
Analysis the Link between Periodontal Diseases and Alzheimer’s Disease: A Systematic Review


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of Research Question
2.2. Goals
2.3. Elligibility Criteria
2.4. Information Sources and Search Strategy
2.5. Selection Process
2.6. Data Collection Process
2.7. Risk of Bias
3. Results
3.1. Characteristics of the Included Studies
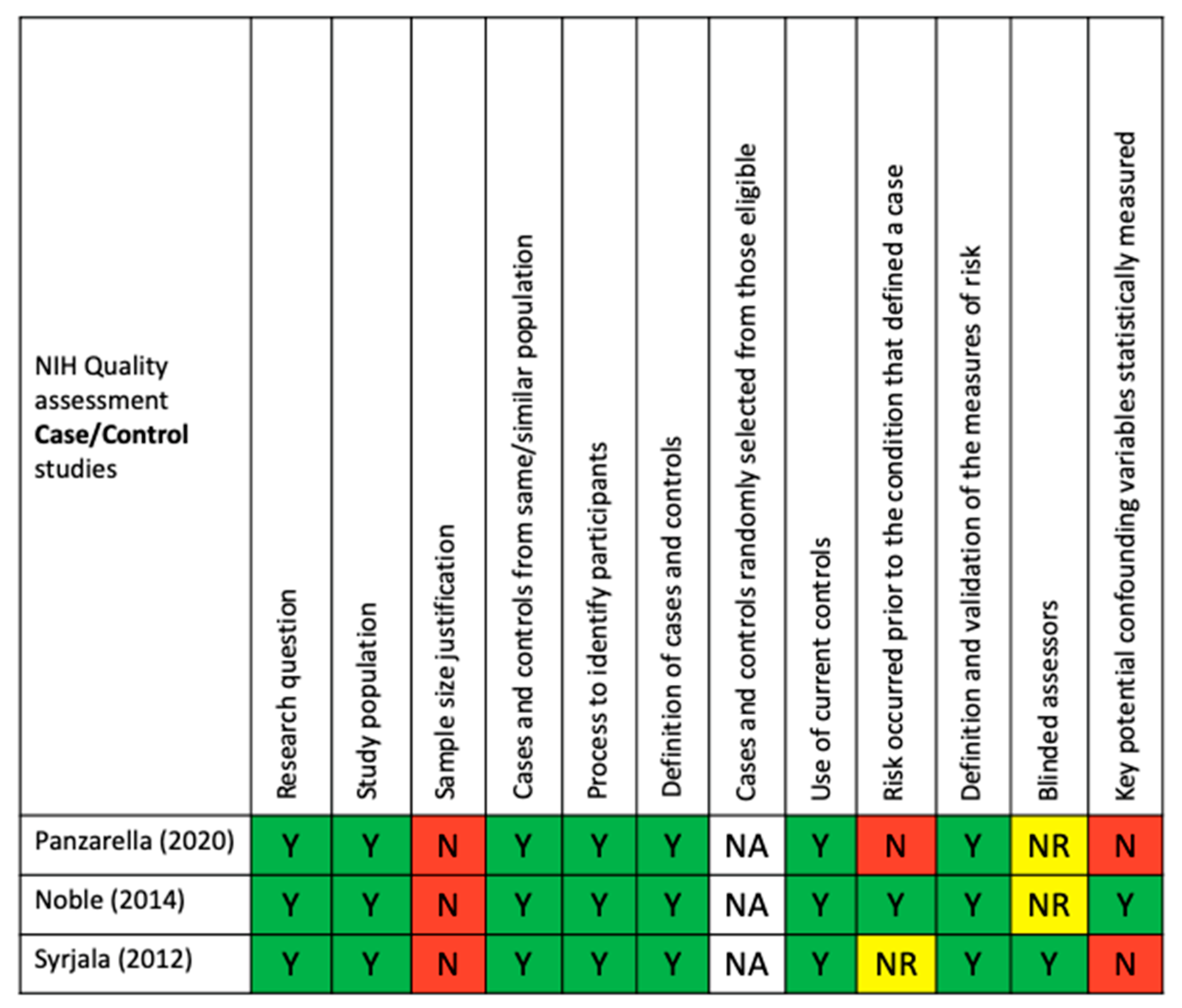
3.2. Bias and Quality of Included Studies
3.3. Association between AD and Periodontal Bacterial Pathogens
3.4. Association between Alzheimer’s Disease and Clinical Periodontal Markers
4. Discussion
4.1. Link between Alzheimer’s Disease and Periodontal Disease
4.2. Limitation of Selected Studies
4.3. Periodontal Bacteria: Towards a Better Understanding of the Link
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Masson, E. Le Microbiote Buccal: Bases Fondamentales et Applications en Physiopathologie. Available online: https://www.em-consulte.com/article/1340101/le-microbiote-buccal-bases-fondamentales-et-applic (accessed on 29 April 2021).
- Ezzo, P.J.; Cutler, C.W. Microorganisms as Risk Indicators for Periodontal Disease. Periodontol 2000 2003, 32, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Leask, A.; Holmes, A.; Black, C.M.; Abraham, D.J. Connective Tissue Growth Factor Gene Regulation. Requirements for Its Induction by Transforming Growth Factor-Beta 2 in Fibroblasts. J. Biol. Chem. 2003, 278, 13008–13015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizzo, G.; Guiglia, R.; Lo Russo, L.; Campisi, G. Dentistry and Internal Medicine: From the Focal Infection Theory to the Periodontal Medicine Concept. Eur. J. Intern. Med. 2010, 21, 496–502. [Google Scholar] [CrossRef]
- Kurgan, S.; Kantarci, A. Molecular Basis for Immunohistochemical and Inflammatory Changes during Progression of Gingivitis to Periodontitis. Periodontol 2000 2018, 76, 51–67. [Google Scholar] [CrossRef]
- Prince, M.; Wimo, A.; Guerchet, M.; Ali, G.-C.; Wu, Y.-T.; Matthew, P. World Alzheimer Report 2015, The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends. Alzheimer’s Dis. Int. 2015, 87, 84. [Google Scholar]
- World Health Organization. Global Burden of Disease 2004 Update: Disability Weights for Diseases and Conditions. Geneva: World Health Organization. Available online: https://www.google.com/search?client=firefox-b-d&q=World+Health+Organization.+Global+Burden+of+Disease+2004+Update%3A+Disability+Weights+for+Diseases+and+Conditions.+Geneva%3A+World+Health+Organization%3B+2004 (accessed on 30 April 2021).
- Kent, S.A.; Spires-Jones, T.L.; Durrant, C.S. The Physiological Roles of Tau and Aβ: Implications for Alzheimer’s Disease Pathology and Therapeutics. Acta Neuropathol. 2020, 140, 417–447. [Google Scholar] [CrossRef] [PubMed]
- Breijyeh, Z.; Karaman, R. Comprehensive Review on Alzheimer’s Disease: Causes and Treatment. Molecules 2020, 25, 5789. [Google Scholar] [CrossRef]
- Armstrong, R. Risk Factors for Alzheimer’s Disease. Folia Neuropathol. 2019, 57, 87–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itzhaki, R.F.; Lathe, R.; Balin, B.J.; Ball, M.J.; Bearer, E.L.; Braak, H.; Bullido, M.J.; Carter, C.; Clerici, M.; Cosby, S.L.; et al. Microbes and Alzheimer’s Disease. J. Alzheimer’s Dis. 2016, 51, 979–984. [Google Scholar] [CrossRef] [Green Version]
- Noble, J.M.; Borrell, L.N.; Papapanou, P.N.; Elkind, M.S.V.; Scarmeas, N.; Wright, C.B. Periodontitis Is Associated with Cognitive Impairment among Older Adults: Analysis of NHANES-III. J. Neurol. Neurosurg. Psychiatry 2009, 80, 1206–1211. [Google Scholar] [CrossRef] [Green Version]
- Iacono, D.; Markesbery, W.R.; Gross, M.; Pletnikova, O.; Rudow, G.; Zandi, P.; Troncoso, J.C. The Nun Study: Clinically Silent AD, Neuronal Hypertrophy, and Linguistic Skills in Early Life. Neurology 2009, 73, 665–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattila, K.J.; Pussinen, P.J.; Paju, S. Dental Infections and Cardiovascular Diseases: A Review. J. Periodontol. 2005, 76, 2085–2088. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.W.; Houcken, W.; Loos, B.G.; Schenkein, H.A.; Tezal, M. Periodontal Disease, Atherosclerosis, Adverse Pregnancy Outcomes, and Head-and-Neck Cancer. Adv. Dent. Res. 2014, 26, 47–55. [Google Scholar] [CrossRef]
- Ranjan, R.; Abhinay, A.; Mishra, M. Can Oral Microbial Infections Be a Risk Factor for Neurodegeneration? A Review of the Literature. Neurol. India 2018, 66, 344–351. [Google Scholar] [CrossRef]
- Ashraf, G.M.; Tarasov, V.V.; Makhmutova, A.; Chubarev, V.N.; Avila-Rodriguez, M.; Bachurin, S.O.; Aliev, G. The Possibility of an Infectious Etiology of Alzheimer Disease. Mol. Neurobiol. 2019, 56, 4479–4491. [Google Scholar] [CrossRef]
- Olsen, I.; Singhrao, S.K. Can Oral Infection Be a Risk Factor for Alzheimer’s Disease? J. Oral. Microbiol. 2015, 7, 29143. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, A.B.; Crean, S.; Olsen, I.; Singhrao, S.K. Periodontitis, Microbiomes and Their Role in Alzheimer’s Disease. Front. Aging Neurosci. 2017, 9, 336. [Google Scholar] [CrossRef] [Green Version]
- Miklossy, J.; McGeer, P.L. Common Mechanisms Involved in Alzheimer’s Disease and Type 2 Diabetes: A Key Role of Chronic Bacterial Infection and Inflammation. Aging 2016, 8, 575–588. [Google Scholar] [CrossRef] [Green Version]
- Miklossy, J. Historic Evidence to Support a Causal Relationship between Spirochetal Infections and Alzheimer’s Disease. Front. Aging Neurosci. 2015, 7, 46. [Google Scholar] [CrossRef] [Green Version]
- Sparks Stein, P.; Steffen, M.J.; Smith, C.; Jicha, G.; Ebersole, J.L.; Abner, E.; Dawson, D. Serum Antibodies to Periodontal Pathogens Are a Risk Factor for Alzheimer’s Disease. Alzheimer’s Dement. 2012, 8, 196–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominy, S.S.; Lynch, C.; Ermini, F.; Benedyk, M.; Marczyk, A.; Konradi, A.; Nguyen, M.; Haditsch, U.; Raha, D.; Griffin, C.; et al. Porphyromonas Gingivalis in Alzheimer’s Disease Brains: Evidence for Disease Causation and Treatment with Small-Molecule Inhibitors. Sci. Adv. 2019, 5, eaau3333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Study Quality Assessment Tools/NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 29 April 2021).
- Panzarella, V.; Mauceri, R.; Baschi, R.; Maniscalco, L.; Campisi, G.; Monastero, R. Oral Health Status in Subjects with Amnestic Mild Cognitive Impairment and Alzheimer’s Disease: Data from the Zabút Aging Project. J. Alzheimer’s Dis. 2020, 82, 1–11. [Google Scholar] [CrossRef]
- Noble, J.M.; Scarmeas, N.; Celenti, R.S.; Elkind, M.S.V.; Wright, C.B.; Schupf, N.; Papapanou, P.N. Serum IgG Antibody Levels to Periodontal Microbiota Are Associated with Incident Alzheimer Disease. PLoS ONE 2014, 9, e114959. [Google Scholar] [CrossRef] [Green Version]
- Syrjälä, A.-M.H.; Ylöstalo, P.; Ruoppi, P.; Komulainen, K.; Hartikainen, S.; Sulkava, R.; Knuuttila, M. Dementia and Oral Health among Subjects Aged 75 Years or Older. Gerodontology 2012, 29, 36–42. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Beydoun, H.A.; Hossain, S.; El-Hajj, Z.W.; Weiss, J.; Zonderman, A.B. Clinical and Bacterial Markers of Periodontitis and Their Association with Incident All-Cause and Alzheimer’s Disease Dementia in a Large National Survey. J. Alzheimer’s Dis. 2020, 75, 157–172. [Google Scholar] [CrossRef]
- Ide, M.; Harris, M.; Stevens, A.; Sussams, R.; Hopkins, V.; Culliford, D.; Fuller, J.; Ibbett, P.; Raybould, R.; Thomas, R.; et al. Periodontitis and Cognitive Decline in Alzheimer’s Disease. PLoS ONE 2016, 11, e0151081. [Google Scholar] [CrossRef] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A New Classification Scheme for Periodontal and Peri-Implant Diseases and Conditions-Introduction and Key Changes from the 1999 Classification. J. Periodontol. 2018, 89 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D. Periodontal Microbial Ecology. Periodontol 2000 2005, 38, 135–187. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L. Microbial Complexes in Subgingival Plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Nuckols, C.C.; Nuckols, C.C. Diagnostic and Statistical Manual of Mental Disorders: DSM-V, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Molloy, D.W.; Standish, T.I. A Guide to the Standardized Mini-Mental State Examination. Int. Psychogeriatr. 1997, 9 (Suppl. 1), 87–94, discussion 143–150. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.C. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Segal, D.L. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Rosen, W.G.; Mohs, R.C.; Davis, K.L. A New Rating Scale for Alzheimer’s Disease. Am. J. Psychiatry 1984, 141, 1356–1364. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The Diagnosis of Dementia Due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- ICD-ICD-9-CM-International Classification of Diseases, Ninth Revision, Clinical Modification. Available online: https://www.cdc.gov/nchs/icd/icd9cm.htm (accessed on 30 April 2021).
- Underlying Cause of Death 1999-2019. Available online: https://wonder.cdc.gov/wonder/help/ucd.html (accessed on 1 May 2021).
- Lane, C.A.; Hardy, J.; Schott, J.M. Alzheimer’s Disease. Eur. J. Neurol. 2018, 25, 59–70. [Google Scholar] [CrossRef]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a Biological Definition of Alzheimer’s Disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Chen, C.-K.; Wu, Y.-T.; Chang, Y.-C. Association between Chronic Periodontitis and the Risk of Alzheimer’s Disease: A Retrospective, Population-Based, Matched-Cohort Study. Alzheimer’s Res. Ther. 2017, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Martande, S.S.; Pradeep, A.R.; Singh, S.P.; Kumari, M.; Suke, D.K.; Raju, A.P.; Naik, S.B.; Singh, P.; Guruprasad, C.N.; Chatterji, A. Periodontal Health Condition in Patients with Alzheimer’s Disease. Am. J. Alzheimer’s Dis. Other. Demen. 2014, 29, 498–502. [Google Scholar] [CrossRef]
- Gil-Montoya, J.A.; Sanchez-Lara, I.; Carnero-Pardo, C.; Fornieles, F.; Montes, J.; Vilchez, R.; Burgos, J.S.; Gonzalez-Moles, M.A.; Barrios, R.; Bravo, M. Is Periodontitis a Risk Factor for Cognitive Impairment and Dementia? A Case-Control Study. J. Periodontol. 2015, 86, 244–253. [Google Scholar] [CrossRef]
- Holmer, J.; Eriksdotter, M.; Schultzberg, M.; Pussinen, P.J.; Buhlin, K. Association between Periodontitis and Risk of Alzheimer’s Disease, Mild Cognitive Impairment and Subjective Cognitive Decline: A Case-Control Study. J. Clin. Periodontol. 2018, 45, 1287–1298. [Google Scholar] [CrossRef]
- Leblhuber, F.; Huemer, J.; Steiner, K.; Gostner, J.M.; Fuchs, D. Knock-on Effect of Periodontitis to the Pathogenesis of Alzheimer’s Disease? Wien. Klin. Wochenschr. 2020, 132, 493–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.; Kim, K.; Chang, J.; Kim, S.M.; Kim, S.J.; Cho, H.-J.; Park, S.M. Association of Chronic Periodontitis on Alzheimer’s Disease or Vascular Dementia. J. Am. Geriatr. Soc. 2019, 67, 1234–1239. [Google Scholar] [CrossRef] [Green Version]
- Ship, J.A.; Puckett, S.A. Longitudinal Study on Oral Health in Subjects with Alzheimer’s Disease. J. Am. Geriatr. Soc. 1994, 42, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.-Q.; Richmond, R.C.; Chen, Y.; Mai, X.-M. Mixed Evidence for the Relationship between Periodontitis and Alzheimer’s Disease: A Bidirectional Mendelian Randomization Study. PLoS ONE 2020, 15, e0228206. [Google Scholar] [CrossRef] [PubMed]
- Poole, S.; Singhrao, S.K.; Kesavalu, L.; Curtis, M.A.; Crean, S. Determining the Presence of Periodontopathic Virulence Factors in Short-Term Postmortem Alzheimer’s Disease Brain Tissue. J. Alzheimer’s Dis. 2013; 36, 665–677. [Google Scholar] [CrossRef]
- Carter, C.J. Genetic, Transcriptome, Proteomic, and Epidemiological Evidence for Blood-Brain Barrier Disruption and Polymicrobial Brain Invasion as Determinant Factors in Alzheimer’s Disease. J. Alzheimer’s Dis. Rep. 2017, 1, 125–157. [Google Scholar] [CrossRef]
- Carter, C.J.; France, J.; Crean, S.; Singhrao, S.K. The Porphyromonas Gingivalis/Host Interactome Shows Enrichment in GWASdb Genes Related to Alzheimer’s Disease, Diabetes and Cardiovascular Diseases. Front. Aging Neurosci. 2017, 9, 408. [Google Scholar] [CrossRef] [Green Version]
- Kamer, A.R.; Craig, R.G.; Pirraglia, E.; Dasanayake, A.P.; Norman, R.G.; Boylan, R.J.; Nehorayoff, A.; Glodzik, L.; Brys, M.; de Leon, M.J. TNF-Alpha and Antibodies to Periodontal Bacteria Discriminate between Alzheimer’s Disease Patients and Normal Subjects. J. Neuroimmunol. 2009, 216, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Beydoun, M.A.; Beydoun, H.A.; Weiss, J.; Hossain, S.; El-Hajj, Z.W.; Zonderman, A.B. Helicobacter Pylori, Periodontal Pathogens, and Their Interactive Association with Incident All-Cause and Alzheimer’s Disease Dementia in a Large National Survey. Mol. Psychiatry 2020, 1–16. [Google Scholar] [CrossRef]
- Singhrao, S.K.; Harding, A. Is Alzheimer’s Disease a Polymicrobial Host Microbiome Dysbiosis? Expert Rev. Anti. Infect. Ther. 2020, 18, 275–277. [Google Scholar] [CrossRef]
- Singhrao, S.K.; Olsen, I. Are Porphyromonas Gingivalis Outer Membrane Vesicles Microbullets for Sporadic Alzheimer’s Disease Manifestation? J. Alzheimer’s Dis. Rep. 2018, 2, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Theilade, E.; Wright, W.H.; Jensen, S.B.; Löe, H. Experimental Gingivitis in Man. II. A Longitudinal Clinical and Bacteriological Investigation. J. Periodontal. Res. 1966, 1, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ritz, H.L. Microbial Population Shifts in Developing Human Dental Plaque. Arch. Oral. Biol. 1967, 12, 1561–1568. [Google Scholar] [CrossRef]
- Marsh, P.D.; Bradshaw, D.J. Dental Plaque as a Biofilm. J. Ind. Microbiol. 1995, 15, 169–175. [Google Scholar] [CrossRef]
- Dioguardi, M.; Crincoli, V.; Laino, L.; Alovisi, M.; Sovereto, D.; Mastrangelo, F.; Russo, L.L.; Muzio, L.L. The Role of Periodontitis and Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease: A Systematic Review. J. Clin. Med. 2020, 9, 495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leira, Y.; Seoane, J.; Blanco, M.; Rodríguez-Yáñez, M.; Takkouche, B.; Blanco, J.; Castillo, J. Association between Periodontitis and Ischemic Stroke: A Systematic Review and Meta-Analysis. Eur. J. Epidemiol. 2017, 32, 43–53. [Google Scholar] [CrossRef]
- De Souza Rolim, T.; Fabri, G.M.C.; Nitrini, R.; Anghinah, R.; Teixeira, M.J.; de Siqueira, J.T.T.; Cestari, J.A.F.; de Siqueira, S.R.D.T. Oral Infections and Orofacial Pain in Alzheimer’s Disease: A Case-Control Study. J. Alzheimer’s Dis. 2014, 38, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Laugisch, O.; Johnen, A.; Maldonado, A.; Ehmke, B.; Bürgin, W.; Olsen, I.; Potempa, J.; Sculean, A.; Duning, T.; Eick, S. Periodontal Pathogens and Associated Intrathecal Antibodies in Early Stages of Alzheimer’s Disease. J Alzheimers Dis. 2018, 66, 105–114. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borsa, L.; Dubois, M.; Sacco, G.; Lupi, L. Analysis the Link between Periodontal Diseases and Alzheimer’s Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 9312. https://doi.org/10.3390/ijerph18179312
Borsa L, Dubois M, Sacco G, Lupi L. Analysis the Link between Periodontal Diseases and Alzheimer’s Disease: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(17):9312. https://doi.org/10.3390/ijerph18179312
Chicago/Turabian StyleBorsa, Leslie, Margaux Dubois, Guillaume Sacco, and Laurence Lupi. 2021. "Analysis the Link between Periodontal Diseases and Alzheimer’s Disease: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 17: 9312. https://doi.org/10.3390/ijerph18179312
APA StyleBorsa, L., Dubois, M., Sacco, G., & Lupi, L. (2021). Analysis the Link between Periodontal Diseases and Alzheimer’s Disease: A Systematic Review. International Journal of Environmental Research and Public Health, 18(17), 9312. https://doi.org/10.3390/ijerph18179312