
COVID-19-Associated Mucormycosis (CAM): An Updated Evidence Mapping

 ,
,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. PCC Elements
- (a)
- Participants: patients with confirmed COVID-19 (RT-PCR) and mucormycosis (either histologically or microbiologically confirmed) based on the definition of Centers for Disease Control and Prevention were included in the study. We also included studies with suspected COVID-19 patients (based on the included studies assessment) who had confirmed mucormycosis.
- (b)
- Concept and context: this review included all studies that described the clinical presentation, treatment modalities, and patient outcomes of CAM.
2.1.2. Types of Sources
2.1.3. Exclusion Criteria
- (a)
- Non-English language studies;
- (b)
- studies with no confirmed mucormycosis; and
- (c)
- systematic reviews, narrative reviews, editorials, opinions, and study protocols were excluded.
2.2. Information Sources and Search Strategy
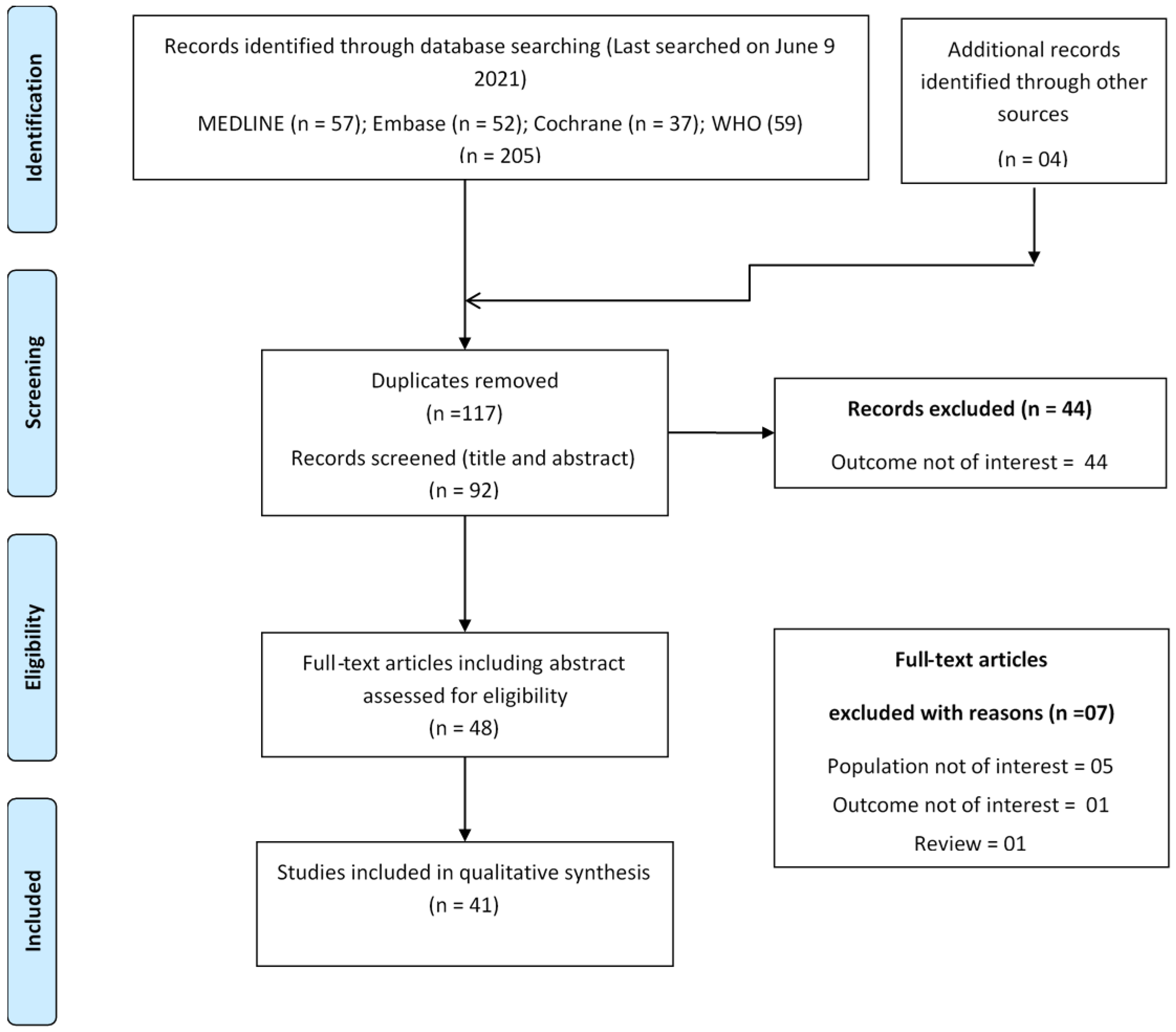
2.3. Selection Process
2.4. Data Extraction
3. Results
3.1. Studies Characteristics
3.2. Clinical Presentation
3.3. Treatment Modalities and Outcomes
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. MEDLINE® ALL <1946 to 8 June 2021> (Ovid)
| # | Search String | No. of Results |
| 1 | exp Coronavirus/ | 77,269 |
| 2 | exp Coronavirus Infections/ | 94,303 |
| 3 | (coronavirus* or corona virus* or OC43 or NL63 or 229E or HKU1 or HCoV* or ncov* or covid* or sars-cov* or sarscov* or Sars-coronavirus* or Severe Acute Respiratory Syndrome Coronavirus* or “Kawasaki like paediatric inflammatory multisystem syndrome” or “Kawasaki like pediatric inflammatory multisystem syndrome” or “PIMS-TS” or “Kawa-COVID-19” or “MIS-C” or “multisystem inflammatory syndrome in children” or pediatric multisystem inflammatory disease).mp. | 159,987 |
| 4 | (or/1–3) and ((20191* or 202*).dp. or 20190101:20301231.(ep).) (147001) | 147,001 |
| 5 | 4 not (SARS or SARS-CoV or MERS or MERS-CoV or Middle East respiratory syndrome or camel * or dromedary* or equine or coronary or coronal or covidence* or covidien or influenza virus or HIV or bovine or calves or TGEV or feline or porcine or BCoV or PED or PEDV or PDCoV or FIPV or FCoV or SADS-CoV or canine or CCov or zoonotic or avian influenza or H1N1 or H5N1 or H5N6 or IBV or murine corona*).mp. | 54,231 |
| 6 | ((pneumonia or covid* or coronavirus* or corona virus* or ncov* or 2019-ncov or sars*).mp. or exp pneumonia/) and Wuhan.mp. | 5278 |
| 7 | (2019-ncov or ncov19 or ncov-19 or 2019-novel CoV or sars-cov2 or sars-cov-2 or sarscov2 or sarscov-2 or SARS-2-nCoV or SARS-2-Cov or SARS-COV-19 or Sars-coronavirus2 or Sars-coronavirus-2 or SARS 2 coronavirus* or Severe Acute Respiratory Syndrome-CoV-2 or SARS-like coronavirus* or coronavirus-19 or covid19 or covid-19 or covid 2019 or ((novel or new or nouveau) adj2 (CoV or nCoV or covid or coronavirus* or corona virus or Pandemi*2)) or ((covid or covid19 or covid-19 or SARS-CoV-2) and pandemic*2) or (coronavirus* and pneumonia)).mp. | 144,923 |
| 8 | (COVID-19 or SARS-CoV-2).rx,px,ox,rn. or (COVID-19 or COVID-19 serotherapy or ORF7b protein, SARS-CoV-2 or ORF6 protein, SARS-CoV-2 or ORF8 protein, SARS-CoV-2 or pediatric multisystem inflammatory disease, COVID-19 related or envelope protein, SARS-CoV-2 or ORF7a protein, SARS-CoV-2 or spike protein, SARS-CoV-2 or ORF3a protein, SARS-CoV-2 or COVID-19 drug treatment or severe acute respiratory syndrome coronavirus 2 or membrane protein, SARS-CoV-2 or ORF1ab polyprotein, SARS-CoV-2 or nucleocapsid protein, Coronavirus or COVID-19 vaccine or COVID-19 diagnostic testing).os,ps,rn,rs. | 8460 |
| 9 | (“32185863” or “32172715” or “32227595” or “32140676” or “32246156” or “32267941” or “32176889” or “32169616” or “32265186” or “32253187” or “32152148” or “32053580” or “32179788” or “32213260” or “32205350” or “32188729” or “32152361” or “32277065” or “32088947” or “32240583” or “31917786” or “32127714” or “32047315” or “32020111” or “32240632” or “32243118” or “32267344” or “32239781” or “32396977” or “32402130” or “32243299” or “32807526” or “32344395” or “32403202” or “32389714” or “32416016” or “32405099” or “32976849” or “32685966” or “33221888” or “32379271” or “32188728” or “32221976” or “32417321” or “32489438” or “32332959” or “32943452” or “32807525” or “32826274” or “32898560” or “32293023” or “33159926” or “32919952” or “32835716” or “32619499” or “32663524” or “32392627” or “32392625” or “33037657” or “32777045” or “32521569” or “32492200” or “32930765” or “33075143” or “32237249” or “32683439” or “32495994” or “32344447” or “32896006” or “32240549” or “32438448” or “32425477” or “32951095” or “32274794” or “32750178” or “32463935” or “32428286” or “32491981” or “32930748” or “32119409” or “32432657” or “33003176” or “32459319” or “32822920” or “32878290” or “32270498” or “32250493” or “32512243” or “32837399” or “32426074” or “32199942” or “32839969” or “32639522” or “33073717” or “32502134” or “32334003” or “32510470” or “32819741” or “32309248” or “32243951” or “32378772” or “32835361” or “32962779” or “32916324” or “32785973” or “32272221” or “32299207” or “33044515” or “33134955” or “32970917” or “32407438” or “32513790” or “32439468” or “33063036” or “33077677” or “32406056” or “32716821” or “32588590” or “32239757” or “32829902” or “32807521” or “32379350” or “33125767” or “32829731” or “32988821” or “32780977” or “32648633” or “32829907” or “32330635” or “32692998” or “33013067” or “33010706” or “32502292” or “32780969” or “32998780” or “32754731” or “32639607” or “32233030” or “32953429” or “32246897” or “32955802” or “32425490” or “32418270” or “32445255” or “32775945” or “32775948” or “32775953” or “32407043”).ui. | 152 |
| 10 | or/5–9 | 147,637 |
| 11 | 10 and 20191201:20301231.(dt). | 145,485 |
| 12 | exp Zygomycosis/ | 4474 |
| 13 | mucormycos#s.mp. | 5053 |
| 14 | Mucormycose.mp. | 98 |
| 15 | mucoromycos#s.mp. | 6 |
| 16 | zygomycos#s.mp. | 1414 |
| 17 | (black fungus or black fungi).mp. | 192 |
| 18 | exp Mucorales/ | 6616 |
| 19 | Mucorales.mp. | 192 |
| 20 | mucoralean.mp. | 70 |
| 21 | Absidia.mp. | 562 |
| 22 | Cunninghamella.mp. | 768 |
| 23 | Mortierella.mp. | 751 |
| 24 | Mucor.mp. | 3382 |
| 25 | Apophysomyces.mp. | 147 |
| 26 | Saksenaea.mp. | 102 |
| 27 | Rhizopus.mp. | 4211 |
| 28 | Rhizomucor.mp. | 691 |
| 29 | Lichtheimia.mp. | 191 |
| 30 | Cokeromyces.mp. | 24 |
| 31 | Actinomucor.mp. | 58 |
| 32 | Syncephalastrum.mp. | 163 |
| 33 | 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 | 14,534 |
| 34 | 11 and 33 | 57 |
| Search was conducted on 9 June 2021 at 4:25 p.m. (CET). | ||
References
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 22 September 2021).
- Challen, R.; Brooks-Pollock, E.; Read, J.M.; Dyson, L.; Tsaneva-Atanasova, K.; Danon, L. Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: Matched cohort study. BMJ 2021, 372, n579. [Google Scholar]
- Vaidyanathan, G. Coronavirus variants are spreading in India—What scientists know so far. Nature 2021, 593, 321–322. [Google Scholar] [CrossRef]
- Miller, I.F.; Becker, A.D.; Grenfell, B.T.; Metcalf, C.J.E. Disease and healthcare burden of COVID-19 in the United States. Nat. Med. 2020, 26, 1212–1217. [Google Scholar] [CrossRef]
- Hussain, S.; Baxi, H.; Jamali, M.C.; Nisar, N.; Hussain, M.S. Burden of diabetes mellitus and its impact on COVID-19 patients: A meta-analysis of real-world evidence. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1595–1602. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Heilbrunn, E.S.; Ba, D.M.; Chinchilli, V.M. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0238215. [Google Scholar] [CrossRef]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.; Sigurslid, H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Liu, J.; Liang, B.; Wang, X.; Wang, H.; Li, W.; Tong, Q.; Yi, J.; Zhao, L.; et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine 2020, 55, 102763. [Google Scholar] [CrossRef]
- Singh, A.K.; Majumdar, S.; Singh, R.; Misra, A. Role of corticosteroid in the management of COVID-19: A systemic review and a Clinician’s perspective. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, A.I.; Singanayagam, A. Immunosuppression for hyperinflammation in COVID-19: A double-edged sword? Lancet 2020, 395, 1111. [Google Scholar] [CrossRef]
- Chen, X.; Liao, B.; Cheng, L.; Peng, X.; Xu, X.; Li, Y.; Hu, T.; Li, J.; Zhou, X.; Ren, B. The microbial co-infection in COVID-19. Appl. Microbiol. Biotechnol. 2020, 1–9. [Google Scholar] [CrossRef]
- Feldman, C.; Anderson, R. The role of co-infections and secondary infections in patients with COVID-19. Pneumonia 2021, 13, 1–15. [Google Scholar] [CrossRef]
- Abdoli, A. Helminths and COVID-19 Co-Infections: A Neglected Critical Challenge. ACS Pharmacol. Transl. Sci. 2020, 3, 1039–1041. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- El-Herte, R.I.; Baban, T.A.; Kanj, S.S. Mucormycosis: A review on environmental fungal spores and seasonal variation of human disease. Adv. Infect. Dis 2012, 2, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.S.; Spellberg, B.; Walsh, T.J.; Kontoyiannis, D.P. Pathogenesis of mucormycosis. Clin. Infect. Dis. 2012, 54, S16–S22. [Google Scholar] [CrossRef] [PubMed]
- Wali, U.; Balkhair, A.; Al-Mujaini, A. Cerebro-rhino orbital mucormycosis: An update. J. Infect. Public Health 2012, 5, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.; Keighley, C.; Wolfe, R.; Lee, W.L.; Slavin, M.; Kong, D.C.; Chen, S.C.-A. The epidemiology and clinical manifestations of mucormycosis: A systematic review and meta-analysis of case reports. Clin. Microbiol. Infect. 2019, 25, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrikkos, G.; Skiada, A.; Lortholary, O.; Roilides, E.; Walsh, T.J.; Kontoyiannis, D.P. Epidemiology and clinical manifestations of mucormycosis. Clin. Infect. Dis. 2012, 54, S23–S34. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Mucormycosis Statistics. Available online: https://www.cdc.gov/fungal/diseases/mucormycosis/statistics.html (accessed on 10 June 2021).
- Kontoyiannis, D.P.; Yang, H.; Song, J.; Kelkar, S.S.; Yang, X.; Azie, N.; Harrington, R.; Fan, A.; Lee, E.; Spalding, J.R. Prevalence, clinical and economic burden of mucormycosis-related hospitalizations in the United States: A retrospective study. BMC Infect. Dis. 2016, 16, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Heimann, S.M.; Vehreschild, M.J.; Cornely, O.A.; Heinz, W.J.; Grüner, B.; Silling, G.; Kessel, J.; Seidel, D.; Vehreschild, J.J. Healthcare burden of probable and proven invasive mucormycosis: A multi-centre cost-of-illness analysis of patients treated in tertiary care hospitals between 2003 and 2016. J. Hosp. Infect. 2019, 101, 339–346. [Google Scholar] [CrossRef]
- ‘Black Fungus’ Declared an Epidemic in 4 States, 1 UT. Available online: http://timesofindia.indiatimes.com/articleshow/82804720.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst (accessed on 10 June 2021).
- Singh, A.K.; Singh, R.; Joshi, S.R.; Misra, A. Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102146. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Singh, B.; Bhadada, S.K.; Banerjee, M.; Bhogal, R.S.; Hage, N.; Kumar, A. COVID-19-associated mucormycosis: An updated systematic review of literature. Mycoses 2021. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Godfrey, C.; McInerney, P.; Soares, C.B.; Khalil, H.; Parker, D. Methodology for JBI scoping reviews. In The Joanna Briggs Institute Reviewers Manual 2015; Joanna Briggs Institute: Adelaide, Australia, 2015; pp. 3–24. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Perters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, S.; Baxi, H.; Riad, A.; Kulgarova, J.; Licenik, R.; Klugar, M. COVID-19 Associated Mucormycosis: Scoping Review Protocol. medRxiv 2021. [Google Scholar] [CrossRef]
- Expert Search Coronavirus (Covid-19) 2019-nCoV on MEDLINE. 2020. Available online: https://tools.ovid.com/ovidtools/expertsearches.html (accessed on 9 June 2021).
- Expert Search COVID-19 Embase 1974 to Present. 2020. Available online: https://tools.ovid.com/coronavirus/ (accessed on 9 June 2021).
- Alekseyev, K.; Didenko, L.; Chaudhry, B. Rhinocerebral mucormycosis and COVID-19 pneumonia. J. Med. Cases 2021, 12, 85. [Google Scholar] [CrossRef]
- Arana, C.; Ramírez, R.E.C.; Xipell, M.; Casals, J.; Moreno, A.; Herrera, S.; Bodro, M.; Cofan, F.; Diekmann, F.; Esforzado, N. Mucormycosis associated with covid19 in two kidney transplant patients. Transpl. Infect. Dis. 2021, 23, e13652. [Google Scholar] [CrossRef]
- Ashour, M.M.; Abdelaziz, T.T.; Ashour, D.M.; Askoura, A.; Saleh, M.I.; Mahmoud, M.S. Imaging spectrum of acute invasive fungal rhino-orbital-cerebral sinusitis in COVID-19 patients: A case series and a review of literature. J. Neuroradiol. 2021, 48, 319–324. [Google Scholar] [CrossRef]
- Bayram, N.; Ozsaygılı, C.; Sav, H.; Tekin, Y.; Gundogan, M.; Pangal, E.; Cicek, A.; Özcan, I. Susceptibility of severe COVID-19 patients to rhino-orbital mucormycosis fungal infection in different clinical manifestations. Jpn. J. Ophthalmol. 2021, 65, 515–525. [Google Scholar] [CrossRef]
- Bellanger, A.-P.; Navellou, J.-C.; Lepiller, Q.; Brion, A.; Brunel, A.-S.; Millon, L.; Berceanu, A. Mixed mold infection with Aspergillus fumigatus and Rhizopus microsporus in a severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) patient. Infect. Dis. Now 2021, 51, 633–635. [Google Scholar]
- Dallalzadeh, L.O.; Ozzello, D.J.; Liu, C.Y.; Kikkawa, D.O.; Korn, B.S. Secondary infection with rhino-orbital cerebral mucormycosis associated with COVID-19. Orbit 2021, 1–4. [Google Scholar] [CrossRef]
- Do Monte Junior, E.S.; Dos Santos, M.E.L.; Ribeiro, I.B.; de Oliveira Luz, G.; Baba, E.R.; Hirsch, B.S.; Funari, M.P.; de Moura, E.G.H. Rare and Fatal Gastrointestinal Mucormycosis (Zygomycosis) in a COVID-19 Patient: A Case Report. Clin. Endosc. 2020, 53, 746–749. [Google Scholar] [CrossRef]
- El-Kholy, N.A.; Abd El-Fattah, A.M.; Khafagy, Y.W. Invasive fungal sinusitis in post COVID-19 patients: A new clinical entity. Laryngoscope 2021. [Google Scholar] [CrossRef]
- Garg, D.; Muthu, V.; Sehgal, I.S.; Ramachandran, R.; Kaur, H.; Bhalla, A.; Puri, G.D.; Chakrabarti, A.; Agarwal, R. Coronavirus disease (Covid-19) associated mucormycosis (CAM): Case report and systematic review of literature. Mycopathologia 2021, 186, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Hanley, B.; Naresh, K.; Roufosse, C.; Nicholson, A.G.; Weir, J.; Cooke, G.S.; Thursz, M.; Manousou, P.; Corbett, R.; Goldin, R.; et al. Histopathological findings and viral tropism in UK patients with severe fatal COVID-19: A post-mortem study. Lancet Microbe 2020, 1, e245–e253. [Google Scholar] [CrossRef]
- Johnson, A.K.; Ghazarian, Z.; Cendrowski, K.D.; Persichino, J.G. Pulmonary aspergillosis and mucormycosis in a patient with COVID-19. Med. Mycol. Case Rep. 2021, 32, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, A.; Jordan, A.; Olewiler, S.; Wehberg, K.; Cortes, M.; Jackson, B.R. A fatal case of Rhizopus azygosporus pneumonia following COVID-19. J. Fungi 2021, 7, 174. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Galougahi, M.; Arastou, S.; Haseli, S. Fulminant mucormycosis complicating coronavirus disease 2019 (COVID-19). Int. Forum Allergy Rhinol. 2021, 11, 1029–1030. [Google Scholar] [CrossRef] [PubMed]
- Khatri, A.; Chang, K.-M.; Berlinrut, I.; Wallach, F. Mucormycosis after Coronavirus disease 2019 infection in a heart transplant recipient—Case report and review of literature. J. Med. Mycol. 2021, 31, 101125. [Google Scholar] [CrossRef]
- Krishna, D.S.; Raj, H.; Kurup, P.; Juneja, M. Maxillofacial Infections in Covid-19 Era—Actuality or the Unforeseen: 2 Case Reports. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–4. [Google Scholar] [CrossRef]
- Krishna, V.; Morjaria, J.; Jalandari, R.; Omar, F.; Kaul, S. Autoptic identification of disseminated mucormycosis in a young male presenting with cerebrovascular event, multi-organ dysfunction and COVID-19 infection. IDCases 2021, 25, e01172. [Google Scholar] [CrossRef]
- Maini, A.; Tomar, G.; Khanna, D.; Kini, Y.; Mehta, H.; Bhagyasree, V. Sino-orbital mucormycosis in a COVID-19 patient: A case report. Int. J. Surg. Case Rep. 2021, 82, 105957. [Google Scholar] [CrossRef]
- Mehta, S.; Pandey, A. Rhino-orbital mucormycosis associated with COVID-19. Cureus 2020, 12, e10726. [Google Scholar] [CrossRef]
- Mekonnen, Z.K.; Ashraf, D.C.; Jankowski, T.; Grob, S.R.; Vagefi, M.R.; Kersten, R.C.; Simko, J.P.; Winn, B.J. Acute invasive rhino-orbital mucormycosis in a patient with COVID-19-associated acute respiratory distress syndrome. Ophthalmic Plast. Reconstr. Surg. 2021, 37, e40. [Google Scholar] [CrossRef]
- Meshram, H.S.; Kute, V.B.; Chauhan, S.; Desai, S. Mucormycosis in post-COVID-19 renal transplant patients: A lethal complication in follow-up. Transpl. Infect. Dis. 2021, 23, e13663. [Google Scholar] [CrossRef]
- Moorthy, A.; Gaikwad, R.; Krishna, S.; Hegde, R.; Kale, P.G.; Rao, P.S.; Haldipur, D.; Bonanthaya, K. SARS-CoV-2, Uncontrolled Diabetes and Corticosteroids—An Unholy Trinity in Invasive Fungal Infections of the Maxillofacial Region? A Retrospective, Multi-centric Analysis. J. Maxillofac. Oral Surg. 2021, 20, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Nehara, H.R.; Puri, I.; Singhal, V.; Ih, S.; Bishnoi, B.R.; Sirohi, P. Rhinocerebral mucormycosis in COVID-19 patient with diabetes a deadly trio: Case series from the north-western part of India. Indian J. Med Microbiol. 2021, 39, 380–383. [Google Scholar] [CrossRef]
- Pakdel, F.; Ahmadikia, K.; Salehi, M.; Tabari, A.; Jafari, R.; Mehrparvar, G.; Rezaie, Y.; Rajaeih, S.; Alijani, N.; Barac, A.; et al. Mucormycosis in patients with COVID-19: A cross-sectional descriptive multicenter study from Iran. Mycoses 2021, 64, 1238–1252. [Google Scholar] [CrossRef] [PubMed]
- Pasero, D.; Sanna, S.; Liperi, C.; Piredda, D.; Branca, G.P.; Casadio, L.; Simeo, R.S.; Buselli, A.; Rizzo, D.; Bussu, F.; et al. A challenging complication following SARS-CoV-2 infection: A case of pulmonary mucormycosis. Infection 2020, 1–6. [Google Scholar] [CrossRef]
- Pauli, M.A.; de Melo Pereira, L.; Monteiro, M.L.; de Camargo, A.R.; Rabelo, G.D. Painful palatal lesion in a COVID-19 patient. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Placik, D.A.; Taylor, W.L.; Wnuk, N.M. Bronchopleural fistula development in the setting of novel therapies for acute respiratory distress syndrome in SARS-CoV-2 pneumonia. Radiol. Case Rep. 2020, 15, 2378–2381. [Google Scholar] [CrossRef]
- Rabagliati, R.; Rodríguez, N.; Núñez, C.; Huete, A.; Bravo, S.; Garcia, P. COVID-19–Associated Mold Infection in Critically Ill Patients, Chile. Emerg. Infect. Dis. 2021, 27, 1454. [Google Scholar] [CrossRef]
- Rao, R.; Shetty, A.; Nagesh, C. Orbital infarction syndrome secondary to rhino-orbital mucormycosis in a case of COVID-19: Clinico-radiological features. Indian J. Ophthalmol. 2021, 69, 1627–1630. [Google Scholar] [CrossRef] [PubMed]
- Ravani, S.A.; Agrawal, G.A.; Leuva, P.A.; Modi, P.H.; Amin, K.D. Rise of the phoenix: Mucormycosis in COVID-19 times. Indian J. Ophthalmol. 2021, 69, 1563–1568. [Google Scholar] [PubMed]
- Revannavar, S.M.; Supriya, P.; Samaga, L.; Vineeth, V. COVID-19 triggering mucormycosis in a susceptible patient: A new phenomenon in the developing world? BMJ Case Rep. CP 2021, 14, e241663. [Google Scholar]
- Saldanha, M.; Reddy, R.; Vincent, M.J. Of the article: Paranasal mucormycosis in COVID-19 patient. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–4. [Google Scholar] [CrossRef]
- Sarkar, S.; Gokhale, T.; Choudhury, S.S.; Deb, A.K. COVID-19 and orbital mucormycosis. Indian J. Ophthalmol. 2021, 69, 1002. [Google Scholar]
- Sen, M.; Lahane, S.; Lahane, T.P.; Parekh, R.; Honavar, S.G. Mucor in a viral land: A tale of two pathogens. Indian J. Ophthalmol. 2021, 69, 244. [Google Scholar]
- Veisi, A.; Bagheri, A.; Eshaghi, M.; Rikhtehgar, M.H.; Kanavi, M.R.; Farjad, R. Rhino-orbital mucormycosis during steroid therapy in COVID-19 patients: A case report. Eur. J. Ophthalmol. 2021, 11206721211009450. [Google Scholar] [CrossRef]
- Waizel-Haiat, S.; Guerrero-Paz, J.A.; Sanchez-Hurtado, L.; Calleja-Alarcon, S.; Romero-Gutierrez, L. A case of fatal rhino-orbital mucormycosis associated with new onset diabetic ketoacidosis and COVID-19. Cureus 2021, 13, e13163. [Google Scholar]
- Werthman-Ehrenreich, A. Mucormycosis with orbital compartment syndrome in a patient with COVID-19. Am. J. Emerg Med. 2021, 42, 264.e5–264.e8. [Google Scholar] [CrossRef]
- Zurl, C.; Hoenigl, M.; Schulz, E.; Hatzl, S.; Gorkiewicz, G.; Krause, R.; Eller, P.; Prattes, J. Autopsy Proven Pulmonary Mucormycosis Due to Rhizopus microsporus in a Critically Ill COVID-19 Patient with Underlying Hematological Malignancy. J. Fungi 2021, 7, 88. [Google Scholar] [CrossRef]
- Mishra, N.; Mutya, V.S.S.; Thomas, A.; Rai, G.; Reddy, B.; Mohanan, A.A. A case series of invasive mucormycosis in patients with COVID-19 infection. Int. J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 867–870. [Google Scholar] [CrossRef]
- Satish, D.; Joy, D.; Ross, A. Balasubramanya. Mucormycosis co-infection associated with global COVID-19: A case series from India. Int. J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 815–820. [Google Scholar] [CrossRef]
- Evert, K.; Dienemann, T.; Brochhausen, C.; Lunz, D.; Lubnow, M.; Ritzka, M.; Keil, F.; Trummer, M.; Scheiter, A.; Salzberger, B.; et al. Autopsy findings after long-term treatment of COVID-19 patients with microbiological correlation. Virchows Arch. 2021, 479, 97–108. [Google Scholar] [CrossRef]
- Khan, N.; Gutierrez, C.G.; Martinez, D.V.; Proud, K.C. A case report of COVID-19 associated pulmonary mucormycosis. Arch. Clin. Cases 2021, 7, 46–51. [Google Scholar] [CrossRef]
- Hoang, K.; Abdo, T.; Reinersman, J.M.; Lu, R.; Higuita, N.I.A. A case of invasive pulmonary mucormycosis resulting from short courses of corticosteroids in a well-controlled diabetic patient. Med. Mycol. Case Rep. 2020, 29, 22–24. [Google Scholar] [CrossRef]
- Pan, A.S.; Srinath, L. Mucormycosis in a patient with AIDS receiving systemic steroids. J. Am. Osteopath. Assoc. 2013, 113, 708–711. [Google Scholar] [CrossRef] [Green Version]
- India Accounts for 1 in 3 New Covid Cases Being Recorded. Available online: https://www.cnbc.com/2021/05/03/india-covid-crisis-charts-show-the-severity-of-the-second-wave.html (accessed on 10 June 2021).
- Corzo-León, D.E.; Chora-Hernández, L.D.; Rodríguez-Zulueta, A.P.; Walsh, T.J. Diabetes mellitus as the major risk factor for mucormycosis in Mexico: Epidemiology, diagnosis, and outcomes of reported cases. Med. Mycol. 2018, 56, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Erener, S. Diabetes, infection risk and COVID-19. Mol. Metabolism. 2020, 39, 101044. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Feng, X.; Li, Q.; Wang, Y.; Li, Q.; Hua, M. Adiponectin, TNF-α and inflammatory cytokines and risk of type 2 diabetes: A systematic review and meta-analysis. Cytokine 2016, 86, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Morales-Franco, B.; Nava-Villalba, M.; Medina-Guerrero, E.O.; Sánchez-Nuño, Y.A.; Davila-Villa, P.; Anaya-Ambriz, E.J.; Charles-Niño, C.L. Host-Pathogen Molecular Factors Contribute to the Pathogenesis of Rhizopus spp. in Diabetes Mellitus. Curr. Trop. Med. Rep. 2021, 8, 6–17. [Google Scholar] [CrossRef]
- Roden, M.M.; Zaoutis, T.E.; Buchanan, W.L.; Knudsen, T.A.; Sarkisova, T.A.; Schaufele, R.L.; Sein, M.; Sein, T.; Chiou, C.C.; Chu, J.H.; et al. Epidemiology and outcome of zygomycosis: A review of 929 reported cases. Clin. Infect. Dis. 2005, 41, 634–653. [Google Scholar] [CrossRef] [Green Version]
- Uğurlu, K.; Selim, S.; Kopar, A.; Songu, M. Rhino-orbital mucormycosis: Clinical findings and treatment outcomes of four cases. Turk. J. Ophthalmol. 2015, 45, 169. [Google Scholar] [CrossRef] [PubMed]
- Rhino-Orbital-Cerebral Mucormycosis. Available online: https://eyewiki.aao.org/Rhino-Orbital-Cerebral_Mucormycosis (accessed on 10 June 2021).
- Patel, A.; Kaur, H.; Xess, I.; Michael, J.; Savio, J.; Rudramurthy, S.; Singh, R.; Shastri, P.; Umabala, P.; Sardana, R.; et al. A multicentre observational study on the epidemiology, risk factors, management and outcomes of mucormycosis in India. Clin. Microbiol. Infect. 2020, 26, 944.e9–944.e15. [Google Scholar] [CrossRef] [PubMed]
- Skiada, A.; Lass-Floerl, C.; Klimko, N.; Ibrahim, A.; Roilides, E.; Petrikkos, G. Challenges in the diagnosis and treatment of mucormycosis. Med. Mycol. 2018, 56, S93–S101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Characterization of Fungal Infections in COVID-19 Infected and Mechanically Ventilated Patients in ICU (MY-CO-VID). Available online: https://clinicaltrials.gov/ct2/show/NCT04368221 (accessed on 25 June 2021).


{kind=link}
| Study | Country | Design | n | Sex | Age (years) | COVID-19 Confirm. | COVID-19 Severity | Onset (days) | Comorbidities | COVID-19 Treatment | Clinical Features | Region | Diagnosis | Genus/Species | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DM | HTN | Asthma | CAD | Other | Steroids | Others | Stain | Cult. | Histo. | ||||||||||||
| Alekseyev et al. 2021 [31] | USA | Case report | 1 | M | 41 | RT-PCR | NR | NR | Yes | No | No | No | DKA | Yes (name NS) | HCQ | NS | NS | No | No | Yes | NS |
| Arana et al. 2021 [32] | Spain | Case report | 1 | M | 62 | RT-PCR | Severe (requiring non-invasive mechanical ventilation) | 7 | Yes | Yes | No | Yes | ESKD | Dexamethasone 6 mg daily for 10 days | Ceftriaxone, azithromycin | Fever, headache and left malar region swelling | Rhinosinusal | No | Yes | No | Rhizopus/Rhizopus oryzae |
| 1 | M | 48 | RT-PCR | Moderate (FiO2: 28%) | 21 | No | Yes | No | No | ESKD | Prednisone 20 mg | HCQ, azithromycin, lopinavir/ritonavir, tocilizumab | Pain and increase in right limb diameter | Musculoskeletal | No | Yes | No | Lichtheimiaceae/Lichtheimia ramosa | |||
| Ashour et al. 2021 [33] | Egypt | Case series | 6 | M/F: 3/3 | 54.66 | RT-PCR (2); NR (4) | Critical (n = 1) on ventilation; NR (n = 5) | Not clear | Yes (100%) | No | No | No | CKD (12.5%) | NR | NR | Ophthalmoplegia (66%), conjunctival chemosis (33%), eyelid edema (33%), facial edema (33%) | Rhino-orbital-cerebral (100%) | No | Yes | Yes | NS |
| Bayram et al. 2021 [34] | Turkey | Case series | 11 | M/F: 9/2 | 73.1 ± 7.7 years (range: 61–88 years) | Suspected | Severe (oxygen saturation <93% in room air) | 14.4 ± 4.3 (range: 7–23 days) | Yes (73%) | Yes (64%) | Yes (18%) | Renal failure (45%) | Dexamethasone (100%) | NR | Proptosis (100%), ophthalmoplegia (64%), orbital pain (82%), conjunctival hyperemia or chemosis (82%), ptosis (64%), fixed and dilated pupil (64%), vision loss (64%), endophthalmitis (54.5%), and decreased vision (27%) | NR | Yes | Yes | Yes | NR | |
| Bellanger et al. 2021 [35] | France | Case report | 1 | M | 55 | RT-PCR | Severe (ICU) | 21 | No | No | No | No | Follicular lymphoma, influenza B | NR | NR | Worsening of respiratory symptoms | NR | NR | Yes | Yes | Rhizopus/Rhizopus microsporus |
| Dallalzadeh et al. 2021 [36] | USA | Case report | 1 | M | 48 | RT-PCR | Critical (ICU, ventilation) | 6 | Yes | No | No | No | Ketoacidosis | Dexamethasone | CCP (COVID-19 convalescent plasma) | NR | Rhino-orbital | Yes | Yes | No | Rhizopus/Rhizopus species |
| El-Kohly et al. 2021 * [38] | Egypt | Cross-sectional | 28 | M/F: 19/17 | 52.92 ± 11.30 | RT-PCR | Mixed (mild (n = 11), moderate (n = 13), severe (n = 12)) | 17.82 ± 2.97 | Yes (27.8%) | Yes (17%) | Yes (8%) | No | CKD (8%) | Yes (name NS) | Antiviral, anticoagulant, and vitamins (name NS) | Headache and facial pain (75%), facial numbness (67%), ophthalmoplegia, and visual loss (64%), ophthalmoplegia (64%), diplopia (17%) | Sinonasal (100%), orbital (81%), cerebral (29%), and palatine (33%) | Yes | Yes | Yes | Mucor-species |
| Evert et al. 2020 [70] | Germany | Case series | 2 | F | 52.5 | RT-PCR | Critical (n = 2 on ventilation) | NR | No | No | No | No | Obesity, liver cirrhosis | Yes | NR | NR | NR | No | No | Yes | Mucor-species |
| Garg et al. 2021 [39] | India | Case report | 1 | M | 55 | RT-PCR | Severe (84% SpO2) | 21 | Yes | Yes | No | No | ESRD, Ischemic cardiomyopathy, venous thrombosis | Dexamethasone (6 mg, once a day for 14 days) | Remdesivir (200 mg on day 1 and 100 mg on days 2–5); supportive care | Cavitary pneumonia with pleural effusion | Pulmonary mucormycosis/cavitary pneumonia with pleural effusion | Yes | Yes | No | Rhizopus/Rhizopus microsporus |
| Hanley et al. 2020 (Autopsy) [40] | UK | Case series | 1 | M | 22 | RT-PCR | Critical (mechanical ventilation, vasopressor, ICU) | Concurrent | NR | NR | NR | NR | Frank necrotic- hemorrhagic pancreatitis; renal failure | NR | NR | NR | NR | Yes | No | Yes | NR |
| Johnson et al. 2021 [41] | USA | Case report | 1 | M | 79 | RT-PCR | Critical (ICU, ventilation) | 19 | Yes | Yes | No | No | Pulmonary aspergillosis | IV dexamethasone (6 mg daily for 10 days) | IV remdesivir (200 mg × 1, then 100 mg daily) | NR | NR | No | Yes (BAL culture) | Yes | Rhizopus/Rhizopus arrhizus |
| Junior et al. 2020 [37] | Brazil | Case report | 1 | M | 86 | Throat swab | Severe (ICU) | Concurrent | No | Yes | No | No | NR | Hydrocortisone | Oseltamivir | Mild abdominal tenderness | NR | Yes | No | Yes | NR |
| Kanwar et al. 2021 [42] | USA | Case report | 1 | M | 56 | RT-PCR | Severe | 13 | No | No | No | No | ESRD | Methylprednisolone | Tocilizumab | Necrotizing pneumonia with empyema | NR | Yes | Yes | No | Rhizopus/Rhizopus azygosporus |
| Karimi-Galougah et al. 2021 [43] | Iran | Case report | 1 | F | 61 | RT-PCR | NR | 21 | Yes | No | No | No | NR | Yes (name NS) | Remdesivir, interferon alpha | Hemifacial pain, proptosis, frozen eye, complete loss of vision, and fixed mydriasis | Rhino-orbital | NR | NR | Yes | NR |
| Khatri et al. 2021 [44] | USA | Case report | 1 | M | 68 | Suspected | Critical | 90 | Yes | Yes | No | Yes | Severe heart failure, obstructive sleep apnea; renal failure | Methylprednisolone/Prednisone (for gout) | CCP | Purplish skin discoloration with fluctuant swelling | Cutaneous | Yes | Yes | Yes | Rhizopus/Rhizopus microsporus |
| Khan et al. 2020 [71] | USA | Case report | 1 | F | 44 | RT-PCR | Critical (ICU, ventilation) | 13 | Yes | No | No | No | No | Methylprednisolone 30 mg IV twice a day | Remdesivir 100 mg IV daily | NR | Pulmonary mucormycosis | Yes | Yes | Yes | NS |
| Krishna et al. 2021 [45] | India | Case report | 1 | M | 34 | RT-PCR | Severe | NR | Yes | Yes | No | No | NR | NR | NR | Swelling pain over the first quadrant teeth | Sinonasal | No | No | Yes | NR |
| Krishna et al. 2021 [46] | UK | Case report (autopsy) | 1 | M | 22 | RT-PCR | Severe (mechanical ventilation) | Autopsy | No | No | No | No | No | Yes (name NS) | Meropenem and teicoplanin | Thrombo-emboli were seen in the lungs, brain, pharynx, nasal mucosa, and trachea | NR | Yes | No | No | Mucorales/NS |
| Maini et al. 2021 [47] | India | Case report | 1 | M | 38 | RT-PCR | Severe (ICU) | 18 | No | No | No | No | NO | Methylprednisolone (80 mg/day) | Inj. remdesivir IV with a loading dose of 200 mg, followed by 100 mg daily for 11 days. | Swelling and pain in the left eye | Rhino-orbital-cerebral | Yes | Yes | Yes | Rhizopus/Rhizopus oryzae |
| Mehta et al. 2020 [48] | India | Case report | 1 | M | 60 | RT-PCR | Critical (ICU, ventilation) | 11 | Yes | No | No | No | No | Methylprednisolone (40 mg twice daily) and dexamethasone (4 mg twice daily) | Oseltamivir (75 mg twice daily), later tocilizumab (400 mg) | Bilateral lid edema with right eye prominence, febrile, breathless, and hypoxic | Rhino-orbital-cerebral | Yes | Yes | Yes | Mucorales/unspecified |
| Mekonnen et al. 2021. [49] | USA | Case report | 1 | M | 60 | Suspected | Critical (mechanical ventilation, ICU) | 4 | Yes | Yes | Yes | No | AKI | Dexamethasone | CCP | Proptosis, erythema and edema of the eyelids, and conjunctival chemosis | Rhino-orbital | Yes | Yes | Yes | Rhizopus/Rhizopus species |
| Meshram et al. 2021 [50] | India | Case report (renal transplant recipients) | 2 | M | 47; 25 | Suspected | Mild | NR | Yes | No | No | No | No | NR | NR | Swelling over the face and black nasal discharge (50%); fever, cough, and black expectoration (50%) | Rhino-orbito-cerebral | No | Yes | Yes | No |
| Mishra et al. 2021 [68] | India | Case series | 10 | M/F: 9/1 | 55.8 | Suspected | Mixed (mild (n = 3); moderate (n = 6); severe (n = 1)) | NR | Yes (80%) | Yes (30%) | No | No | CKD (20%) | Yes (60%) | Remdesivir (50%) | Eye pain, facial pain and nasal block | NS | No | No | Yes | NS |
| Moorthy et al. 2021 [51] | India | Case series | 17 | M:15, F:2 | 54.6, 35–73 (mean, range) | RT-PCR | Not specified | Concurrent (n = 4) | Yes (82.73%)-14 | No | No | No | No | Yes (100%) | NS | Orbital cellulitis, facial swelling, headache, proptosis, oedema of the extraocular muscles, ophthalmoplegia | Sinusitis alone (n = 3), rhino- orbital (n = 6), rhino-orbital- cerebral (n = 5), rhino-cerebral (n = 3) | Yes | No | Yes | Mucorales/unspecified |
| Nehara et al. 2021 [52] | India | Case series | 5 | M/F: 1/4 | 62.2 Average age | RT-PCR | NR | NR | Yes (100%) | Yes (40%) | No | No | Yes (20%) | Dexamethasone | Oxygen supplementation, intravenous meropenem, remdesivir (40%), subcutaneous enoxaparin, tablet azithromycin, basal-bolus insulin, and supportive care | Severe headache, diminished vision, chemosis, mild proptosis, complete ophthalmoplegia, blackish discharge from the nasal cavity, and black crust on the hard palate | Rhinocerebral | Yes | Yes | Yes | Rhizopus/Rhizopus arrhizus |
| Pakdel et al. 2021 [53] | Iran | Cross-sectional | 15 | M: 10; F: 5 | Median age: 52 (14–71) | RT-PCR | Severe (34%) | Median: 7 (1–37) | Yes (87%) | Yes (46%) | Yes (13%) | No | Ketoacidosis (6%) | Dexamethsaone (46%) | Yes (7%) | Unilateral periorbital pain and edema (73%), eyelid ptosis (73%), acute vision loss (73%), proptosis (73%), unilateral facial edema (60%), cranial nerve palsy (60%), headache (33%), fever (27%), nasal blockage (13%), and ear pain (7%) | Mixed (rhinorbital (47%); sino-orbital (33%), isolated orbital movement (13%), and others) | Yes | No | Yes | NS |
| Pasero et al. 2020 [54] | Italy (renal transplant) | Case report | 1 | M | 66 | RT-PCR | Critical (ICU) | 14 | No | Yes | No | No | Renal failure | No | HCQS, lopinavir, ritonavir | NS | NS | Yes | Yes | No | Rhizopus/Rhizopus species |
| Pauli et al. 2021 [55] | Brazil | Case report | 1 | F | 50 | Suspected | Mild | 8 | Yes | No | No | No | No | Hydrocortisone | NR | Deep ulcerated lesion located at the center of the hard palate | Palatal ulcer | Yes | No | Yes | Mucorales/unspecified) |
| Placik et al. 2020 [56] | USA | Case report | 1 | M | 49 | RT-PCR | Critical | 14 | No | No | No | No | No | Dexamethasone | Remdesivir, tocilizumab | Necrotizing pneumonia with bronchopleural fistula | NS | Yes | Yes | Yes | Rhizopus/Rhizopus species |
| Rabagliati et al. 2021 [57] | Chile | Retrospective cohort study | 1 | M | 55 | Suspected | Critical (ICU) | Not specified | Yes | Yes | No | Yes | Atrial fibrillation | 812 mg prednisone equivalent | No | NS | NS | No | Yes | No | Rhizopus/Rhizopus microsporus |
| Rao et al. 2021 [58] | India | Case report | 1 | M | 66 | Suspected | NR | NR | No | No | No | No | No | Systematic steroids | NR | Complete left ptosis and proptosis, chemosis and fixed dilated left pupil, and absence of left ocular movements in all directions of gaze, vision loss in the left eye | Rhino-orbito-cerebral | No | Yes | No | Fungal hyphae |
| Ravani et al. 2021 [59] | India | Retrospective cohort | 18 | NR | NR | RT-PCR | NR | 60 | Yes (100%) | NR | NR | NR | NR | Dexamethasone | NR | Diminution of vision (<6/60 in 81% of patients) and ophthalmoplegia (77%), orbital cellulitis (61%), pansinusitis (77%) | NR | No | No | Yes | NS |
| Revannavar et al. 2021 [60] | India | Case report | 1 | F | NR | RT-PCR | Mild | Not specified | Yes | No | No | No | No | NR | NR | Left-sided facial pain, complete ptosis and fever, tenderness of all sinuses on left side, ophthalmoplegia (left eye), left eye visual acuity | NS | No | Yes | Yes | Rhizopus/Rhizopus species |
| Saldanha et al. 2021 [61] | India | Case report | 1 | F | 32 | RT-PCR | Not specified | Concurrent | Yes | No | No | No | No | NR | NR | Left eye complete ptosis and left facial pain, visual acuity (left eye) | NS | No | Yes | Yes | NS |
| Sarkar et al. 2021 [62] | India | Case series | 6 | M:4, F:2 | 44 | RT-PCR | Critical (n = 6) | Concurrent | Yes (100%) | No | No | No | Ketoacidosis (33%) | Dexamethasone | Remdesivir (84%) | Visual acquity (100%) | Rhino-orbital (n = 5), rhino- orbital-cerebral (n = 1) | Yes | Yes | No | Rhizopus (n = 4), Mucorales (n = 2) |
| Satish et al. 2021 [69] | India | Case series | 11 | NR | NR | RT-PCR | Mixed (mild (n = 2); moderate (n = 3); severe (n = 4); asymptomatic (n = 2) | NR | Yes (100%) | No | No | No | No | NR | NR | NR | NS | Yes | No | No | NR |
| Sen et al. 2021 [63] | India | Retrospective cohort | 6 (5 patients post covid-19 recoved) | M | 60.5 ± 12 (range 46.2 to 73.9) years | RT-PCR | Severe | NR | Yes (100%) | Yes (50%) | No | Yes (16.6%) | Diabetic ketoacidosis (50%) | Intravenous methylprednisolone/dexamethasone/oral prednisolone (84%) | No | Pain, redness, and periocular swelling, drooping of eyelids, limitation of ocular movements, and painful loss of vision | Rhino-orbital-cerebral | No | Yes | Yes | Mucorales/unspecified |
| Veisi et al. 2021 [64] | Iran | Case report | 1 | F | 40 | RT-PCR | Mild | NR | No | No | No | No | No | Dexamethasone (8 mg/day) | Remdesivir 200 mg on day 1 followed by 100 mg daily for 4 days, and IV levofloxacin (500 mg/day), | Bilateral visual loss, periorbital pain, and visual acuity | Rhino-orbito-cerebral | NR | NR | Yes | NR |
| 1 | M | 54 | RT-PCR | NR | NR | Yes | No | No | No | Dexamethasone (8 mg/day) | Remdesivir 200 mg on day 1 followed by 100 mg daily for 4 days, IV levofloxacin (500 mg/day) | Left orbital pain and periorbital swelling together with progressive vision loss | Rhino-orbital | NR | NR | Yes | NR | ||||
| Waizel-Haiat et al. 2021 [65] | Mexico | Case report | 1 | F | 24 | RT-PCR | Critical (ICU) | Concurrent | Yes | No | No | No | Ketoacidosis, renal failure | NA | NA | Left lid swelling and maxillary hypoesthesia, left hyperemic conjunctiva, and an opaque cornea | Rhino-orbital | Yes | Yes | No | Lichtheimia (Absidia) species |
| Werthman-Ehrenreich et al. 2021 [66] | USA | Case report | 1 | F | 33 | Suspected | Severe (ICU) | Concurrent | Yes | Yes | Yes | No | Ketoacidosis, renal failure | No | Remdesivir, CCP | Eye ptosis | Rhino-orbital-cerebral | Yes | Yes | No | Mucorales/unspecified |
| Zurl et al. 2021 [67] | Austria | Case report | 1 | M | 53 | RT-PCR | Critical (ICU) | Concurrent | No | No | No | No | Myelodysplastic syndromes, acute myeloid leukemia | Prednisolone | Tocilizumab | NR | Fungal pneumonia with effusion | Yes | No | Yes | Rhizopus/Rhizopus microsporus |
| Study (Author, Year) | Country | Treatment | Patient Outcome * | |
|---|---|---|---|---|
| Medical Management | Surgical Management | |||
| Alekseyev et al. 2021 [31] | USA | NR | Yes | Lived |
| Arana et al. 2021 [32] | Spain | Amphotericin B (LAmB 5 mg/kg/day), isavuconazole, and subsequently posaconazole | Yes (surgical debridement) | Lived |
| Amphotericin B (LAmB 5 mg/kg/day) together with isavuconazole 200 mg/8 h for 24 days | Yes (surgical debridement) | Lived | ||
| Ashour et al. 2021 [33] | Egypt | Amphotericin B | Yes (surgical debridement (n = 4)) | Lived (67%), Died (33%) |
| Bayram et al. 2021 [34] | Turkey | Amphotericin B, voriconazole | Yes (all patients: endoscopic sinus surgery with extensive debridement) | Lived (36%), Died (64%) |
| Bellanger et al. 2021 [35] | France | Amphotericin B (LAmB 5 mg/kg/day) | No | Died |
| Dallalzadeh et al. 2021 [36] | USA | AMB/isavuconazole | No | Died |
| El-Kohly et al. 2021 * [38] | Egypt | Amphotericin B; voriconazole; posaconazole | Yes (endoscopic debridement (n = 27)) | Lived (64%), Died (36%) |
| Evert et al. 2020 [70] | Germany | NR | NR | Died (100%) |
| Garg et al. 2021 [39] | India | Amphotericin B (LAmB 5 mg/kg/day) | No | Lived |
| Hanley et al. 2020 [40] | UK | NR | NR | Died |
| Johnson et al. 2021 [41] | USA | Amphotericin B (LAmB 400 mg daily) | Yes (no tracheostomy, and percutaneous endoscopic gastrostomy) | Lived |
| Junior et al. 2020 [37] | Brazil | No | NR | Died |
| Kanwar et al. 2021 [42] | USA | Amphotericin B (LAmB 5 mg/kg/day) | Yes (robotic decortication surgery) | Died |
| Karimi-Galougah et al. 2021 [43] | Iran | Yes (not specified) | Yes (endonasal endoscopic debridement of necrotic tissue, right eye exenteration) | Lived |
| Khatri et al. 2021 [44] | USA | Amphotericin B + posaconazole | Yes (thoracic cavity debridement) | Died |
| Khan et al. 2020 [71] | USA | Amphotericin B (5 mg/kg/day) | No | Died |
| Krishna et al. 2021 [45] | India | Amphotericin B (LAmB 5 mg/kg/day) | Yes (surgical resection) | Lived |
| Krishna et al. 2021 [46] | UK | Caspofungin | No | Died |
| Maini et al. 2021 [47] | India | Amphotericin B 300 mg/day, tobramycin and fluconazole | Yes (debridement) | Lived |
| Mehta et al. 2020 [48] | India | Amphotericin B | No | Died |
| Mekonnen et al. 2021. [49] | USA | Amphotericin B (LAmB) + caspofungin/posaconazole | Yes (sinus debridement) | Died |
| Meshram et al. 2021 [50] | India | Amphotericin B | Yes (maxillectomy) | Died |
| Mishra et al. 2021 [68] | India | Amphotericin B | Yes ((all patients (mixed or any single surgery): functional endoscopic sinus surgery, endoscopic maxillectomy, local debridement) | Lived (50%), Died (40%), Lost to follow-up (10%) |
| Moorthy et al. 2021 [51] | India | Amphotericin B (5 mg/kg/day) | Yes (FESS (n = 17), maxillectomy(n = 11), exenteration (n = 11)) | Died (35.29%) |
| Nehara et al. 2021 [52] | India | Amphotericin B (LAmB 5 mg/kg/day), posaconazole | No | Lived (60%), Died (40%) |
| Pakdel et al. 2021 [53] | Iran | Amphotericin B (LAmB 5 mg/kg/day), oral posaconazole | Yes (sinus debridement (n = 12); orbital externation (n = 5); palatal debridement (n = 2)) | Lived (53%), Died (47%) |
| Pasero et al. 2020 [54] | Italy | Amphotericin B/isavuconazole | No | Died |
| Pauli et al. 2021 [55] | Brazil | Amphotericin B | Yes (debridement) | Lived |
| Placik et al. 2020 [56] | USA | Amphotericin B | Yes (resection) | Died |
| Rabagliati et al. 2021 [57] | Chile | Amphotericin B (LAmB) | No | Died |
| Rao et al. 2021 [58] | India | Amphotericin B (LAmB) | Yes (endoscopic sinus surgery) | NR |
| Ravani et al. 2021 [59] | India | Amphotericin B (LAmB 5 mg/kg/day) | Yes (sinus debridement; n = 18) | Lived (94%), Died (6%) |
| Revannavar et al. 2021 [60] | India | Amphotericin B | Yes (endoscopic sinus surgery) | Lived |
| Saldanha et al. 2021 [61] | India | Amphotericin B (25 mg/day) | Yes (endoscopic sinus surgery) | Lived |
| Sarkar et al. 2021 [62] | India | Amphotericin B | Yes (maxillectomy (n = 3), debridement (n = 1)) | Died |
| Satish et al. 2021 [69] | India | Amphotericin B | Yes (all patients: surgical debridement) | No data |
| Sen et al. 2021 [63] | India | Amphotericin B (LAmB)+ voriconazole/posaconazole | Yes (exenteration (n = 2), sinus debridement (n = 3)) | Lived |
| Veisi et al. 2021 [64] | Iran | Amphotericin B (4 mg/kg/day) | Yes (surgical debridement) | Died |
| Amphotericin B (3 mg/kg/day) | Yes (endoscopic sinus surgery) | Lived | ||
| Waizel-Haiat et al. 2021 [65] | Mexico | Amphotericin B | No | Died |
| Werthman-Ehrenreich et al. 2021 [66] | USA | Amphotericin B | Yes (sinus debridement) | Died |
| Zurl et al. 2021 [67] | Austria | No | No | Died |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussain, S.; Baxi, H.; Riad, A.; Klugarová, J.; Pokorná, A.; Slezáková, S.; Líčeník, R.; Najmi, A.K.; Klugar, M. COVID-19-Associated Mucormycosis (CAM): An Updated Evidence Mapping. Int. J. Environ. Res. Public Health 2021, 18, 10340. https://doi.org/10.3390/ijerph181910340
Hussain S, Baxi H, Riad A, Klugarová J, Pokorná A, Slezáková S, Líčeník R, Najmi AK, Klugar M. COVID-19-Associated Mucormycosis (CAM): An Updated Evidence Mapping. International Journal of Environmental Research and Public Health. 2021; 18(19):10340. https://doi.org/10.3390/ijerph181910340
Chicago/Turabian StyleHussain, Salman, Harveen Baxi, Abanoub Riad, Jitka Klugarová, Andrea Pokorná, Simona Slezáková, Radim Líčeník, Abul Kalam Najmi, and Miloslav Klugar. 2021. "COVID-19-Associated Mucormycosis (CAM): An Updated Evidence Mapping" International Journal of Environmental Research and Public Health 18, no. 19: 10340. https://doi.org/10.3390/ijerph181910340
APA StyleHussain, S., Baxi, H., Riad, A., Klugarová, J., Pokorná, A., Slezáková, S., Líčeník, R., Najmi, A. K., & Klugar, M. (2021). COVID-19-Associated Mucormycosis (CAM): An Updated Evidence Mapping. International Journal of Environmental Research and Public Health, 18(19), 10340. https://doi.org/10.3390/ijerph181910340