song, L.; Zhang, Y.; et al. Progression of Myopia in School-Aged Children After COVID-19 Home Confinement. JAMA Ophthalmol. 2021, 139, 293–300. [Google Scholar] [CrossRef]
- Marino, C.; Andrade, B.; Campisi, S.C.; Wong, M.; Zhao, H.; Jing, X.; Aitken, M.; Bonato, S.; Haltigan, J.; Wang, W.; et al. Association Between Disturbed Sleep and Depression in Children and Youths: A Systematic Review and Meta-analysis of Cohort Studies. JAMA Netw. Open 2021, 4, e212373. [Google Scholar] [CrossRef] [PubMed]
- Sampasa-Kanyinga, H.; Colman, I.; Goldfield, G.S.; Janssen, I.; Wang, J.; Podinic, I.; Tremblay, M.S.; Saunders, T.J.; Sampson, M.; Chaput, J.P. Combinations of physical activity, sedentary time, and sleep duration and their associations with depressive symptoms and other mental health problems in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 72. [Google Scholar] [CrossRef]
- Guo, Y.; Miller, M.A.; Cappuccio, F.P. Short duration of sleep and incidence of overweight or obesity in Chinese children and adolescents: A systematic review and meta-analysis of prospective studies. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Chaabane, S.; Doraiswamy, S.; Chaabna, K.; Mamtani, R.; Cheema, S. The Impact of COVID-19 School Closure on Child and Adolescent Health: A Rapid Systematic Review. Children 2021, 8, 415. [Google Scholar] [CrossRef]
- Ulaganathan, S.; Read, S.A.; Collins, M.J.; Vincent, S.J. Influence of seasons upon personal light exposure and longitudinal axial length changes in young adults. Acta Ophthalmol. 2019, 97, e256–e265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharlova, I.; Deng, W.H.; Mamen, J.; Mamen, A.; Fredriksen, M.V.; Fredriksen, P.M. The Weather Impact on Physical Activity of 6–12 Year Old Children: A Clustered Study of the Health Oriented Pedagogical Project (HOPP). Sports 2020, 8, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolle, E.; Steene-Johannessen, J.; Andersen, L.B.; Anderssen, S.A. Seasonal variation in objectively assessed physical activity among children and adolescents in Norway: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 36. [Google Scholar] [CrossRef] [Green Version]
- Silva, P.; Seabra, A.; Saint-Maurice, P.; Soares-Miranda, L.; Mota, J. Physical activity intensities in youth: The effect of month of assessment. Ann. Hum. Biol. 2013, 40, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Riddoch, C.J.; Mattocks, C.; Deere, K.; Saunders, J.; Kirkby, J.; Tilling, K.; Leary, S.D.; Blair, S.N.; Ness, A.R. Objective measurement of levels and patterns of physical activity. Arch. Dis. Child. 2007, 92, 963–969. [Google Scholar] [CrossRef] [Green Version]
- Ridgers, N.D.; Salmon, J.; Timperio, A. Too hot to move? Objectively assessed seasonal changes in Australian children’s physical activity. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 77. [Google Scholar] [CrossRef] [Green Version]
- Ridgers, N.D.; Salmon, J.; Timperio, A. Seasonal changes in physical activity during school recess and lunchtime among Australian children. J. Sports Sci. 2018, 36, 1508–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Pre-Pandemic β | Social Restrictions β | p Value * | |
|---|---|---|---|
| Physical activity (counts per minute) | 595 ± 145 | 429 ± 139 | 0.001 £ |
| 596 (459, 719) | 385 (345, 563) | ||
| (353–806) | (168–736) | ||
| Time MVPA (minutes per day) | 86 ± 39 | 46 ± 30 | 0.004 |
| 85 (49, 123) | 33 (25, 76) | ||
| (27–163) | (1–110) | ||
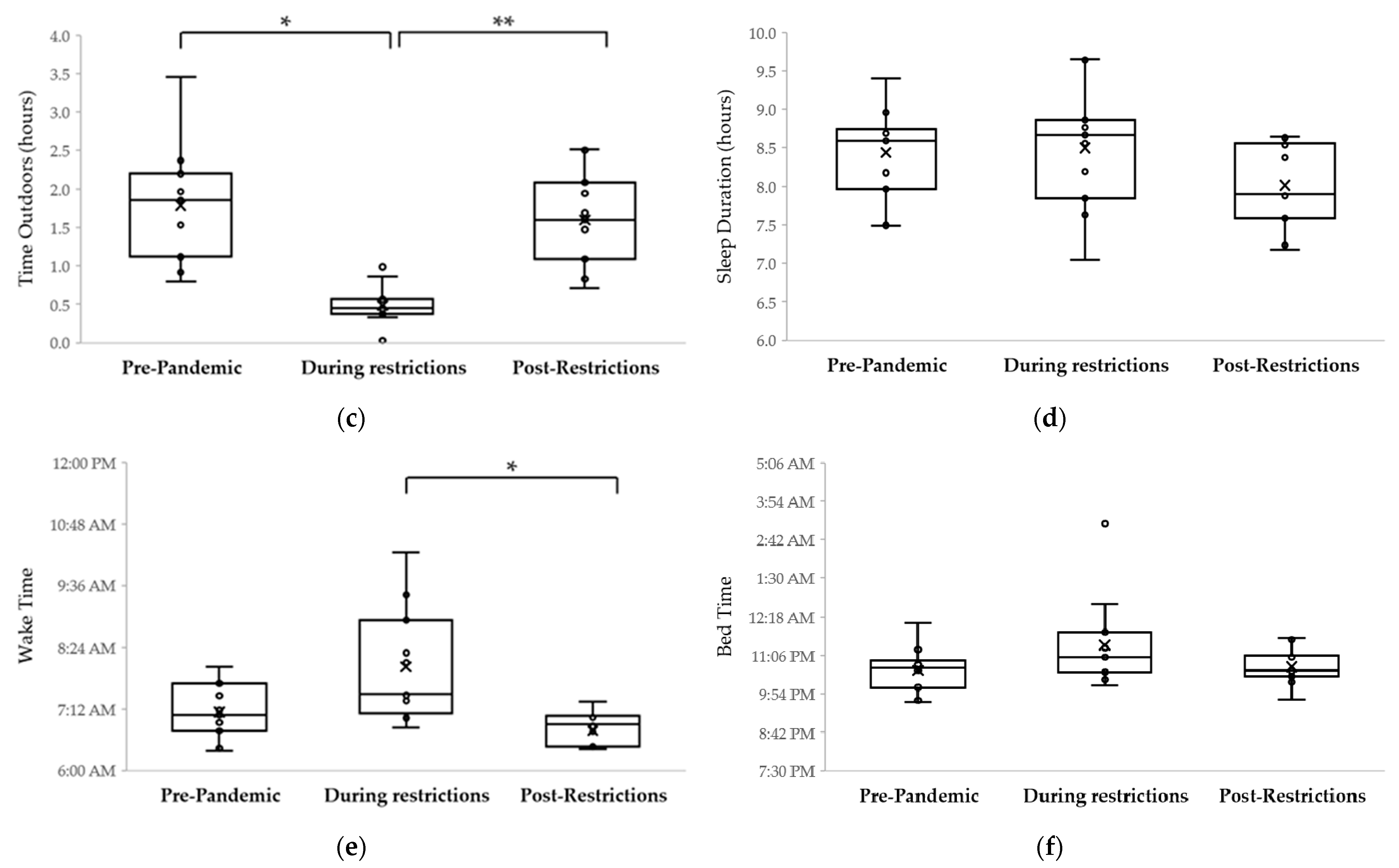
| Time outdoors (hours per day) | 1.8 ± 1.0 | 0.7 ± 0.7 | 0.001 |
| 1.6 (1.1, 2.2) | 0.5 (0.4, 0.8) | ||
| (0.3–4.4) | (0.0–3.0) | ||
| Sleep duration (hours per night) | 8.4 ± 0.6 | 8.5 ± 0.7 | >0.99 |
| 8.6 (7.6, 8.9) | 8.7 (8.2, 8.9) | ||
| (7.4–9.4) | (7.0–9.7) | ||
| Bedtime | 10:35 p.m. ± 53 min | 11:34 p.m. ± 109 min | 0.02 |
| 10:42 p.m. (9:42 p.m.–11:17 p.m.) | 11:13 (10:20 p.m., 12:03 a.m.) | ||
| (9:06 p.m.–12:06 a.m.) | (9:21 p.m.–4:38 a.m.) | ||
| Waketime | 7:04 a.m. ± 38 min | 08:12 a.m. ± 89 min | 0.004 |
| 7:05 a.m. (6:36 a.m., 7:33 a.m.) | 8:04 a.m. (7:01 a.m.–8:55 a.m.) | ||
| (5:53 a.m.–08:16 a.m.) | (6:39 a.m.–12:05 p.m.) |
| Estimated Difference in Activity (Pre-PANDEMIC MINUS during Restrictions) | Estimated Mean Change (cpm) | 95% CI | p Value |
|---|---|---|---|
| 12:00 to 3:59 a.m. | 14 | −34, 62 | >0.99 |
| 4:00 to 7:59 a.m. | −62 | −111, −13 | 0.33 |
| 8:00 to 11:59 a.m. | −267 | −348, −186 | <0.001 |
| 12:00 to 3:59 p.m. | −146 | −227, −65 | <0.001 |
| 4:00 to 7:59 p.m. | −162 | −243, −81 | <0.001 |
| 8:00 to 11:59 p.m. | −27 | −108, 54 | >0.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shneor, E.; Doron, R.; Levine, J.; Zimmerman, D.R.; Benoit, J.S.; Ostrin, L.A.; Gordon-Shaag, A. Objective Behavioral Measures in Children before, during, and after the COVID-19 Lockdown in Israel. Int. J. Environ. Res. Public Health 2021, 18, 8732. https://doi.org/10.3390/ijerph18168732
Shneor E, Doron R, Levine J, Zimmerman DR, Benoit JS, Ostrin LA, Gordon-Shaag A. Objective Behavioral Measures in Children before, during, and after the COVID-19 Lockdown in Israel. International Journal of Environmental Research and Public Health. 2021; 18(16):8732. https://doi.org/10.3390/ijerph18168732
Chicago/Turabian StyleShneor, Einat, Ravid Doron, Jonathan Levine, Deena Rachel Zimmerman, Julia S. Benoit, Lisa A. Ostrin, and Ariela Gordon-Shaag. 2021. "Objective Behavioral Measures in Children before, during, and after the COVID-19 Lockdown in Israel" International Journal of Environmental Research and Public Health 18, no. 16: 8732. https://doi.org/10.3390/ijerph18168732
APA StyleShneor, E., Doron, R., Levine, J., Zimmerman, D. R., Benoit, J. S., Ostrin, L. A., & Gordon-Shaag, A. (2021). Objective Behavioral Measures in Children before, during, and after the COVID-19 Lockdown in Israel. International Journal of Environmental Research and Public Health, 18(16), 8732. https://doi.org/10.3390/ijerph18168732