
Influence of Work on Andropause and Menopause: A Systematic Review


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion Criteria
2.3. Exclusion Criteria
- Animal studies.
- Articles not in English.
- Reviews/conference abstracts or letters to the editor.
- Studies published before 2000 were excluded due to the vast changes—in terms of technology, tools, organization and methods and working environment—that have affected work over the past 20 years.
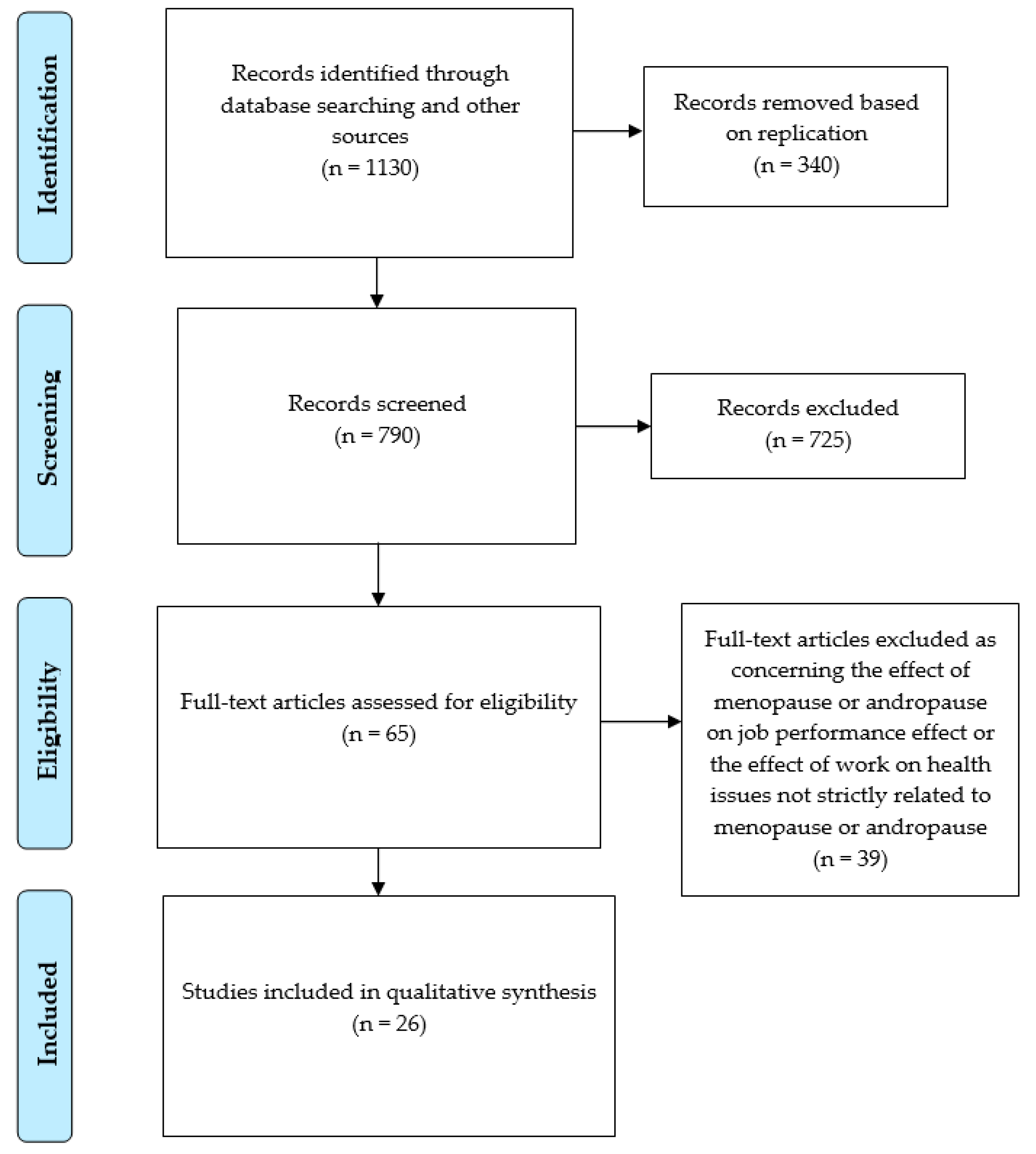
2.4. Studies Selection
3. Results
3.1. Aging and Gonadal Status in Male Workers
3.2. Aging and Gonadal Status in Female Workers
3.2.1. Influence of Work on Menopause Onset
3.2.2. Influence of Work on Menopausal Symptoms
3.2.3. Quality of the Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- van den Beld, A.W.; Kaufman, J.M.; Zillikens, M.C.; Lamberts, S.W.J.; Egan, J.M.; van der Lely, A.J. The physiology of endocrine systems with ageing. Lancet Diabetes Endocrinol. 2018, 6, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Gracia, C.R.; Freeman, E.W. Onset of the Menopause Transition: The Earliest Signs and Symptoms. Obstet. Gynecol. Clin. N. Am. 2018, 45, 585–597. [Google Scholar] [CrossRef]
- Salonia, A.; Rastrelli, G.; Hackett, G.; Seminara, S.B.; Huhtaniemi, I.T.; Rey, R.A.; Hellstrom, W.J.G.; Palmert, M.R.; Corona, G.; Dohle, G.R.; et al. Paediatric and adult-onset male hypogonadism. Nat. Rev. Dis. Prim. 2019, 5, 1–21. [Google Scholar] [CrossRef]
- T’Sjoen, G.; Goemaere, S.; De Meyere, M.; Kaufman, J.M. Perception of males’ aging symptoms, health and well-being in elderly community-dwelling men is not related to circulating androgen levels. Psychoneuroendocrinology 2004, 29, 201–214. [Google Scholar] [CrossRef]
- Bariola, E.; Jack, G.; Pitts, M.; Riach, K.; Sarrel, P. Employment conditions and work-related stressors are associated with menopausal symptom reporting among perimenopausal and postmenopausal women. Menopause 2017, 24, 247–251. [Google Scholar] [CrossRef]
- El Khoudary, S.R.; Thurston, R.C. Cardiovascular Implications of the Menopause Transition: Endogenous Sex Hormones and Vasomotor Symptoms. Obstet. Gynecol. Clin. N. Am. 2018, 45, 641–661. [Google Scholar] [CrossRef]
- Pye, S.R.; Huhtaniemi, I.T.; Finn, J.D.; Lee, D.M.; O’Neill, T.W.; Tajar, A.; Bartfai, G.; Boonen, S.; Casanueva, F.F.; Forti, G.; et al. Late-onset hypogonadism and mortality in aging men. J. Clin. Endocrinol. Metab. 2014, 99, 1357–1366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bupp, M.R.G.; Potluri, T.; Fink, A.L.; Klein, S.L. The confluence of sex hormones and aging on immunity. Front. Immunol. 2018, 9, 1269. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Kratzik, C.W.; Reiter, W.J.; Riedl, A.M.; Lunglmayrt, G.; Brandstätter, N.; Rücklinger, E.; Metka, M.; Huber, J. Hormone profiles, body mass index and aging male symptoms: Results of the Androx Vienna Municipality study. Aging Male 2004, 7, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Fukai, S.; Akishita, M.; Miyao, M.; Ishida, K.; Toba, K.; Ouchi, Y. Age-related changes in plasma androgen levels and their association with cardiovascular risk factors in male Japanese office workers. Geriatr. Gerontol. Int. 2010, 10, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Hirokawa, K.; Taniguchi, T.; Fujii, Y.; Takaki, J.; Tsutsumi, A. Job demands as a potential modifier of the association between testosterone deficiency and andropause symptoms in Japanese middle-aged workers: A cross-sectional study. Maturitas 2012, 73, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Bann, D.; Hardy, R.; Cooper, R.; Lashen, H.; Keevil, B.; Wu, F.C.W.; Holly, J.M.P.; Ong, K.K.; Ben-Shlomo, Y.; Kuh, D. Socioeconomic conditions across life related to multiple measures of the endocrine system in older adults: Longitudinal findings from a British birth cohort study. Soc. Sci. Med. 2015, 147, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Hirokawa, K.; Taniguchi, T.; Fujii, Y.; Takaki, J.; Tsutsumi, A. Modification Effects of Changes in Job Demands on Associations Between Changes in Testosterone Levels and Andropause Symptoms: 2-Year Follow-up Study in Male Middle-Aged Japanese Workers. Int. J. Behav. Med. 2016, 23, 464–472. [Google Scholar] [CrossRef]
- Łopuszańska-Dawid, M.; Szklarska, A.; Kołodziej, H.; Lipowicz, A.; Jankowska, E.A. The relationship between: Occupational status, biological condition and androgen hormone level among Polish adult men: The Wroclaw Male Study. Aging Male 2016, 19, 231–238. [Google Scholar] [CrossRef]
- Pastuszak, A.W.; Moon, Y.M.; Scovell, J.; Badal, J.; Lamb, D.J.; Link, R.E.; Lipshultz, L.I. Poor Sleep Quality Predicts Hypogonadal Symptoms and Sexual Dysfunction in Male Nonstandard Shift Workers. Urology 2017, 102, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Samipoor, F.; Pakseresht, S.; Rezasoltani, P.; Mehrdad, M. The association between hypogonadism symptoms with serum testosterone, FSH and LH in men. Aging Male 2018, 21, 1–8. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Kohn, T.P.; Santiago, J.E.; Sigalos, J.T.; Kirby, E.W.; Hockenberry, M.S.; Pickett, S.M.; Pastuszak, A.W.; Lipshultz, L.I. Increased Risk of Hypogonadal Symptoms in Shift Workers With Shift Work Sleep Disorder. Urology 2020, 138, 52–59. [Google Scholar] [CrossRef]
- Zhao, G.; Wang, L.; Yan, R.; Dennerstein, L. Menopausal symptoms: Experience chinese women. Climacteric 2000, 3, 135–144. [Google Scholar] [CrossRef]
- Farr, S.L.; Cai, J.; Savitz, D.A.; Sandler, D.P.; Hoppin, J.A.; Cooper, G.S. Pesticide exposure and timing of menopause: The agricultural health study. Am. J. Epidemiol. 2006, 163, 731–742. [Google Scholar] [CrossRef] [Green Version]
- Cassou, B.; Mandereau, L.; Aegerter, P.; Touranchet, A.; Derriennic, F. Work-related factors associated with age at natural menopause in a generation of French gainfully employed women. Am. J. Epidemiol. 2007, 166, 429–438. [Google Scholar] [CrossRef]
- Kaczmarek, M. The timing of natural menopause in Poland and associated factors. Maturitas 2007, 57, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Fleming, L.E.; Levis, S.; Leblanc, W.G.; Dietz, N.A.; Arheart, K.L.; Wilkinson, J.D.; Clark, J.; Serdar, B.; Davila, E.P.; Lee, D.J. Earlier age at menopause, work, and tobacco smoke exposure. Menopause 2008, 15, 1103–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Wang, M.; Cheng, N.; Zheng, T.; Hu, X.; Li, H.; Chan, C.; Zhang, Y.; Ren, X.; Bai, Y. Sulfur dioxide exposure and other factors affecting age at natural menopause in the Jinchuan cohort. Climacteric 2015, 18, 722–732. [Google Scholar] [CrossRef]
- Stock, D.; Knight, J.A.; Raboud, J.; Cotterchio, M.; Strohmaier, S.; Willett, W.; Eliassen, A.H.; Rosner, B.; Hankinson, S.E.; Schernhammer, E. Rotating night shift work and menopausal age. Hum. Reprod. 2019, 34, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Samtani, R.; Garg, D.; Sharma, N.; Deb, R. Sociodemographic pattern of postmenopausal women and health issues: A study in rural Bathinda, Punjab. J. Midlife. Health 2020, 11, 168–170. [Google Scholar] [CrossRef]
- Olaolorun, F.M.; Lawoyin, T.O. Experience of menopausal symptoms by women in an urban community in Ibadan, Nigeria. Menopause 2009, 16, 822–830. [Google Scholar] [CrossRef]
- Sovani, P.; Mukundan, G. Comparison of postmenopausal voice changes across professional and non-professional users of the voice. S. Afr. J. Commun. Disord. 2010, 57, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.S.; Kim, J.H.; Park, M.S.; Yang, J.; Ko, Y.H.; Ko, S.D.; Joe, S.H. Factors influencing the severity of menopause symptoms in Korean post-menopausal women. J. Korean Med. Sci. 2010, 25, 758–765. [Google Scholar] [CrossRef] [Green Version]
- Oğurlu, N.; Küçük, M.; Aksu, H. Influence of employment status on menopausal symptoms. Int. J. Gynecol. Obstet. 2011, 112, 204–207. [Google Scholar] [CrossRef]
- Hammam, R.A.M.; Abbas, R.A.; Hunter, M.S. Menopause and work—The experience of middle-aged female teaching staff in an Egyptian governmental faculty of medicine. Maturitas 2012, 71, 294–300. [Google Scholar] [CrossRef]
- Matsuzaki, K.; Uemura, H.; Yasui, T. Associations of menopausal symptoms with job-related stress factors in nurses in Japan. Maturitas 2014, 79, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Huseth-Zosel, A.; Strand, M.; Perry, J. Socioeconomic differences in the menopausal experience of chinese women. Post Reprod. Health 2014, 20, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, D.; Murray, J.; Farrington, D.; Vannick, C. Testing the Cambridge quality checklists on a review of disrupted families and crime. Crim. Behav. Ment. Health 2012, 22, 303–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| 1—“aging” AND “workers” AND “hormones” |
| 2—aging” AND “workers” AND “testosterone” |
| 3—“aging” AND “workers” AND “andropause” |
| 4—“aging” AND “workers” AND “menopause” |
| 5—“aging” AND “occupational” AND “hormones” |
| 6—“aging” AND “occupational” AND “testosterone” |
| 7—“aging” AND “occupational” AND “andropause” |
| 8—“aging” AND “occupational” AND “menopause” |
| 9—“aging” AND “job” AND “hormones” |
| 10—“aging” AND “job” AND “testosterone” |
| 11—“aging” AND “job” AND “andropause” |
| 12—“aging” AND “job” AND “menopause” |
| 13—“andropause” AND “occupational” AND “workers” |
| 14—“menopause” AND “occupational” AND “workers” |
| 15—“workplace” AND “aging” AND “hormones” |
| 16—“workplace” AND “aging” AND “testosterone” |
| 17—“workplace” AND “aging” AND “andropause” |
| 18—“workplace” AND “aging” AND “menopause” |
| 19—“occupational health” AND “aging” AND “hormones” |
| 20—“occupational health” AND “aging” AND “testosterone” |
| 21—“occupational health” AND “aging” AND “andropause” |
| 22—“occupational health” AND “aging” AND “menopause” |
| 23—“andropause” AND “job” |
| 24—“menopause” AND “job” |
| Reference | Study Design | Worker Type | No. of Subjects | Age | Country | Hormones Evaluated | Aim of the Study | Outcome Measures | Additional Tools | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Kratzik et al., 2004 [10] | Cross-sectional | Blue-collar workers | 664 | 40–60 | Austria | LH, T, E2, PRL, SHBG, BAT | To explore the relationship between hormonal status and the AMS score, taking into consideration the influence of BMI and age on hormonal status | AMS | BMI | Low T or BAT levels involved a significantly increased risk of psychological symptoms of andropause. Low T and BAT, together with aging, increased the risk of somatovegetative symptoms, whereas aging increased the risk of sexual symptoms. |
| Fukai et al., 2010 [11] | Cross-sectional * and longitudinal ** (FU 5 years) | Office workers | 139 (96 and 76 *, 33 **) | 52.7 ± 5.9 and 51.5 ± 6.8 * 54.3 ± 5.4 ** | Japan | TT, FT DHEAS, | To assess age-related changes in plasma androgen levels in healthy middle-aged men and elucidate whether any clinical parameters measured in health check-ups were associated with hormonal changes | Blood pressure, BMI, waist circumference, lipid panel | Age was negatively associated with FT and DHES, but not with TT. In the longitudinal survey, the 5-year changes in androgen levels were not significant. | |
| Hirokawa et al., 2012 [12] | Cross-sectional | Employees of a medium-sized company | 183 | 51.9 ± 7.7 (34–67) | Japan | TT | To establish whether job demands modify the association between low T levels and andropause symptoms | Japanese version of JCQ, AMS, hormonal parameters | Information on history of lifestyle diseases, smoking status, alcohol consumption and sleeping hours | Low TT levels were associated with more psychological andropause symptoms. High job demands, age, and TT levels were positively associated with the total score of andropause symptoms and with somatic and psychological symptom scores. |
| Bann et al., 2015 [13] | Longitudinal (FU 60–64 years) | Professional, intermediate, skilled (non-manual), skilled (manual), partly skilled, unskilled | 875 | 60–64 | U.K. | IGF-1, IGF-2, IGFBP-3, TT, SHBG, cFT, evening salivary cortisol | To test the hypothesis that lower SEP across life could be associated with an adverse hormone profile across multiple axes | SEP indicators across life: paternal occupation at 4 yo, highest educational level at 26 yo, highest occupational class at 53 yo, self-reported household income at 60–64 yo | At 60–64 years, lower education and lower income were associated with lower T levels, lower education was associated with lower IGF-1, and a lower lifetime SEP score was associated with higher evening cortisol. The socioeconomic patterning of endocrine function determinants may become more pronounced in older men. | |
| Hirokawa et al., 2016 [14] | Longitudinal (FU 2 years) | Employees of a medium-sized company | 104 | 52.8 ± 7.2 (36–62) | Japan | TT | To establish whether changes in job demands modify associations between changes in T levels and andropause symptoms | Japanese version of JCQ, AMS, hormonal parameters | Information on past history of lifestyle diseases, smoking status, alcohol consumption and sleep hours | Changes in T levels correlated negatively with changes in psychological symptoms, sexual symptoms, and total AMS score, whereas changes in job demands positively correlated only with somatic changes. The interaction of changes in job demands and T levels was associated with changes in psychological symptoms. |
| Łopuszańska-Dawid et al., 2016 [15] | Cross-sectional | Professionals, soldiers, and skilled workers | 300 | 30–65 | Poland | IGF-1, TT, cFT, SHBG, E2, DHEAS | To investigate the relationship between occupational activity and biological condition in adult men | 11 measures of general biological condition, 6 hormonal parameters | Data on socioeconomic status, lifestyle, type of work, general life satisfaction (low, medium, high), and approach to life (optimist, pessimist, mixed) | Relative biological age with reference to the general and hormonal parameters was lowest in professionals and highest in skilled workers. Professionals had the highest IFG-1, cFT, and DHEAS values, whereas skilled workers had the lowest TT, E2, and DHEAS values |
| Pastuszak et al., 2017 [16] | Cross-sectional | Shift workers | 676 (182 non-standard shift workers ° and 494 standard shift workers °°) | 41.4 ± 10.8 ° 46.4 ± 14.7 °° | U.S.A. | TT, FT, E2, DHEA, FSH, LH | To evaluate the impact of sleep quality on hypogonadism symptoms and sexual function in standard and non-standard male shift workers | ADAM, qADAM, IIEF, self-reported satisfaction with sleep quality | In non-standard shift workers, better sleep quality was associated with fewer hypogonadism symptoms and a better sexual function. Sleep quality did not affect hormone levels, which were comparable in standard and non-standard shift workers. | |
| Samipoor et al., 2018 [17] | Cross-sectional | Self-employed subjects, employees, and workers | 140 | 52.1 ± 7.1 | Iran | TT, FT, FSH, LH | To clarify the association between hypogonadism symptoms and sex hormone levels, according to anthropometric and socioeconomic parameters (including occupation) | AMS | Information on history of lifestyle diseases, smoking status, alcohol consumption and blood pressure | No significant association between T levels and andropause symptoms. Significant association between occupation and hypogonadism symptoms, with the highest score in self-employed subjects |
| Balasubramanian et al., 2020 [18] | Cross-sectional | Shift workers versus daytime workers | 2571 | 42.9 (weighted average) | U.S.A. | TT, FSH, LH | To examine the association among shift work, sleep disorders and hypogonadism symptoms in shift workers | qADAM, ADAM | RAPA, CCI, PHQ-9 | Non-standard shift workers showed worse hypogonadism symptoms than daytime workers; the further presence of sleep disorders was associated with even worse hypogonadism symptoms and lower T levels. Age was a significant independent predictor of T level in shift workers with or without sleep disorders. |
| Reference | Study Design | Worker Type | No. of Subjects | Country | Exposure | Results |
|---|---|---|---|---|---|---|
| Zhao et al., 2000 [19] | Cross-sectional | Professionals and farmers | 806 | China | Rural environment | Professional city women experienced a later age at menopause than women farmers living in rural areas. |
| Farr et al., 2006 [20] | Longitudinal prospective | Farm workers | 8038 | U.S.A. | Pesticides | The median time to menopause increased by 3 months for any pesticide exposure and by 5 months for hormonally active pesticides. |
| Cassou et al., 2007 [21] | Longitudinal prospective | Gainfully employed women | 1594 | France | Occupational factors | Occupational factors, such as job control or high-strain jobs and difficult schedules, were associated with earlier age at menopause in women with and without a history of depression, respectively. Smoking increased the risk of earlier menopause. |
| Kaczmarek et al., 2007 [22] | Cross-sectional | Not specified | 7183 | Poland | Occupation | Occupational status is not a risk factor for earlier age at menopause. |
| Fleming et al., 2008 [23] | Cross-sectional | White collar, service, farm workers, blue collar | 5029 | U.S.A. | Smoking | Primary tobacco use and secondhand smoke were associated with earlier menopause. Service and manufacturing industry workers had a greater potential secondhand smoke exposure and showed earlier age at menopause (not significant). |
| Wang et al., 2015 [24] | Retrospective cohort | White collar, blue collar | 3167 | China | Sulfur dioxide | Blue-collar workers experienced earlier menopause than white-collar workers. Exposure to sulfur dioxide (especially for 21 to 25 years) was associated with earlier age at menopause. |
| Stock et al., 2019 [25] | Longitudinal prospective | Rotating night shift nurses | 80,840 | U.S.A. | Night shifts | Rotating night shift work was associated with an increased risk of earlier menopause, especially among women aged < 45 years. |
| Samtani et al., 2020 [26] | Cross-sectional | Agriculture, other | 425 | India | Pesticides | Pesticide exposure was associated with older age at menopause (not significant). |
| Reference | Study Design | Worker Type | No. of Subjects | Country | Symptoms | Results |
|---|---|---|---|---|---|---|
| Zhao et al., 2000 [19] | Cross-sectional | Professional workers and farmers | 806 | China | Vasomotor and psychological symptoms, bone/joint pain | In the peri- and postmenopausal period, professional city women showed a higher prevalence of menopausal symptoms than women farmers living in rural areas. |
| Olaolorun et al., 2009 [27] | Cross-sectional | Managerial and professional, intermediate, or routine and material workers | 1189 | Nigeria | Joint and muscular discomfort, physical and mental exhaustion, sexual problems, hot flashes | Occupation significantly correlated with menopausal symptoms, especially with psychological symptoms. |
| Sovani et al., 2010 [28] | Cross-sectional | Professional (teachers) and non-professional (clerks) voice users | 92 | India | Voice changes | All women exhibited menopausal voice changes, but professional voice users presented a higher severity and rate of changes. |
| Lee et al., 2010 [29] | Cross-sectional | Non-employed, employed | 657 | Korea | Menopause Rating Scale | Employed women with jobs had less severe menopausal symptoms than non-employed women |
| Oǧurlu et al., 2011 [30] | Cross-sectional | Non-employed, employed | 132 | Turkey | Climateric Complaint Tool (15 symptoms) | Non-working women were more likely to report hot flashes, sleeping difficulties, headache, irritability, depressive mood, muscle and joint pain, and urinary complaints than working women. Working status was an independent predictor of the severity of climacteric symptoms on multivariate logistic regression analysis. |
| Hammam et al., 2012 [31] | Cross-sectional | Medical teaching staff | 131 | Egypt | Depressed mood, vasomotor symptoms, anxiety, sexual and sleep problems | Several workplace factors (poor physical environment, confined spaces/crowding, insufficient sanitary/rest/refreshment facilities, and poor workstation design) worsened menopausal symptoms. |
| Matsuzaki et al., 2014 [32] | Cross-sectional | Nurses | 1169 | Japan | Green’s Climateric Scale (21 symptoms) | High levels of job-related stress significantly correlated with menopausal symptoms in all nurses, although stressors were different for those with and without managerial positions. |
| Huseth-Zosel et al., 2014 [33] | Cross-sectional | Non-employed, white-collar and blue-collar workers | 296 | China | Hot flashes, dry skin/eyes, sleeplessness, heart palpitations, musculoskeletal pain, neurological symptoms, emotional distress | Employment, particularly a white-collar job, exerted some protective effect on certain menopausal symptoms. |
| Bariola et al., 2017 [5] | Cross-sectional | Higher education workers | 476 | Australia | Menopause Symptom Index (19 symptoms) | Lower menopausal symptom reporting was associated with workplace conditions such as greater supervisor support, working full, and control over temperature. |
| Work and Andropause (n = 9) | Work and Age at Menopause (n = 8) | Work and Menopausal Symptoms (n = 9) | |
|---|---|---|---|
| Correlate score | |||
| 0 | 0 | 0 | 0 |
| 1 | 3 | 0 | 1 |
| 2 | 3 | 0 | 3 |
| 3 | 3 | 8 | 5 |
| 4 | 0 | 0 | 0 |
| 5 | 0 | 0 | 0 |
| Risk factor score | |||
| 1. Cross-sectional data | 6 | 4 | 9 |
| 2. Retrospective data | 0 | 1 | 0 |
| 3. Prospective data | 3 | 3 | 0 |
| Causal risk factor score | |||
| 1. Study without a comparison group No analysis of change 2. Inadequately controlled study No analysis of change 3. Study without a comparison group With analysis of change 4. Inadequately controlled study With analysis of change 5. Controlled non-experimental study No analysis of change 6. Controlled non-experimental study With analysis of change 7. Randomized experiment Targeting a risk factor | 6 0 3 0 0 0 0 | 8 0 0 0 0 0 0 | 9 0 0 0 0 0 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martelli, M.; Zingaretti, L.; Salvio, G.; Bracci, M.; Santarelli, L. Influence of Work on Andropause and Menopause: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 10074. https://doi.org/10.3390/ijerph181910074
Martelli M, Zingaretti L, Salvio G, Bracci M, Santarelli L. Influence of Work on Andropause and Menopause: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(19):10074. https://doi.org/10.3390/ijerph181910074
Chicago/Turabian StyleMartelli, Margherita, Laura Zingaretti, Gianmaria Salvio, Massimo Bracci, and Lory Santarelli. 2021. "Influence of Work on Andropause and Menopause: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 19: 10074. https://doi.org/10.3390/ijerph181910074
APA StyleMartelli, M., Zingaretti, L., Salvio, G., Bracci, M., & Santarelli, L. (2021). Influence of Work on Andropause and Menopause: A Systematic Review. International Journal of Environmental Research and Public Health, 18(19), 10074. https://doi.org/10.3390/ijerph181910074