
Effects of Performing Applied Muscle Tension during Recovery after Phlebotomy in Young, First-Time Donors: A Pilot Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Study Design and Statistical Analysis
3. Results
3.1. Haemodynamic Findings
3.2. Questionnaire Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Hong Kong Red Cross Blood Transfusion Service, 2020 Blood Donation Infographic. Available online: https://www5.ha.org.hk/rcbts/blood-collect-2020 (accessed on 20 September 2021).
- Sun, F. Hong Kong Blood Bank Makes Urgent Appeal as COVID-19 Pandemic Fears Keep Donors Away, Supplies Dry Up. Available online: https://www.scmp.com/news/hong-kong/society/article/3098316/hong-kong-blood-bank-makes-urgent-appeal-COVID-19-pandemic (accessed on 10 September 2021).
- Wong, H.K.; Chu, C.C.Y.; Lau, C.W.; Leung, J.N.S.; Lee, I.Y.M.; Lee, C.K. Vasovagal reaction in blood donors: Prediction and its impact on donor return. ISBT Sci. Ser. 2018, 13, 421–428. [Google Scholar] [CrossRef]
- France, C.R.; France, J.L.; Frame-Brown, T.A.; Venable, G.A.; Menitove, J.E. Fear of blood draw and total draw time combine to predict vasovagal reactions among whole blood donors. Transfusion 2016, 56, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Newman, B.H. Management of Young Blood Donors. Transfus. Med. Hemotherapy 2014, 41, 284–295. [Google Scholar] [CrossRef] [Green Version]
- Marchiondo, K.J. Emergency: Recognizing and treating vasovagal syncope. AJN Am. J. Nurs. 2010, 110, 50–53. [Google Scholar] [CrossRef]
- Ditto, B.; Wilkins, J.A.; France, C.R.; Lavoie, P.; Adler, P.J. On-site training in applied muscle tension to reduce vasovagal reactions to blood donation. J. Behav. Med. 2003, 26, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Ditto, B.; Byrne, N.; Holly, C. Physiological correlates of applied tension may contribute to reduced fainting during medical procedures. Ann. Behav. Med. 2009, 37, 306–314. [Google Scholar] [CrossRef]
- Ditto, B.; France, C.R.; Albert, M.; Byrne, N. Dismantling applied tension: Mechanisms of a treatment to reduce blood donation-related symptoms. Transfusion 2007, 47, 2217–2222. [Google Scholar] [CrossRef]
- Holly, C.D.; Torbit, L.; Ditto, B. Applied tension and coping with blood donation: A randomized trial. Ann. Behav. Med. 2012, 43, 173–180. [Google Scholar] [CrossRef]
- France, C.R.; France, J.L.; Himawan, L.K.; Stephens, K.Y.; Frame-Brown, T.A.; Venable, G.A.; Menitove, J.E. How afraid are you of having blood drawn from your arm? A simple fear question predicts vasovagal reactions without causing them among high school donors. Transfusion 2013, 53, 315–321. [Google Scholar] [CrossRef] [PubMed]
- France, C.R.; France, J.L.; Wissel, M.E.; Ditto, B.; Dickert, T.; Himawan, L.K. Donor anxiety, needle pain, and syncopal reactions combine to determine retention: A path analysis of two-year donor return data. Transfusion 2013, 53, 1992–2000. [Google Scholar] [CrossRef] [Green Version]
- Kowalsky, J.M.; France, J.L.; Wissel, M.E.; France, C.R. Effect of applied muscle tension on cerebral oxygenation in female blood donors. Transfusion 2011, 51, 1802–1808. [Google Scholar] [CrossRef]
- France, C.R.; Ditto, B.; Wissel, M.E.; France, J.L.; Dickert, T.; Rader, A.; Sinclair, K.; McGlone, S.; Trost, Z.; Matson, E. Predonation hydration and applied muscle tension combine to reduce presyncopal reactions to blood donation. Transfusion 2010, 50, 1257–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morand, C.; Coudurier, N.; Rolland, C.; Thoret, S.; Legrand, D.; Tiberghien, P.; Bosson, J.L. Prevention of syncopal-type reactions after whole blood donation: A cluster-randomized trial assessing hydration and muscle tension exercise. Transfusion 2016, 56, 2412–2421. [Google Scholar] [CrossRef]
- Wieling, W.; France, C.R.; van Dijk, N.; Kamel, H.; Thijs, R.D.; Tomasulo, P. Physiologic strategies to prevent fainting responses during or after whole blood donation. Transfusion 2011, 51, 2727–2738. [Google Scholar] [CrossRef]
- Boulton, D.; Taylor, C.E.; Macefield, V.G.; Green, S. Effect of contraction intensity on sympathetic nerve activity to active human skeletal muscle. Front. Physiol. 2014, 5, 194. [Google Scholar] [CrossRef] [Green Version]
- Wieling, W.; de Lange, F.J.; Jardine, D.L. The heart cannot pump blood that it does not receive. Front. Physiol. 2014, 5, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, J.E. Guyton and Hall Textbook of Medical Physiology, 13th ed.; Elsevier Health Sciences: Philadelphia, PA, USA, 2016; pp. 109–122. [Google Scholar]
- Sarelius, I.; Pohl, U. Control of muscle blood flow during exercise: Local factors and integrative mechanisms. Acta Physiol. 2010, 199, 349–365. [Google Scholar] [CrossRef] [PubMed]
- Ost, L.G.; Jerremalm, A.; Jansson, L. Individual response patterns and the effects of different behavioral methods in the treatment of agoraphobia. Behav. Res. Ther. 1984, 22, 697–707. [Google Scholar] [CrossRef]
- Ost, L.G.; Lindahl, I.L.; Sterner, U.; Jerremalm, A. Exposure in vivo vs applied relaxation in the treatment of blood phobia. Behav. Res. Ther. 1984, 22, 205–216. [Google Scholar] [CrossRef]
- Ditto, B.; France, C.R.; Lavoie, P.; Roussos, M.; Adler, P.J. Reducing reactions to blood donation with applied muscle tension: A randomized controlled trial. Transfusion 2003, 43, 1269–1275. [Google Scholar] [CrossRef]
- Knobloch, K.; Lichtenberg, A.; Winterhalter, M.; Rossner, D.; Pichlmaier, M.; Phillips, R. Non-invasive cardiac output determination by two-dimensional independent doppler during and after cardiac surgery. Ann. Thorac. Surg. 2005, 80, 1479–1483. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.L.; Pinder, M.; Parsons, R.; Roberts, B.; van Heerden, P.V. Clinical evaluation of USCOM ultrasonic cardiac output monitor in cardiac surgical patients in intensive care unit. Br. J. Anaesth. 2005, 94, 287–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Critchley, L.A.; Peng, Z.Y.; Fok, B.S.; Lee, A.; Phillips, R.A. Testing the reliability of a new ultrasonic cardiac output monitor, the USCOM, by using aortic flowprobes in anesthetized dogs. Anesth. Analg. 2005, 100, 748–753. [Google Scholar] [CrossRef]
- Phillips, R.A.; Hood, S.G.; Jacobson, B.M.; West, M.J.; Wan, L.; May, C.N. Pulmonary artery catheter (PAC) accuracy and efficacy compared with flow probe and transcutaneous doppler (USCOM): An ovine cardiac output validation. Crit. Care Res. Pract. 2012, 2012, 621496. [Google Scholar] [CrossRef]
- Lee, S.W.Y.; Khaw, K.S.; Kee, W.D.N.; Leung, T.Y.; Critchley, L.A.H. Haemodynamic effects from aortocaval compression at different angles of lateral tilt in non-labouring term pregnant women. Br. J. Anaesth. 2012, 109, 950–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.C.W.; Lee, S.W.Y.; Khaw, K.; Ali, A.; Sheridan, S.E.; Wong, S.H.S. Haemodynamic responses of wearing low-pressure sports compression tights during an orthostatic challenge in healthy individuals. J. Sci. Med. Sport 2018, 21, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Critchley, L.A.; Lee, D.C.; Khaw, K.S.; Lee, S.W. The effect of head up tilting on bioreactance cardiac output and stroke volume readings using suprasternal transcutaneous doppler as a control in healthy young adults. J. Clin. Monit. Comput. 2016, 30, 519–526. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Baseline | Phlebotomy | Recovery | |||
|---|---|---|---|---|---|---|
| 50% Donated | 100% Donated | 5 min | 10 min | |||
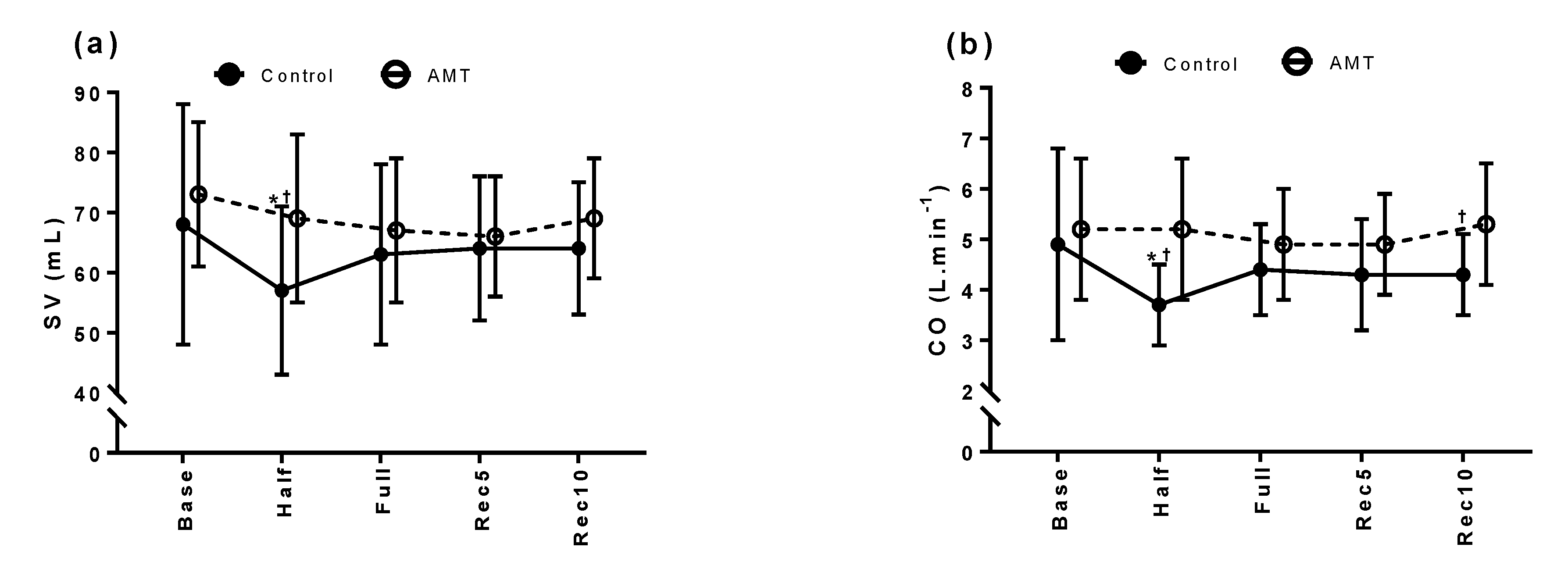
| SV (mL) | Control | 68 ± 20 | 57 ± 14 *,† | 63 ± 15 | 64 ± 12 | 64 ± 11 |
| AMT | 73 ± 12 | 69 ± 14 | 67 ± 12 | 66 ± 10 | 69 ± 10 | |
| CO (L·min−1) | Control | 4.9 ± 1.9 | 3.7 ± 0.8 *,† | 4.4 ± 0.9 | 4.3 ± 1.1 | 4.3 ± 0.8 † |
| AMT | 5.2 ± 1.4 | 5.2 ± 1.4 | 4.9 ± 1.1 | 4.9 ± 1.0 | 5.3 ± 1.2 | |
| SVR (dyn·s·cm−5) | Control | 1689 ± 945 | 1962 ± 427 *,† | 1666 ± 416 | 1640 ± 401 | 1591 ± 338 |
| AMT | 1523 ± 404 | 1569 ± 415 | 1653 ± 332 | 1547 ± 393 | 1379 ± 239 | |
| HR (beat·min−1) | Control | 71 ± 14 | 67 ± 11 | 70 ± 12 | 68 ± 13 | 68 ± 11 |
| AMT | 70 ± 11 | 75 ± 10 | 73 ± 8 | 74 ± 11 | 77 ± 12 | |
| SBP (mmHg) | Control | 113 ± 11 | 116 ± 14 | 116 ± 11 † | 112 ± 10 | 110 ± 10 † |
| AMT | 118 ± 8 | 125 ± 11 | 127 ± 14 | 118 ± 14 | 119 ± 10 | |
| DBP (mmHg) | Control | 72 ± 7 † | 74 ± 8 | 72 ± 7 † | 70 ± 6 † | 68 ± 9 |
| AMT | 79 ± 5 | 80 ± 8 | 81 ± 11 | 79 ± 12 | 74 ± 9 | |
| STAI Y1 | STAI Y2 | Immediate BDRI | Delayed BDRI | Return Rates | |
|---|---|---|---|---|---|
| Control | 31 ± 8 | 35 ± 8 | 1 ± 1 | 4 ± 10 | 88% † |
| AMT | 38 ± 11 | 42 ± 12 | 3 ± 3 | 2 ± 2 * | 59% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, C.H.Y.; Khaw, M.L.; Leung, W.S.; Tam, S.Y.; Chu, C.Y.; Lee, C.K.; Lee, S.W.Y. Effects of Performing Applied Muscle Tension during Recovery after Phlebotomy in Young, First-Time Donors: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 10541. https://doi.org/10.3390/ijerph181910541
Cheung CHY, Khaw ML, Leung WS, Tam SY, Chu CY, Lee CK, Lee SWY. Effects of Performing Applied Muscle Tension during Recovery after Phlebotomy in Young, First-Time Donors: A Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10541. https://doi.org/10.3390/ijerph181910541
Chicago/Turabian StyleCheung, Cara H. Y., May L. Khaw, Wan Shun Leung, Shing Yau Tam, Chui Yee Chu, Cheuk Kwong Lee, and Shara W. Y. Lee. 2021. "Effects of Performing Applied Muscle Tension during Recovery after Phlebotomy in Young, First-Time Donors: A Pilot Study" International Journal of Environmental Research and Public Health 18, no. 19: 10541. https://doi.org/10.3390/ijerph181910541
APA StyleCheung, C. H. Y., Khaw, M. L., Leung, W. S., Tam, S. Y., Chu, C. Y., Lee, C. K., & Lee, S. W. Y. (2021). Effects of Performing Applied Muscle Tension during Recovery after Phlebotomy in Young, First-Time Donors: A Pilot Study. International Journal of Environmental Research and Public Health, 18(19), 10541. https://doi.org/10.3390/ijerph181910541