
A Study on the Reliability and Validity of the Korean Health Literacy Instrument for Late School-Aged Children


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants and Setting
2.3. Measurement
2.3.1. Selection of Constituent Factors
2.3.2. Development of a Preliminary Tool
2.3.3. Expert Validity Verification
2.4. Ethical Consideration
2.5. Data Collection
2.6. Data Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Validity
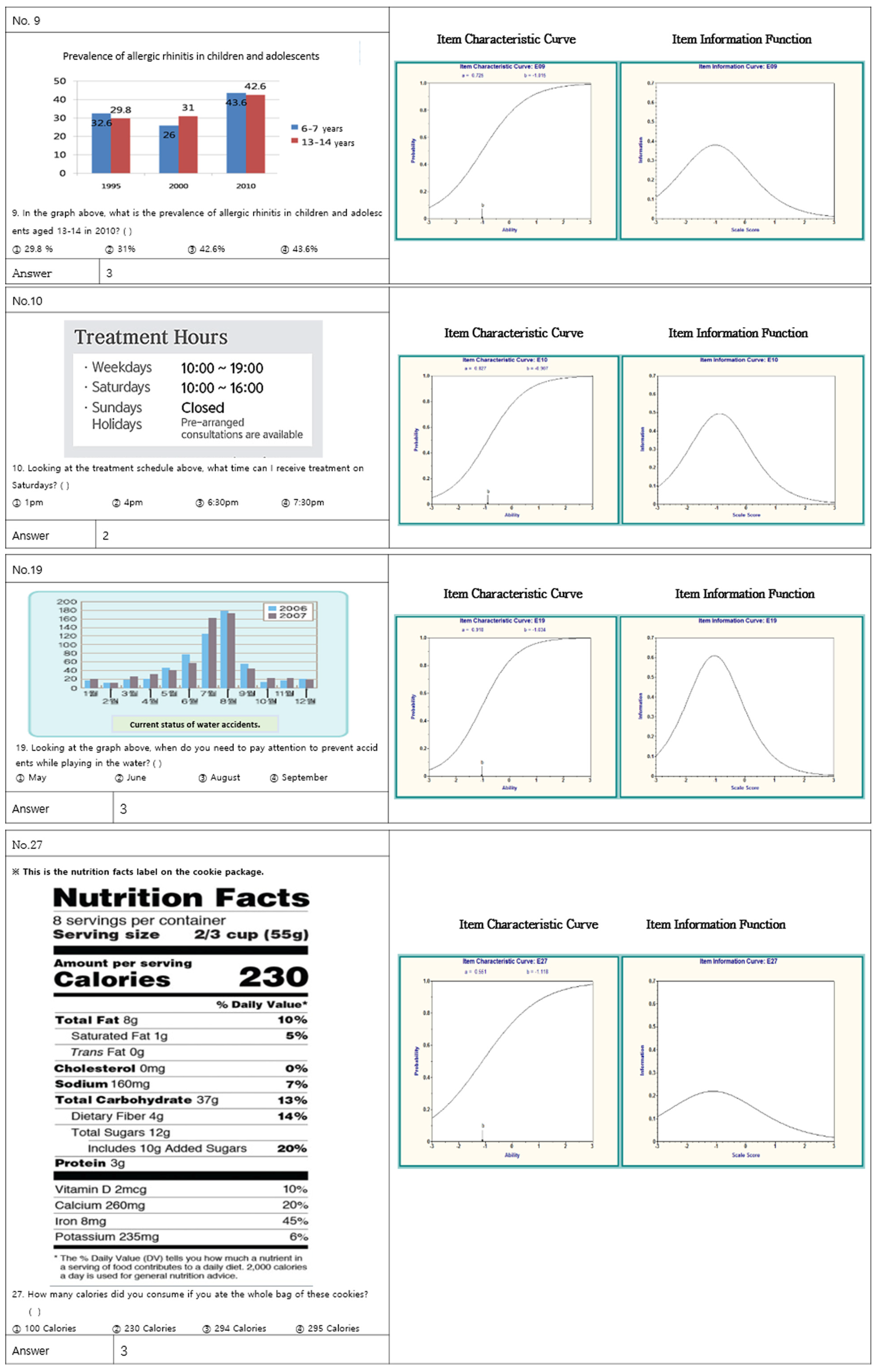
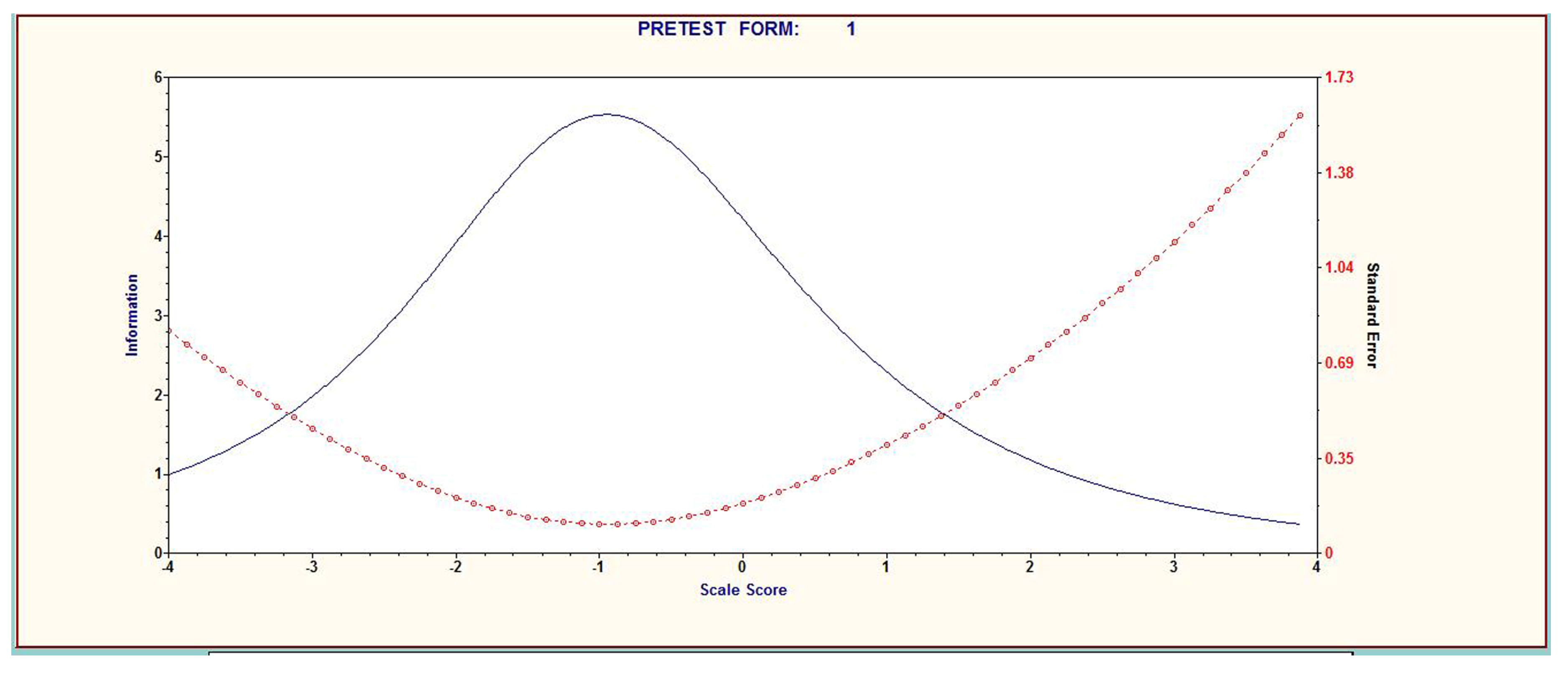
3.2.1. Item Analysis
3.2.2. Construct Validity
3.2.3. Criterion-Related Validity
3.3. Reliability
3.4. Final Item Selection
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Shanghai declaration on promoting health in the 2030 Agenda for Sustainable Development. Health Promot. Int. 2017, 32, 7–8. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health and Welfare, Korea Institute for Healthcare Accreditation. Korea Patient Safety Incident Report. 2018. Available online: https://www.kops.or.kr/portal/board/reference/boardDetail.do?bbsId=reference&nttNo=11544070324902 (accessed on 28 May 2020).
- US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Health Communication and Health Information Technology. Available online: http://www.healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicId=18 (accessed on 4 February 2014).
- US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. National Action Plan to Improve Health Literacy. Available online: http://www.health.gov/communication/HLActionPlan/pdf/Health_Literacy_Action_Plan.pdf (accessed on 4 February 2014).
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Wolf, M.S.; Gazmararian, J.A.; Baker, D.W. Health Literacy and Health Risk Behaviors Among Older Adults. Am. J. Prev. Med. 2007, 32, 19–24. [Google Scholar] [CrossRef]
- Kang, S.J. Development of the Korean Health Literacy Instrument for Adults. Ph.D. Thesis, Yonsei University, Seoul, Korea, 26 August 2011. [Google Scholar]
- An, J.; Yang, S.J. Development of a Health Literacy Assessment Scale for Asian Immigrant Women in South Korea. J. Korean Acad. Commun. Health Nurs. 2015, 26, 330–341. [Google Scholar] [CrossRef] [Green Version]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.; Pignone, M.; Mockbee, J.; Hale, F.A. Quick Assessment of Literacy in Primary Care: The Newest Vital Sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.W.; Kang, S.J.; Lee, H.J.; Hyun, S.I. Testing health literacy skills in older Korean adults. Patient Educ. Couns. 2009, 75, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Lee, E. The Influence of Functional Literacy on Perceived Health Status in Korean Older Adults. J. Korean Acad. Nurs. 2008, 38, 195–203. [Google Scholar] [CrossRef]
- Manganello, J.A. Health literacy and adolescents: A framework and agenda for future research. Health Educ. Res. 2007, 23, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Armstrong, R.; Waters, E.; Sathish, T.; Alif, S.; Browne, G.R.; Yu, X. Quality of health literacy instruments used in children and adolescents: A systematic review. BMJ Open 2018, 8, e020080. [Google Scholar] [CrossRef] [PubMed]
- Marlow, D.R.; Reading, B.A. Textbook of Pediatric Nursing, 6th ed.; W. B. Saunders: Philadelphia, PA, USA, 1989. [Google Scholar]
- Bang, K.S.; Chae, S.M.; Kim, J.Y.; Kang, H.J. Relationships be-tween body image, self-esteem and family strengths in late school aged children. Korean Parent-Child Health J. 2012, 15, 33–38. [Google Scholar]
- Kang, K.A.; Kim, S.J.; Kim, H.O.; Lee, M.N. Child Adolescence Health Nursing; Goonja Publisher: Seoul, Korea, 2019. [Google Scholar]
- Squiers, L.; Peinado, S.; Berkman, N.; Boudewyns, V.; McCormack, L. The Health Literacy Skills Framework. J. Health Commun. 2012, 17, 30–54. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Liao, L.L.; Shih, S.F.; Chang, T.C.; Chi, H.Y.; Osborne, R.H. Development and implementation of Taiwan’s child health literacy test. Taiwan J. Public Health. 2014, 33, 251–270. [Google Scholar] [CrossRef]
- Schmidt, C.O.; Fahland, R.A.; Franze, M.; Splieth, C.; Thyrian, J.R.; Plachta-Danielzik, S.; Hoffmann, W.; Kohlmann, T. Health-related behaviour, knowledge, attitudes, communication and social status in school children in Eastern Germany. Health Educ. Res. 2010, 25, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Okan, O.; Lopes, E.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L.; et al. Generic health literacy measurement instruments for children and adolescents: A systematic review of the literature. BMC Public Health 2018, 18, 166. [Google Scholar] [CrossRef] [Green Version]
- Hulin, C.L.; Lissak, R.I.; Drasgow, F. Recovery of Two- and Three-Parameter Logistic Item Characteristic Curves: A Monte Carlo Study. Appl. Psychol. Meas. 1982, 6, 249–260. [Google Scholar] [CrossRef] [Green Version]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis; Wiley: Hoboken, NJ, USA, 1992. [Google Scholar]
- Paakkari, L.; Torppa, M.; Mazur, J.; Boberova, Z.; Sudeck, G.; Kalman, M.; Paakkari, O. A Comparative Study on Adolescents’ Health Literacy in Europe: Findings from the HBSC Study. Int. J. Environ. Res. Public Health 2020, 17, 3543. [Google Scholar] [CrossRef]
- Davis, T.C.; Wolf, M.S.; Arnold, C.L.; Byrd, R.S.; Long, S.W.; Springer, T.; Kennen, E.; Bocchini, J.A. Development and Validation of the Rapid Estimate of Adolescent Literacy in Medicine (REALM-Teen): A Tool to Screen Adolescents for Below-Grade Reading in Health Care Settings. Pediatrics 2006, 118, e1707–e1714. [Google Scholar] [CrossRef]
- Tsubakita, T.; Kawazoe, N.; Kasano, E. A New Functional Health Literacy Scale for Japanese Young Adults Based on Item Response Theory. Asia Pac. J. Public Health 2017, 29, 149–158. [Google Scholar] [CrossRef]
- Manganello, J.A.; Colvin, K.F.; Chisolm, D.J.; Arnold, C.; Hancock, J.; Davis, T. Validation of the Rapid Estimate for Adolescent Literacy in Medicine Short Form (REALM-TeenS). Pediatrics 2017, 139, 20163286. [Google Scholar] [CrossRef] [Green Version]
- Lynn, M.R. Determination and Qualification of Content Validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef]
- Seong, T.J. Validity & Reliability; Hak Ji Sa: Seoul, Korea, 2010. [Google Scholar]
- De Vellis, R.F. Scale Development: Theory and Applications, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Seong, T.J. Understanding and Application of Item Response Theory; Kyoyook Book: Paju, Korea, 2009. [Google Scholar]
- Yim, M.K.; Huh, S. Testing Unidimensionality and Goodness-of-fitness for the Application of Item Response Theory to the Korean Medical Licensing Examination. Korean J. Med. Educ. 2007, 19, 163–169. [Google Scholar] [CrossRef]
- Baker, D.W.; Williams, M.V.; Parker, R.; Gazmararian, J.A.; Nurss, J. Development of a brief test to measure functional health literacy. Patient Educ. Couns. 1999, 38, 33–42. [Google Scholar] [CrossRef]
- Parker, R.M.; Baker, D.W.; Williams, M.V. The test of functional health literacy in adults. J. Gen. Intern. Med. 1995, 10, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1978. [Google Scholar]



{kind=link}
{kind=link}
| Domain | Sub Domain | Item | Constituent Factor | I-CVI ¶ | ||
|---|---|---|---|---|---|---|
| Document § | Numbers ‡ | 1st | 2nd | |||
| HDL * | (1) Health terminology (2) Physical activity | Health terminology | √ | 1.0 | 1.0 | |
| Health terminology | √ | 0.7 | 0.8 | |||
| Health terminology | √ | 0.7 | 0.8 | |||
| Ambulatory treatment | √ | 0.8 | 0.8 | |||
| Clinic time table | √ | 0.6 | 0.9 | |||
| Medical department | √ | 1.0 | 1.0 | |||
| Safety accident graph | √ | 0.9 | 0.9 | |||
| Safety accident graph | √ | 0.7 | 0.8 | |||
| Physical activity | √ | 1.0 | 1.0 | |||
| Obesity prevention | √ | 1.0 | 1.0 | |||
| (3) Healthy food (4) Food sanitation (5) Food allergy (6) Healthy eating habits | Food Additives | √ | 0.8 | 0.8 | ||
| Food allergy | √ | 0.9 | 0.9 | |||
| Snack documentation | √ | 0.9 | 0.9 | |||
| Snack documentation | √ | 0.6 | 0.9 | |||
| Food composition table | √ | 0.8 | 0.8 | |||
| Food composition table | √ | 0.8 | 0.8 | |||
| PM ** | (1) Immunology and vaccination (2) Infectious disease (3) Scoliosis (4) Tooth decay prevention and management | Vaccination Precautions | √ | 0.8 | 0.8 | |
| Cough manners | √ | 0.9 | 0.9 | |||
| IDP **** | √ | 1.0 | 1.0 | |||
| Scoliosis prevention | √ | 0.8 | 0.8 | |||
| Disease graph | √ | 1.0 | 1.0 | |||
| Tooth decay graph | √ | 1.0 | 1.0 | |||
| Dental caries description | √ | 0.8 | 0.8 | |||
| DA *** | (1) Appropriate drug use (2) Smoking prevention | Dosage, usage instructions of drug | √ | 0.9 | 0.9 | |
| Concept of drug abuse | √ | 0.9 | 0.9 | |||
| Concept of drug abuse | √ | 0.9 | 0.9 | |||
| Appropriate drug use | √ | 1.0 | 1.0 | |||
| Appropriate drug use | √ | 0.8 | 0.8 | |||
| Understanding non-smoking sign | √ | 1.0 | 1.0 | |||
| Item Contents | Classical Item Response Theory (CTT) | Item Response Theory (IRT) | ||||
|---|---|---|---|---|---|---|
| MFC * | α Value ** | Difficulty | Dis *** | Difficulty | Dis *** | |
| Health terminology | 0.39 | 0.82 | 0.56 | 0.48 | −0.49 | 0.70 |
| Health terminology | 0.39 | 0.82 | 0.55 | 0.56 | −0.39 | 0.72 |
| Health terminology | 0.15 ‡ | 0.86 | ||||
| What you need for hospital care | 0.32 | 0.82 | 0.63 | 0.34 | −0.89 | 0.40 |
| Dosage, usage instructions of drug | 0.57 | 0.82 | 0.61 | 0.49 | −1.03 | 0.27 |
| Reading the disease-specific graphs | 0.49 | 0.81 | 0.66 | 0.35 | −1.05 | 0.72 |
| Concept of drug abuse | 0.21 ‡ | 0.82 | 0.57 | 0.46 | ||
| Concept of drug abuse | 0.22 ‡ | 0.86 | ||||
| Understanding non-smoking sign | 0.34 | 0.81 | 0.62 | 0.56 | −1.02 | 0.73 |
| Understanding Clinic timetable | 0.38 | 0.81 | 0.58 | 0.33 | −0.91 | 0.83 |
| Understanding medical department | 0.32 | 0.82 | 0.70 | 0.57 | −0.76 | 0.67 |
| Reading cavitation related graphs | 0.32 | 0.82 | 0.61 | 0.55 | −1.72 | 0.31 |
| Understanding coughing manners | 0.33 | 0.83 | 0.64 | 0.56 | −0.57 | 0.99 |
| Understanding food additives | 0.33 | 0.81 | 0.76 | 0.21 | −0.69 | 0.98 |
| Scoliosis prevention | 0.41 | 0.84 | 0.60 | 0.46 | −1.02 | 0.90 |
| Reading safety accident graph | 0.40 | 0.81 | 0.75 | 0.26 | −1.03 | 0.87 |
| Vaccination Precautions | 0.41 | 0.83 | 0.57 | 0.64 | −1.36 | 0.08 |
| Appropriate drug use instruction | 0.49 | 0.81 | 0.76 | 0.47 | −0.34 | 0.65 |
| Reading safety accident graph | 0.41 | 0.80 | 0.62 | 0.58 | −1.03 | 0.92 |
| Physical activity | 0.36 | 0.82 | 0.64 | 0.49 | −1.88 | 0.29 |
| Obesity prevention | 0.39 | 0.81 | 0.60 | 0.49 | −0.73 | 0.52 |
| Infectious diseases prevention | 0.39 | 0.81 | 0.62 | 0.43 | −0.55 | 0.51 |
| School meals- food allergy | 0.38 | 0.82 | 0.66 | 0.56 | −0.60 | 0.54 |
| Snack documentation-Expiration date | 0.14 ‡ | 0.86 | ||||
| Snack documentation-Induce allergies | 0.33 | 0.82 | 0.67 | 0.44 | −0.718 | 0.41 |
| Food composition table | 0.46 | 0.82 | 0.62 | 0.45 | −1.561 | 0.21 |
| Food composition table | 0.34 | 0.81 | 0.70 | 0.47 | −1.118 | 0.55 |
| Understanding dental caries instruction | 0.39 | 0.81 | 0.65 | 0.41 | −0.954 | 0.74 |
| Appropriate drug use instruction | 0.39 | 0.81 | 0.64 | 0.46 | −1.179 | 0.50 |
| M ± SD | 0.64 | 0.30 | ||||
| Item Contents | Factor Loading | KR-20 | |
|---|---|---|---|
| Factor 1 | Factor 2 | Reliability Coefficient | |
| Understanding Clinic timetable | 0.71 | 0.38 | |
| Scoliosis Prevention | 0.68 | 0.41 | |
| Understanding non-smoking sign | 0.65 | 0.34 | |
| Understanding dental caries instruction | 0.56 | 0.39 | |
| Understanding food additives | 0.51 | 0.33 | 0.88 |
| Appropriate drug use instruction | 0.50 | 0.43 | |
| Obesity prevention | 0.48 | 0.39 | |
| Vaccination Precautions | 0.47 | 0.41 | |
| Infectious diseases prevention | 0.44 | 0.39 | |
| School meals- food allergy | 0.42 | 0.38 | |
| Reading safety accident graph | 0.41 | 0.72 | |
| Safety accident graph | 0.39 | 0.70 | |
| Reading cavitation related graphs | 0.41 | 0.48 | 0.82 |
| Food composition table | 0.41 | 0.46 | |
| Food composition table | 0.34 | 0.43 | |
| Dosage, usage instructions of drug | 0.38 | 0.40 | |
| Eigen value | 5.79 | 1.99 | 0.85 |
| Factor | χ2 (df) | p | CFI | TLI | RMSEA |
|---|---|---|---|---|---|
| One Factor | 142.02(51) | 0.032 | 0.85 | 0.87 | 0.08 |
| Two Factor | 228.75(63) | 0.002 | 0.96 | 0.95 | 0.06 |
| Three Factor | 77.96(40) | 0.184 | 0.73 | 0.78 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-K.; Kim, E.-G. A Study on the Reliability and Validity of the Korean Health Literacy Instrument for Late School-Aged Children. Int. J. Environ. Res. Public Health 2021, 18, 10304. https://doi.org/10.3390/ijerph181910304
Park S-K, Kim E-G. A Study on the Reliability and Validity of the Korean Health Literacy Instrument for Late School-Aged Children. International Journal of Environmental Research and Public Health. 2021; 18(19):10304. https://doi.org/10.3390/ijerph181910304
Chicago/Turabian StylePark, Sook-Kyoung, and Eun-Gyeong Kim. 2021. "A Study on the Reliability and Validity of the Korean Health Literacy Instrument for Late School-Aged Children" International Journal of Environmental Research and Public Health 18, no. 19: 10304. https://doi.org/10.3390/ijerph181910304
APA StylePark, S. -K., & Kim, E. -G. (2021). A Study on the Reliability and Validity of the Korean Health Literacy Instrument for Late School-Aged Children. International Journal of Environmental Research and Public Health, 18(19), 10304. https://doi.org/10.3390/ijerph181910304