
Gender Differences in Depressive Traits among Rural and Urban Chinese Adolescent Students: Secondary Data Analysis of Nationwide Survey CFPS



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Ethical Considerations
2.3. Measurements
2.3.1. Depressive Traits
2.3.2. Demographic Variables
2.4. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Confirmatory Factor Analysis (CFA) Model
3.3. Measurement Invariance Tests
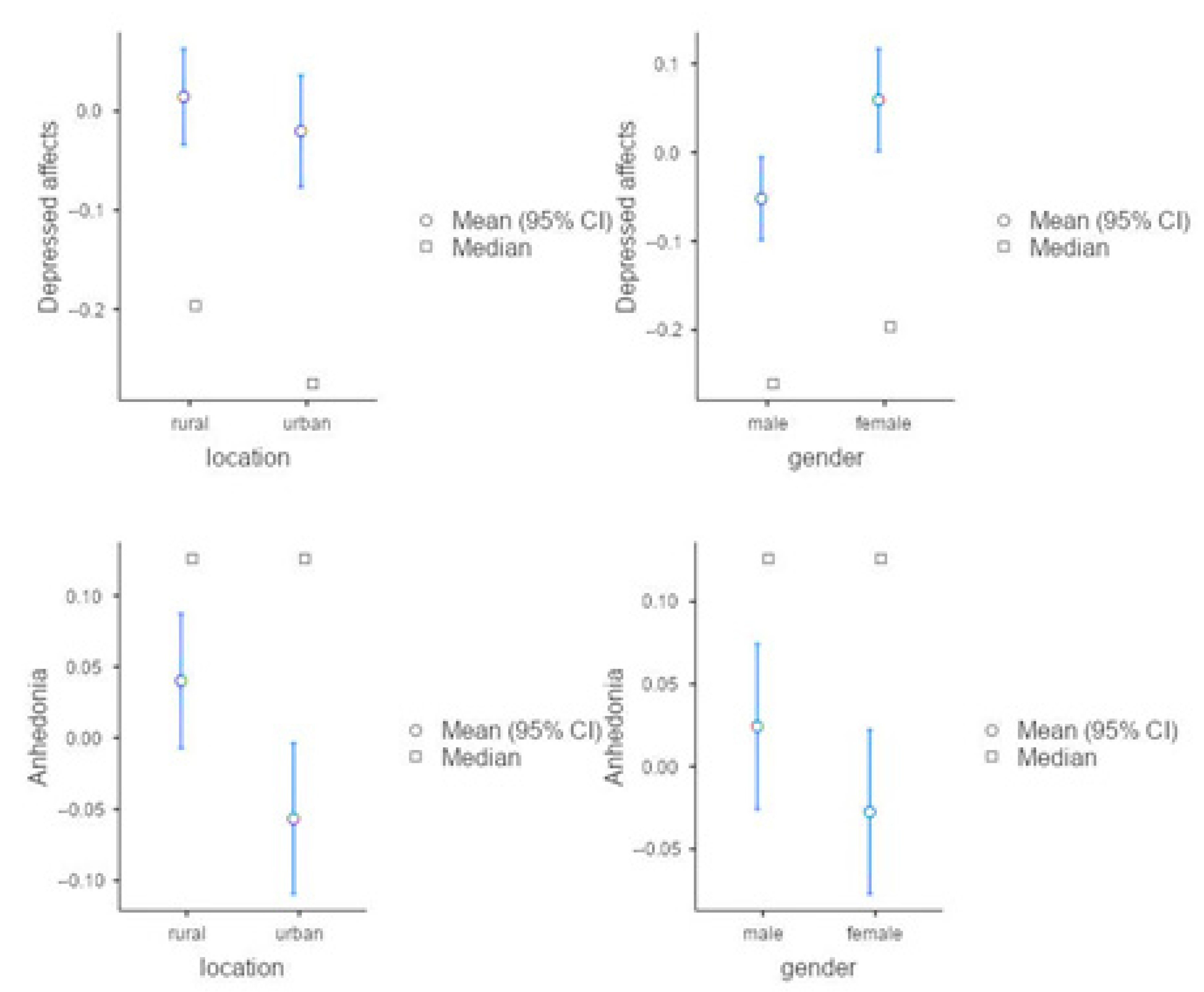
3.4. Multivariate Analysis of Variance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, L.; Chen, X.; Li, H. Bullying victimization, school belonging, academic engagement and achievement in adolescents in rural China: A serial mediation model. Child. Youth Serv. Rev. 2020, 113, 104946. [Google Scholar] [CrossRef]
- Lu, S. Family migration and youth psychosocial development: An ecological perspective. Child. Youth Serv. Rev. 2020, 113, 104953. [Google Scholar] [CrossRef]
- Li, J.; Shi, L.; Liang, H.; Ding, G.; Xu, L. Urban-rural disparities in health care utilization among Chinese adults from 1993 to 2011. BMC Health Serv. Res. 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Y.; Zhou, X. Income inequality in today’s China. Proc. Natl. Acad. Sci. USA 2014, 111, 6928–6933. [Google Scholar] [CrossRef] [Green Version]
- Wu, X. The Household Registration System and Rural-Urban Educational Inequality in Contemporary China. Chin. Soc. Rev. 2011, 44, 31–51. [Google Scholar] [CrossRef]
- Hao, L.; Hu, A.; Lo, J. Two Aspects of the Rural-Urban Divide and Educational Stratification in China: A Trajectory Analysis. Comp. Educ. Rev. 2014, 58, 509–536. [Google Scholar] [CrossRef] [Green Version]
- Bronfenbrenner, U. The Ecology of Human Development; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Ellonen, N.; Kääriäinen, J.; Autio, V. Adolescent depression and school social support: A multilevel analysis of a Finnish sample. J. Commun. Psychol. 2008, 36, 552–567. [Google Scholar] [CrossRef]
- Wentzel, K.R. Socialisation in School Settings. In Handbook of Socialization: Theory and Research; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Beaudry, M.B.; Swartz, K.; Miller, L.; Schweizer, B.; Glazer, K.; Wilcox, H. Effectiveness of the Adolescent Depression Awareness Program (ADAP) on Depression Literacy and Mental Health Treatment. J. Sch. Health 2019, 89, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, M.; Paprock, K. Teacher Job Satisfaction and Retention: A Comparison Study between the US and China. 2006. Available online: https://eric.ed.gov/?id=ED492688 (accessed on 1 August 2021).
- Peng, W.-J.; McNess, E.; Thomas, S.; Wu, X.R.; Zhang, C.; Li, J.Z.; Tian, H.S. Emerging perceptions of teacher quality and teacher development in China. Int. J. Educ. Dev. 2014, 34, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Rabinowitz, T.; Murphy, K.M.; Amour, J.L.; Ricci, M.A.; Caputo, M.P.; Newhouse, P.A. Benefits of a Telepsychiatry Consultation Service for Rural Nursing Home Residents. Telemed. e-Health 2010, 16, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Hankin, B.L.; Abramson, L.Y. Development of gender differences in depression: Description and possible explanations. Ann. Med. 1999, 31, 372–379. [Google Scholar] [CrossRef]
- Afifi, M. Gender differences in mental health. Singap. Med. J. 2007, 48, 385. [Google Scholar]
- Chandra, A.; Minkovitz, C.S. Stigma starts early: Gender differences in teen willingness to use mental health services. J. Adolesc. Health 2006, 38, 754.e1–754.e8. [Google Scholar] [CrossRef] [PubMed]
- Flisher, A.J.; Kramer, R.A.; Grosser, R.C.; Alegria, M.; Bird, H.R.; Bourdon, K.H.; Goodman, S.H.; Greenwald, S.; Horwitz, S.M.; Moore, R.E.; et al. Correlates of unmet need for mental health services by children and adolescents. Psychol. Med. 1997, 27, 1145–1154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, M.-Y.; Sarri, R. Women’s health status and gender inequality in China. Soc. Sci. Med. 1997, 45, 1885–1898. [Google Scholar] [CrossRef]
- Hesketh, T.; Ding, Q.J.; Jenkins, R. Suicide ideation in Chinese adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 230–235. [Google Scholar] [CrossRef]
- Pritchard, C. Suicide in the People’s Republic of China categorized by age and gender: Evidence of the influence of culture on suicide. Acta Psychiatr. Scand. 1996, 93, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Liu, X. The relation analysis of anxiety, depression and quality of sleeping in college students. Chin. Ment. Health J. 1997, 11, 25–33. [Google Scholar]
- Hershatter, G.; Zheng, W. Chinese History: A Useful Category of Gender Analysis. Am. Hist. Rev. 2008, 113, 1404–1421. [Google Scholar] [CrossRef]
- Greenberger, E.; Chen, C.; Tally, S.R.; Dong, Q. Family, peer, and individual correlates of depressive symptomatology among US and Chinese adolescents. J. Consult. Clin. Psychol. 2000, 68, 209. Available online: https://content.apa.org/record/2000-15237-002 (accessed on 1 August 2021). [CrossRef]
- Law, S.; Liu, P. Suicide in China: Unique demographic patterns and relationship to depressive disorder. Curr. Psychiatry Rep. 2008, 10, 80–86. [Google Scholar] [CrossRef]
- Kleinman, A.; Kleinman, J. The transformation of everyday social experience: What a mental and social health perspective reveals about Chinese communities under global and local change. Cult. Med. Psychiatry 1999, 23, 7–24. [Google Scholar] [CrossRef]
- Oakley, A. The Ann Oakley Reader: Gender, Women and Social Science; Bristol University Press: Bristol, UK, 2005. [Google Scholar]
- Karam, A. Girls’ education and gender socialisation in the Mediterranean. Educ. Res. Gend. 2010, 47–63. Available online: https://www.iss.europa.eu/sites/default/files/EUISSFiles/10papers_04_Education-Research-Gender_0.pdf (accessed on 1 August 2021).
- Zhou, Q.; Fan, L.; Yin, Z. Association between family socioeconomic status and depressive symptoms among Chinese adolescents: Evidence from a national household survey. Psychiatry Res. 2018, 259, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M. Age changes in depressive disorders: Some developmental considerations. Dev. Emot. Regul. Disregul. 1991, 273–300. [Google Scholar] [CrossRef]
- Allgood-Merten, B.; Lewinsohn, P.M.; Hops, H. Sex differences and adolescent depression. J. Abnorm. Psychol. 1990, 99, 55. [Google Scholar] [CrossRef] [PubMed]
- Bayram, N.; Bilgel, N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Tao, F.; Hao, J.; Wan, Y. The Mediating Effects of Stress and Coping on Depression among Adolescents in China. J. Child Adolesc. Psychiatr. Nurs. 2010, 23, 173–180. [Google Scholar] [CrossRef]
- Xie, Y.; Zhang, X.; Tu, P.; Ren, Q. China Family Panel Studies User’s Manual; Peking University: Beijing, China, 2017. [Google Scholar]
- Studies CFP. Zhongguo Jiating Zhuizong Diaocha 2018 Nian Huizong Wenjuan [China Family Panel Studies 2018 Questionnaires]. Available online: https://www.isss.pku.edu.cn/cfps/docs/20190912173717403310.pdf (accessed on 1 August 2021).
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Matsunaga, Y.; Izumo, T.; Morofuji, Y.; Horie, N.; Hayashi, K.; Matsuo, T. Revascularization for Aplastic or Twiglike Middle Cerebral Artery: A Case Report. J. Stroke Cerebrovasc. Dis. 2018, 27, e78–e79. [Google Scholar] [CrossRef]
- Landis, R.S.; Beal, D.; Tesluk, P.E. A Comparison of Approaches to Forming Composite Measures in Structural Equation Models. Organ. Res. Methods 2000, 3, 186–207. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Gentina, E.; Tang, T.L.-P.; Gu, Q. Do Parents and Peers Influence Adolescents’ Monetary Intelligence and Consumer Ethics? French and Chinese Adolescents and Behavioral Economics. J. Bus. Ethics 2018, 151, 115–140. [Google Scholar] [CrossRef]
- Nugent, G.C.; Kunz, G.M.; Sheridan, S.M.; Glover, T.A.; Knoche, L.L. Rural Education Research in the United States; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Hill, J.P.; Lynch, M.E. The Intensification of Gender-Related Role Expectations during Early Adolescence. Girls Puberty 1983, 1983, 201–228. [Google Scholar] [CrossRef]
- Petersen, A.C.; Sarigiani, P.A.; Kennedy, R.E. Adolescent depression: Why more girls? J. Youth Adolesc. 1991, 20, 247–271. [Google Scholar] [CrossRef] [PubMed]
- Festinger, L. A Theory of Social Comparison Processes. Hum. Relat. 1954, 7, 117–140. [Google Scholar] [CrossRef]
- Tartaglia, S.; Bergagna, E. Social networking sites passive use and its effects on sad-happy mood. Psihologija 2021, 8. [Google Scholar] [CrossRef]
- De Vries, D.A.; Kühne, R. Facebook and self-perception: Individual susceptibility to negative social comparison on Facebook. Pers. Individ. Dif. 2015, 86, 217–221. [Google Scholar] [CrossRef]
- Twenge, J.M.; Campbell, W.K. Self-Esteem and Socioeconomic Status: A Meta-Analytic Review. Pers. Soc. Psychol. Rev. 2002, 6, 59–71. [Google Scholar] [CrossRef]
- The State Council of the People’s Republic of China. Guowuyuan Bangongting Guanyu Yinfa Xiangcun Jiaoshi Zhichi Jihua (2015–2020 Nian) de Tongzhi [Rural Teacher Support Plan (Year 2015–Year 2020)]. 2015. Available online: http://www.gov.cn/zhengce/content/2015-06/08/content_9833.htm (accessed on 26 August 2021).
- Education and Sports Bureau of Nanchong City. Nanchongshi Tiyu He Jiaoyuju Dui Shizhengxie Liujie Yici Huiyi Di 318 Hao Tianan Dafu de Han [Education and Sports Bureau of Nanchong City’s Letter of Reply to Proposal No. 318 of the First Session of the Sixth CPPCC]. 2016. Available online: http://jytyj.nanchong.gov.cn/news/9873.html (accessed on 26 August 2021).
- Wu, L.; Jiao, H.; Ye, L.; Tang, P. Temporal and Spatial Characteristics of Provincial Education Urbanization in China and Its Influencing Factors. Sci. Geogr. Sin. 2018, 38, 58–66. [Google Scholar]
- TCPG of the PR of China. Weishenme Yaozai Chengxiang Pubian Shixing Mianfei Yiwu Jiaoyu [Why It Is Necessary to Promote Free Compulsory Education in Urban and Rual Areas]. 2021. Available online: http://www.gov.cn/2008gzbg/content_923979.htm (accessed on 1 August 2021).
- Qian, M. Female Education Resources and Sustained Regional Development. J. Peking Univ. Soc. Sci. 1997, 4, 84–90. Available online: http://www.shehui.pku.edu.cn/upload/editor/file/20181019/20181019152839_1193.pdf (accessed on 26 August 2021).
- JICA. Zhongguo Xingbie Chayi XInxi Jianshe Diaocha Baogao [Survey Report on Gender Gap in China]; JICA: Tokyo, Japan, 2016.


{kind=link}
| Item | Item-Aspect |
|---|---|
| 1. I felt depressed | depressed affect |
| 2. I felt that everything I did was an effort | depressed affect |
| 3. My sleep was restless | somatic symptom |
| 4. I was happy | anhedonia |
| 5. I felt lonely | depressed affect |
| 6. I enjoyed life | anhedonia |
| 7. I felt sad | depressed affect |
| 8. I could not get “going” | depressed affect |
| Variable | Outcome | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Gender | Female | 1018 | 46.8% |
| Male | 1155 | 53.2% | |
| Region | Rural | 1272 | 58.4% |
| Urban | 901 | 41.5% | |
| Age | 10-year-old | 377 | 17.3% |
| 11-year-old | 368 | 16.9% | |
| 12-year-old | 372 | 17.1% | |
| 13-year-old | 383 | 17.6% | |
| 14-year-old | 388 | 17.9% | |
| 15-year-old | 285 | 13.1% |
| Dimension | Item | Factor Loading |
|---|---|---|
| Depressed Affect | Item 1 | 0.602 |
| Item 2 | 0.458 | |
| Item 3 | 0.399 | |
| Item 5 | 0.656 | |
| Item 7 | 0.696 | |
| Item 8 | 0.473 | |
| Anhedonia | Item 4 | 0.698 |
| Item 6 | 0.756 |
| Model | χ2/df | CFI | TLI | SRMR | RMSEA |
|---|---|---|---|---|---|
| 1. Two-factor structure for the whole sample | 19.369/4 | 0.994 | 0.984 | 0.013 | 0.042 |
| 2. Two-factor structure for male students | 14.306/4 | 0.991 | 0.976 | 0.018 | 0.043 |
| 3. Two-factor structure for female students | 7.561/4 | 0.997 | 0.993 | 0.010 | 0.030 |
| 4. Two-factor structure for urban students | 7.685/4 | 0.996 | 0.991 | 0.013 | 0.032 |
| 5. Two-factor structure for rural students | 6.33/4 | 0.994 | 0.985 | 0.013 | 0.040 |
| Dependent Variable | Sum of Squares | Mean Square | F | p | |
|---|---|---|---|---|---|
| Region | Depressed Affect | 0.6357 | 0.6357 | 0.8385 | 0.36 |
| Anhedonia | 4.9339 | 4.9339 | 7.0116 | 0.008 | |
| Gender | Depressed Affect | 6.5892 | 6.5892 | 8.6911 | 0.003 |
| Anhedonia | 1.5826 | 1.5826 | 2.249 | 0.134 | |
| Gender × Region | Depressed Affect | 0.0473 | 0.0473 | 0.0624 | 0.803 |
| Anhedonia | 1.0315 | 1.0315 | 1.4658 | 0.226 | |
| Residuals | Depressed Affect | 1644.4269 | 0.7581 | ||
| Anhedonia | 1526.2896 | 0.7037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.; Huang, Y.; Riad, A. Gender Differences in Depressive Traits among Rural and Urban Chinese Adolescent Students: Secondary Data Analysis of Nationwide Survey CFPS. Int. J. Environ. Res. Public Health 2021, 18, 9124. https://doi.org/10.3390/ijerph18179124
Chen W, Huang Y, Riad A. Gender Differences in Depressive Traits among Rural and Urban Chinese Adolescent Students: Secondary Data Analysis of Nationwide Survey CFPS. International Journal of Environmental Research and Public Health. 2021; 18(17):9124. https://doi.org/10.3390/ijerph18179124
Chicago/Turabian StyleChen, Weilong, Yi Huang, and Abanoub Riad. 2021. "Gender Differences in Depressive Traits among Rural and Urban Chinese Adolescent Students: Secondary Data Analysis of Nationwide Survey CFPS" International Journal of Environmental Research and Public Health 18, no. 17: 9124. https://doi.org/10.3390/ijerph18179124
APA StyleChen, W., Huang, Y., & Riad, A. (2021). Gender Differences in Depressive Traits among Rural and Urban Chinese Adolescent Students: Secondary Data Analysis of Nationwide Survey CFPS. International Journal of Environmental Research and Public Health, 18(17), 9124. https://doi.org/10.3390/ijerph18179124