
A Systematic Review of the Impact of Wildfires on Sleep Disturbances


Abstract
:1. Introduction
2. Method
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
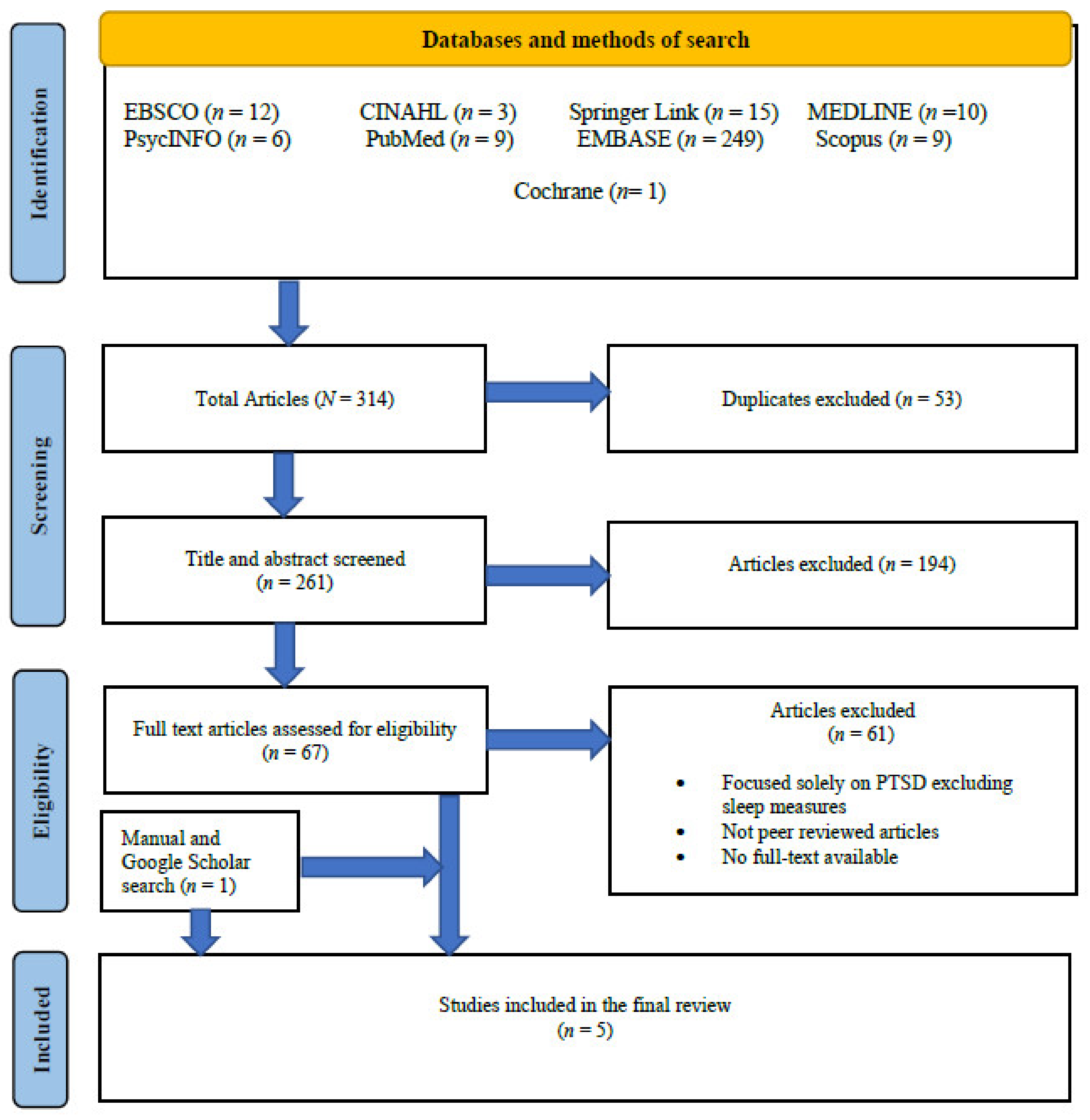
2.5. Study Selection
2.6. Quality Assessment
3. Results
3.1. Findings from the Included Studies
3.1.1. Prevalence of Sleep Disorders
3.1.2. Prevalence of Sleep Disturbances in Children
3.1.3. Most Prevalent Sleep Disturbances
3.1.4. Prevalence of Sleep Disturbances and PTSD
3.1.5. Proximity to Fires, Gender, Age and Sleep Disturbances
3.1.6. Timing of Sleep Disturbance Assessment Relative to Fire Occurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Agyapong, V.I.O.; Juhas, M.; Omege, J.; Denga, E.; Nwaka, B.; Akinjise, I.; Corbett, S.E.; Brown, M.; Chue, P.; Li, X.-M.; et al. Prevalence Rates and Correlates of Likely Post-Traumatic Stress Disorder in Residents of Fort McMurray 6 Months After a Wildfire. Int. J. Ment. Health Addict. 2021, 14, 632–650. [Google Scholar] [CrossRef]
- Change Science Program (USA). Climate Change Impacts in the United States, Highlights; US National Climate Assessment; US Global Change Research Program: Washington, DC, USA, 2014. [Google Scholar]
- Pengilley, V. Milk Shortage Fears Amid Australian Bushfires as Dairy Farmer Fears Devastation from Animal Deaths. ABC News, 6 January 2020. Available online: https://www.abc.net.au/news/2020-01-06/nsw-fires-put-dairy-industry-arisk/11842386(accessed on 10 April 2021).
- Bowman, D.M.J.S.; Williamson, G.; Abatzoglou, J.T.; Kolden, C.A.; Cochrane, M.A.; Smith, A.M.S. Human exposure and sensitivity to globally extreme wildfire events. Nat. Ecol. Evol. 2017, 1, 58. [Google Scholar] [CrossRef] [PubMed]
- Mcrae, R.; Sharples, J. Assessing mitigation of the risk from extreme wildfires using MODIS hotspot data. In Proceedings of the 21st International Congress on Modelling and Simulation, Gold Coast, Australia, 29 November–4 December 2015; Available online: https://www.mssanz.org.au/modsim2015/A4/mcrae2.pdf (accessed on 23 April 2021).
- Strauss, D.; Bednar, L.; Mees, R. Do one percent of the forest fires cause ninety-nine percent of the damage? For. Sci. 1989, 35, 319–328. [Google Scholar]
- Williams, J. Exploring the onset of high-impact mega-fires through a forest land management prism. For. Ecol. Manag. 2013, 294, 4–10. [Google Scholar] [CrossRef]
- Willis, O. Recognising the Mental Health Impact of Bushfires as Another Summer Approaches. ABC News, 13 October 2020. Available online: //www.abc.net.au/news/health/2020-10-13/recognising-the-mental-health-im-pact-of-bushfires/12760568(accessed on 21 May 2021).
- Guha-Sapir, D.; Below, R.; Hoyois, P. EM-DAT: International Disaster Database; Université Catholique de Louvain: Ottignies-Louvain-la-Neuve, Belgium, 2015. [Google Scholar]
- Berry, H.L.; Bowen, K.; Kjellstrom, T. Climate change and mental health: A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef]
- Hirschberger, G. Collective trauma and the social construction of meaning. Front. Psychol. 2018, 9, 1441. [Google Scholar] [CrossRef]
- Smith, E.; Burkle, J.F., Jr. Collective Trauma is Real, and Could Hamper Australian Communities’ Bushfire Recovery. The Conversation. 24 February 2020. Available online: https://aifs.gov.au/cfca/2020/02/25/collective-trauma-re-al-and-could-hamper-Australian-communities-bushfire (accessed on 21 May 2021).
- Lowe, S.R.; Bonumwezi, J.L.; Valdespino-Hayden, Z.; Galea, S. Posttraumatic stress and depression in the aftermath of environmental disasters: A review of quantitative studies published in 2018. Curr. Environ. Health Rep. 2019, 6, 344–360. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publishing, Inc.: Washington, DC, USA, 2013. [Google Scholar]
- Germain, A.; Shear, M.K.; Hall, M.; Buysse, D.J. Effects of a brief behavioral treatment for PTSD-related sleep disturbances: A pilot study. Behav. Res. Ther. 2007, 45, 627–632. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Roth, T. Characteristics of insomnia in the United States: Results of the 1991 National Sleep Foundation Survey. I. Sleep 1999, 22, 347–353. [Google Scholar]
- Sateia, M.J.; Doghramji, K.; Hauri, P.J.; Morin, C.M. Evaluation of chronic insomnia. An american academy of sleep medicine review. Sleep 2000, 23, 1–66. [Google Scholar] [CrossRef] [Green Version]
- Kato, H.; Asukai, N.; Miyake, Y.; Minakawa, K.; Nishiyama, A. Post-traumatic symptoms among younger and elderly evacuees in the early stages following the 1995 Hanshin-Awaji earthquake in Japan. Acta Psychiatr. Scand. 1996, 93, 477–481. [Google Scholar] [CrossRef]
- Kuch, K.; Cox, B.J. Symptoms of PTSD in 124 survivors of the Holocaust. Am. J. Psychiatry 1992, 149, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Jang, T.-W.; Jeong, K.S.; Ahn, Y.-S.; Choi, K.-S. The relationship between the pattern of shift work and sleep disturbances in Korean firefighters. Int. Arch. Occup. Environ. Health 2019, 93, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, I.; Eguia, F.; Gelaye, B.; Peterlin, B.L.; Tadesse, M.G.; Lemma, S.; Berhane, Y.; A Williams, M. Sleep disturbances and quality of life in Sub-Saharan African migraineurs. J. Headache Pain 2015, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadorff, M.R.; Nazem, S.; Fiske, A. Insomnia symptoms, nightmares, and suicidal ideation in a college student sample. Sleep 2011, 34, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Roth, T.; Ancoli-Israel, S. Daytime consequences and correlates of insomnia in the United States: Results of the 1991 national sleep foundation survey. II. Sleep Res Sleep Med. 1999, 22, S354–S358. [Google Scholar]
- Simon, G.E.; Vonkorff, M. Prevalence, burden, and treatment of insomnia in primary care. Am. J. Psychiatry 1997, 154, 1417–1423. [Google Scholar]
- Uchmanowicz, I.; Markiewicz, K.; Uchmanowicz, B.; Kołtuniuk, A.; Rosińczuk, J. The relationship between sleep disturbances and quality of life in elderly patients with hypertension. Clin. Interv. Aging 2019, 14, 155–165. [Google Scholar] [CrossRef] [Green Version]
- Fergusson, D.M.; Horwood, L.J.; Boden, J.M.; Mulder, R.T. Impact of a major disaster on the mental health of a well-studied cohort. JAMA Psychiatry 2014, 71, 1025. [Google Scholar] [CrossRef] [Green Version]
- Goldmann, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef]
- Laugharne, J.; Van de Watt, G.; Janca, A. After the fire: The mental health consequences of fire disasters. Curr. Opin. Psychiatry 2011, 24, 72–77. [Google Scholar] [CrossRef]
- Babson, K.A.; Feldner, M.T. Temporal relations between sleep problems and both traumatic event exposure and PTSD: A critical review of the empirical literature. J. Anxiety Disord. 2010, 24, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.M. Estimating disease prevalence and incidence using administrative data: Some assembly required. J. Rheumatol. 2013, 40, 1241–1243. [Google Scholar] [CrossRef] [Green Version]
- Noordzij, M.; Dekker, F.; Zoccali, C.; Jager, K.J. Measures of disease frequency: Prevalence and incidence. Nephron Clin. Pract. 2010, 115, c17–c20. [Google Scholar] [CrossRef] [PubMed]
- Siegel, C.E.; Laska, E.; Meisner, M. Estimating capacity requirements for mental health services after a disaster has occurred: A call for new data. Am. J. Public Health 2004, 94, 582–585. [Google Scholar] [CrossRef] [PubMed]
- Colvonen, P.J.; Straus, L.D.; Stepnowsky, C.; McCarthy, M.; Goldstein, L.; Norman, S.B. Recent Advancements in Treating Sleep Disorders in Co-Occurring PTSD. Curr. Psychiatry Rep. 2018, 20, 48. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, 713–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaac, F.; Kennedy, G.; Toukshati, S. Bushfires and Sleep Disorders. PROSPERO. Available online: https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=231659 (accessed on 17 February 2021).
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. -Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Krakow, B.J.; Melendrez, D.C.; Johnston, L.G.; Clark, J.O.; Santana, E.M.; Warner, T.D.; Hollifield, M.A.; Schrader, R.; Lee, S.A. Sleep dynamic therapy for cerro grande fire evacuees with posttraumatic stress symptoms: A preliminary report. J. Clin. Psychiatry 2002, 63, 673–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psarros, C.; Theleritis, C.; Economou, M.; Tzavara, C.; Kioulos, K.T.; Mantonakis, L.; Soldatos, C.R.; Bergiannaki, J.D. Insomnia is related to the early development of PTSD in victims of wildfires. Plur. Psychiatry II 2015, 21, 29–34. [Google Scholar]
- Belleville, G.; Ouellet, M.-C.; Morin, C.M. Post-traumatic stress among evacuees from the 2016 fort mcmurray wildfires: Exploration of psychological and sleep symptoms three months after the evacuation. Int. J. Environ. Res. Public Health 2019, 16, 1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, R.; Ribbe, D.P.; Cunningham, P.B.; Weddle, J.D.; Langley, A.K. Psychological impact of fire disaster on children and their parents. Behav. Modif. 2002, 26, 163–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krakow, B.; Haynes, P.L.; Warner, T.D.; Santana, E.; Melendrez, D.; Johnston, L.; Hollifield, M.; Sisley, B.N.; Koss, M.; Shafer, L. Nightmares, insomnia, and sleep-disordered breathing in fire evacuees seeking treatment for posttraumatic sleep disturbance. J. Trauma Stress 2004, 17, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Psarros, C.; Theleritis, C.; Economou, M.; Tzavara, C.; Kioulos, K.T.; Mantonakis, L.; Soldatos, C.R.; Bergiannaki, J.-D. Insomnia and PTSD one month after wildfires: Evidence for an independent role of the “fear of imminent death”. Int. J. Psychiatry Clin. Pr. 2017, 21, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Silveira, S.; Kornbluh, M.; Withers, M.; Grennan, G.; Ramanathan, V.; Mishra, J. Chronic mental health sequelae of climate change extremes: A case study of the deadliest californian wildfire. Int. J. Environ. Res. Public Health 2021, 18, 1487. [Google Scholar] [CrossRef] [PubMed]
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a clini-cian-administered PTSD scale. J. Trauma Stress 1995, 8, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Krakow, B.; Melendrez, D.; Ferreira, E.; Clark, J.; Warner, T.D.; Sisley, B.; Sklar, D. Prevalence of insomnia symptoms in patients with sleep-disordered breathing. Chest 2001, 120, 1923–1929. [Google Scholar] [CrossRef] [Green Version]
- Quan, S.F.; Gillin, J.C.; Littner, M.R.; Shepard, J.W. Sleep–related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. Sleep 1999, 22, 667–689. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Lichstein, K.L.; Morin, C.M. Recommendations for a standard research assessment of Insomnia. Sleep 2006, 29, 1155–1173. [Google Scholar] [CrossRef]
- Germain, A.; Hall, M.; Krakow, B.; Shear, M.K.; Buysse, D.J. A brief sleep scale for posttraumatic stress disorder: Pittsburgh sleep quality index addendum for PTSD. J. Anxiety Disord. 2005, 19, 233–244. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Matsumoto, S.; Yamaoka, K.; Inoue, M.; Inoue, M.; Muto, S.; Teikyo Ishinomaki Research Group. Implications for social support on prolonged sleep difficulties among a disaster-affected population: Second report from a cross-sectional survey in Ishinomaki, Japan. PLoS ONE 2015, 10, e0130615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, B.S.; La Greca, A.M.; A Colgan, C.; Herge, W.; Chan, S.; Medzhitova, J.; Short, M.; Auslander, B. Sleep problems and posttraumatic stress: Children exposed to a natural disaster. J. Pediatr. Psychol. 2020, 45, 1016–1026. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, M.M.; Colvonen, P.J.; Norman, S.B.; Afari, N.; Allard, C.; Drummond, S.P. Prevalence and mental health correlates of Insomnia in first-encounter veterans with and without military sexual trauma. Sleep 2015, 38, 1547–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milanak, M.E.; Zuromski, K.; Cero, I.; Wilkerson, A.K.; Resnick, H.S.; Kilpatrick, D.G. Traumatic event exposure, posttraumatic stress disorder, and sleep disturbances in a national sample of U.S. adults. J. Trauma Stress 2019, 32, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neylan, T.C.; Marmar, C.R.; Metzler, T.J.; Weiss, D.S.; Zatzick, D.F.; Delucchi, K.L.; Wu, R.M.; Schoenfeld, F.B. Sleep disturbances in the Vietnam generation: Findings from a nationally representative sample of male vietnam veterans. Am. J. Psychiatry 1998, 155, 929–933. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Shapiro, C.M. Sleep disturbances and psychiatric disorders associated with posttraumatic stress disorder in the general population. Compr. Psychiatry 2000, 41, 469–478. [Google Scholar] [CrossRef]
- Plumb, T.R.; Peachey, J.T.; Zelman, D.C. Sleep disturbance is common among servicemembers and veterans of Operations Enduring Freedom and Iraqi Freedom. Psychol. Serv. 2014, 11, 209–219. [Google Scholar] [CrossRef]
- Williams, S.G.; Collen, J.; Orr, N.; Holley, A.B.; Lettieri, C. Sleep disorders in combat-related PTSD. Sleep Breath. 2015, 19, 175–182. [Google Scholar] [CrossRef]
- Secrist, M.E.; John, S.G.; Harper, S.L.; Edge, N.A.C.; Sigel, B.A.; Sievers, C.; Kramer, T. Nightmares in treatment-seeking youth: The role of cumulative trauma exposure. J. Child Adolesc. Trauma 2020, 13, 249–256. [Google Scholar] [CrossRef]
- Arjmand, H.-A.; Seabrook, E.; Bakker, D.; Rickard, N. Mental health consequences of adversity in australia: National bushfires associated with increased depressive symptoms, while COVID-19 pandemic associated with increased symptoms of anxiety. Front. Psychol. 2021, 12, 635158. [Google Scholar] [CrossRef] [PubMed]
- Kartal, D.; Arjmand, H.-A.; Varker, T.; Cowlishaw, S.; O’Donnell, M.; Phelps, A.; Howard, A.; Hopwood, M.; McFarlane, A.; Bryant, R.A.; et al. Cross-lagged relationships between insomnia and posttraumatic stress disorder in treatment-receiving veterans. Behav. Ther. 2021, 52, 982–994. [Google Scholar] [CrossRef] [PubMed]
- Colvonen, P.J.; Straus, L.D.; Drummond, S.P.; Angkaw, A.C.; Norman, S.B. Examining sleep over time in a randomized control trial comparing two integrated PTSD and alcohol use disorder treatments. Drug Alcohol Depend. 2020, 209, 107905. [Google Scholar] [CrossRef] [PubMed]
- Edinger, J.D.; Arnedt, J.T.; Bertisch, S.M.; Carney, C.E.; Harrington, J.J.; Lichstein, K.L.; Sateia, M.J.; Troxel, W.M.; Zhou, E.S.; Kazmi, M.U.; et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: An American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J. Clin. Sleep Med. 2021, 17, 263–298. [Google Scholar] [CrossRef]
- Breslau, N.; Roth, T.; Burduvali, E.; Kapke, A.; Schultz, L.; Roehrs, T. Sleep in lifetime posttraumatic stress disorder: A community-based polysomnographic study. Arch. Gen. Psychiatry 2004, 61, 508–516. [Google Scholar] [CrossRef]
- Tempesta, D.; Curcio, G.; De Gennaro, L.; Ferrara, M. Long-term impact of earthquakes on sleep quality. PLoS ONE 2013, 8, e55936. [Google Scholar] [CrossRef]
- Koopman, C.; Classen, C.; Spiegel, D. Dissociative responses in the immediate aftermath of the Oakland/Berkeley firestorm. J. Trauma Stress 1996, 9, 521–540. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Wang, Y.; Tang, W. Risk Factors of Post-traumatic Stress and Depressive Disorders in Longmenshan Adolescents After the 2013 Lushan Earthquake. Community Ment. Health J. 2018, 55, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Geng, F.; Fan, F.; Mo, L.; Simandl, I.; Liu, X. Sleep problems among adolescent survivors following the 2008 wenchuan earthquake in China. J. Clin. Psychiatry 2013, 74, 67–74. [Google Scholar] [CrossRef]
- Thordardottir, E.B.; Gudmundsdottir, H.; Gudmundsdottir, B.; Hrólfsdóttir, A.M.; Aspelund, T.; Hauksdóttir, A. Development and predictors of psychological outcomes following the 2008 earthquake in Iceland: A longitudinal cohort study. Scand. J. Public Health 2019, 47, 269–279. [Google Scholar] [CrossRef]
- Bryant, R.A.; Gibbs, L.; Gallagher, H.C.; Pattison, P.; Lusher, D.; MacDougall, C.; Harms, L.; Block, K.; Sinnott, V.; Ireton, G.; et al. Longitudinal study of changing psychological outcomes following the Victorian black Saturday bushfires. Aust. N. Z. J. Psychiatry 2018, 52, 542–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Database | Keywords |
|---|---|
| EBSCO | (sleep-wake disorder * OR insomnia OR insomniac OR delayed sleep phase disorder * OR sleep apnea OR sleep apnoea OR parasomnia sleep deprivation OR sleep paralysis OR night sweats OR REM sleep disorder * OR excessive sleep OR sleep walking OR hypersomnia OR circadian rhythm sleep disorder OR narcolepsy OR RLS OR restless leg syndrome OR REM sleep behaviour disorder * OR REM sleep behavior disorder * OR night terrors OR bruxism OR sleep movement disorder * OR sleep related breathing disorder * OR sleep onset OR sleep maintenance OR non-24 h sleep wake disorder OR nightmare OR nightmares) AND (bushfires OR wildfires OR wildland fires OR forest fires OR brushfires) |
| PsychINFO | |
| Medline, CINAHL | |
| Complete | |
| EMBASE | |
| PubMed | |
| Cochrane Library | |
| Scopus | ((bushfires OR wildfires OR wildland fires AND fires OR brushfires) AND (sleep AND disorders OR insomnia OR nightmares)) |
| SpringerLink | Bushfires AND wildfires AND sleep disorders AND sleep difficulties AND PTSD |
| Authors | Country | Period Following the Fires | Sample Size | Measures of Sleep | Summary of Findings |
|---|---|---|---|---|---|
| Belleville et al., 2019 [40] | Canada | Three months after the 2016 wildfires in Fort McMurray | 379 adult evacuees (subsample of 55 adult completed diagnostic interview) | CAPS #E6 ISI PSQI-A PSQI | 60% of the sample had a provisional diagnosis of PTSD. Repeated disturbing memories were reported by 77.4% [95% CI: 72.90–81.35] of their sample, 76.7% [95% CI: 72.13–80.65] reported feeling upset when reminded of the stressful experience and 72.5% [95% CI: 67.78–76.75] reported trouble falling or staying asleep. In a subsample of 55 individuals, 29.1% [95% CI: 18.77–42.14] met the clinical criteria for PTSD with 43.6% [95% CI: 31.38–56.73] of the sample receiving diagnosis of insomnia. |
| Jones et al. [41] | USA | Six weeks following the 1990 Wildfires Southern California | 13 children in the High Loss group HL (M = 9.1 years) 9 children in the Low Loss group LL (M = 9.8 years) | Items derived from the Diagnostic Interview for Children and Adolescents | The measure of PTSD showed the following: item, “dreaming about it repeatedly” (HL 46.2% VS. 33.3%LL). Item, “I had trouble falling asleep/staying asleep” (HL 69.2% VS. 33.3% LL). Impact of Event Scale (IES) was administered a month following the first measurement. The two groups reported the following: item, I “had trouble falling asleep or staying asleep because of a picture or a thought about it that came into my mind” (HL 84.6% VS 44.4% LL). Item, “I had a dream about it” (HL 53.8% vs. 55.6% LL). |
| Krakow et al. [42] | New Mexico | Six to ten months following the 2000 Cerro Grande Fire | 78 adult survivors of the fire | SMH SDBDC Autoset Portable II DDNSI FOSQ global ISI | Most participants, 98.7%, had psychophysiological insomnia, 94.8% of participants had presumptive sleep disordered breathing and 33.3% had chronic nightmare disorder. The insomnia symptoms were in the moderate to severe range. Sleep quality was rated fair to poor by those who suffered from insomnia. 92% of the sample reported morning dry mouth, morning headache. Nocturia was reported by 86% of the sample. Dry mouth upon awakening was reported by 51%. Morning headache was reported by 29%. Obstructive sleep apnoea was reported by 41% and 54% reported predominantly upper airway resistance 31% of the sample presented with classic snoring and obstructive sleep apnoea, and 69% presented with atypical symptom. |
| Psarros et al. [43] | Greece | One month following the fires of August 2007 | 92 adult survivors of the fires | AIS | 63.0% [95% CI: 53.0–73.1%] of the sample reported symptoms of insomnia, with 57.6% of the sample reported awakenings during the night followed by 34.8% of the sample reporting delayed sleep induction Nightmares were found to be significantly different, p = 0.002, between those with PTSD 46.5% and those without PTSD 12.3%. |
| Silveira et al. [44] | USA | Six months post the 2018 Camp fire California | 725 adult residents affected by the fires | PROMIS | Scores on the PCL-5 Post-Traumatic Stress Disorder were significantly higher in directly exposed individuals (n = 124 not exposed, n = 201 indirectly exposed, n = 147 directly exposed) with B regression weight reported to be (−3.88, 1.95 and 9.54, respectively) PTSD/PCL-5 scores were positively correlated with childhood trauma. Directly Exposes Sleep Quality (PROMIS) < indirectly Exposed < Nonexposed (p < 0.001) Higher sleep disturbance (PROMIS) scores predicted higher PCL-5 scores. |
| JBI Checklist Appraisal Tool | Included Studies | ||||
|---|---|---|---|---|---|
| Belleville et al. [40] | Jones et al. [41] | Krakow et al. [42] | Psarros et al. [43] | Silveira et al., 2021 [44] | |
| Was the sample frame appropriate to address the target population? | Yes | Yes | Yes | Yes | Yes |
| Were study participants sampled in an appropriate way? | Yes | Yes | Yes | Yes | Yes |
| Was the sample size adequate? | Yes | No | Yes | Yes | Yes |
| Were the study subjects and the setting described in detail? | Yes | Yes | Yes | Yes | Yes |
| Was the data analysis conducted with sufficient coverage of the identified sample? | Yes | Yes | Yes | Yes | Yes |
| Were valid methods used for the identification of the condition? | Yes | No | Yes | Yes | No |
| Was the condition measured in a standard, reliable way for all participants? | Yes | No | Yes | Unclear | Yes |
| Was there appropriate statistical analysis? | Yes | Yes | Yes | Yes | Yes |
| Was the response rate adequate, and if not, was the low response rate managed appropriately? | Yes | Yes | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isaac, F.; Toukhsati, S.R.; Di Benedetto, M.; Kennedy, G.A. A Systematic Review of the Impact of Wildfires on Sleep Disturbances. Int. J. Environ. Res. Public Health 2021, 18, 10152. https://doi.org/10.3390/ijerph181910152
Isaac F, Toukhsati SR, Di Benedetto M, Kennedy GA. A Systematic Review of the Impact of Wildfires on Sleep Disturbances. International Journal of Environmental Research and Public Health. 2021; 18(19):10152. https://doi.org/10.3390/ijerph181910152
Chicago/Turabian StyleIsaac, Fadia, Samia R. Toukhsati, Mirella Di Benedetto, and Gerard A. Kennedy. 2021. "A Systematic Review of the Impact of Wildfires on Sleep Disturbances" International Journal of Environmental Research and Public Health 18, no. 19: 10152. https://doi.org/10.3390/ijerph181910152
APA StyleIsaac, F., Toukhsati, S. R., Di Benedetto, M., & Kennedy, G. A. (2021). A Systematic Review of the Impact of Wildfires on Sleep Disturbances. International Journal of Environmental Research and Public Health, 18(19), 10152. https://doi.org/10.3390/ijerph181910152