
Health Effects Related to Wind Turbine Sound: An Update


Abstract
:1. Introduction
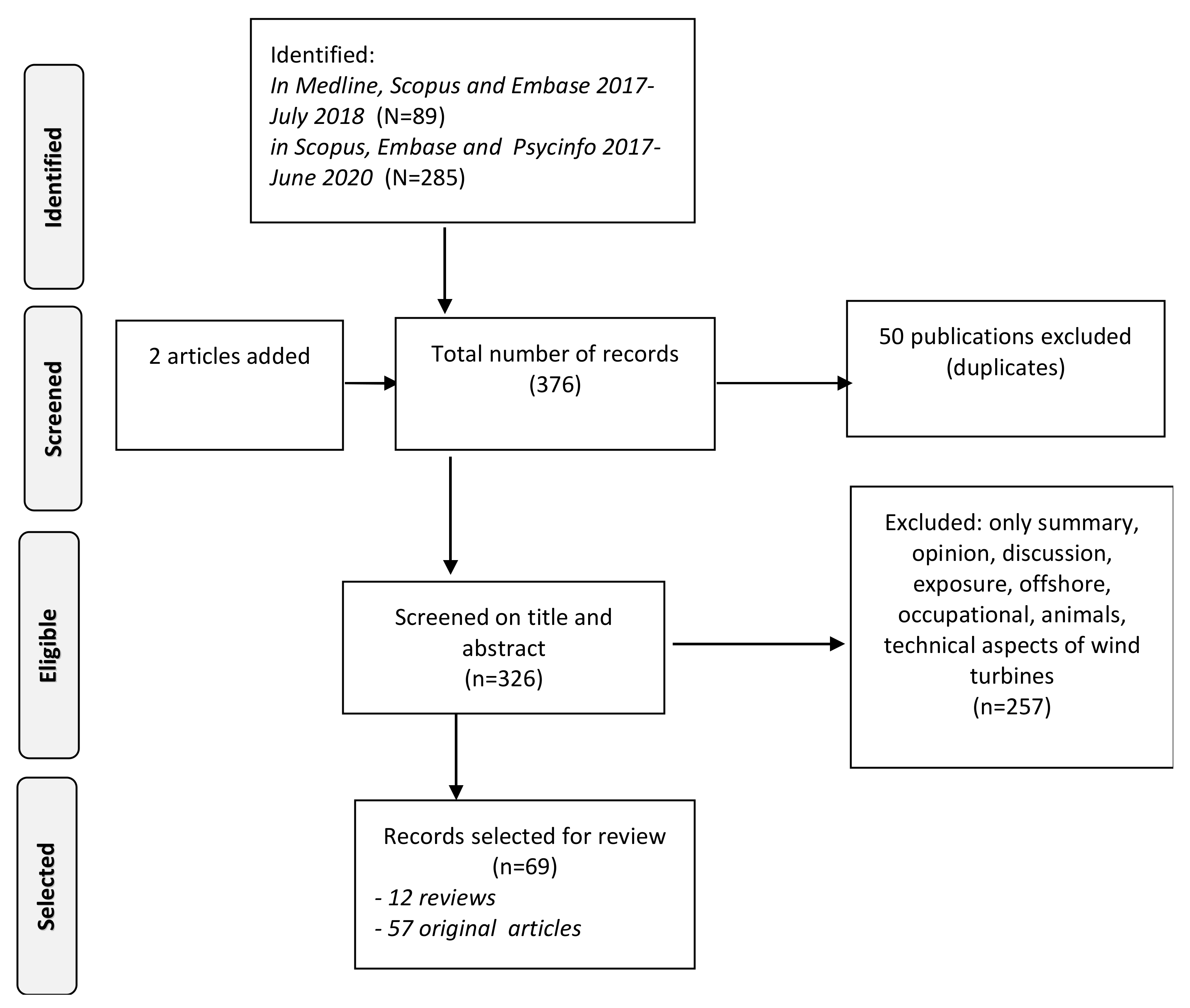
2. Materials and Methods
2.1. Data Sources and Search
2.2. In- and Exclusion Criteria
2.3. Procedure
2.4. Data Extraction
- Acronym/Author and Year of Publication;
- Country;
- Number of studies/participants;
- Study Design (including sampling strategy);
- Quality;
- Exposure source, characterisation and range;
- Outcome type and ascertainment of the outcome.
- Adjustment for possible confounders;
- Direction and strength of reported effect size.
2.5. Assessment of Quality of Evidence
3. Results
3.1. Reviews on Wind Turbine Sound and Health

{kind=link}
| Author | Country | Design | Number Studies/Participants | Time Range | Quality of Evidence | Sound Level Exposure Range | Outcome | Effect Size | Confounders |
|---|---|---|---|---|---|---|---|---|---|
| Basner and McGuire, 2018 [10] | USA | Review | 6 studies (3815) | 2000–2014 | Very low—low | Per 10 dB | Self-reported or physiologically and behavioural measured sleep disturbance | OR = 1.60 (95% CI: 0.86–2.94) not significant, highly heterogenous | No |
| Clark and Paunovic, 2018 [15] | United Kingdom | Review | 5 reviews | 2000–2014 | Low to moderate | Poor, often distance used as proxy | Cognitive effects | No effect | No |
| Clark and Paunovic, 2018 [16] | United Kingdom | Review | 0 | 2000–2014 | Na | Poor, often distance used as proxy | Mental health effects | Not applicable. | No |
| Clark et al., 2020 [17] | United Kingdom | Review | 2 studies | 2014–2020 | Very low to moderate | Poor, often distance used as proxy | Low birth weight, preterm birth, small for gestational age, wellbeing | No effect | No |
| Guski et al., 2017 [4] | Germany | Review | 4 studies | 2000–2014 | Low quality of evidence | Per 5 dB | Annoyance | summary correlation r = 0.278; p = 0.001; 95% CI = 0.11–0.430). | No |
| Freiberg et al., 2019 [9] | Germany | Review | 84 papers/68 studies | 2000–2018 | Reporting quality 46%; 21% generalizable | Sound levels over a range of frequencies, shadow flicker, blinking lights, or vibrations. | Range of self-reported complaints; physiological effects | Age, sex, and socioeconomic status in 28% | |
| Micic et al., 2018 [13] | Australia | Review | 20 studies | 2000–2017 | Not mentioned | % time above 39 dB(A) | Self-reported or physiologically and behavioural measures of sleep disturbance | Attitude NS, economic benefit | |
| Simos et al., 2019 [8] | Switzerland | Review | 104 papers/67 studies | 2000–2019 | Not mentioned | Not mentioned | Annoyance and other impacts | No | |
| van Kempen et al., 2018 [14] | Netherlands | Review | 3 studies | 2000–2014 | Very low | Per 5 dB | Hypertension, IHD, Diabetes, Stroke | Age, gender | |
| van Kamp et al., 2020 [6,7] | Netherlands | Review | 5 studies | 2014–2020 | Low to moderate | Measured, modelled Sound Pressure Level C- and A- weighted | Annoyance, sleep, HBP, stroke, diabetes | demographics, NS, attitude, shadow flicker, Amplitude Modulation |
3.2. Original Studies on WT Sound and Health
3.2.1. Annoyance
| Author | Country | Design † | Sample Size (Response Rate) ‡ | Quality | Exposure Type and Assessment | Outcome Type and Assessment | Confounders Considered in Analyses | Reported Associations |
|---|---|---|---|---|---|---|---|---|
| Klæboe and Sundfor, 2016 [18] | Norway | CS (after) | 90 (38) | Moderate | WT sound pressure level (37–47 dBA LAeq) | Annoyance (ISO 5-point standard scale) | Attitudes, demographics, visual judgements, NS | Noise from WTs evaluated as 17–18 dBA more annoying than road traffic noise (within range of 11–26 dBA reported by [19,20]). Role of non-acoustical factors large |
| Pawlaczyk-Łuszczyń ska, 2018 [21] | Poland | CS | 517 (78) | Moderate | WT calculated sound levels and randomly verified by in situ measurement A-weighted SPL (LAeq,T), A and G-weighted sound pressure levels (LCeq,T and LGeq,T) | Annoyance (ISO 5-point standard scale) | Satisfaction, visual aspects, demographics, attitude | %HA and WT sound level (OR > 1.00) and negative attitude towards WTs; decrease %HA with increasing distance (OR < 1.00), |
| Radun et al., 2019 [22] | Finland | CS | 429 (57) 318 eligible for participation | High | WT A-weighted equivalent SPL, LAeq, and categorized [25–30], [30–35], [35–40] and [40–46] | Annoyance, self-reported sleep disturbance (indoor, outdoor) | Trust in authorities and operators, visibility, economic benefits, age, gender, education, type of dwelling, distance | WT sound level and annoyance outdoor OR 1.41 (1.14, 1.74) < 0.01 (R2 = 0.71) Indoor: none Sleep OR = 1.38 (1.16, 1.65) < 0.01(R2 = 0.50) |
| Song et al., 2016 [23] | China | CS | 227 (77) | Moderate | WT A-weighted equivalent SPL, LAeq, sound levels (44.1–56.7 dBA) | Annoyance, Sleep disturbance (self-reported) | Gender, age residence time, visibility, NS, attitude, general opinion about WTs | %HA increased from 39.5% (95% CI: 28.4–51.4%) to 75.0% (95% CI: 50.9–91.3%. Sleep disturbance and LAeq r2 = 0.209 |
| Michaud et al., 2018b [24] | Canada | CS | 1238 (79) | High | WT calculated sound levels A- and C-weighted Distance; Blinking warning lights, vibrations, visual impact and shadow flicker | Integrated Annoyance score | Age, gender, education, lifestyle, chronic illness, stress, quality of life, dwelling characteristics, | Explained variance 58–69% Annoyance significantly increased in areas between 1 km and 550 m (mean 1.59; 95% CI 1.02, 2.15) and was highest within 550 m (mean 4.25; 95% CI 3.34, 5.16). |
| Michaud et al., 2018c [25] | Canada | CS | 1238 (79) | High | Integrated Annoyance score | Blood pressure Cortisol levels), symptoms Quality of life Nonspecific | Age, gender, education, lifestyle, chronic illness, stress, quality of life, dwelling characteristics, | Total annoyance differed significantly between people reporting one or more symptoms (mean score 2.53 to 3.72) versus those without symptoms (0.96 to 1.41). No association with cortisol concentrations, systolic blood pressure, and rated quality of life was confirmed. |
| Botelho et al., 2017 [26] | Portugal | CS | 80 | Moderate | SPL LAeq | Annoyance, noise mitigating measures | Attitude, NS, visibility, co-ownership | Decisions to insulate house related to WT sound levels, not to annoyance. |
| Hongisto et al., 2017 [27] | Finland | CS | 429 (55) | Moderate | Laeq modelled 26.7–44.2 dB LAeq | Annoyance (4-point scale) | Demographics, NS, residential satisfaction, attitude towards WTs, visibility of WTs, trust towards authorities or operators | Below 40 dB LAeq large WTs (>3 MW) lead to similar indoor noise annoyance levels as smaller ones (<1.5 MW) do |
| Haac et al., 2019 [30] | USA | CS | 1043 (14–28) | Moderate | L1 hr max | Audibility, annoyance (not ISO standard) | Attitude, NS, moving into the area before or after the wind park was operationalized | Audibility annoyance: OR: 11.0; 95% CI: 4.8–25.4). |
| Schäffer et al., 2018 [28] | Switzerland | EXP | 52 | Moderate | AM, Laeq | Annoyance 11-point ISO standard scale | Perceived loudness, perceived sound characteristics | Effect of sound level, AM and visuals |
| Schäffer et al., 2019 [29] | Switzerland | EXP | 43 | High | WT sound (33–49 dBA) synthesized for distances 100–600 m, with and without periodic AM | Annoyance 11-point ISO standard scale | Gender, age, attitude towards WTs, NS and visual aspects | Increase in sound level and AM increased annoyance, presence of visualized landscape decreased annoyance, visibility of WT increased annoyance. Effect of attitude, not of other factors |
| Hübner et al., 2019 [31] | Germany/USA | CS | USA 900 (22%) Germany1029 (28%) | Moderate | Distance A-weighted LAeq-sound pressure level | Health symptoms, annoyance, stress, coping, sleep time, REM, self-reported disturbance | Range of confounders | Distance and SPL not correlated to noise annoyance; NS and attitude regarding fairness strongly associated with stress and annoyance |
| Pohl et al., 2018 [32] | Germany | LO | 212/133 (Before/after 38% | Moderate | A-weighted LAeq sound pressure levels, recordings, distance | Annoyance (5-point ISO standard scale), stress | Attitude | Distance to closest WT (r = –0.13) and ISO SPL: r = 0.27) according to ISO 9613-2 (1993), r = 0.27). |
| Krogh et al., 2019 [33] | Canada | CS | 67 | Na | Distance | Tendency to move | Loss, grief, anxiety | Not mentioned |
3.2.2. Sleep
| Author | Country | Design † | Sample Size (Response Rate) ‡ | Quality | Exposure Type and Assessment | Outcome Type and Assessment | Confounders Considered in Analyses | Reported Associations |
|---|---|---|---|---|---|---|---|---|
| Lane et al., 2016 [11] | Canada | CS | 27 | Low | Noise measurements in bedroom (LAeq and LAmax) for 5 consecutive nights | Actigraphy Subjective variables of sleep: Sleep diary | Age, gender | No statistically significant differences were found between the two groups on any of the objective and subjective sleep measures after adjustment for gender and age. |
| Poulsen et al., 2019 [34] | Denmark | CS | 583,968 addresses after exclusion of people who emigrated | Moderate | A-weighted sound pressure level (10–10,000 Hz) outdoor and A weighted Low Frequency sound pressure level indoor (10–60 Hz) | Sleep (prescribed medication) | Age, gender, income, education, marital status Dwelling, distance to the road | Five-year mean outdoor night-time WT sound level of ≥42 dB was associated with a hazard ratio (HR) = 1.14 (95% CI: 0.98, 1.33) for sleep medication. Indoor night-time LF_WT among persons ≥ 65 exposed to ≥15 dB HR = 1.37 (0.81, 2.31) for sleep medication |
| Radun et al., 2019 [22] | Finland | CS | 429 (57) 318 eligible | High | WT A-weighted equivalent SPL, LAeq, sound levels modelled and categorized [25–30], [30–35], [35–40] and [40–46] | Annoyance, self-reported sleep disturbance (in/outdoor) | Trust in authorities and operators, visibility, economic benefits, age, gender, education, type of dwelling, distance | Sound level and annoyance outdoor OR = 1.41 (1.14, 1.74) <0.01 (r2 = 0.71) Indoor: none Sleep 1.38 (1.16, 1.65) p < 0.01 (r2 = 0.50) |
| Morsing et al., 2018 [35] | Sweden | EXP | 6 | Low | AM, Frequency and beats predictors (taped) | Sleep (objective and subjective measures) | Age, gender | Chi2 8–15 (subjective sleep disturbance Chi2 7–11: Awakenings |
| Smith et al., 2019 [36] | Sweden | EXP | 50 | High | AM, Frequency and beats/slag predictors if bad sleep (taped) | Self-reported sleep quality and physiological measures | Subjective stress and NS | Longer REM sleep latency (+16.8 min) and lower amount of REM sleep (−11.1 min, −2.2%) in WTN nights. No effect on other measures. |
| Song et al., 2016 [23] | China | CS | 227 (77) | Moderate | WT sound measurements, 5 noise level categories (44.1–56.7 dBA Lden) | Annoyance, Sleep disturbance (self-reported) | Gender, age residence time, visibility, NS, attitude, general opinion about WTs | %HA increased from 39.5% (95% CI: 28.4–51.4%) to 75.0% (95% CI: 50.9–91.3%. Sleep disturbance and LAeq r2 = 0.209 |
| Kageyama et al., 2016 [37] | Japan | CS | 1079 (47) | Moderate | LAeq,n outdoor, estimates per address 36–40 dBA and <35 dBA | Sleep symptoms, insomnia (both self-reported) | Road traffic, NS, attitude towards WTs, age, gender, education | Insomnia more prevalent in areas with levels > 40 at night |
3.2.3. Cardiovascular Effects
3.2.4. Metabolic Effects
3.2.5. Mental Health and Cognitive Effects and Other Effects
3.3. Reviews on Social and Physical Aspects Other Than Noise
3.4. Original Studies on Social and Physical Aspects Other Than Noise
3.4.1. Visual Aspects
| Author | Country | Design † | Quality | Sample Size †† (Response Rate) | Exposure Type and Assessment | Outcome Type and Assessment | Aspects Considered | Reported Associations |
|---|---|---|---|---|---|---|---|---|
| Schäffer et al., 2019 [29] | Switzerland | EXP | High | 43 | (i) Distance to wind turbine (ii) periodic AM (iii) visual setting. | Noise-annoyance rating (11-point ISO standard scale) | NS and visual aspects. | Presence of a visualised landscape decreased annoyance, visibility of WT increased annoyance |
| Delicado et al., 2017 [50] | Portugal | Media analysis | Moderate | Na | Media exposure. | Annoyance | Social aspects: acceptance and opinions. Visual and economic aspects. | Landscape matters are more visible and important and at times sufficient to reject approval or change of the siting of a wind farm. |
| Grima Murcia et al., 2017 [51] | Spain | LAB | Low | 14 | Visual stimuli and EEG | Amount of seconds a picture with or without wind turbines can be seen | Visual aspects | No effect |
| Lamy et al., 2017 [52] | USA | Qual | Low | 15 | Distance to wind turbines | Worry and concern about new projects | Visual impact, economics, noise and flicker effects, safety and personal experience with wind. | Economic benefits and visual aspects most important to participants, followed by noise, hazard to wildlife, and safety concerns. |
| Frantál et al., 2017 [53] | Czech Republic | CS | Moderate | 474 (not mentioned) | (i) Distance to wind turbines, (ii) number of turbines, (iii) capacity and size turbines. | Annoyance | Visual aspects: landscape disruption | e.g., the percentage of participants who found visual disruption of the landscape the most noticeable negative impact. |
| Sklenicka and Zouhar, 2018 [54] | Czech Republic | CS | High | 400 (not mentioned) | Link to the acceptance of wind farms by the public and authorities | Not mentioned. Participants were shown pictures including photoshopped wind turbines. | Visual aspects | Landscape indices, elevation landmarks, elevation variation. Visual impact is also quantified by using a formula. |
| Landeta-Manzano et al., 2018 [55] | Spain | LO Interviews | Moderate | 153 (stake holders and experts) | (i) Main characteristic of the wind turbines. (ii) Frequency rates of sick leaves due to work accidents and Hazard Ratio with regard to the hours of exposure support of wind turbines | Health and safety issues, effects of noise and non-ionizing radiation, ‘perceived’ health risk linked to the level of community involvement | Social aspects: acceptance. Visual aspects, health and safety issues, community involvement and social investment. | Contribution to the community acceptance expressed in negative or positive scores and main actions in relation to safety in health. |
3.4.2. Demographic, Personal, and Socioeconomic Factors
Demographics
Personal Factors
Social, Economic and Political Aspects
| Author | Country | Design † | Quality | Sample Size (Response Rate) †† | Exposure Type and Assessment | Outcome Type and Assessment | Aspects Considered | Reported Associations |
|---|---|---|---|---|---|---|---|---|
| Clark and Botterill, 2018 [68] | Australia | Qual mixed | Low | 22 | Not mentioned | Health effects as a social phenomenon | Social and personal factors: wind turbine syndrome | Qualitative: stake, interest and legitimacy determine competing descriptions about the ‘facts’ of WT health effects. |
| Kongprasit et al., 2017 [67] | Thailand | CS | High | 729 (93) | Public attitude and acceptance to wind farms | Percentage of respondents that work and live in or near the proposed site installations. | Social aspects | No significant differences regarding early brain processing when looking at landscapes with and without solar power systems or wind turbines. |
| Liebe et al., 2017 [63] | Switzerland | Panel, factorial survey, experiment (FSE) | High | 1800 (Panel)) | Public attitude and acceptance to wind farms | (i) Number of turbines (ii) electricity use (iii) distance to turbines. | Social aspects: acceptance and fairness | Overall acceptance levels in numbers of residents. |
| Kim et al., 2018 [70] | Republic of Korea | Interview, media and policy analysis | Low | 7 | Not mentioned | Not mentioned | Social aspects: acceptance. | Not mentioned. |
| Gölz and Wedderhoff, 2018 [71] | Germany | CS | Moderate | 2009 (18) | Not mentioned. | Risk perception of energy system transformation. | Social aspects: acceptance, fairness and attitude | Structural equation model (SEM) using fit indices and descriptive data of regional acceptance figures. |
| Scherhaufer et al., 2017 [65] | Austria | Qual | Moderate | 172 | Not mentioned. | Not mentioned. | Social aspects: Acceptance. Economic aspect, NS, Visual aspects. | Patterns of acceptance and perceived importance defined as very to somewhat important. |
| Langer et al., 2018 [62] | Germany | CS | High | 1400 (Panel) | (i) visibility from place of residence. (ii) Experience with wind energy. (iii) Number of WTs in vicinity, (iiii) Distance to place of residence. | Perceived side effects e.g., fear of infrasound. | Social aspects: acceptance. Visual aspects. Fear of infrasound. | Acceptance of wind turbines: Not affected by distance, Significant association with distributive justice Fear of Infrasound Mixed association with modes of participation |
| Scherhaufer et al., 2018 [72] | Austria | Qual | Moderate | 241 (97/144) | Not mentioned | Not mentioned | Social aspects: acceptance. | Integrating scientific and lay people perspectives as a way forward. |
| Sæþórsdóttiret al., 2018 [73] | Iceland | CS | Moderate | 1351 | No link is made. | (i) Distance to wind turbines. (ii) Capacity and size of wind turbines. (iii) visibility of wind turbine. (iiii) Number of wind turbines. | Acceptance. Economic aspects: tourism and visual aspects for tourists. | One-third of the travellers is less likely to visit the Southern Highlands if a proposed wind farm were built, Two-thirds think that wind turbines would decrease the area’s attractiveness. |
| Wen et al., 2018 [76] | United Kingdom | Literature study: meta-analysis | Low | None. | (i) Distance toWTs (ii) Number of WTs (iii) WT height. | Preference for locating wind farms. | Visual aspects | Willingness To Accept and Willingness To Pay |
| Thomson and Kempton, 2018 [75] | United States | CS | Moderate | 534 (34) | (i) Capacity of WTs (ii) ability to see and hear WTs. (iii) number of days WT is visible (iiii) cardinal direction from front of house. | Attitude towards wind turbines. | Visual aspects, auditory impacts and social aspects. | Amount of dollars (Willingness To Pay) |
3.5. Health-Related Effects of Low-Frequency Sound and Infrasound
3.5.1. Original Studies on Audibility of Infrasound and Low-Frequency Sound
| Author | Country | Design † | Participants ‡ (Age Range) | Exposure Type and Assessment | Outcome Type and Assessment | Reported Associations |
|---|---|---|---|---|---|---|
| Behler and Uppenkamp, 2020 [84] | Germany | LAB | 19 (21–34) | 8 or 32 Hz tones applied monaurally | Loudness and unpleasantness, brain activity | Same brain regions active as for typical audio sound: average in agreement with earlier studies, but large differences between subjects in rating sound |
| Burke et al., 2019 [85] | Germany | LAB | 13 (18–30) | 5 or 12 Hz tones and/or 100 or 1000 Hz or 250–4000 Hz pink noise applied monaurally | Detection threshold of one sound with or without other sound | Detection threshold of audio sound not influenced by IS tones; threshold of IS tones raised by medium loud audio sound |
| Weichenberger et al., 2017 [86] | Germany | LAB | 14 (18–30) | 8 tones in range 2.5–125 Hz applied monaurally | Spatial coherence and temporal independence in brain activity | No brain activity for medium-loud 12 Hz and for no sound; brain activity in AC and two other brain areas for near-threshold sound |
| Jurado and Marquardt, 2020a [88] | United Kingdom | LAB | 13 (20–34) | soft to relatively loud 11 Hz or 38 Hz continuous sound (10–20 min) | Brain (EEG) response in relation to perceived loudness | No relevant effect of sound on EEG |
| Marquardt and Jurado, 2018 [89] | United Kingdom | LAB | 12 (18–49) | 8 Hz tone and 63 or 125 Hz tone, or 63/125 Hz tone modulated at 8 Hz with 25% or 37.5% modulation depth applied to preferred ear | Assessment: is sound amplitude modulated or sum of 8 and 63/125 Hz tone | Participants’ rating of each sound type not better than chance; for all sounds or slightly better |
| Jurado et al., 2019 [90] | Ecuador | LAB | 34 (19–29) | 4 tones (40, 63, 80 and 1000 Hz) and 4 two tone complexes centred at the same 4 frequencies, with frequency differences of 1, 2, 5 and 12 Hz. | Loudness matching of tone and tone complex | Results in agreement with literature and loudness models |
| van Kamp et al., 2017 [91] | Netherlands | CS | 3972 (35) | calculated level of transport and industrial noise | Annoyance from humming noise, NS, residential satisfaction, house insulation | Lower background sound levels at night associated with higher annoyance from humming sounds |
| Maijala et al., 2020 [80,92] | Finland | CS, LAB | survey: 1351 (18–96);lab study: 26 | wind turbine sound samples with highest infrasound levels and amplitude modulation values | Annoyance and physiological response | Participants who reported infrasound-related symptoms not able to perceive infrasound in noise samples and found samples with infrasound not more annoying than those without related symptoms |
| Jurado and Marquardt, 2020b [93] | United Kingdom | LAB | 15 (20–34) | 3 stimuli applied monaurally for 120 s: 6 ms 500 Hz bursts, 5 Hz repetition rate; 500 Hz modulated at 40 Hz 100% modulation depth; 4, 16 or 40 Hz | Myogenic (neck muscle) potential in response to vestibular stimulus | No significant vestibular response at 4 Hz and same for most subjects at 16 Hz |
| Conference papers + reports | ||||||
| Takahashi, 2017 [94] | Japan | LAB | 4 (21–47) | Infrasound stimuli at 16, 20, 25, 3.5, 40 and 50 Hz from speakers | Hearing thresholds (HT) and threshold values for unpleasantness (UT) and vibration in head (VhT) | UT higher than VhT, both higher than HT at all frequencies |
| Krahe et al., 2020 [81] | Germany | LAB | 44 (-) | Infrasound stimuli (3, 5, 10, 18 Hz) above 85 dB(G) and silence | Perception, unpleasantness and physiological response (blood pressure, ECG, EEG, balance tests) | Perception of all sounds, predominantly by ear; no physiological effects; participants with earlier experience of infrasound not more sensitive |
3.5.2. Effect of Lower Frequencies Compared to ‘Normal’ Sound
3.5.3. Sub-Audible Including Vestibular Effects
3.5.4. Effect of Vibrations
4. Discussion
4.1. Summary of the Findings
4.2. Evidence on Adverse Health Effects of WT Sound
4.3. Evidence on the Role of Physical, Social and Personal Factors
4.4. Evidence on Adverse Effects of Low-Frequency Sound and Infrasound
4.5. Strength and Limitations
4.6. Implication for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van den Berg, F.; van Kamp, I. Health Effects Related to Wind Turbine Sound. Commissioned by the Swiss Federal Office for the Environment (FOEN); National Institute for Public Health and the Environment: Bilthoven, The Netherlands, 2017.
- Van Kamp, I.; van den Berg, F. Health effects related to wind turbine sound, including low-frequency sound and infrasound. Acoust. Aust. 2018, 46, 31–57. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Health. 2021. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools, (accessed on 26 August 2021).
- Guski, R.; Schreckenberg, D.; Schuemer, R. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Annoyance. Int. J. Environ. Res. Public Health 2017, 14, 1539. [Google Scholar] [CrossRef] [Green Version]
- International Standard Organization. Acoustics—Assessment of Noise Annoyance by means of Social and Socio-Acoustic Surveys (ISO/TS 15666:2003); International Organization for Standardization: Geneva, Switzerland, 2003. [Google Scholar]
- Van Kamp, I.; Simon, S.; Notley, H.; Baliatsas, C.; van Kempen, E. Evidence Relating to Environmental Noise Exposure and Annoyance, Sleep Disturbance, Cardio-Vascular and Metabolic Health Outcomes in the Context of IGCB (N): A Scoping Review of New Evidence. Int. J. Environ. Res. Public Health 2020, 17, 3016. [Google Scholar] [CrossRef]
- Van Kamp, I.; van Kempen, E.E.M.M.; Simon, S.N.; Baliatsas, C. Review of Evidence Relating to Environmental Noise Exposure and Annoyance, Sleep Disturbance, Cardio-Vascular and Metabolic Health Outcomes in the Context of the Interdepartmental Group on Costs and Benefits Noise Subject Group (IGCB (N)); RIVM Report 2019-0088; National Institute for Public Health and the Environment: Catharijnesingel, The Netherlands, 2020. [CrossRef]
- Simos, J.; Cantoreggi, N.; Christie, D.; Forbat, J. Wind turbines and health: A review with suggested recommendations. Environ. Risques St. 2019, 18, 149–159. [Google Scholar]
- Freiberg, A.; Schefter, C.; Girbig, M.; Murta, V.C.; Seidler, A. Health effects of wind turbines on humans in residential settings: Results of a scoping review. Environ. Res. 2019, 169, 446–463. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; McGuire, S. WHO environmental noise guidelines for the European region: A systematic review on environmental noise and effects on sleep. Int. J. Environ. Res. Public Health 2018, 15, 519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lane, J.D.; Bigelow, P.L.; Majowicz, S.E.; McColl, R.S. Impacts of Industrial Wind Turbine Noise on Sleep Quality: Results From a Field Study of Rural Residents in Ontario Canada. J. Environ. Health 2016, 79, 8–13. [Google Scholar] [PubMed]
- Michaud, D.S.; Feder, K.; Keith, S.E.; Voicescu, S.A.; Marro, L.; Than, J.; Guay, M.; Denning, A.; Murray, B.J.; Weiss, S.K.; et al. Effects of wind turbine noise on self-reported and objective measures of sleep. Sleep 2016, 39, 97–109. [Google Scholar] [CrossRef] [Green Version]
- Micic, G.; Zajamsek, B.; Lack, L.; Hansen, K.; Doolan, C.; Hansen, C.; Mercer, J. A review of the potential impacts of wind farm noise on sleep. Acoust. Aust. 2018, 46, 87–97. [Google Scholar] [CrossRef]
- Van Kempen, E.; Casas, M.; Pershagen, G.; Foraster, M. WHO environmental noise guidelines for the European region: A systematic review on environmental noise and cardiovascular and metabolic effects: A summary. Int. J. Environ. Res. Public Health 2018, 15, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, C.; Paunovic, K. WHO Environmental noise guidelines for the European Region: A systematic review on environmental noise and quality of life, wellbeing and mental health. Int. J. Environ. Res. Public Health 2018, 15, 2400. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.; Paunovic, K. WHO environmental noise guidelines for the european region: A systematic review on environmental noise and cognition. Int. J. Environ. Res. Public Health 2018, 15, 285. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.; Crumpler, C.; Notley, H. Evidence for environmental noise effects on health for the United Kingdom policy context: A systematic review of the effects of environmental noise on mental health, wellbeing, quality of life, cancer, dementia, birth, reproductive outcomes, and cognition. Int. J. Environ. Res. Public Health 2020, 17, 393. [Google Scholar] [CrossRef] [Green Version]
- Klaeboe, R.; Sundfor, H.B. Windmill Noise Annoyance, Visual Aesthetics, and Attitudes towards Renewable Energy Sources. Int. J. Environ. Res. Public Health 2016, 13, 746. [Google Scholar] [CrossRef] [Green Version]
- Michaud, D.S.; Keith, S.E.; Feder, K.; Voicescu, S.A.; Marro, L.; Than, J.; Guay, M.; Bower, T.; Denning, A.; Lavigne, E.; et al. Personal and situational variables associated with wind turbine noise annoyance. J. Acoust. Soc. Am. 2016, 139, 1455–1466. [Google Scholar] [CrossRef] [Green Version]
- Janssen, S.A.; Vos, H.; Eisser, A.R.; Pedersen, E. A comparison between exposure-response relationships for wind turbine annoyance and annoyance due to other noise sources. J. Acoust. Soc. Am. 2011, 130, 3746–3753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawlaczyk-Łuszczyńska, M.; Zaborowski, K.; Dudarewicz, A.; Zamojska Daniszewska, M.; Waszkowska, M. Response to noise emitted by wind farms in people living in nearby areas. Int. J. Environ. Res. Public Health 2018, 15, 1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radun, J.; Hongisto, V.; Suokas, M. Variables associated with wind turbine noise annoyance and sleep disturbance. Build. Environ. 2019, 150, 339–348. [Google Scholar] [CrossRef]
- Song, K.; Di, G.; Xu, Y.; Chen, X. Community survey on noise impacts induced by 2MW wind turbines in China. J. Low Freq. Noise Vib. Act. Control 2016, 35, 279–290. [Google Scholar] [CrossRef]
- Michaud, D.S.; Marro, L.; McNamee, J. Derivation and application of a composite annoyance reaction construct based on multiple wind turbine features. Can. J. Public Health 2018, 109, 242–251. [Google Scholar] [CrossRef] [Green Version]
- Michaud, D.S.; Marro, L.; McNamee, J. The association between self-reported and objective measures of health and aggregate annoyance scores toward wind turbine installations. Can. J. Public Health 2018, 109, 252–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botelho, A.; Arezes, P.; Bernardo, C.; Dias, H.; Pinto, L.M.C. Effect of Wind Farm Noise on Local Residents’ Decision to Adopt Mitigation Measures. Int. J. Environ. Res. Public Health 2017, 14, 753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hongisto, V.; Oliva, D.; Keranen, J. Indoor noise annoyance due to 3-5 megawatt wind turbines-An exposure-response relationship. J. Acoust. Soc. Am. 2017, 142, 2185–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schäffer, B.; Pieren, R.; Schlittmeier, S.J.; Brink, M. Effects of different spectral shapes and amplitude modulation of broadband noise on annoyance reactions in a controlled listening experiment. Int. J. Environ. Res. Public Health 2018, 15, 1029. [Google Scholar] [CrossRef] [Green Version]
- Schäffer, B.; Pieren, R.; Hayek, U.W.; Biver, N.; Grêt-Regamey, A. Influence of visibility of wind farms on noise annoyance–A laboratory experiment with audio-visual simulations. Landsc. Urban Plan. 2019, 186, 67–78. [Google Scholar] [CrossRef]
- Haac, T.R.; Kaliski, K.; Landis, M.; Hoen, B.; Rand, J.; Firestone, J.; Pohl, J. Wind turbine audibility and noise annoyance in a national US survey: Individual perception and influencing factors. J. Acoust. Soc. Am. 2019, 146, 1124–1141. [Google Scholar] [CrossRef] [Green Version]
- Hübner, G.; Pohl, J.; Hoen, B.; Firestone, J.; Rand, J.; Elliott, D.; Haac, R. Monitoring annoyance and stress effects of wind turbines on nearby residents: A comparison of US and European samples. Environ. Int. 2019, 132, 105090. [Google Scholar] [CrossRef]
- Pohl, J.; Gabriel, J.; Hübner, G. Understanding stress effects of wind turbine noise—The integrated approach. Energy Policy 2018, 112, 119–128. [Google Scholar] [CrossRef]
- Krogh, C.M.; McMurtry, R.Y.; Dumbrille, A.; Hughes, D.; Gillis, L. Preliminary Results: Exploring Why Some Families Living in Proximity to Wind Turbine Facilities Contemplate Vacating Their Homes—A Community-Based Study. Open Access Libr. J. 2020, 7, e6118. [Google Scholar] [CrossRef]
- Poulsen, A.H.; Raaschou-Nielsen, O.; Peña, A.; Hahmann, A.N.; Nordsborg, R.B.; Ketzel, M.; Sørensen, M. Impact of long-term exposure to wind turbine noise on redemption of sleep medication and antidepressants: A nationwide cohort study. Environ. Health Perspect. 2019, 127, 037005. [Google Scholar] [CrossRef]
- Morsing Ageborg, J.; Smith, M.G.; Ögren, M.; Thorsson, P.; Pedersen, E.; Forssén, J.; Persson Waye, K. Wind turbine noise and sleep: Pilot studies on the influence of noise characteristics. Int. J. Environ. Res. Public Health 2018, 15, 2573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.G.; Ögren, M.; Thorsson, P.; Hussain-Alkhateeb, L.; Pedersen, E.; Forssén, J.; Ageborg Morsing, J.; Persson Waye, K. A laboratory study on the effects of wind turbine noise on sleep: Results of the polysomnographic WiTNES study. Sleep 2020, 43, zsaa046. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, T.; Yano, T.; Kuwano, S.; Sueoka, S.; Tachibana, H. Exposure-response relationship of wind turbine noise with self-reported symptoms of sleep and health problems: A nationwide socioacoustic survey in Japan. Noise Health 2016, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, A.H.; Raaschou-Nielsen, O.; Peña, A.; Hahmann, A.N.; Nordsborg, R.B.; Ketzel, M.; Sørensen, M. Long-term exposure to wind turbine noise and redemption of antihypertensive medication: A nationwide cohort study. Environ. Int. 2018, 121, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, A.H.; Raaschou-Nielsen, O.; Peña, A.; Hahmann, A.N.; Nordsborg, R.B.; Ketzel, M.; Sørensen, M. Long-term exposure to wind turbine noise and risk for myocardial infarction and stroke: A nationwide cohort study. Environ. Health Perspect. 2019, 2019, 037004. [Google Scholar] [CrossRef] [Green Version]
- Bräuner, E.V.; Jørgensen, J.T.; Duun-Henriksen, A.K.; Backalarz, C.; Laursen, J.E.; Pedersen, T.H.; Andersen, Z.J. Long-term wind turbine noise exposure and incidence of myocardial infarction in the Danish nurse cohort. Environ. Int. 2018, 121, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Bräuner, E.V.; Jørgensen, J.T.; Duun-Henriksen, A.K.; Backalarz, C.; Laursen, J.E.; Pedersen, T.H.; Andersen, Z.J. Association Between Long-Term Exposure to Wind Turbine Noise and the Risk of Stroke: Data From the Danish Nurse Cohort. J. Am. Heart Assoc. 2019, 8, e013157. [Google Scholar] [CrossRef] [Green Version]
- Bräuner, E.V.; Jørgensen, J.T.; Duun-Henriksen, A.K.; Backalarz, C.; Laursen, J.E.; Pedersen, T.H.; Andersen, Z.J. Long-term wind turbine noise exposure and the risk of incident atrial fibrillation in the Danish Nurse cohort. Environ. Int. 2019, 130, 104915. [Google Scholar] [CrossRef]
- Pedersen, E.; Waye, K.P. Wind turbine noise, annoyance and self-reported health and wellbeing in different living environments. Occup. Environ. Med. 2007, 64, 480–486. [Google Scholar] [CrossRef] [Green Version]
- Bakker, R.H.; Pedersen, E.; van den Berg, G.P.; Stewart, R.E.; Lok, W.; Bouma, J. Impact of wind turbine sound on annoyance, selfreported sleep disturbance and psychological distress. Sci. Total Environ. 2012, 425, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, E. Health aspects associated with wind turbine noise: Results from three field studies. Noise Control Eng. J. 2011, 59, 47–53. [Google Scholar] [CrossRef]
- Michaud, D.S.; Feder, K.; Keith, S.E.; Voicescu, S.A.; Marro, L.; Than, J.; Lavigne, E. Exposure to wind turbine noise: Perceptual responses and reported health effects. J. Acoust. Soc. Am. 2016, 139, 1443–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulsen, A.H.; Raaschou-Nielsen, O.; Peña, A.; Hahmann, A.N.; Nordsborg, R.B.; Ketzel, M.; Sørensen, M. Long-term exposure to wind turbine noise at night and risk for diabetes: A nationwide cohort study. Environ. Res. 2018, 165, 40–45. [Google Scholar] [CrossRef]
- Poulsen, A.H.; Raaschou-Nielsen, O.; Peña, A.; Hahmann, A.N.; Nordsborg, R.B.; Ketzel, M.; Sørensen, M. Pregnancy exposure to wind turbine noise and adverse birth outcomes: A nationwide cohort study. Environ. Res. 2018, 167, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Freiberg, A.; Schefter, C.; Hegewald, J.; Seidler, A. The influence of wind turbine visibility on the health of local residents: A systematic review. Int. Arch. Occup. Environ. Health 2019, 92, 609–628. [Google Scholar] [CrossRef] [PubMed]
- Delicado, A.; Truninger, M.; Figueiredo, E.; Silva, L.; Horta, A. A Blot on the landscape: Consensus and Controversies on Wind Farms in Rural Portugal. In Transforming the Rural; Emerald Publishing Limited: Bingley, UK, 2017; Volume 24, pp. 179–195. [Google Scholar]
- Grima Murcia, M.D.; Sanchez Ferrer, F.; Sorinas, J.; Ferrandez, J.M.; Fernandez, E.J. Application of electroencephalographic techniques to the study of visual impact of renewable energies. J. Environ. Manag. 2017, 200, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Lamy, J.; Azevedo, I.M.L.; de Bruine, W.; Morgan, M.G. Perceptions of wind energy projects in two coastal Massachusetts communities. Electr. J. 2017, 30, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Frantál, B.; Van Der Horst, D.; Kunc, J.; Jaňurová, M. Landscape disruption or just a lack of economic benefits? Exploring factors behind the negative perceptions of wind turbines. J. Landsc. Ecol. 2017, 15, 139–147. [Google Scholar]
- Sklenicka, P.; Zouhar, J. Predicting the visual impact of onshore wind farms via landscape indices: A method for objectivizing planning and decision processes. Appl. Energy 2018, 209, 445–454. [Google Scholar] [CrossRef]
- Landeta-Manzano, B.; Arana-Landín, G.; Calvo, P.M.; Heras-Saizarbitoria, I. Wind energy and local communities: A manufacturer’s efforts to gain acceptance. Energy Policy 2018, 121, 314–324. [Google Scholar] [CrossRef]
- Asensio, C.; Gasco, L.; de Arcas, G. A Review of NonAcoustic Measures to Handle Community Response to Noise around Airports. Curr. Pollut. Rep. 2017, 3, 230–244. [Google Scholar] [CrossRef]
- Lercher, P.; De Coensel, B.; Dekonink, L.; Botteldooren, D. Community Response to Multiple Sound Sources: Integrating Acoustic and Contextual Approaches in the Analysis. Int. J. Environ. Res. Public Health 2017, 14, 663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haubrich, J.; Burtea, N.E.; Hooper, P.; Hudson, R.; Radulescu, D.; Rajé, F.; Schreckenberg, D. Foundations for a comprehensive approach of acoustic and non-acoustic measures of aircraft noise annoyance mitigation. In Proceedings of the Aerospace Europe Conference, Bordeaux, France, 25–28 February 2020. [Google Scholar]
- Van Kamp, I.; Davies, H. Noise and health in vulnerable groups: A review. Noise Health 2013, 15, 153–159. Available online: https://www.noiseandhealth.org/text.asp?2013/15/64/153/112361 (accessed on 26 August 2021). [CrossRef] [PubMed]
- Beuret, J.E. Is trust negotiable? Building a place-based general interest for the acceptance of the Saint Brieuc and Saint Nazaire offshore wind farms. Geogr. Econ. Soc. 2016, 18, 335–358. [Google Scholar]
- Brennan, N.; Van Rensburg, T.M.; Morris, C. Public acceptance of large-scale wind energy generation for export from Ireland to the UK: Evidence from Ireland. J. Environ. Plan. Manag. 2017, 60, 1967–1992. [Google Scholar] [CrossRef]
- Langer, K.; Decker, T.; Menrad, K. Public participation in wind energy projects located in Germany: Which form of participation is the key to acceptance? Renew. Energy 2017, 112, 63–73. [Google Scholar] [CrossRef]
- Liebe, U.; Bartczak, A.; Meyerhoff, J. A turbine is not only a turbine: The role of social context and fairness characteristics for the local acceptance of wind power. Energy Policy 2017, 107, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Macdonald, C.; Glass, J.; Creamer, E. What Is the Benefit of Community Benefits? Exploring Local Perceptions of the Provision of Community Benefits from a Commercial Wind Energy Project. Scott. Geogr. J. 2017, 133, 172–191. [Google Scholar] [CrossRef] [Green Version]
- Scherhaufer, P.; Höltinger, S.; Salak, B.; Schauppenlehner, T.; Schmidt, J. Patterns of acceptance and non-acceptance within energy landscapes: Acase study on wind energy expansion in Austria. Energy Policy 2017, 109, 863–870. [Google Scholar] [CrossRef]
- Sonnberger, M.; Ruddat, M. Local and socio-political acceptance of wind farms in Germany. Technol. Soc. 2017, 51, 56–65. [Google Scholar] [CrossRef]
- Kongprasit, S.; Waewsak, J.; Chaichana, T. Wind Turbine and Local Acceptance in Southern Thailand. Energy Procedia 2017, 138, 380–385. [Google Scholar] [CrossRef]
- Clark, S.; Botterill, L.C. Contesting facts about wind farms in Australia and the legitimacy of adverse health effects. Health 2018, 22, 337–355. [Google Scholar] [CrossRef] [Green Version]
- Janhunen, S.; Hujala, M.; Pätäri, S. The acceptability of wind farms: The impact of public participation. J. Environ. Policy Plan. 2018, 20, 214–235. [Google Scholar] [CrossRef]
- Kim, H.; Cho, S.H.; Song, S. Wind, power, and the situatedness of community engagement. Public Underst. Sci. 2018, 28, 38–52. [Google Scholar] [CrossRef]
- Gölz, S.; Wedderhoff, O. Explaining regional acceptance of the German energy transition by including trust in stakeholders and perception of fairness as socio-institutional factors. Energy Res. Soc. Sci. 2018, 43, 96–108. [Google Scholar] [CrossRef]
- Scherhaufer, P.; Höltinger, S.; Salak, B.; Schauppenlehner, T.; Schmidt, J. A participatory integrated assessment of the social acceptance of wind energy. Energy Res. Soc. Sci. 2018, 45, 164–172. [Google Scholar] [CrossRef]
- Sæþórsdóttir, A.D.; Ólafsdóttir, R.; Smith, D. Turbulent times: Tourists’ attitudes towards wind turbines in the Southern Highlands in Iceland. Int. J. Sustain. Energy 2018, 37, 886901. [Google Scholar] [CrossRef]
- Van Den Berg, F.; Pedersen, E.; Bouma, J.; Bakker, R. Visual and Acoustic Impact of Wind Turbine Farms on Residents. Final Report. 2008. Available online: https://research.rug.nl/en/publications/project-windfarmperception-visual-and-acoustic-impact-of-wind-tur (accessed on 26 August 2021).
- Thomson, H.; Kempton, W. Perceptions and attitudes of residents living near a wind turbine compared with those living near a coal power plant. Renew. Energy 2018, 123, 301–311. [Google Scholar] [CrossRef]
- Wen, C.; Dallimer, M.; Carver, S.; Ziv, G. Valuing the visual impact of wind farms: A calculus method for synthesizing choice experiments studies. Sci. Total Environ. 2018, 637–638, 58–68. [Google Scholar] [CrossRef]
- Williams, S.C.P. Sounds you can’t hear can still hurt your ears. Sci. Mag. 2014, 30. Available online: https://www.sciencemag.org/news/2014/09/sounds-you-cant-hear-can-still-hurt-your-ears (accessed on 26 August 2021).
- Jakobsen, J. Danish guidelines on environmental low frequency noise, infrasound and vibration. J. Low Freq. Noise Vib. Act. Control 2001, 20, 141–148. [Google Scholar] [CrossRef]
- German Standard DIN 45680. Messung und Beurteilung tieffrequenter Geräuschimmissionen (Measurement and Assessment of Low-Frequency Noise Immissions; in Germann); Deutsches Institut für Normung: Berlin, Germany, 1997. [Google Scholar]
- Maijala, P.; Turunen, A.; Kurki, I.; Vainio, L.; Pakarinen, S.; Kaukinen, C.; Lukander, K.; Tiittanen, P.; Yli-Tuomi, T.; Taimisto, P.; et al. Infrasound Does Not Explain Symptoms Related to Wind Turbines; Prime Minister’s Office: Helsinki, Finland, 2020.
- Krahé, D.; Alaimo Di Loro, A.; Müller, U.; Elmenhorst, E.; De Gioannis, R.; Schmitt, S.; Belke, C.; Benz, S.; Großarth, S.; Schreckenberg, D.; et al. Lärmwirkungen von Infraschallimmissionen (Noise Effects from Infrasound Immissions); Umweltbundesamt: Dessau-Roßlau, Germany, 2020.
- EARS Project Communiqué: Assessment and Safety of Non-Audible Sound. June 2015. Available online: https://www.ptb.de/emrp/ears-home.html (accessed on 26 August 2021).
- Koch, C. Hearing beyond the limit: Measurement, perception and impact of infrasound and ultrasonic noise. In Proceedings of the 12th ICBEN Congress on Noise as a Public Health Problem, Zürich, Switzerland, 18–22 June 2017. [Google Scholar]
- Behler, O.; Uppenkamp, S. Activation in human auditory cortex in relation to the loudness and unpleasantness of low-frequency and infrasound stimuli. PLoS ONE 2020, 15, e0229088. [Google Scholar]
- Burke, E.; Hensel, J.; Fedtke, T.; Uppenkamp, S.; Koch, C. Detection Thresholds for Combined Infrasound and Audio-Frequency Stimuli. Acta Acust. United Acust. 2019, 105, 1173–1182. [Google Scholar] [CrossRef]
- Weichenberger, M.; Bauer, M.; Kühler, R.; Hensel, J.; Forlim, C.G.; Ihlenfeld, A.; Ittermann, B.; Gallinat, J.; Koch, C.; Kühn, S. Altered cortical and subcortical connectivity due to infrasound administered near the hearing threshold- Evidence from fMRI. PLoS ONE 2017, 12, e0174420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weichenberger, M.; Kühler, R.; Bauer, M.; Hensel, J.; Brühl, R.; Ihlenfeld, A.; Kühn, S. Brief bursts of infrasound may improve cognitive function–An fMRI study. Hear. Res. 2015, 328, 87–93. [Google Scholar] [CrossRef]
- Jurado, C.; Marquardt, T. Brain’s Frequency Following Responses to Low-Frequency and Infrasound. Arch. Acoust. 2020, 45, 313–319. [Google Scholar]
- Marquardt, T.; Jurado, C. Amplitude Modulation May Be Confused with Infrasound. Acta Acust. United Acust. 2018, 104, 825–829. [Google Scholar] [CrossRef]
- Jurado, C.; Gordillo, D.; Moore, B.C.J. On the loudness of low-frequency sounds with fluctuating amplitudes. J. Acoust. Soc. Am. 2019, 146, 1142–1149. [Google Scholar] [CrossRef] [PubMed]
- Van Kamp, I.; Breugelmans, O.; Van Poll, R.; Baliatsas, C.; Van Kempen, E. Determinants of annoyance from humming sound as indicator of low frequency noise. In Proceedings of the ACOUSTICS 2017 Perth: Sound, Science and Society, Perth, Australia, 19–22 November 2017. [Google Scholar]
- Maijala, P.; Kurki, I.; Vainio, L.; Pakarinen, S.; Kuuramo, C.; Lukander, K.; Tiippana, K.; Virkkala, J.; Stickler, E.; Sainio, M. Annoyance, perception, and physiological effects of wind turbine infrasound. J. Acoust. Soc. Am. 2021, 149, 2238–2248. [Google Scholar] [CrossRef]
- Jurado, C.; Marquardt, T. On the Effectiveness of airborne infrasound in eliciting vestibular-evoked myogenic responses. J. Low Freq. Noise Vib. Act. Control 2020, 39, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, Y. Study on the relationship between unpleasantness and perception of vibration in the head of subjects exposed to low-frequency noise. In INTER-NOISE and NOISE-CON Congress and Conference Proceedings; Institute of Noise Control Engineering: Washington, DC, USA, 2017. [Google Scholar]
- Takahashi, Y. Vibratory sensation induced by low-frequency noise: The threshold for “vibration perceived in the head” in normal-hearing subjects. J. Low Freq. Noise Vib. Act. Control 2013, 32, 1–10. [Google Scholar] [CrossRef] [Green Version]
- WHO. Environmental Noise Guidelines for the European Region; WHO: Bonn, Germany, 2018. [Google Scholar]
- Van den Berg, F.; Van Kamp, I. Audibility and health effects of infra sound. In Proceedings of the 9th International Conference on Wind Turbine Noise, 18–21 May 2021. [Google Scholar]

| (a) | |||||||
| Author | Country | Design † | Study Population | Exposure Range (dB) in Lden | Ascertainment Hypertension * (prev/inc/mor) | ||
| N (%) ‡ | Gender # | Age Range (years) | |||||
| Michaud et al., 2018c [25] | Canada | CS | 1238 (79) | MF | 18–79 | <25, 25–30, 30–35, 35–40, 40–46 | 2 (prev) |
| Poulsen et al., 2018a [38] | Denmark | CO | 535,675 | MF | 25–85 | <24, 24–30, 30–36, 36–42, ≥42 | 3 (inc) |
| (b) | |||||||
| Author | Country | Design † | Study Population | Exposure Range (dB) in Lden | Ascertainment IHD * (prev/inc/mor) | ||
| N (%) ‡ | Gender # | Age Range (years) | |||||
| Bräuner et al., 2018a [40] | Denmark | CO | 23,994 | F | ≥44 | Unexposed, <21.5, 21.5–25.4, 25.4–29.9, >29.9 | 3 (inc) |
| Poulsen et al., 2019b [39] | Denmark | CO | 535,675 | MF | 25–85 | <24, 24–30, 30–36, 36–42, ≥42 | 3 (inc) |
| Author | Country | Design † | Study Population | Exposure Range (dB) in Lden | Ascertainment Diabetes ** (prev/inc/mor) | ||
|---|---|---|---|---|---|---|---|
| N (%) ‡ | Sex # | Age Range (years) | |||||
| Michaud et al., 2016b [46] | Canada | CS | 1238 (79) | MF | 18–79 | <25, 25–30, 30–35, 35–40, 40–46 | 1, 2 (prev) |
| Poulsen et al., 2018a [47] | Denmark | CO | 614,731 | MF | 25–85 | <24, 24–<30, 30–<36, 36–<42, ≥42 | 3 (inc) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Kamp, I.; van den Berg, F. Health Effects Related to Wind Turbine Sound: An Update. Int. J. Environ. Res. Public Health 2021, 18, 9133. https://doi.org/10.3390/ijerph18179133
van Kamp I, van den Berg F. Health Effects Related to Wind Turbine Sound: An Update. International Journal of Environmental Research and Public Health. 2021; 18(17):9133. https://doi.org/10.3390/ijerph18179133
Chicago/Turabian Stylevan Kamp, Irene, and Frits van den Berg. 2021. "Health Effects Related to Wind Turbine Sound: An Update" International Journal of Environmental Research and Public Health 18, no. 17: 9133. https://doi.org/10.3390/ijerph18179133
APA Stylevan Kamp, I., & van den Berg, F. (2021). Health Effects Related to Wind Turbine Sound: An Update. International Journal of Environmental Research and Public Health, 18(17), 9133. https://doi.org/10.3390/ijerph18179133