
Association between the Concentrations of Metallic Elements in Maternal Blood during Pregnancy and Prevalence of Abdominal Congenital Malformations: The Japan Environment and Children’s Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection in JECS
2.2. Ethical Statement
2.3. Identified Congenital Abnormalities
2.4. Measurements of the Blood Content of Five Metallic Elements
2.5. Selected Participants in Present Study
2.6. Statistical Analysis
3. Results
Parental Characteristics

{kind=link}
{kind=link}
{kind=link}
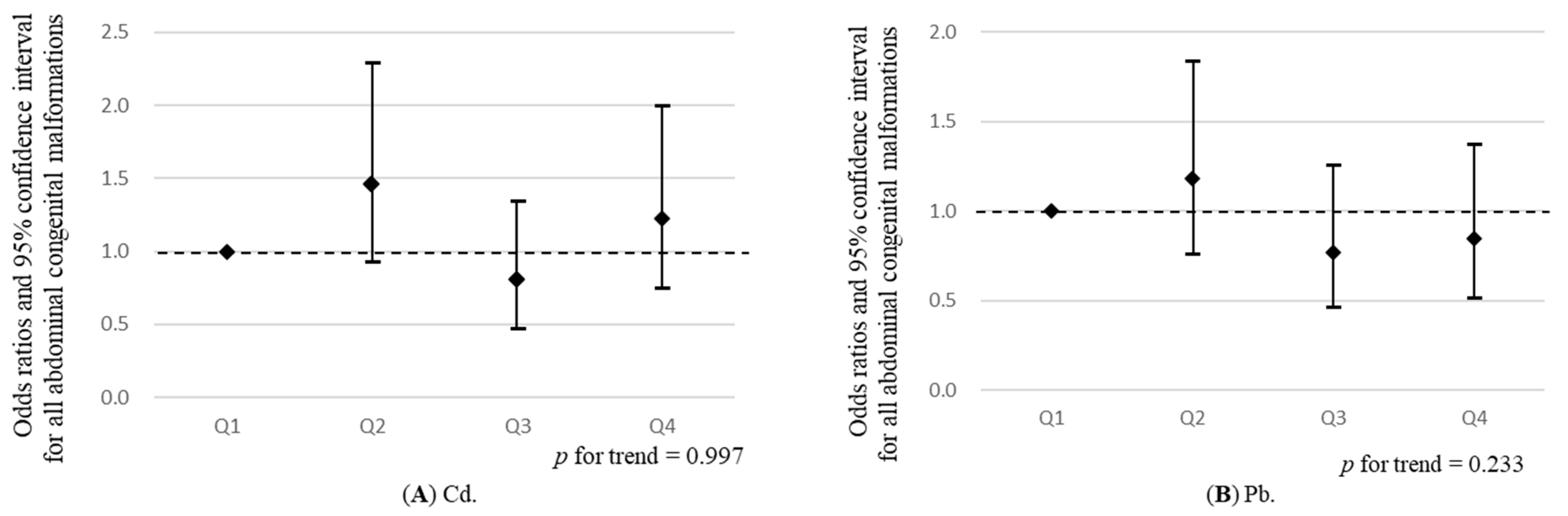
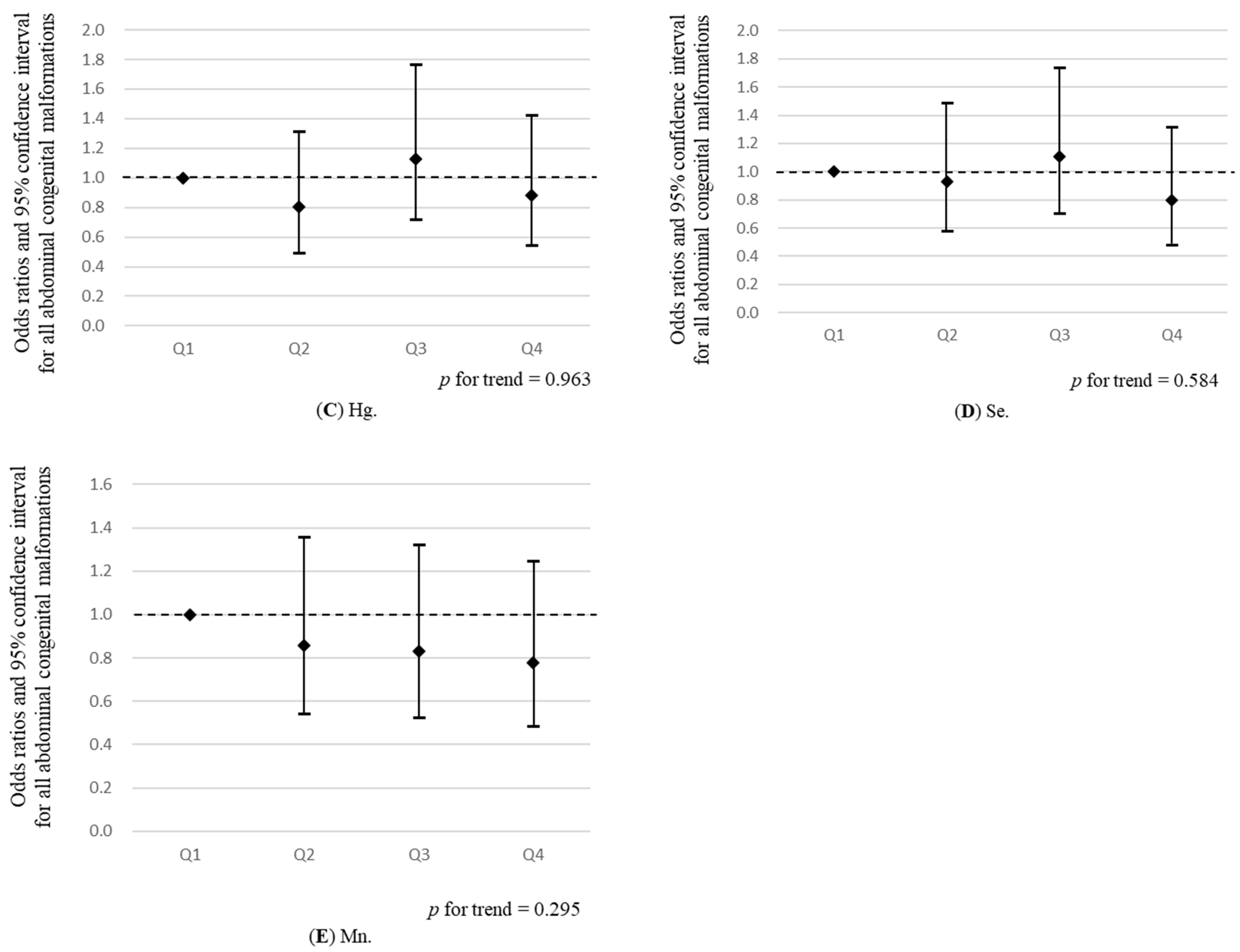
| Cd | Case /Control (n) | Adjusted OR (95% CI) | Pb | Case /Control (n) | Adjusted OR (95% CI) | Hg | Case /Control (n) | Adjusted OR (95% CI) | Se | Case /Control (n) | Adjusted OR (95% CI) | Mn | Case /Control (n) | Adjusted OR (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | 34/23,117 | 1 | Q1 | 37/22,571 | 1 | Q1 | 37/22,268 | 1 | Q1 | 36/22,348 | 1 | Q1 | 40/22,507 | 1 |
| Q2 | 44/21,323 | 1.46 (0.93, 2.29) | Q2 | 44/22,174 | 1.19 (0.76, 1.84) | Q2 | 29/22,218 | 0.80 (0.49, 1.31) | Q2 | 34/22,717 | 0.93 (0.58, 1.49) | Q2 | 35/22,858 | 0.86 (0.55, 1.36) |
| Q3 | 26/22,951 | 0.80 (0.48, 1.35) | Q3 | 28/22,382 | 0.77 (0.47, 1.26) | Q3 | 41/22,335 | 1.13 (0.72, 1.77) | Q3 | 41/22,889 | 1.11 (0.71, 1.74) | Q3 | 33/22,080 | 0.83 (0.52, 1.32) |
| Q4 | 35/21,743 | 1.22 (0.75, 2.00) | Q4 | 30/22,007 | 0.85 (0.52, 1.38) | Q4 | 32/22,313 | 0.88 (0.55, 1.42) | Q4 | 28/21,180 | 0.80 (0.48, 1.32) | Q4 | 31/21,689 | 0.78 (0.48, 1.25) |
| p for trend | 0.997 | 0.233 | 0.963 | 0.585 | 0.296 | |||||||||
| Cd | Case/ Control (n) | Adjusted OR (95% CI) | Pb | Case/ Control (n) | Adjusted OR (95% CI) | Hg | Case/ Control (n) | Adjusted OR (95% CI) | Se | Case/ Control (n) | Adjusted OR (95% CI) | Mn | Case/ Control (n) | Adjusted OR (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diaphragmatic hernia | ||||||||||||||
| Q1 | 10/23,117 | 1 | Q1 | 9/22,571 | 1 | Q1 | 4/22,268 | 1 | Q1 | 7/22,348 | 1 | Q1 | 13/22,507 | 1 |
| Q2 | 11/21,323 | 1.24 (0.52, 2.93) | Q2 | 11/22,174 | 1.24 (0.51, 2.99) | Q2 | 8/222,18 | 2.00 (0.60, 6.64) | Q2 | 7/22,717 | 0.95 (0.33, 2.71) | Q2 | 11/22,858 | 0.80 (0.36, 1.79) |
| Q3 | 10/22,951 | 1.08 (0.44, 2.62) | Q3 | 8/22,382 | 0.89 (0.34, 2.31) | Q3 | 13/22,335 | 3.22 (1.05, 9.90) * | Q3 | 9/22,889 | 1.18 (0.44, 3.18) | Q3 | 9/22,080 | 0.68 (0.29, 1.60) |
| Q4 | 4/21,743 | 0.48 (0.15, 1.58) | Q4 | 7/22,007 | 0.81 (0.30, 2.20) | Q4 | 10/22,313 | 2.50 (0.78, 8.00) | Q4 | 12/21,180 | 1.68 (0.66, 4.31) | Q4 | 2/21,689 | 0.15 (0.03, 0.68) * |
| p for trend | 0.297 | 0.543 | 0.089 | 0.221 | 0.010 | |||||||||
| Omphalocele | ||||||||||||||
| Q1 | 7/23,117 | 1 | Q1 | 11/22,571 | 1 | Q1 | 7/22,268 | 1 | Q1 | 1/22,348 | 1 | Q1 | 7/22,507 | 1 |
| Q2 | 8/21,323 | 1.26 (0.45, 3.51) | Q2 | 8/22,174 | 0.72 (0.29, 1.81) | Q2 | 3/22,218 | 0.44 (0.11, 1.71) | Q2 | 10/22,717 | 9.96 (1.27, 77.88) * | Q2 | 8/22,858 | 1.14 (0.41, 3.16) |
| Q3 | 3/22,951 | 0.44 (0.11, 1.74) | Q3 | 4/22,382 | 0.35 (0.11, 1.12) † | Q3 | 10/22,335 | 1.50 (0.57, 3.96) | Q3 | 10/22,889 | 10.06 (1.28, 78.77) * | Q3 | 4/22,080 | 0.59 (0.17, 2.03) |
| Q4 | 9/21,743 | 1.42 (0.50, 4.00) | Q4 | 4/22,007 | 0.35 (0.11, 1.13) † | Q4 | 7/22,313 | 1.10 (0.38, 3.15) | Q4 | 6/21,180 | 6.56 (0.78, 54.75) † | Q4 | 8/21,689 | 1.22 (0.44, 3.37) |
| p for trend | 0.846 | 0.033 | 0.439 | 0.152 | 0.962 | |||||||||
| Gastroschisis | ||||||||||||||
| Q1 | 4/23,117 | 1 | Q1 | 0/22,571 | - | Q1 | 2/22,268 | 1 | Q1 | 4/22,348 | 1 | Q1 | 2/22,507 | 1 |
| Q2 | 2/21,323 | 0.55 (0.10, 3.03) | Q2 | 2/22,174 | 1 | Q2 | 4/22,218 | 2.06 (0.38, 11.26) | Q2 | 1/22,717 | 0.24 (0.03, 2.13) | Q2 | 4/22,858 | 1.92 (0.35, 10.49) |
| Q3 | 0/22,951 | - | Q3 | 2/22,382 | 1.00 (0.14, 7.09) | Q3 | 1/22,335 | 0.53 (0.05, 5.89) | Q3 | 3/22,889 | 0.72 (0.16, 3.25) | Q3 | 2/22,080 | 0.97 (0.14, 6.91) |
| Q4 | 3/21,743 | 0.88 (0.18, 4.28) | Q4 | 5/22,007 | 2.63 (0.50, 13.70) | Q4 | 2/22,313 | 1.07 (0.15, 7.71) | Q4 | 1/21,180 | 0.26 (0.03, 2.34) | Q4 | 1/21,689 | 0.47 (0.04, 5.26) |
| p for trend | 0.935 | 0.212 | 0.717 | 0.317 | 0.431 | |||||||||
| Cd | Case/ Control (n) | Adjusted OR (95% CI) | Pb | Case/ Control (n) | Adjusted OR (95% CI) | Hg | Case/ Control (n) | Adjusted OR (95% CI) | Se | Case/ Control (n) | Adjusted OR (95% CI) | Mn | Case/ Control (n) | Adjusted OR (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Esophageal atresia with or without fistula | ||||||||||||||
| Q1 | 3/23,117 | 1 | Q1 | 2/22,571 | 1 | Q1 | 3/22,268 | 1 | Q1 | 2/22,348 | 1 | Q1 | 3/22,507 | 1 |
| Q2 | 6/21,323 | 2.94 (0.59, 14.72) | Q2 | 2/22,174 | 0.49 (0.04, 5.43) | Q2 | 1/22,218 | 0.48 (0.04, 5.31) | Q2 | 3/22,717 | 1.67 (0.26, 10.97) | Q2 | 3/22,858 | 1.45 (0.24, 8.69) |
| Q3 | 0/22,951 | - | Q3 | 2/22,382 | 0.95 (0.13, 6.80) | Q3 | 3/22,335 | 1.39 (0.23, 8.36) | Q3 | 2/22,889 | 1.06 (0.14, 8.21) | Q3 | 4/22,080 | 1.98 (0.36, 10.84) |
| Q4 | 1/21,743 | 0.44 (0.04, 5.10) | Q4 | 4/22,007 | 1.88 (0.33, 10.50) | Q4 | 3/22,313 | 1.36 (0.23, 8.27) | Q4 | 3/21,180 | 1.29 (0.19, 8.84) | Q4 | 0/21,689 | - |
| p for trend | 0.362 | 0.346 | 0.527 | 0.946 | 0.424 | |||||||||
| Duodenal atresia/stenosis | ||||||||||||||
| Q1 | 3/23,117 | 1 | Q1 | 4/22,571 | 1 | Q1 | 3/22,268 | 1 | Q1 | 5/22,348 | 1 | Q1 | 0/22,507 | - |
| Q2 | 2/21,323 | 0.72 (0.12, 4.39) | Q2 | 1/22,174 | 0.25 (0.03, 2.27) | Q2 | 3/22,218 | 0.99 (0.20, 4.90) | Q2 | 2/22,717 | 0.39 (0.08, 2.02) | Q2 | 3/22,858 | 1 |
| Q3 | 3/22,951 | 0.98 (0.19, 5.05) | Q3 | 2/22,382 | 0.50 (0.09, 2.75) | Q3 | 2/22,335 | 0.64 (0.11, 3.82) | Q3 | 4/22,889 | 0.76 (0.20, 2.86) | Q3 | 4/22,080 | 1.37 (0.31, 6.14) |
| Q4 | 3/21,743 | 1.01 (0.19, 5.44) | Q4 | 4/22,007 | 0.99 (0.24, 4.06) | Q4 | 3/22,313 | 0.92 (0.18, 4.62) | Q4 | 0/21,180 | - | Q4 | 4/21,689 | 1.35 (0.30, 6.04) |
| p for trend | 0.915 | 0.910 | 0.812 | 0.666 | 0.702 | |||||||||
| Intestinal atresia/stenosis | ||||||||||||||
| Q1 | 3/23,117 | 1 | Q1 | 3/22,571 | 1 | Q1 | 3/22,268 | 1 | Q1 | 2/22,348 | 1 | Q1 | 4/22,507 | 1 |
| Q2 | 6/21,323 | 2.28 (0.56, 9.20) | Q2 | 4/22,174 | 1.40 (0.31, 6.29) | Q2 | 4/22,218 | 1.30 (0.29, 5.81) | Q2 | 5/22,717 | 2.41 (0.47, 12.47) | Q2 | 2/22,858 | 0.47 (0.09, 2.58) |
| Q3 | 2/22,951 | 0.73 (0.12, 4.46) | Q3 | 3/22,382 | 1.06 (0.21, 5.27) | Q3 | 4/22,335 | 1.26 (0.28, 5.64) | Q3 | 6/22,889 | 2.82 (0.56, 14.06) | Q3 | 2/22,080 | 0.49 (0.09, 2.68) |
| Q4 | 2/21,743 | 0.87 (0.14, 5.46) | Q4 | 3/22,007 | 1.12 (0.22, 5.64) | Q4 | 2/22,313 | 0.62 (0.10, 3.76) | Q4 | 0/21,180 | - | Q4 | 5/21,689 | 1.22 (0.33, 4.57) |
| p for trend | 0.575 | 0.989 | 0.643 | 0.215 | 0.717 | |||||||||
| Anorectal atresia/stenosis | ||||||||||||||
| Q1 | 5/23,117 | 1 | Q1 | 10/22,571 | 1 | Q1 | 11/22,268 | 1 | Q1 | 15/22,348 | 1 | Q1 | 12/22,507 | 1 |
| Q2 | 11/21,323 | 2.57 (0.89, 7.43) † | Q2 | 15/22,174 | 1.65 (0.74, 3.67) | Q2 | 6/22,218 | 0.54 (0.20, 1.47) | Q2 | 7/22,717 | 0.49 (0.20, 1.19) | Q2 | 5/22,858 | 0.41 (0.14, 1.15) † |
| Q3 | 9/22,951 | 2.02 (0.67, 6.11) | Q3 | 5/22,382 | 0.57 (0.19, 1.68) | Q3 | 10/22,335 | 0.90 (0.38, 2.12) | Q3 | 7/22,889 | 0.50 (0.20, 1.24) | Q3 | 7/22,080 | 0.58 (0.23, 1.47) |
| Q4 | 10/21,743 | 2.65 (0.88, 8.00) † | Q4 | 5/22,007 | 0.62 (0.21, 1.83) | Q4 | 8/22,313 | 0.69 (0.28, 1.73) | Q4 | 6/21,180 | 0.48 (0.18, 1.24) | Q4 | 11/21,689 | 0.93 (0.41, 2.11) |
| p for trend | 0.149 | 0.158 | 0.633 | 0.099 | 0.969 | |||||||||
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- World Health Organization. World Health Organization Media Centre Congenital Anomalies Fact Sheet Updated September 2016. Available online: https://www.who.int/news-room/fact-sheets/detail/congenital-anomalies (accessed on 16 November 2020).
- Tashiro, A.; Yoshida, H.; Okamoto, E. Infant, neonatal, and post-neonatal mortality trends in a disaster region and in Japan, 2002–2012: Aa multi-attribute compositional study. BMC Pub. Health 2019, 19, 1085. [Google Scholar] [CrossRef]
- National Research Council. Toxicologic Effects of Methylmercury; National Academy Press: Washington, WA, USA, 2000.
- Alexander, P.G.; Clark, K.L.; Tuan, R.S. Prenatal exposure to environmental factors and congenital limb defects. Birth Defects Res. C Embryo Today 2016, 108, 243–273. [Google Scholar] [CrossRef]
- Wani, A.L.; Ara, A.; Usmani, J.A. Lead toxicity: A review. Interdiscip. Toxicol. 2015, 8, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewicka, I.; Kocylowski, R.; Grzesiak, M.; Gaj, Z.; Oszukowski, P.; Suliburska, J. Selected trace elements concentrations in pregnancy and their possible role-literature review. Ginekol. Pol. 2017, 88, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Satoh, H.; Murata, K.; Eto, K. Adverse effects of methylmercury: Environmental health research implications. Environ. Health Perspect. 2010, 118, 1137–1145. [Google Scholar] [CrossRef] [Green Version]
- Ou, Y.Q.; Bloom, M.S.; Nie, Z.Q.; Han, F.Z.; Mai, J.Z.; Chen, J.M.; Lin, S.; Liu, X.; Zhuang, J. Associations between toxic and essential trace elements in maternal blood and fetal congenital heart defects. Environ. Int. 2017, 106, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, M.; Shibata, E.; Askew, D.J.; Morokuma, S.; Aiko, Y.; Senju, A.; Araki, S.; Sanefuji, M.; Ishihara, Y. Associations between metal concentrations in whole blood and placenta previa and placenta accreta: The Japan Environment and Children’s Study (JECS). Environ. Health Prev. Med. 2019, 24, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, M.; Sakurai, K.; Eguchi, A.; Yamazaki, S.; Nakayama, S.F.; Isobe, T.; Takeuchi, A.; Sato, T.; Hata, A.; Moriaf, C.; et al. Association between blood manganese level during pregnancy and birth size: The Japan environment and children’s study (JECS). Environ. Res. 2019, 172, 117–126. [Google Scholar] [CrossRef]
- Kawamoto, T.; Nitta, H.; Murata, K.; Toda, E.; Tsukamoto, N.; Hasegawa, M.; Yamagata, Z.; Kayama, F.; Kishi, R.; Ohya, Y.; et al. Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Michikawa, T.; Nitta, H.; Nakayama, S.F.; Yamazaki, S.; Isobe, T.; Tamura, K.; Suda, E.; Ono, M.; Yonemoto, J.; Iwai-Shimada, M.; et al. Baseline profile of participants in the Japan Environment and Children’s Study (JECS). J. Epidemiol. 2018, 28, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Mezawa, H.; Tomotaki, A.; Yamamoto-Hanada, K.; Ishitsuka, K.; Ayabe, T.; Konishi, M.; Saito, M.; Yang, L.; Suganuma, N.; Hirahara, F.; et al. Prevalence of congenital anomalies in the Japan Environment and Children’s Study. J. Epidemiol. 2019, 29, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, S.F.; Iwai-Shimada, M.; Oguri, T.; Isobe, T.; Takeuchi, A.; Kobayashi, Y.; Michikawa, T.; Yamazaki, S.; Nitta, H.; Kawamoto, T.; et al. Blood mercury, lead, cadmium, manganese and selenium levels in pregnant women and their determinants: The Japan Environment and Children’s Study (JECS). J. Expo. Sci. Environ. Epidemiol. 2019, 29, 633–647. [Google Scholar] [CrossRef] [Green Version]
- Sanders, A.P.; Desrosiers, T.A.; Warren, J.L.; Herring, A.H.; Enright, D.; Olshan, A.F.; Meyer, R.E.; Fry, R.C. Association between arsenic, cadmium, manganese, and lead levels in private wells and birth defects prevalence in North Carolina: A semi-ecologic study. BMC Public Health 2014, 14, 955. [Google Scholar] [CrossRef] [Green Version]
- Cordier, S.; Chevrier, C.; Robert-Gnansia, E.; Lorente, C.; Brula, P.; Hours, M. Risk of congenital anomalies in the vicinity of municipal solid waste incinerators. Occup. Environ. Med. 2004, 61, 8–15. [Google Scholar]
- Karakis, I.; Landau, D.; Yitshak-Sade, M.; Hershkovitz, R.; Rotenberg, M.; Sarov, B.; Grotto, I.; Novack, L. Exposure to metals and congenital anomalies: A biomonitoring study of pregnant Bedouin-Arab women. Sci. Total Environ. 2015, 517, 106–112. [Google Scholar] [CrossRef]
- Yamada, M.; Asakura, K.; Sasaki, S.; Hirota, N.; Notsu, A.; Todoriki, H.; Miura, A.; Fukui, M.; Date, C. Estimation of intakes of copper, zinc, and manganese in Japanese adults using 16-day semi-weighed diet records. Asia Pac. J. Clin. Nutr. 2014, 23, 465–472. [Google Scholar]
- Stoll, C.; Alembik, Y.; Dott, B.; Roth, M.P. Risk factors in congenital abdominal wall defects (omphalocele and gastroschisi): A study in a series of 265,858 consecutive births. Ann. Genet. 2001, 44, 201–208. [Google Scholar] [CrossRef]
- Hackshaw, A.; Rodeck, C.; Boniface, S. Maternal smoking in pregnancy and birth defects: A systematic review based on 173 687 malformed cases and 11.7 million controls. Hum. Reprod. Update 2011, 17, 589–604. [Google Scholar] [CrossRef] [Green Version]
- Caputo, C.; Wood, E.; Jabbour, L. Impact of fetal alcohol exposure on body systems: A systematic review. Birth Defects Res. C Embryo Today 2016, 108, 174–180. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, X.H.; Zheng, X.M.; Liu, T.Z.; Zhang, W.B.; Zheng, H.; Chen, M.F. Maternal gestational smoking, diabetes, alcohol drinking, pre-pregnancy obesity and the risk of cryptorchidism: A systematic review and meta-analysis of observational studies. PLoS ONE 2015, 10, e0119006. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Chen, X.L.; Chen, H.J.; Ma, Z.L.; Zhou, J.W. Maternal alcohol consumption before and during pregnancy and the risks of congenital heart defects in offspring: A systematic review and meta-analysis. Congenit. Heart Dis. 2015, 10, E216–E224. [Google Scholar] [CrossRef]



| Metallic Elements | All (n = 89,273) | Normal (n = 89,134) | Abdominal Congenital Malformations (n = 139) | p | ||||
|---|---|---|---|---|---|---|---|---|
| Minimum | 25th Percentile | Median | 75th Percentile | Maximum | Median (IQR) | Median (IQR) | ||
| Pb (ng/g) | 1.2 | 4.7 | 5.84 | 7.32 | 110 | 5.85 (4.70, 7.32) | 5.53 (4.59, 7.00) | 0.094 |
| Cd (ng/g) | 0.0951 | 0.494 | 0.661 | 0.902 | 5.33 | 0.66 (0.49, 0.90) | 0.62 (0.50, 0.92) | 0.546 |
| Hg (n/g) | 0.182 | 2.55 | 3.64 | 5.2 | 58.8 | 3.64 (2.55, 5.20) | 3.69 (2.45, 5.01) | 0.827 |
| Se (ng/g) | 82.8 | 156 | 168 | 182 | 976 | 168.00 (156.00, 182.00) | 168.00 (155.00, 180.00) | 0.773 |
| Mn (ng/g) | 3.06 | 12.6 | 15.3 | 18.6 | 60.8 | 15.30 (12.60, 18.60) | 14.90 (12.20, 18.20) | 0.458 |
| Abdominal Congenital Malformations | ICD-10 Code | All | Male | Female | Unknown |
|---|---|---|---|---|---|
| N | N (%) | N (%) | N (%) | ||
| Diaphragmatic hernia | Q79.0 | 35 | 16 (45.7) | 19 (54.3) | 0 (0.0) |
| Omphalocele | Q79.2 | 27 | 11 (40.7) | 16 (59.3) | 0 (0.0) |
| Gastroschisis | Q79.3 | 9 | 6 (66.7) | 3 (33.3) | 0 (0.0) |
| Esophageal atresia with or without fistula | Q39.0 Q39.1 | 10 | 5 (50.0) | 4 (40.0) | 1 (10.0) |
| Duodenal atresia/stenosis | Q41.0 | 11 | 7 (63.6) | 4 (36.4) | 0 (0.0) |
| Intestinal atresia/stenosis | Q41.1–Q41.9 | 13 | 6 (46.2) | 7 (53.8) | 0 (0.0) |
| Anorectal atresia/stenosis | Q42.0–Q42.9 | 35 | 21 (60.0) | 14 (40.0) | 0 (0.0) |
| Characteristics | All | Non-Malformed | Abdominal Congenital Malformations | |
|---|---|---|---|---|
| Maternal Characteristics | ||||
| Age at delivery (years old) | N or N (%) | Mean ± SD | N (%) | N (%) |
| <25 | 10,265 (11.50) | 10,244 (11.49) | 21 (15.11) | |
| 25 to <30 | 26,545 (29.73) | 26,507 (29.74) | 38 (27.34) | |
| 30 to <35 | 31,260 (35.02) | 31,216 (35.02) | 44 (31.65) | |
| ≥35 | 21,203 (23.75) | 21,167 (23.75) | 36 (25.90) | |
| Mean ± SD | Mean ± SD | |||
| Pre-pregnancy weight | 89,234 | 53.12 ± 8.85 | 53.11 ± 8.85 | 53.59 ± 9.01 |
| Height | 89,253 | 158.12 ± 5.35 | 158.12 ± 5.35 | 158.57 ± 4.95 |
| Parity | N or N (%) | N (%) | N (%) | |
| Nulliparous | 43,097 (48.44) | 43,022 (48.43) | 75 (54.35) | |
| Multiparous | 45,870 (51.56) | 45,807 (51.57) | 63 (45.65) | |
| Smoking habit | ||||
| Never | 51,924 (58.16) | 51,846 (58.17) | 78 (56.12) | |
| Quit before pregnancy | 21,217 (23.77) | 21,172 (23.75) | 45 (32.37) | |
| Smoking during pregnancy | 16,132 (18.07) | 16,116 (18.08) | 16 (11.51) | |
| Drinking habit | ||||
| Never | 30,825 (34.53) | 30,773 (34.52) | 52 (37.41) | |
| Quit before pregnancy | 49,330 (55.26) | 49,252 (55.26) | 78 (56.12) | |
| Drinking during pregnancy | 9118 (10.21) | 9109 (10.22) | 9 (6.47) | |
| Educational duration (year) | ||||
| <10 | 4137 (4.69) | 4129 (4.68) | 8 (5.84) | |
| 10–<13 | 27,892 (31.59) | 27,855 (31.60) | 37 (27.01) | |
| 13–<15 | 37,288 (42.23) | 37,218 (42.22) | 70 (51.09) | |
| 15–<17 | 18,977 (21.49) | 18,955 (21.50) | 22 (16.06) | |
| Paternal characteristics | ||||
| Age at entry (years old) | N or N (%) | N (%) | N (%) | |
| <25 | 3385 (7.22) | 3379 (7.22) | 6 (8.57) | |
| 25 to <30 | 11,210 (23.92) | 11,194 (23.92) | 16 (22.86) | |
| 30 to <35 | 15,516 (33.11) | 15,485 (33.09) | 31 (44.29) | |
| ≥35 | 16,753 (35.75) | 16,736 (35.77) | 17 (24.29) | |
| Smoking habit | ||||
| Never | 24,084 (26.98) | 24,051 (26.98) | 33 (23.74) | |
| Quit before pregnancy | 20,753 (23.25) | 20,713 (23.24) | 40 (28.78) | |
| Smoking during pregnancy | 44,436 (49.78) | 44,370 (49.78) | 66 (47.48) | |
| Educational duration (year) | ||||
| <10 | 6430 (7.31) | 6423 (7.31) | 7 (5.11) | |
| 10–<13 | 32,538 (36.98) | 32,489 (36.99) | 49 (35.77) | |
| 13–<15 | 19,880 (22.60) | 19,850 (22.60) | 30 (21.90) | |
| 15–<17 | 29,132 (33.11) | 29,081 (33.11) | 51 (37.23) | |
| Household income (million yen) | ||||
| <2 | 4622 (5.59) | 4614 (5.59) | 8 (6.30) | |
| 2–<4 | 28,705 (34.73) | 28,663 (34.74) | 42 (33.07) | |
| 4–<6 | 27,334 (33.08) | 27,290 (33.07) | 44 (34.65) | |
| 6–<8 | 13,115 (15.87) | 13,092 (15.87) | 23 (18.11) | |
| 8–<10 | 5359 (6.48) | 5351 (6.48) | 8 (6.30) | |
| ≥10 | 3507 (4.24) | 3505 (4.25) | 2 (1.57) | |
| All | Non-Malformed | Abdominal Congenital Malformations | p | ||
|---|---|---|---|---|---|
| Infant characteristics | |||||
| N or N (%) | Mean ± SD | Mean ± SD | Mean ± SD | p a | |
| Gestational weeks | 89235 | 38.87 ± 1.46 | 38.87 ± 1.46 | 37.76 ± 2.68 | <0.001 |
| Birth weight | 89183 | 3033.77 ± 402.47 | 3034.21 ± 401.95 | 2743.65 ± 594.58 | <0.001 |
| N (%) | N (%) | p b | |||
| Vaginal delivery | 72,701 (81.65) | 72,612 (81.68) | 89 (64.96) | <0.001 | |
| Cesarean section | 16,339 (18.35) | 16,291 (18.32) | 48 (35.04) | ||
| Sex | |||||
| Male | 45,662 (51.15) | 45,591 (51.15) | 71 (51.08) | <0.001 | |
| Female | 43,609 (48.85) | 43,542 (48.85) | 67 (48.20) | ||
| Unknown | 2 (0.00) | 1 (0.00) | 1 (0.72) | ||
| Birth year | |||||
| 2011 | 8713 (9.76) | 8696 (9.76) | 17 (12.23) | 0.807 | |
| 2012 | 25,335 (28.38) | 25,297 (28.38) | 38 (27.34) | ||
| 2013 | 31,815 (35.64) | 31,767 (35.64) | 48 (34.53) | ||
| 2014 | 23,410 (26.22) | 23,374 (26.22) | 36 (25.90) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyashita, C.; Saijo, Y.; Ito, Y.; Ikeda-Araki, A.; Itoh, S.; Yamazaki, K.; Kobayashi, S.; Ait Bamai, Y.; Masuda, H.; Tamura, N.; et al. Association between the Concentrations of Metallic Elements in Maternal Blood during Pregnancy and Prevalence of Abdominal Congenital Malformations: The Japan Environment and Children’s Study. Int. J. Environ. Res. Public Health 2021, 18, 10103. https://doi.org/10.3390/ijerph181910103
Miyashita C, Saijo Y, Ito Y, Ikeda-Araki A, Itoh S, Yamazaki K, Kobayashi S, Ait Bamai Y, Masuda H, Tamura N, et al. Association between the Concentrations of Metallic Elements in Maternal Blood during Pregnancy and Prevalence of Abdominal Congenital Malformations: The Japan Environment and Children’s Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10103. https://doi.org/10.3390/ijerph181910103
Chicago/Turabian StyleMiyashita, Chihiro, Yasuaki Saijo, Yoshiya Ito, Atsuko Ikeda-Araki, Sachiko Itoh, Keiko Yamazaki, Sumitaka Kobayashi, Yu Ait Bamai, Hideyuki Masuda, Naomi Tamura, and et al. 2021. "Association between the Concentrations of Metallic Elements in Maternal Blood during Pregnancy and Prevalence of Abdominal Congenital Malformations: The Japan Environment and Children’s Study" International Journal of Environmental Research and Public Health 18, no. 19: 10103. https://doi.org/10.3390/ijerph181910103
APA StyleMiyashita, C., Saijo, Y., Ito, Y., Ikeda-Araki, A., Itoh, S., Yamazaki, K., Kobayashi, S., Ait Bamai, Y., Masuda, H., Tamura, N., Itoh, M., Yamaguchi, T., Yamazaki, S., Kishi, R., & The Japan Environment and Children’s Study Group. (2021). Association between the Concentrations of Metallic Elements in Maternal Blood during Pregnancy and Prevalence of Abdominal Congenital Malformations: The Japan Environment and Children’s Study. International Journal of Environmental Research and Public Health, 18(19), 10103. https://doi.org/10.3390/ijerph181910103