
Kidcope and the COVID-19 Pandemic: Understanding High School Students’ Coping and Emotional Well-Being




Abstract
:1. Introduction
1.1. COVID-19 Pandemic and Youth Emotional Well-Being
1.2. Coping and Disasters
1.3. Study Hypothesis
2. Methods
2.1. Setting
2.2. Measures
3. Analyses
4. Results
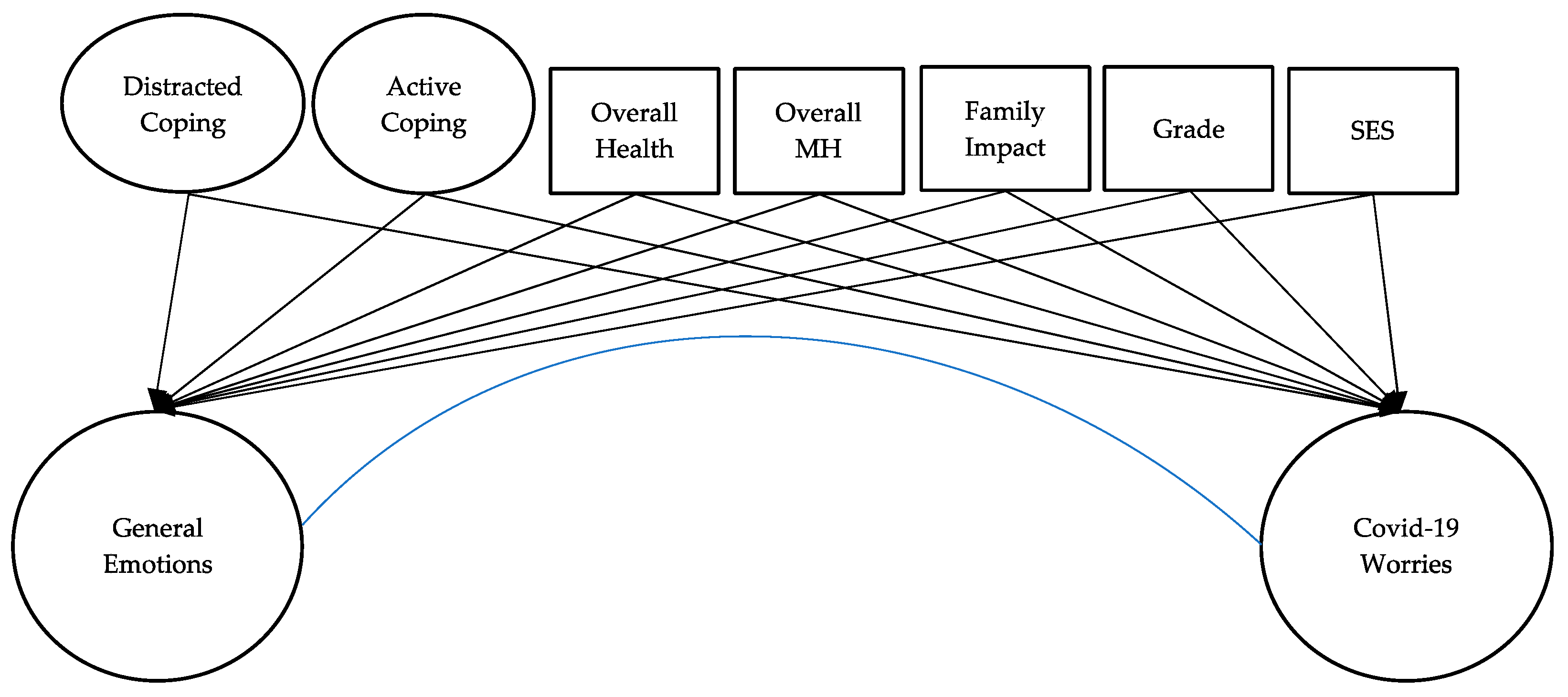
SEM Model
5. Discussion
5.1. Implications
5.2. Limitations and Directions for Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). COVID-10 Death Data and Resources. 2021. Available online: https://www.cdc.gov/nchs/nvss/covid-19.htm (accessed on 15 June 2021).
- Naja, M.; Wedderburn, L.; Ciurtin, C. COVID-19 infection in children and adolescents. Br. J. Hosp. Med. 2020, 81, 1–10. [Google Scholar] [CrossRef]
- Witt, A.; Ordóñez, A.; Martin, A.; Vitiello, B.; Fegert, J.M. Child and adolescent mental health service provision and research during the COVID-19 pandemic: Challenges, opportunities, and a call for submissions. Child Adolesc. Psychiatry Ment. Health 2020, 14, 1–4. [Google Scholar] [CrossRef]
- Golberstein, E.; Wen, H.; Miller, B.F. Coronavirus disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatr. 2020, 174, 819–820. [Google Scholar] [CrossRef] [Green Version]
- Duan, L.; Shao, X.; Wang, Y.; Huang, Y.; Miao, J.; Yang, X.; Zhu, G. An investigation of mental health status of children and adolescents in china during the outbreak of COVID-19. J. Affect. Disord. 2020, 275, 112–118. [Google Scholar] [CrossRef]
- Nearchou, F.; Flinn, C.; Niland, R.; Subramaniam, S.S.; Hennessy, E. Exploring the Impact of COVID-19 on Mental Health Outcomes in Children and Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 8479. [Google Scholar] [CrossRef] [PubMed]
- Octavius, G.S.; Silviani, F.R.; Lesmandjaja, A.; Juliansen, A. Impact of COVID-19 on adolescents’ mental health: A systematic review. Middle East Curr. Psychiatry 2020, 27, 1–8. [Google Scholar] [CrossRef]
- Shen, K.; China National Clinical Research Center for Respiratory Diseases; Yang, Y.; Wang, T.; Zhao, D.; Jiang, Y.; Jin, R.; Zheng, Y.; Xu, B.; Xie, Z.; et al. Diagnosis, treatment, and prevention of 2019 novel coronavirus infection in children: Experts’ consensus statement. World J. Pediatr. 2020, 16, 223–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caouette, J.; Guyer, A.E. Gaining insight into adolescent vulnerability for social anxiety from developmental cognitive neuroscience. Dev. Cogn. Neurosci. 2014, 8, 65–76. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.; He, M.; Herrenkohl, T.I.; Catalano, R.F.; Toumbourou, J. Multiple Identification and Risks: Examination of Peer Factors Across Multiracial and Single-Race Youth. J. Youth Adolesc. 2012, 41, 847–862. [Google Scholar] [CrossRef] [Green Version]
- Sanders, J.; Munford, R. Youth-centred practice: Positive youth development practices and pathways to better outcomes for vulnerable youth. Child. Youth Serv. Rev. 2014, 46, 160–167. [Google Scholar] [CrossRef]
- Pigaiani, Y.; Zoccante, L.; Zocca, A.; Arzenton, A.; Menegolli, M.; Fadel, S.; Ruggeri, M.; Colizzi, M. Adolescent Lifestyle Behaviors, Coping Strategies and Subjective Wellbeing during the COVID-19 Pandemic: An Online Student Survey. Health 2020, 8, 472. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Xue, Q.; Zhou, Y.; Zhu, K.; Liu, Q.; Zhang, J.; Song, R. Mental Health Status Among Children in Home Confinement During the Coronavirus Disease 2019 Outbreak in Hubei Province, China. JAMA Pediatrics 2020, 174, 898. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.-J.; Zhang, L.-G.; Wang, L.-L.; Guo, Z.-C.; Wang, J.-Q.; Chen, J.-C.; Liu, M.; Chen, X.; Chen, J.-X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef]
- De Miranda, D.M.; da Silva Athanasio, B.; de Sena Oliveira, A.C.; Silva, A.C.S. How is COVID-19 pandemic impacting mental health of children and adolescents? Int. J. Disaster Risk Reduct. 2020, 51, 101845. [Google Scholar] [CrossRef] [PubMed]
- Douglas, P.K.; Douglas, D.B.; Harrigan, D.C.; Douglas, K.M. Preparing for pandemic influenza and its aftermath: Mental health issues considered. Int. J. Emerg. Ment. Health Hum. Resil. 2009, 11, 137. [Google Scholar]
- Papadatou, D.; Giannopoulou, I.; Bitsakou, P.; Bellali, T.; Talias, M.A.; Tselepi, K. Adolescents’ reactions after a wildfire disaster in Greece. J. Trauma. Stress 2012, 25, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Pfefferbaum, B.; Noffsinger, M.A.; Wind, L.H.; Allen, J.R. Children’s Coping in the Context of Disasters and Terrorism. J. Loss Trauma 2014, 19, 78–97. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wang, L.; Zhang, X.-L.; Shi, J.-N. Understanding the Impact of Trauma Exposure on Posttraumatic Stress Symptomatology: A Structural Equation Modeling Approach. J. Loss Trauma 2012, 17, 98–110. [Google Scholar] [CrossRef]
- Du, B.; Ma, X.; Ou, X.; Jin, Y.; Ren, P.; Li, J. The prevalence of posttraumatic stress in adolescents eight years after the Wenchuan earthquake. Psychiatry Res. 2018, 262, 262–269. [Google Scholar] [CrossRef]
- Kilmer, R.P.; Gil-Rivas, V. Exploring Posttraumatic Growth in Children Impacted by Hurricane Katrina: Correlates of the Phenomenon and Developmental Considerations. Child Dev. 2010, 81, 1211–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, L.; Ren, H.; Cao, R.; Hu, Y.; Qin, Z.; Li, C.; Mei, S. The Effect of COVID-19 on Youth Mental Health. Psychiatr. Q. 2020, 91, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Álvarez, B.; López-Romero, L.; Isdahl-Troye, A.; Gómez-Fraguela, J.A.; Romero, E. Children coping, contextual risk and their interplay during the COVID-19 pandemic: A Spanish case. Front. Psychol. 2020, 11, 3427. [Google Scholar] [CrossRef]
- DiGangi, J.A.; Gomez, D.; Mendoza, L.; Jason, L.A.; Keys, C.B.; Koenen, K.C. Pretrauma risk factors for posttraumatic stress disorder: A systematic review of the literature. Clin. Psychol. Rev. 2013, 33, 728–744. [Google Scholar] [CrossRef] [PubMed]
- Tol, W.A.; Song, S.; Jordans, M.J. Annual research review: Resilience and mental health in children and adolescents living in areas of armed conflict–a systematic review of findings in low-and middle-income countries. J. Child Psychol. Psychiatry 2013, 54, 445–460. [Google Scholar] [CrossRef]
- Spirito, A.; Stark, L.J.; Williams, C. Development of a Brief Coping Checklist for Use with Pediatric Populations. J. Pediatr. Psychol. 1988, 13, 555–574. [Google Scholar] [CrossRef]
- Vigna, J.F.; Hernandez, B.C.; Kelley, M.L.; Gresham, F.M. Coping Behavior in Hurricane-Affected African American Youth: Psychometric Properties of the Kidcope. J. Black Psychol. 2009, 36, 98–121. [Google Scholar] [CrossRef]
- Clavé, S.; Tsimaratos, M.; Boucekine, M.; Ranchin, B.; Salomon, R.; Dunand, O.; Garnier, A.; Lahoche, A.; Fila, M.; Roussey, G.; et al. Quality of life in adolescents with chronic kidney disease who initiate haemodialysis treatment. BMC Nephrol. 2019, 20, 163. [Google Scholar] [CrossRef]
- Fernando, G.A.; Berger, D.E. The role of religion in youth exposed to disasters in Sri Lanka. J. Prev. Interv. Community 2017, 45, 238–249. [Google Scholar] [CrossRef]
- Holen, S.; Waaktaar, T.; Lervåg, A.; Ystgaard, M. The effectiveness of a universal school-based programme on coping and mental health: A randomised, controlled study of Zippy’s Friends. Educ. Psychol. 2012, 32, 657–677. [Google Scholar] [CrossRef]
- La Greca, A.M.; Lai, B.; Joormann, J.; Auslander, B.B.; Short, M.A. Children’s risk and resilience following a natural disaster: Genetic vulnerability, posttraumatic stress, and depression. J. Affect. Disord. 2013, 151, 860–867. [Google Scholar] [CrossRef]
- Donaldson, D.; Prinstein, M.J.; Danovsky, M.; Spirito, A. Patterns of children’s coping with life stress: Implications for clinicians. Am. J. Orthopsychiatry 2000, 70, 351–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmose, M.; Duch, C.; Elklit, A. Children’s coping styles and trauma symptoms after an explosion disaster. Scand. J. Child Adolesc. Psychiatry Psychol. 2016, 4, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Bedel, A.; Işik, E.; Hamarta, E. Psychometric Properties of the KIDCOPE in Turkish Adolescents. Egit. Bilim 2014, 39, 227–235. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows, Version 27.0; IBM: Armonk, NY, USA, 2020. [Google Scholar]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bowen, N.K.; Guo, S. Structural Equation Modeling; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with EQS and EQS/Windows: Basic Concepts, Applications, and Programming; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models, 1st ed.; Bollen, K.A., Long, J.S., Eds.; Sage Focus Editions: Newbury Park, CA, USA, 1993; pp. 136–162. ISBN 978-0803945074. [Google Scholar]
- Lorenzo, N.E.; Zeytinoglu, S.; Morales, S.; Listokin, J.; Almas, A.N.; Degnan, K.A.; Henderson, H.; Chronis-Tuscano, A.; Fox, N.A. Transactional Associations Between Parent and Late Adolescent Internalizing Symptoms During the COVID-19 Pandemic: The Moderating Role of Avoidant Coping. J. Youth Adolesc. 2021, 50, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.-T.; Del Toro, J.; Scanlon, C.L.; Schall, J.D.; Zhang, A.L.; Belmont, A.M.; Voltin, S.E.; Plevniak, K.A. The roles of stress, coping, and parental support in adolescent psychological well-being in the context of COVID-19: A daily-diary study. J. Affect. Disord. 2021, 294, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Li, M.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z.; Xiong, Z. Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry 2020, 20, 426. [Google Scholar] [CrossRef]
- Zhang, C.; Ye, M.; Fu, Y.; Yang, M.; Luo, F.; Yuan, J.; Tao, Q. The Psychological Impact of the COVID-19 Pandemic on Teenagers in China. J. Adolesc. Health 2020, 67, 747–755. [Google Scholar] [CrossRef]
- Zimmer-Gembeck, M.J.; Skinner, E.A. The Development of Coping: Implications for Psychopathology and Resilience. Dev. Psychopathol. 2016, 1–61. [Google Scholar] [CrossRef]
- Fear, J.M.; Champion, J.E.; Reeslund, K.L.; Forehand, R.; Colletti, C.; Roberts, L.; Compas, B.E. Parental depression and interparental conflict: Children and adolescents’ self-blame and coping responses. J. Fam. Psychol. 2009, 23, 762–766. [Google Scholar] [CrossRef] [Green Version]
- Orgilés, M.; Morales, A.; Delvecchio, E.; Francisco, R.; Mazzeschi, C.; Pedro, M.; Espada, J.P. Coping Behaviors and Psychological Disturbances in Youth Affected by the COVID-19 Health Crisis. Front. Psychol. 2021, 12, 565657. [Google Scholar] [CrossRef]
- De Vaus, J.; Hornsey, M.; Kuppens, P.; Bastian, B. Exploring the East-West Divide in Prevalence of Affective Disorder: A Case for Cultural Differences in Coping with Negative Emotion. Pers. Soc. Psychol. Rev. 2017, 22, 285–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bibbins-Domingo, K. This Time Must Be Different: Disparities During the COVID-19 Pandemic. Ann. Intern. Med. 2020, 173, 233–234. [Google Scholar] [CrossRef]
- Chowkwanyun, M.; Reed, A.L. Racial Health Disparities and COVID-19—Caution and Context. N. Engl. J. Med. 2020, 383, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Montenovo, L.; Jiang, X.; Rojas, F.L.; Schmutte, I.; Simon, K.; Weinberg, B.; Wing, C. Determinants of Disparities in COVID-19 Job Losses; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Marques, S.S.; Braidwood, R. Impact of the Coronavirus Lockdown on Older Adolescents Engaged in a School-Based Stress Management Program: Changes in Mental Health, Sleep, Social Support, and Routines. Child. Sch. 2021, cdab006. [Google Scholar] [CrossRef]
- Shalaby, R.; Vuong, W.; Hrabok, M.; Gusnowski, A.; Mrklas, K.; Li, D.; Snaterse, M.; Surood, S.; Cao, B.; Li, X.-M.; et al. Gender Differences in Satisfaction with a Text Messaging Program (Text4Hope) and Anticipated Receptivity to Technology-Based Health Support During the COVID-19 Pandemic: Cross-sectional Survey Study. JMIR mHealth uHealth 2021, 9, e24184. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, S.; Stoyanov, S.; Pirkis, J.; Kõlves, K. Use of Kids Helpline by Children and Young People in Australia During the COVID-19 Pandemic. J. Adolesc. Health 2021, 68, 1067–1074. [Google Scholar] [CrossRef]
- Alavi, M.; Visentin, D.C.; Thapa, D.K.; Hunt, G.E.; Watson, R.; Cleary, M. Chi-square for model fit in confirmatory factor analysis. J. Adv. Nurs. 2020, 76, 2209–2211. [Google Scholar] [CrossRef] [PubMed]
- Powell, T.; Wegmann, K.; Backode, E. Coping and Post-Traumatic Stress in Children and Adolescents after an Acute Onset Disaster: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4865. [Google Scholar] [CrossRef]


{kind=link}
| N (%) | |
|---|---|
| Grade | |
| 9th Grade | 17 (11.6) |
| 10th Grade | 51 (32.2) |
| 11th Grade | 77 (53.1) |
| Gender | |
| Female | 113 (77.3) |
| Male | 33 (22.6) |
| Received Financial Assistance | |
| Yes | 25 (17.1) |
| No | 116 (79.5) |
| Family Impact of COVID-19 | |
| Fallen physically ill | 8 (4.3) |
| Hospitalized | 1 (0.5) |
| Put into self-quarantine with symptoms | 10 (5.4) |
| Put into self-quarantine without symptoms | 41 (21.9) |
| Lost or been laid off from job | 13 (7.0) |
| Reduced ability to earn money | 36 (19.3) |
| Passed away | 1 (0.5) |
| None of the above | 77 (41.2) |
| M (SD) | |
| COVID Worries | |
| Being affected | 2.15 (0.99) |
| Friends or family being affected | 2.75 (1.18) |
| Physical health influenced by COVID-19 | 1.92 (1.03) |
| Mental health influenced by COVID-19 | 2.88 (1.38) |
| General Emotional Distress | |
| How worried were you generally | 2.28 (0.98) |
| How happy verses sad were you | 3.07 (0.99) |
| How much you enjoy your usual activities | 3.44 (0.97) |
| How relaxed versus anxious were you | 2.98 (1.18) |
| How fidgety or restless were you | 2.54 (1.19) |
| How fatigued or tired were you | 2.56 (1.24) |
| How well you are able to concentrate or focus | 3.38 (1.42) |
| How irritable or easily angered were you | 2.79 (1.26) |
| How lonely were you | 2.69 (1.16) |
| How often did you have negative thoughts | 2.88 (1.26) |
| Mental Health Prior to COVID-19 | 2.85 (1.19) |
| Overall Physical health | 2.27 (0.96) |
| Used Strategy | Effectiveness | |
|---|---|---|
| N (%) | M (SD) | |
| Disengagement Coping | ||
| 1. Tried to forget about the pandemic | 46 (31.7) | 1.85 (0.69) |
| 2. Did something to forget it like watch TV/play video games | 76 (52.4) | 2.28 (0.64) |
| 3. Kept quiet about the pandemic | 29 (20.0) | 1.78 (0.77) |
| 4. Did nothing | 45 (31.0) | 1.70 (0.77) |
| Active Coping | ||
| 5. Tried to fix problem by thinking of answers | 12 (8.3) | 1.63 (0.79) |
| 6. Address pandemic by talking to someone | 36 (24.8) | 1.88 (0.70) |
| 7. Tried to calm self-down | 68 (46.9) | 2.11 (0.71) |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Disengagement Coping | |||||||||
| 1. Coping: tried to forget | – | ||||||||
| 2. Coping: watch TV | 0.31 ** | – | |||||||
| 3. Coping: kept quiet | 0.23 * | 0.16 | – | ||||||
| 4. Coping: did nothing | 0.18 | 0.17 | 0.05 | – | |||||
| Active Coping | |||||||||
| 5. Coping: fix problem | 0.07 | −0.10 | −0.26 * | −0.17 | – | ||||
| 6. Coping: talk to someone | −0.02 | 0.03 | −0.07 | −0.27 * | 0.25 * | – | |||
| 7. Coping: calm self | −0.03 | 0.25 * | −0.20 | −0.14 | 0.23 * | 0.27 ** | – | ||
| Mental Health | |||||||||
| 8. COVID worries | −0.08 | −0.07 | 0.14 | −0.02 | −0.06 | −0.26 * | −0.40 ** | – | |
| 9. General emotional distress | −0.13 | −0.13 | 0.06 | −0.02 | −0.07 | −0.29 * | −0.31 ** | 0.59 *** | – |
| Main Predictors | Outcomes | |
|---|---|---|
| General Emotional Distress | COVID-19 Worries | |
| Active coping | 0.054 (0.070) | 0.115 (0.061) |
| Disengagement coping | −0.442 * (−0.451) | −0.777 † (−0.322) |
| Model Fit Indexes | ||
| Chi-Square Test | p < 0.05 | |
| RMSEA | 0.062 | |
| CFI | 0.855 | |
| TLI | 0.827 | |
| SRMR | 0.096 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, W.-J.; Powell, T.; Tan, K.; Chen, J.-H. Kidcope and the COVID-19 Pandemic: Understanding High School Students’ Coping and Emotional Well-Being. Int. J. Environ. Res. Public Health 2021, 18, 10207. https://doi.org/10.3390/ijerph181910207
Hsieh W-J, Powell T, Tan K, Chen J-H. Kidcope and the COVID-19 Pandemic: Understanding High School Students’ Coping and Emotional Well-Being. International Journal of Environmental Research and Public Health. 2021; 18(19):10207. https://doi.org/10.3390/ijerph181910207
Chicago/Turabian StyleHsieh, Wan-Jung, Tara Powell, Kevin Tan, and Jun-Hong Chen. 2021. "Kidcope and the COVID-19 Pandemic: Understanding High School Students’ Coping and Emotional Well-Being" International Journal of Environmental Research and Public Health 18, no. 19: 10207. https://doi.org/10.3390/ijerph181910207
APA StyleHsieh, W. -J., Powell, T., Tan, K., & Chen, J. -H. (2021). Kidcope and the COVID-19 Pandemic: Understanding High School Students’ Coping and Emotional Well-Being. International Journal of Environmental Research and Public Health, 18(19), 10207. https://doi.org/10.3390/ijerph181910207