
Provision of Psychodynamic Psychotherapy in Austria during the COVID-19 Pandemic: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measures
- Psychodynamic orientation in which patients are treated: Guided Affective Imagery, Hypnosis, Autogenous Relaxation, others
- Format they are currently providing psychotherapy (videoconferencing, telephone, in-person with and without additional safety measures)
- Provision of remote psychotherapy (videoconferencing, telephone) before COVID-19 (no, often, from time to time, rarely)
- Attitudes toward remote psychotherapy (videoconferencing, telephone) before COVID-19 (retrospectively) as well as in the current situation (5-point scale from 1 “very good” to 5 “very critically”)
- Number of adult patients, adolescents and children treated before the COVID-19 lockdown
- Number of adult patients, adolescents and children treated since the COVID-19 lockdown (16 March 2020) via videoconferencing, via telephone, in personal contact with and without additional safety measures
- Number of therapies per patient group (adult patients, adolescents, children) suspended and terminated since the COVID-19 lockdown
- Planned psychotherapy format directly after the lockdown
- Planned psychotherapy format until the end of the COVID-19 pandemic
- Planned psychotherapy format after the COVID-19 pandemic
- Perception of any limitations/difficulties or benefits of remote psychotherapy (a number of free-text questions were also included; however, results of this analysis will be published separately)
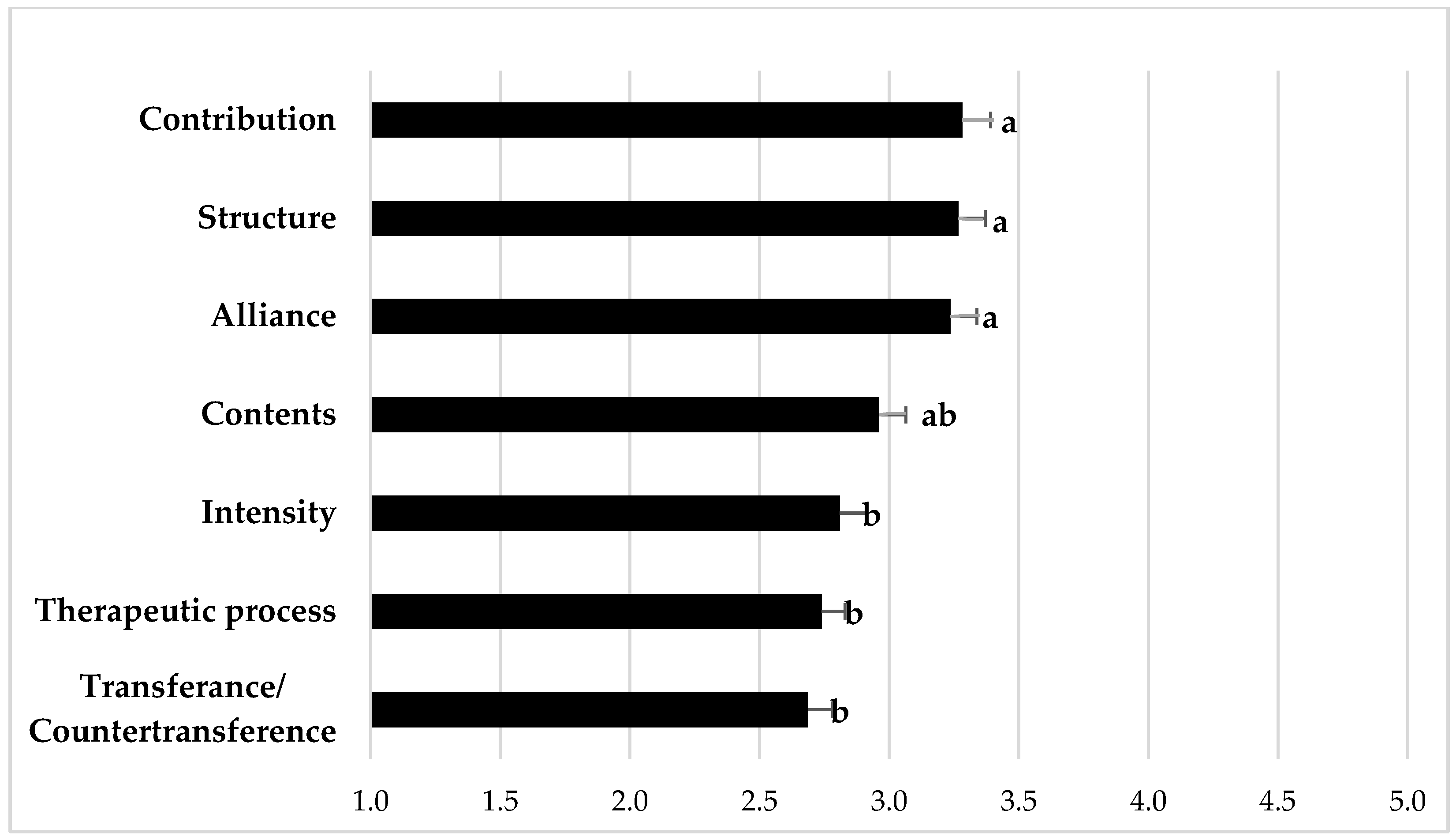
- Rating of potential experienced changes through the remote setting (videoconferencing, telephone) concerning seven aspects (therapeutic alliance, therapeutic process, content of sessions, patients’ and therapists’ contribution to the therapeutic dialogue, intensity of sessions, structure of sessions, transference-countertransference) on a 5-point scale from 1 “very strong change” to 5 “no change”
- Estimated willingness of different groups of patients to switch to remote psychotherapy (telephone or videoconferencing) on a 5-point scale from 1 “very high willingness” to 5 “very low willingness” for the following groups: patients with psychiatric disorders; clients without psychiatric disorders, e.g., clients undergoing psychotherapy for personality development; specific groups of psychiatric diagnosis (delusional disorders, affective disorders, somatoform disorders, personality disorders); and different levels of personality structure (high, medium, low)—these categories were derived from a psychodynamic model used to organize disorders along a structural continuum of severity, with high referring to a neurotic level (i.e., the healthiest level of personality organization, describing people with intact reality testing, a consistent sense of self and others and mature defense mechanisms), low referring to a borderline level (i.e., a low level of personality organization, describing people with difficulties with reality testing, an inconsistent sense of self and others and primitive defense functioning), and medium referring to the level at the transition between the neurotic and borderline level [17].
2.3. Statistics
3. Results
3.1. Study Sample
3.2. Changes in the Provision of Psychotherapy Due to the COVID-19 Lockdown
3.3. Provision of Psychotherapy after the COVID-19 Lockdown
3.4. Attitudes toward Remote Psychotherapy
3.5. Willingness of Patients to Switch to Remote Psychotherapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swartz, H.A. The role of psychotherapy during the COVID-19 pandemic. Am. J. Psychother. 2020, 73, 41–42. [Google Scholar] [CrossRef] [PubMed]
- Probst, T.; Stippl, P.; Pieh, C. Changes in provision of psychotherapy in the early weeks of the COVID-19 lockdown in Austria. Int. J. Environ. Res. Public Health 2020, 17, 3815. [Google Scholar] [CrossRef]
- Humer, E.; Thomas, P. Provision of Remote Psychotherapy during the COVID-19 Pandemic. Digit. Psychol. 2020, 1, 27–31. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Dale, R.; Budimir, S.; Probst, T.; Stippl, P.; Pieh, C. Mental health during a COVID-19 lockdown over the Christmas period in Austria. SSRN Electron. J. 2021. [Google Scholar] [CrossRef]
- Humer, E.; Stippl, P.; Pieh, C.; Pryss, R.; Probst, T. Psychodynamic, humanistic, systemic, and behavioral psychotherapists’ experiences with remote psychotherapy during COVID-19 in Austria: A cross-sectional online survey (Preprint). J. Med. Internet Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.L.; Miller, C.J.; Lindsay, J.A.; Bauer, M.S. A systematic review of providers’ attitudes toward telemental health via videoconferencing. Clin. Psychol. Sci. Pract. 2020. [Google Scholar] [CrossRef]
- Humer, E.; Sitppl, P.; Pieh, C.; Pryss, R.; Probst, T. Experiences of Psychotherapists With Remote Psychotherapy During the COVID-19 Pandemic: Cross-sectional Web-Based Survey Study. J. Med. Internet Res. 2020. [Google Scholar] [CrossRef]
- Backhaus, A.; Agha, Z.; Maglione, M.L.; Repp, A.; Ross, B.; Zuest, D.; Rice-Thorp, N.M.; Lohr, J.; Thorp, S.R. Videoconferencing psychotherapy: A systematic review. Psychol. Serv. 2012. [Google Scholar] [CrossRef]
- Bashshur, R.L.; Shannon, G.W.; Bashshur, N.; Yellowlees, P.M. The Empirical Evidence for Telemedicine Interventions in Mental Disorders. Telemed. e-Health 2016. [Google Scholar] [CrossRef] [Green Version]
- Jenkins-Guarnieri, M.A.; Pruitt, L.D.; Luxton, D.D.; Johnson, K. Patient perceptions of telemental health: Systematic review of direct comparisons to in-person psychotherapeutic treatments. Telemed. e-Health 2015. [Google Scholar] [CrossRef]
- Langarizadeh, M.; Tabatabaei, M.S.; Tavakol, K.; Naghipour, M.; Rostami, A.; Moghbeli, F. Telemental health care, an effective alternative to conventional mental care: A systematic review. Acta Inf. Med. 2017. [Google Scholar] [CrossRef] [Green Version]
- Lopez, A.; Schwenk, S.; Schneck, C.D.; Griffin, R.J.; Mishkind, M.C. Technology-Based Mental Health Treatment and the Impact on the Therapeutic Alliance. Curr. Psychiatry Rep. 2019. [Google Scholar] [CrossRef]
- Austrian Federal Ministry of Social Affairs, Health, Care, and Consumer Protection. PsychotherapeutInnenliste. Available online: http://psychotherapie.ehealth.gv.at/ (accessed on 1 August 2021).
- Engard, N.C. LimeSurvey http://limesurvey.org. Public Serv. Q. 2009. [Google Scholar] [CrossRef]
- Heidegger, K.E. The Situation of Psychotherapy in Austria. Available online: https://www.europsyche.org/app/uploads/2019/05/Situation-Psychotherapy-in-Austria-2017-10-20.pdf (accessed on 8 March 2021).
- Ermann, M. Psychosomatische Medizin und Psychotherapie, 5th ed.; Kohlhammer: Stuttgart, Germany, 2007; pp. 87–115. [Google Scholar]
- Humer, E.; Pieh, C.; Kuska, M.; Barke, A.; Doering, B.K.; Gossmann, K.; Trnka, R.; Meier, Z.; Kascakova, N.; Tavel, P.; et al. Provision of Psychotherapy during the COVID-19 Pandemic among Czech, German and Slovak Psychotherapists. Int. J. Environ. Res. Public Health 2020, 17, 4811. [Google Scholar] [CrossRef] [PubMed]
- Caparrotta, L. Digital technology is here to stay and the psychoanalytic community should grapple with it. Psychoanal. Psychother. 2013, 296–305. [Google Scholar] [CrossRef]
- Johansson, R.; Ekbladh, S.; Hebert, A.; Lindström, M.; Möller, S.; Petitt, E.; Poysti, S.; Larsson, M.H.; Rousseau, A.; Carlbring, P.; et al. Psychodynamic Guided Self-Help for Adult Depression through the Internet: A Randomised Controlled Trial. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Scharff, J.S. Clinical issues in analyses over the telephone and the internet. Int. J. Psychoanal. 2012, 93, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Chherawala, N.; Shane, G. Up-to-date review of psychotherapy via videoconference: Implications and recommendations for the RANZCP Psychotherapy Written Case during the COVID-19 pandemic. Australas. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- Migone, P. Psychoanalysis on the Internet: A Discussion of its Theoretical Implications for Both Online and Offline Therapeutic Technique. Psychoanal. Psychol. 2013, 30, 281–299. [Google Scholar] [CrossRef]
- Bayles, M. Is Physical Proximity Essential to the Psychoanalytic Process? An Exploration Through the Lens of Skype? Psychoanal. Dial. 2012, 22, 569–585. [Google Scholar] [CrossRef]
- Brenes, G.A.; Ingram, C.W.; Danhauer, S.C. Benefits and Challenges of Conducting Psychotherapy by Telephone. Prof. Psychol. Res. Prac. 2012, 42, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Roesler, C. Tele-analysis: The use of media technology in psychotherapy and its impact on the therapeutic relationship. J. Anal. Psychol. 2017, 62, 372–394. [Google Scholar] [CrossRef]
- Huscsava, M.; Plener, P.; Kothgassner, O.D. Teletherapy for Adolescent Psychiatric Outpatients: The Soaring Flight of so far Idle Technologies during the COVID-19 Pandemic. Digit. Psychol. 2020. [Google Scholar] [CrossRef]
- Probst, T.; Haid, B.; Schimböck, W.; Reisinger, A.; Gasser, M.; Eichberger-Heckmann, H.; Stippl, P.; Jesser, A.; Humer, E.; Korecka, N.; et al. Therapeutic interventions in in-person and remote psychotherapy: Survey with psychotherapists and patients experiencing in-person and remote psychotherapy during COVID-19. Clin. Psychol. Psychother. 2021. [Google Scholar] [CrossRef] [PubMed]
- Adler, G.; Pritchett, L.R.; Kauth, M.R.; Nadorff, D. A pilot project to improve access to Telepsychotherapy at rural clinics. Telemed. e-Health 2014. [Google Scholar] [CrossRef] [PubMed]
- Elford, R.; White, H.; Bowering, R.; Ghandi, A.; Maddiggan, B.; St John, K.; House, M.; Harnett, J.; West, R.; Battcock, A. A randomized, controlled trial of child psychiatric assessments conducted using videoconferencing. J. Telemed. Telecare 2000. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, T.L.; Hogan, J.B.; Keegan, F.; Davis, M.L.; Wassef, M.; Day, S.; Lindsay, J.A. Recent Advances in Delivering Mental Health Treatment via Video to Home. Curr. Psychiatry Rep. 2018, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | n | % |
|---|---|---|
| Gender | ||
| Female | 131 | 81.4 |
| Male | 28 | 17.4 |
| Others | 2 | 1.2 |
| Age | ||
| ≤40 | 23 | 14.3 |
| 41–50 | 62 | 38.5 |
| 51–60 | 46 | 28.6 |
| >60 | 30 | 18.6 |
| Years in profession | ||
| ≤5 | 45 | 28.0 |
| 5.1–10 | 40 | 24.8 |
| 10.1–20 | 40 | 24.8 |
| >20 | 36 | 22.4 |
| Psychodynamic Orientation 1 | ||
| Guided affective imagery | 132 | 72.9 |
| Autogenous relaxation | 8 | 4.4 |
| Hypnosis | 32 | 17.7 |
| Others | 9 | 5.0 |
| Patient Group | Before COVID-19 Lockdown, M (SD) | During COVID-19 Lockdown, M (SD) | Statistics |
|---|---|---|---|
| Adults | 13.34 | 10.53 | ME “change” F (1; 6.137) = 48.639; p < 0.001 |
| (7.66) | (7.88) | ||
| Adolescents | 1.24 | 0.98 | ME “patient group” F (1.138; 66.376) = 353.188; p < 0.001 |
| (2.66) | (2.24) | ||
| Children | 0.63 | 0.35 | IE “change × patient group” |
| (2.13) | (1.65) | F (1.251; 10.392) = 26.522; p < 0.001 |
| Patient Group | M | SD | Statistics |
|---|---|---|---|
| Adults | |||
| Videoconferencing | 4.34 | 4.54 | ME “format” F (2; 8.706) = 4.906; p = 0.010 |
| Telephone | 3.35 | 4.07 | |
| In-person | 2.85 | 4.77 | |
| ME “patient group” F (2; 12.732) = 243.736; p < 0.001 | |||
| Adolescents | |||
| Videoconferencing | 0.460 | 1.35 | |
| Telephone | 0.286 | 0.88 | IE “format × patient group” |
| In-person | 0.236 | 0.75 | F (2.065; 12.621) = 4.179; p = 0.015 |
| Children | |||
| Videoconferencing | 0.106 | 0.46 | |
| Telephone | 0.118 | 0.82 | |
| In-person | 0.130 | 1.22 |
| Patient Group | Percentage (SD) | Statistics |
|---|---|---|
| Adults | Suspended: | |
| Suspended | 26.72 (25.57) | F(1.397; 0.431) = 1.710; |
| Terminated | 1.11 (3.14) | p = 0.201 |
| Adolescents | ||
| Suspended | 47.02 (82.30) | Terminated: |
| Terminated | 1.33 (0.07) | F(1.292; 0.002) = 0.947; |
| Children | p = 0.362 | |
| Suspended | 54.44 (42.09) | |
| Terminated | 0.00 (0.00) |
| n | % | |
|---|---|---|
| Already switched all remote psychotherapies back to in-person format | 21 | 13.0 |
| Yes, will switch all remote psychotherapies to in-person | 59 | 36.6 |
| Yes, partially | 59 | 36.6 |
| No, not yet | 22 | 13.7 |
| n | % | |
|---|---|---|
| I will wear a mask | 26 | 18.7 |
| Patients have to wear a mask | 22 | 15.8 |
| I will keep a safe distance of 1 m | 137 | 98.6 |
| I will disinfect all surfaces in the practice regularly | 127 | 91.4 |
| Other measures (e.g., face shield, keeping the window open) | 87 | 62.6 |
| I will apply no additional safety measures | 0 | 0 |
| n | % | |
|---|---|---|
| Yes, I feel more comfortable with it | 8 | 5.0 |
| Yes, if the patient feels more comfortable with it | 86 | 53.4 |
| Yes, if there is no other way | 57 | 35.4 |
| No | 10 | 6.2 |
| Diagnosis | M | SD | Statistics |
|---|---|---|---|
| Delusional disorder | 3.17 | 1.581 | F(2.143; 1.058) = 3.723; |
| Affective disorder | 2.39 | 1.243 | p = 0.031 |
| Somatoform disorder | 2.28 | 1.274 | |
| Personality disorder | 2.61 | 1.290 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jesser, A.; Muckenhuber, J.; Lunglmayr, B.; Dale, R.; Humer, E. Provision of Psychodynamic Psychotherapy in Austria during the COVID-19 Pandemic: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 9046. https://doi.org/10.3390/ijerph18179046
Jesser A, Muckenhuber J, Lunglmayr B, Dale R, Humer E. Provision of Psychodynamic Psychotherapy in Austria during the COVID-19 Pandemic: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(17):9046. https://doi.org/10.3390/ijerph18179046
Chicago/Turabian StyleJesser, Andrea, Johanna Muckenhuber, Bernd Lunglmayr, Rachel Dale, and Elke Humer. 2021. "Provision of Psychodynamic Psychotherapy in Austria during the COVID-19 Pandemic: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 17: 9046. https://doi.org/10.3390/ijerph18179046
APA StyleJesser, A., Muckenhuber, J., Lunglmayr, B., Dale, R., & Humer, E. (2021). Provision of Psychodynamic Psychotherapy in Austria during the COVID-19 Pandemic: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(17), 9046. https://doi.org/10.3390/ijerph18179046