
Development and Evaluation of a Community Surveillance Method for Estimating Deaths Due to Injuries in Rural Nepal

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
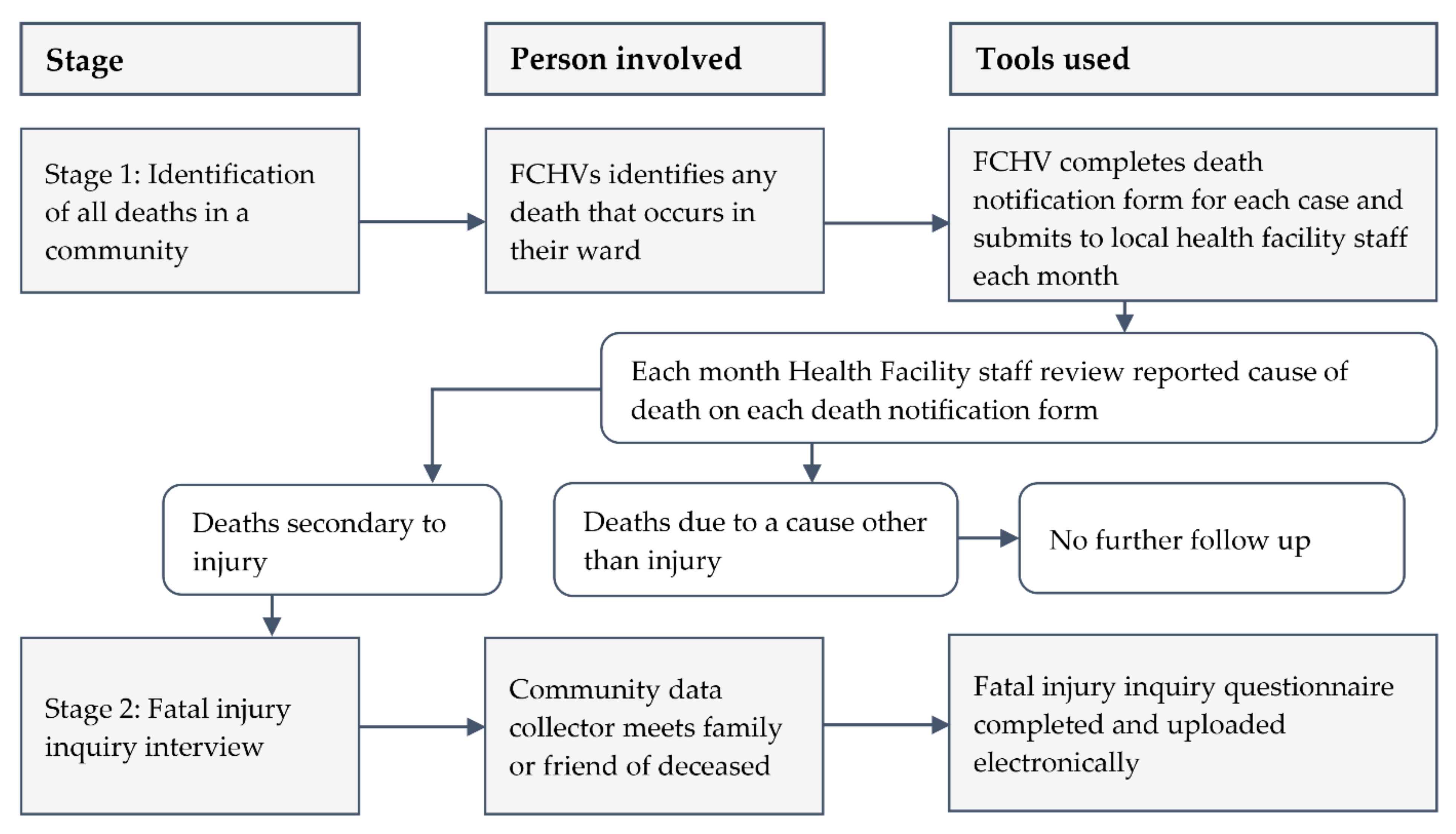
2.1. Development of a Surveillance Method
2.1.1. Two-Stage Data Collection Approach
2.1.2. Data Collection Tools
2.1.3. Data Management
2.2. Evaluation of the Surveillance Method
2.2.1. Study Sites and Study Populations
2.2.2. Training
2.2.3. Piloting and Data Collection
2.2.4. Quality Control and Analysis of Data
2.2.5. Evaluation of the Method
3. Results
3.1. Feedback from FCHVs and Health Facility Staff
3.2. Estimation of Deaths Due to Injury
4. Discussion
4.1. Key Issues Arising from Our Findings
4.2. Opportunities and Challenges
4.3. Strengths and Limitations
4.4. Implications for Policy, Practice and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Injuries and Violence: The Facts 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Pant, P.R.; Banstola, A.; Bhatta, S.; Mytton, J.A.; Acharya, D.; Bhattarai, S.; Bisignano, C.; Castle, C.D.; Prasad Dhungana, G.; Dingels, Z.V.; et al. Burden of injuries in Nepal, 1990–2017: Findings from the Global Burden of Disease Study 2017. Inj. Prev. 2020, 26, i57–i66. [Google Scholar] [CrossRef] [PubMed]
- United Nations. UN Least Developed Countries. Available online: http://unohrlls.org/about-ldcs/ (accessed on 9 June 2020).
- Ministry of Health and Population. The Annual Report of the Department of the Health Services (2018/19); Goverment of Nepal: Kathmandu, Nepal, 2019.
- Joshi, S.; Shrestha, S. Economic and social burden due to injuries and violence in Nepal: A cross-sectional study. Kathmandu Univ. Med. J. KUMJ 2009, 7, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Pant, P.R.; Deave, T.; Banstola, A.; Bhatta, S.; Joshi, E.; Adhikari, D.; Manandhar, S.R.; Joshi, S.K.; Mytton, J.A. Home-related and work-related injuries in Makwanpur district, Nepal: A household survey. Inj. Prev. 2020, 043986. [Google Scholar] [CrossRef] [PubMed]
- Laflamme, L.; Burrows, S.; Hasselberg, M. Socioeconomic Differences in Injury Risks: A Review of Findings and a Discussion of Potential Countermeasures; World Health Organization: Copenhagen, Denmark, 2009. [Google Scholar]
- Mathers, C.D.; Ma Fat, D.; Inoue, M.; Rao, C.; Lopez, A.D. Counting the dead and what they died from: An assessment of the global status of cause of death data. Bull World Health Organ. 2005, 83, 171–177. [Google Scholar]
- World Health Organization. Regional Strategy for Strengthening the Role of the Health Sector for Improving CRVS (2015–2024); WHO Regional Office for South-East Asia: New Delhi, India, 2015. [Google Scholar]
- Sharma, G. Leading causes of mortality from diseases and injury in Nepal: A report from national census sample survey. J. Inst. Med. Nepal 2006, 28, 7–11. [Google Scholar] [CrossRef]
- Mytton, J.A.; Bhatta, S.; Thorne, M.; Pant, P.R. Understanding the burden of injuries in Nepal: A systematic review of published studies. Cogent. Med. 2019, 6, 1673654. [Google Scholar] [CrossRef]
- Khatri, R.B.; Mishra, S.R.; Khanal, V. Female community health volunteers in community-based health programs of Nepal: Future perspective. Front. Public Health 2017, 5, 181. [Google Scholar] [CrossRef]
- World Health Organization. Verbal Autopsy Standards: Ascertaining and Attributing Causes of Death—The 2016 WHO Verbal Autopsy Instrument. Available online: https://www.who.int/healthinfo/statistics/verbalautopsystandards/en/ (accessed on 28 May 2018).
- Khanal, S.; Dawson, P.; Houston, R. Verbal autopsy to ascertain causes of neonatal deaths in a community setting: A study from Morang, Nepal. J. Nepal Med. Assoc. 2011, 51, 21–27. [Google Scholar] [CrossRef]
- Manandhar, S.; Ojha, A.; Manandhar, D.; Shrestha, B.; Shrestha, D.; Saville, N.; Costello, A.; Osrin, D. Causes of stillbirths and neonatal deaths in Dhanusha district, Nepal: A verbal autopsy study. Kathmandu Univ. Med. J. KUMJ 2010, 8, 62. [Google Scholar] [CrossRef] [Green Version]
- Serina, P.; Riley, I.; Hernandez, B.; Flaxman, A.D.; Praveen, D.; Tallo, V.; Joshi, R.; Sanvictores, D.; Stewart, A.; Mooney, M.D. What is the optimal recall period for verbal autopsies? Validation study based on repeat interviews in three populations. Popul. Health Metr. 2016, 14, 40. [Google Scholar] [CrossRef] [Green Version]
- Pant, P.R.; Towner, E.; Ellis, M.; Manandhar, D.; Pilkington, P.; Mytton, J. Epidemiology of unintentional child injuries in the Makwanpur District of Nepal: A household survey. Int. J. Env. Res. Public Health 2015, 12, 15118–15128. [Google Scholar] [CrossRef]
- Bhatta, S.; Mytton, J.A.; Deave, T. Assessment of home hazards for non-fatal childhood injuries in rural Nepal: A community survey. Inj. Prev. 2020, 27, 104–110. [Google Scholar] [CrossRef]
- Halim, A.; Utz, B.; Biswas, A.; Rahman, F.; Van Den Broek, N. Cause of and contributing factors to maternal deaths; a cross-sectional study using verbal autopsy in four districts in Bangladesh. BJOG 2014, 121, 86–94. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed Inf. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Central Bureau of Statistics. National Population and Housing Census 2011 (National Report); National Planning Commission, Central Bureau of Statistics: Kathmandu, Nepal, 2012. [Google Scholar]
- The World Bank. Death Rate, Crude (Per 1,000 People)—Nepal. Available online: https://data.worldbank.org/indicator/SP.DYN.CDRT.IN?locations=NP (accessed on 18 June 2018).
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- Kimberlin, C.L.; Winterstein, A.G. Validity and reliability of measurement instruments used in research. Am. J. Health Syst. Pharm. 2008, 65, 2276–2284. [Google Scholar] [CrossRef]
- Jagnoor, J.; Ponnaiah, M.; Varghese, M.; Ivers, R.; Kumar, R.; Prinja, S.; Christou, A.; Jain, T. Potential for establishing an injury surveillance system in India: A review of data sources and reporting systems. BMC Public Health 2020, 20, 1909. [Google Scholar] [CrossRef]
- Alonge, O.; Agrawal, P.; Talab, A.; Rahman, Q.S.; Rahman, A.F.; El Arifeen, S.; Hyder, A.A. Fatal and non-fatal injury outcomes: Results from a purposively sampled census of seven rural subdistricts in Bangladesh. Lancet Glob. Health 2017, 5, e818–e827. [Google Scholar] [CrossRef] [Green Version]
- Jagnoor, J.; Suraweera, W.; Keay, L.; Ivers, R.Q.; Thakur, J.; Jha, P. Unintentional injury mortality in India, 2005: Nationally representative mortality survey of 1.1 million homes. BMC Public Health 2012, 12, 487. [Google Scholar] [CrossRef] [Green Version]
- Palanivel, C.; Yadav, K.; Gupta, V.; Rai, S.K.; Misra, P.; Krishnan, A. Causes of death in rural adult population of North India (2002–2007), using verbal autopsy tool. Indian J. Public Health 2013, 57, 78–83. [Google Scholar]
- Thomas, L.-M.; D’Ambruoso, L.; Balabanova, D. Verbal autopsy in health policy and systems: A literature review. BMJ Glob. Health 2018, 3, e000639. [Google Scholar] [CrossRef] [Green Version]
- Hazard, R.H.; Buddhika, M.P.; Hart, J.D.; Chowdhury, H.R.; Firth, S.; Joshi, R.; Avelino, F.; Segarra, A.; Sarmiento, D.C.; Azad, A.K. Automated verbal autopsy: From research to routine use in civil registration and vital statistics systems. BMC Med. 2020, 18, 60. [Google Scholar] [CrossRef] [Green Version]
- NHRC. Nepal Burden of Disease 2017: A Country Report Based on the Global Burden of Disease 2017 Study; Nepal Health Research Council (NHRC), Ministry of Health and Population (MoHP) and Monitoring Evaluation and Operational Research (MEOR): Kathmandu, Nepal, 2019. [Google Scholar]
- Hagaman, A.K.; Maharjan, U.; Kohrt, B.A. Suicide surveillance and health systems in Nepal: A qualitative and social network analysis. Int. J. Ment. Health Syst. 2016, 10, 46. [Google Scholar] [CrossRef]
- Marahatta, K.; Samuel, R.; Sharma, P.; Dixit, L.; Shrestha, B.R. Suicide burden and prevention in Nepal: The need for a national strategy. WHO South East Asia J. Public Health 2017, 6, 45–49. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. Status of Civil Registration and Vital Statistics in South Asia Countries 2018; Regional Office for South Asia (ROSA): Kathmandu, Nepal, 2019. [Google Scholar]
- Ide, N.; Fitzpatrick, A.; Flaxman, A.; Koju, R.; Tamrakar, D.; Hernandez, B. Estimation of causes of death in suburban Nepal using verbal autopsy. Kathmandu Univ. Med. J. KUMJ 2016, 14, 112–119. [Google Scholar]
- Phillips, D.E.; Lozano, R.; Naghavi, M.; Atkinson, C.; Gonzalez-Medina, D.; Mikkelsen, L.; Murray, C.J.; Lopez, A.D. A composite metric for assessing data on mortality and causes of death: The vital statistics performance index. Popul. Health Metr. 2014, 12, 14. [Google Scholar] [CrossRef] [Green Version]
- Hagaman, A.K.; Khadka, S.; Lohani, S.; Kohrt, B. Suicide in Nepal: A modified psychological autopsy investigation from randomly selected police cases between 2013 and 2015. Soc. Psychiatry Psychiatr Epidemiol. 2017, 52, 1483–1494. [Google Scholar] [CrossRef]
- Ghimire, S.; Devkota, S.; Budhathoki, R.; Thakur, A.; Sapkota, N. Psychiatric Comorbidities in Patients with Deliberate Self-Harm in a Tertiary Care Center. JNMA J. Nepal Med. Assoc. 2014, 52, 697–701. [Google Scholar] [CrossRef]
- Thapaliya, S.; Gupta, A.K.; Tiwari, S.; Belbase, M.; Paudyal, S. Pattern of suicide Attempts in southern nepal: A Multi-centered retrospective study. Med. Phoenix 2018, 3, 41–47. [Google Scholar] [CrossRef]
- Mills, S.; Lee, J.K.; Rassekh, B.M. An introduction to the civil registration and vital statistics systems with applications in low-and middle-income countries. J. Health Popul. Nutr. 2019, 38, 23. [Google Scholar] [CrossRef] [Green Version]
- Mikkelsen, L.; Phillips, D.E.; AbouZahr, C.; Setel, P.W.; de Savigny, D.; Lozano, R.; Lopez, A.D. A global assessment of civil registration and vital statistics systems: Monitoring data quality and progress. Lancet 2015, 386, 1395–1406. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Two Rural Municipalities | Total Population | Total Deaths (Expected) |
|---|---|---|
| Total population | 64,602 | |
| Any deaths estimated | 0.6% * of 64,602 | 387 |
| Injury death expected | 10% ** of 387 | 39 |
| All-Cause Deaths | Deaths from Unintentional Injury * | Deaths from Self-Harm and Assault ** | All-Injury Deaths | |||
|---|---|---|---|---|---|---|
| n | Proportion (95% CI) | n | Proportion (95% CI) | n | Proportion (95% CI) | |
| Overall (n = 457) | 23 | 5.0 (3.0–6.0) | 44 | 9.6 (6.9–12.3) | 67 | 14.6 (11.4–17.9) |
| Age (years), median (IQR) | - | 55 (19–65) | - | 36.5 (25.3–53.5) | - | 40 (24–56) |
| Male (n = 264) | 17 | 6.4 (3.5–9.4) | 24 † | 9.1 (5.6–12.6) | 41 | 15.5 (11.2–19.9) |
| Female (n = 193) | 6 | 3.1 (0.7–5.6) | 20 ‡ | 10.4 (6.1–14.7) | 26 | 13.5 (8.7–18.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhatta, S.; Mytton, J.; Joshi, E.; Bhatta, S.; Adhikari, D.; Manandhar, S.R.; Joshi, S.K. Development and Evaluation of a Community Surveillance Method for Estimating Deaths Due to Injuries in Rural Nepal. Int. J. Environ. Res. Public Health 2021, 18, 8912. https://doi.org/10.3390/ijerph18178912
Bhatta S, Mytton J, Joshi E, Bhatta S, Adhikari D, Manandhar SR, Joshi SK. Development and Evaluation of a Community Surveillance Method for Estimating Deaths Due to Injuries in Rural Nepal. International Journal of Environmental Research and Public Health. 2021; 18(17):8912. https://doi.org/10.3390/ijerph18178912
Chicago/Turabian StyleBhatta, Santosh, Julie Mytton, Elisha Joshi, Sumiksha Bhatta, Dhruba Adhikari, Sunil Raja Manandhar, and Sunil Kumar Joshi. 2021. "Development and Evaluation of a Community Surveillance Method for Estimating Deaths Due to Injuries in Rural Nepal" International Journal of Environmental Research and Public Health 18, no. 17: 8912. https://doi.org/10.3390/ijerph18178912
APA StyleBhatta, S., Mytton, J., Joshi, E., Bhatta, S., Adhikari, D., Manandhar, S. R., & Joshi, S. K. (2021). Development and Evaluation of a Community Surveillance Method for Estimating Deaths Due to Injuries in Rural Nepal. International Journal of Environmental Research and Public Health, 18(17), 8912. https://doi.org/10.3390/ijerph18178912