
Ergonomic Risk Assessment of Dental Students—RULA Applied to Objective Kinematic Data

 , ,
, , 
 , ,
, ,  and
and 
Abstract
:1. Background
2. Material and Methods
2.1. Subjects
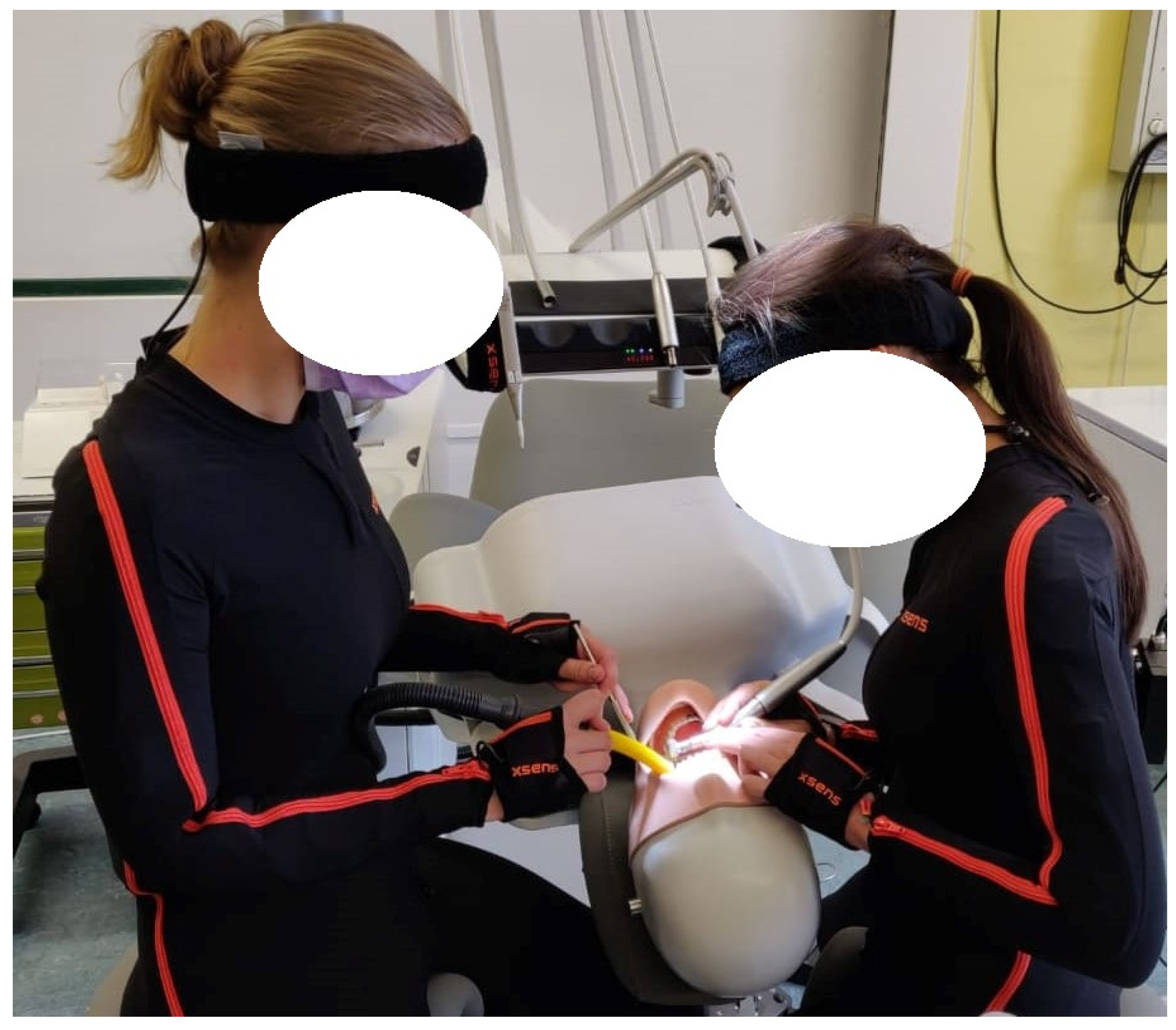
2.2. Measurement System
2.3. Measurement Protocol
2.4. RULA
- -
- 1–2: Posture is acceptable if not maintained.
- -
- 3–4: Further investigation needed. May need changes.
- -
- 5–6: Further investigation and changes needed soon.
- -
- 7: Investigation and changes required immediately.
- Median + interquartile distance (IQR);
- Relative time score;
- Ergonomic risk potential (ERP).
- Neck Score - RULA Step 9
- Trunk Score - RULA Step 10
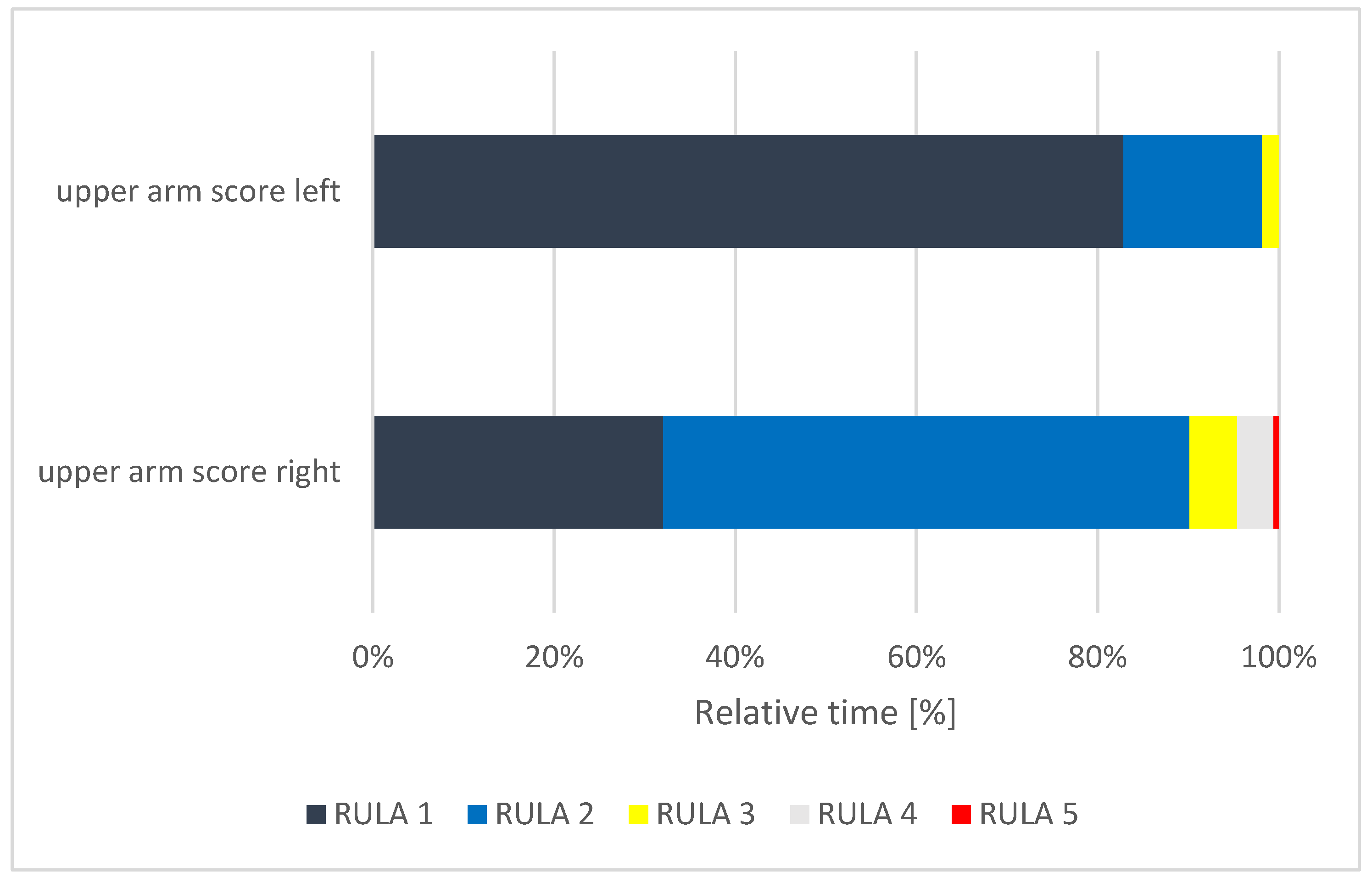
- Upper Arm Score (left and right) - RULA Step 1
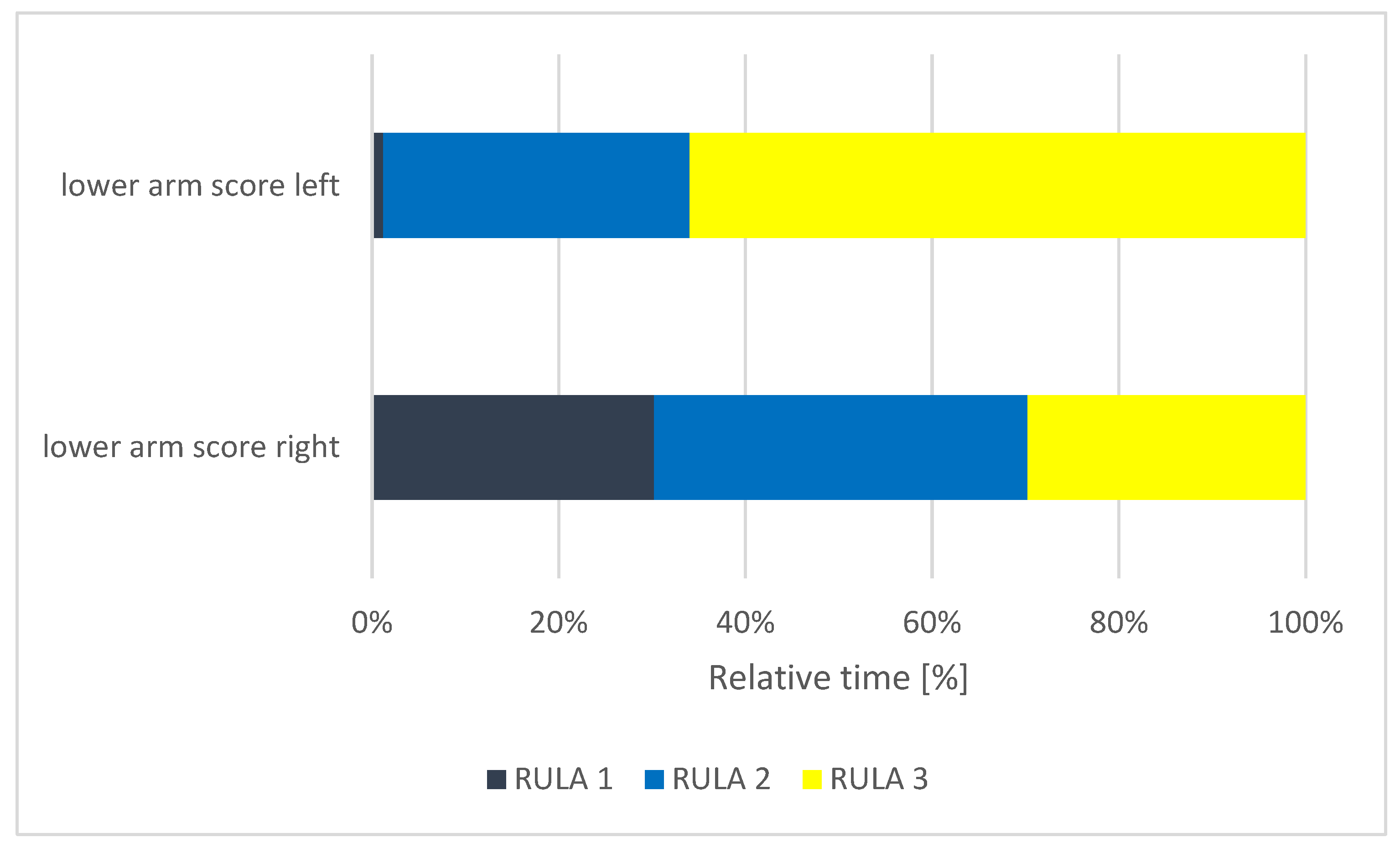
- Lower Arm Score (left and right) - RULA Step 2
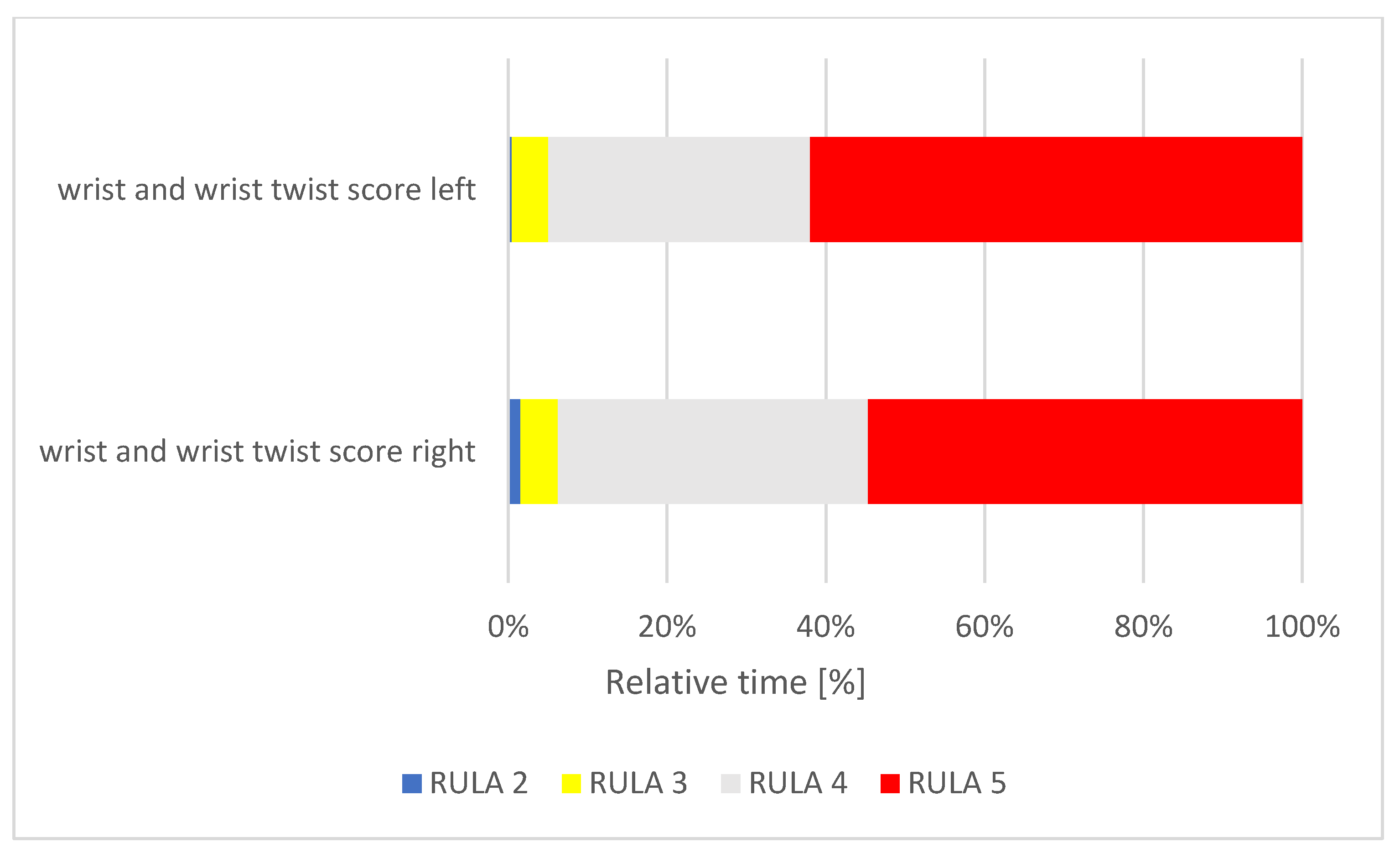
- Wrist Score (left and right) - RULA Step 3 + 4
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alghadir, A.; Zafar, H.; Iqbal, Z.A. Work-related musculoskeletal disorders among dental professionals in Saudi Arabia. J. Phys. Ther. Sci. 2015, 27, 1107–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopinadh, A.; Devi, K.N.N.; Chiramana, S.; Manne, P.; Sampath, A.; Babu, M.S. Ergonomics and musculoskeletal disorder: As an occupational hazard in dentistry. J. Contemp. Dent. Pract. 2013, 14, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.M.; Sahitya, S.; Penmetsa, G.S.; Supraja, S.; Kengadaran, S.; Chaitanya, A. Assessment of knowledge, attitude, and practice related to ergonomics among the students of three different dental schools in India: An original research. J. Educ. Health Promot. 2020, 9, 266. [Google Scholar] [CrossRef] [PubMed]
- Rafie, F.; Zamani Jam, A.; Shahravan, A.; Raoof, M.; Eskandarizadeh, A. Prevalence of upper extremity musculoskeletal disorders in dentists: Symptoms and risk factors. J. Environ. Public Health 2015, 2015, 517346. [Google Scholar] [CrossRef] [PubMed]
- Dajpratham, P.; Ploypetch, T.; Kiattavorncharoen, S.; Boonsiriseth, K. Prevalence and associated factors of musculoskeletal pain among the dental personnel in a dental school. J. Med. Assoc. Thai. 2010, 93, 714–721. [Google Scholar]
- Fe, B. The occupational hazards in dental practice. Oral Hyg. 1946, 36, 1194–1201. [Google Scholar]
- Diaz-Caballero, A.-J.; Gómez-Palencia, I.-P.; Díaz-Cárdenas, S. Ergonomic factors that cause the presence of pain muscle in students of dentistry. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e906–e911. [Google Scholar] [CrossRef] [Green Version]
- Dable, R.A.; Wasnik, P.B.; Yeshwante, B.J.; Musani, S.I.; Patil, A.K.; Nagmode, S.N. Postural assessment of students evaluating the need of ergonomic seat and magnification in dentistry. J. Indian Prosthodont. Soc. 2014, 14, 51–58. [Google Scholar] [CrossRef]
- Aghahi, R.H.; Darabi, R.; Hashemipour, M.A. Neck, back, and shoulder pains and ergonomic factors among dental students. J. Educ. Health Promot. 2018, 7, 40. [Google Scholar] [CrossRef]
- Botta, A.C.; Presoto, C.D.; Wajngarten, D.; Campos, J.A.D.B.; Garcia, P.P.N.S. Perception of dental students on risk factors of musculoskeletal disorders. Eur. J. Dent. Educ. 2018, 22, 209–214. [Google Scholar] [CrossRef]
- Santucci, N.M.; Jellin, J.; Davenport, T.E. Dental and physical therapy faculty collaborate in assessing and educating dental students on musculoskeletal disorders. J. Dent. Educ. 2021, 85, 53–59. [Google Scholar] [CrossRef]
- Ng, A.; Hayes, M.J.; Polster, A. Musculoskeletal disorders and working posture among dental and oral health students. Healthcare 2016, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, M.; Cockrell, D.; Smith, D.R. A systematic review of musculoskeletal disorders among dental professionals. Int. J. Dent. Hyg. 2009, 7, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Finsen, L.; Christensen, H.; Bakke, M. Musculoskeletal disorders among dentists and variation in dental work. Appl. Ergon. 1998, 29, 119–125. [Google Scholar] [CrossRef]
- Feng, B.; Liang, Q.; Wang, Y.; Andersen, L.L.; Szeto, G. Prevalence of work-related musculoskeletal symptoms of the neck and upper extremity among dentists in China. BMJ Open 2014, 4, e006451. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, B.P.; Singh, G.K.; Niraula, S.R. Work related complaints among dentists. JNMA J. Nepal Med. Assoc. 2008, 47, 77–81. [Google Scholar] [CrossRef]
- Aminian, O.; Banafsheh Alemohammad, Z.; Sadeghniiat-Haghighi, K. Musculoskeletal disorders in female dentists and pharmacists: A cross-sectional study. Acta Med. Iran. 2012, 50, 635–640. [Google Scholar]
- Yamalik, N. Musculoskeletal disorders (MSDs) and dental practice; part 1. General information-terminology, aetiology, work-relatedness, magnitude of the problem, and prevention. Int. Dent. J. 2006, 56, 359–366. [Google Scholar] [CrossRef]
- Blanc, D.; Farre, P.; Hamel, O. Variability of musculoskeletal strain on dentists: An electromyographic and goniometric study. Int. J. Occup. Saf. Ergon. 2014, 20, 295–307. [Google Scholar] [CrossRef]
- Leggat, P.A.; Kedjarune, U.; Smith, D.R. Occupational health problems in modern dentistry: A review. Ind. Health 2007, 45, 611–621. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.; Burke, F.J.T.; Macdonald, E.B.; Gilmour, H.; Hill, K.B.; Morris, A.J.; White, D.A.; Muirhead, E.K.; Murray, K. Dental practitioners and ill health retirement: Causes, outcomes and re-employment. Br. Dent. J. 2010, 209, E7. [Google Scholar] [CrossRef] [PubMed]
- Burke, F.J.; Main, J.R.; Freeman, R. The practice of dentistry: An assessment of reasons for premature retirement. Br. Dent. J. 1997, 182, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.B.; Burke, F.J.T.; Brown, J.; Macdonald, E.B.; Morris, A.J.; White, D.A.; Murray, K. Dental practitioners and ill health retirement: A qualitative investigation into the causes and effects. Br. Dent. J. 2010, 209, E8. [Google Scholar] [CrossRef] [Green Version]
- Aljanakh, M.; Shaikh, S.; Siddiqui, A.A.; Al-Mansour, M.; Hassan, S.S. Prevalence of musculoskeletal disorders among dentists in the Hail Region of Saudi Arabia. Ann. Saudi Med. 2015, 35, 456–461. [Google Scholar] [CrossRef]
- Aminian, O.; Alemohammad, Z.B.; Hosseini, M.H. Neck and upper extremity symptoms among male dentists and pharmacists. Work 2015, 51, 863–868. [Google Scholar] [CrossRef]
- Lietz, J.; Kozak, A.; Nienhaus, A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS ONE 2018, 13, e0208628. [Google Scholar] [CrossRef] [Green Version]
- Lietz, J.; Ulusoy, N.; Nienhaus, A. Prevention of musculoskeletal diseases and pain among dental professionals through ergonomic interventions: A systematic literature review. Int. J. Environ. Res. Public Health 2020, 17, 3482. [Google Scholar] [CrossRef]
- Ayers, K.M.S.; Thomson, W.M.; Newton, J.T.; Morgaine, K.C.; Rich, A.M. Self-reported occupational health of general dental practitioners. Occup. Med. 2009, 59, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamal, A.M.; Ahmed, D.R.M.; Habib, S.F.K.; Al-Mohareb, R.A. Ergonomics of preclinical dental students and potential musculoskeletal disorders. J. Dent. Educ. 2020, 84, 1438–1446. [Google Scholar] [CrossRef]
- Kierklo, A.; Kobus, A.; Jaworska, M.; Botuliński, B. Work-related musculoskeletal disorders among dentists—A questionnaire survey. Ann. Agric. Environ. Med. 2011, 18, 79–84. [Google Scholar] [PubMed]
- Shirzaei, M.; Mirzaei, R.; Khaje-Alizade, A.; Mohammadi, M. Evaluation of ergonomic factors and postures that cause muscle pains in dentistry students’ bodies. J. Clin. Exp. Dent. 2015, 7, e414–e418. [Google Scholar] [CrossRef] [Green Version]
- Da Neves, T.C.; Viana, L.N.; Wajngarten, D.; Garcia, P.P.N.S. Preclinical dental training: Association between difficulty in performing restorative procedures and the adoption of ergonomic posture. Eur. J. Dent. Educ. 2019, 23, 373–377. [Google Scholar] [CrossRef]
- Pejčić, N.; Petrović, V.; Đurić-Jovičić, M.; Medojević, N.; Nikodijević-Latinović, A. Analysis and prevention of ergonomic risk factors among dental students. Eur. J. Dent. Educ. 2020, 25, 460–479. [Google Scholar] [CrossRef] [PubMed]
- Movahhed, T.; Dehghani, M.; Arghami, S.; Arghami, A. Do dental students have a neutral working posture? J. Back Musculoskelet. Rehabil. 2016, 29, 859–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervera-Espert, J.; Pascual-Moscardó, A.; Camps-Alemany, I. Wrong postural hygiene and ergonomics in dental students of the University of Valencia (Spain) (part I). Eur. J. Dent. Educ. 2018, 22, e48–e56. [Google Scholar] [CrossRef] [PubMed]
- Garbin, A.J.Í.; Garbin, C.A.S.; Diniz, D.G.; Yarid, S.D. Dental students’ knowledge of ergonomic postural requirements and their application during clinical care. Eur. J. Dent. Educ. 2011, 15, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Kanaparthy, A.; Kanaparthy, R.; Boreak, N. Postural awareness among dental students in Jizan, Saudi Arabia. J. Int. Soc. Prev. Community Dent. 2015, 5, S107–S111. [Google Scholar] [CrossRef]
- Faust, A.M.; Ahmed, S.N.; Johnston, L.B.; Harmon, J.B. Teaching methodologies for improving dental students’ implementation of ergonomic operator and patient positioning. J. Dent. Educ. 2021, 85, 370–378. [Google Scholar] [CrossRef]
- Koni, A.; Kufersin, M.; Ronchese, F.; Travan, M.; Cadenaro, M.; Larese Filon, F. Approach to prevention of musculoskeletal symptoms in dental students: An interventional study. Med. Lav. 2018, 109, 276–284. [Google Scholar] [CrossRef]
- Garcia, P.P.N.S.; Gottardello, A.C.A.; Wajngarten, D.; Presoto, C.D.; Campos, J.A.D.B. Ergonomics in dentistry: Experiences of the practice by dental students. Eur. J. Dent. Educ. 2017, 21, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Rajvanshi, H.; Anshul, K.; Mali, M.; Sarin, S.; Zaidi, I.; Kumar, V.R. Ergonomics in dentistry: An ounce of prevention is better than pounds of cure: A review. Int. J. Sci. Stud. 2015, 3, 183–187. [Google Scholar]
- Middlesworth, M. RULA: Eine Schritt-für-Schritt-Anleitung. Available online: https://ergo-plus.com/wp-content/uploads/RULA-A-Step-by-Step-Guide1.pd (accessed on 26 July 2021).
- Maurer-Grubinger, C.; Holzgreve, F.; Fraeulin, L.; Betz, W.; Erbe, C.; Brueggmann, D.; Wanke, E.M.; Nienhaus, A.; Groneberg, D.A.; Ohlendorf, D. Combining ergonomic risk assessment (RULA) with inertial motion capture technology in dentistry-using the benefits from two worlds. Sensors 2021, 21, 4077. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, D.; Maltry, L.; Hänel, J.; Betz, W.; Erbe, C.; Maurer-Grubinger, C.; Holzgreve, F.; Wanke, E.M.; Brüggmann, D.; Nienhaus, A.; et al. SOPEZ: Study for the optimization of ergonomics in the dental practice—Musculoskeletal disorders in dentists and dental assistants: A study protocol. J. Occup. Med. Toxicol. 2020, 15, 22. [Google Scholar] [CrossRef]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Hoehne-Hückstädt, U.; Herda, C.; Ellegast, R.; Hermanns, I.; Hamburger, R.; Ditchen, D. Muskel-Skelett-Erkrankungen der Oberen Extremität und Berufliche Tätigkeit: Entwicklung Eines Systems zur Erfassung und Arbeitswissenschaftlichen Bewertung von Komplexen Bewegungen der Oberen Extremität bei Beruflichen Tätigkeiten; Institut für Arbeitsschutz der DGUV (IFA): Sankt Augustin, Germany, 2007. [Google Scholar]
- Vignais, N.; Miezal, M.; Bleser, G.; Mura, K.; Gorecky, D.; Marin, F. Innovative system for real-time ergonomic feedback in industrial manufacturing. Appl. Ergon. 2013, 44, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Vignais, N.; Bernard, F.; Touvenot, G.; Sagot, J.-C. Physical risk factors identification based on body sensor network combined to videotaping. Appl. Ergon. 2017, 65, 410–417. [Google Scholar] [CrossRef]
- Yousef, M.K.; Al Zain, A.O. Posture evaluation of dental students. JKAU Med. Sci. 2009, 16, 51–68. [Google Scholar] [CrossRef] [Green Version]
- Giersiepen, K.; Spallek, M. Carpal tunnel syndrome as an occupational disease. Deutsches Arzteblatt-Arztliche Mitteilungen-Ausgabe A 2011, 108, 238–242. [Google Scholar] [CrossRef]
- Sakzewski, L.; Naser-ud-Din, S. Work-related musculoskeletal disorders in dentists and orthodontists: A review of the literature. Work 2014, 48, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.-F.; Kao, Y.-H. Influence of pain location and hand dominance on scapular kinematics and EMG activities: An exploratory study. BMC Musculoskelet. Disord. 2011, 12, 267. [Google Scholar] [CrossRef] [Green Version]
- Haas, Y.; Naser, A.; Haenel, J.; Fraeulin, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; et al. Prevalence of self-reported musculoskeletal disorders of the hand and associated conducted therapy approaches among dentists and dental assistants in Germany. PLoS ONE 2020, 15, e0241564. [Google Scholar] [CrossRef] [PubMed]
- Rytkönen, E.; Sorainen, E.; Leino-Arjas, P.; Solovieva, S. Hand-arm vibration exposure of dentists. Int. Arch. Occup. Environ. Health 2006, 79, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, D.; Naser, A.; Haas, Y.; Haenel, J.; Fraeulin, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; et al. Prevalence of musculoskeletal disorders among dentists and dental students in Germany. Int. J. Environ. Res. Public Health 2020, 17, 8740. [Google Scholar] [CrossRef] [PubMed]
- Ramaswami, E.; Nimma, V.; Jakhete, A.; Lingam, A.S.; Contractor, I.; Kadam, S. Assessment of occupational hazards among dentists practicing in Mumbai. J. Family Med. Prim. Care 2020, 9, 2016–2021. [Google Scholar] [CrossRef]
- Sharma, P.; Golchha, V. Awareness among Indian dentist regarding the role of physical activity in prevention of work related musculoskeletal disorders. Indian J. Dent. Res. 2011, 22, 381–384. [Google Scholar] [CrossRef]
- Meyer, V.P.; Micheelis, W. Arbeitsbelastungen bei Zahnärzten in Niedergelassener Praxis: Eine Arbeitsmedizinische Bestandsaufnahme zu Wirbelsäulenbelastungen, Berufsdermatosen und Stressfaktoren; Deutscher Zahnärzte Verlag DÄV-Hanser: Köln, Germany, 2001; ISBN 3934280242. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Personal Characteristics | DSs * | DAs * |
|---|---|---|
| Sex | ||
| Female | 12 (80%) | 13 (86.7%) |
| Male | 3 (20%) | 2 (13.3%) |
| Median age (years) | 27 (2.5) | 21.5 (4) |
| Median height (cm) | 170 (18) | 165.5 (6.25) |
| Median body weight (kg) | 68 (14.5) | 59 (8) |
| Handedness | ||
| Right | 15 (100%) | 15 (100%) |
| Left | 0 (0%) | 0 (0%) |
| Task | Quadrant 1 | Quadrant 2 | Quadrant 3 | Quadrant 4 | |
|---|---|---|---|---|---|
| General Dentistry/Students | Tooth filling of tooth 16 | Preparation of tooth 26 for crown uptake | Root canal treatment on tooth 35 | Tartar removal in the 4th quadrant | |
| 1 | Prepare tooth cavity with a cylindrical diamond bur and the use of wedges | Occlusal reduction using an occlusal reducer | Perform an entrance cavity and trepanation on tooth 35 using a diamond-coated cylinder | Removal of supra- and subgingival tartar/calculus using scalers an curettes | |
| 2 | Create a Tofflemire die using a die clamp | Chamfer preparation using a torpedo-shaped diamond burand approximal reducer | Find the channel entrance using an endo file | ||
| 3 | Tooth filling with ketac® while using a ketac®-set and a cougar/heidemann | Manual preparation of the canal using an ISO 20–40 endo file with regular irrigation using a irrigation cannula |
| Worksheet-Steps | Parameters | Modifications of the RULA Parameters | Additional Information |
|---|---|---|---|
| STEP 1 | Leaning arm | Since the arms of the dental students were not supported at any time, 0 was given as the score of the leaning arm. | |
| STEP 3 | Wrist is bent laterally | If the lateral bend of the wrist was less than −10° (radial deviation) or more than 10° (ulnar deviation), +1 was added to the wrist score. | The RULA score does not show how much the wrists need to be bent. |
| STEP 4 | Wrist twist | If the wrist twist was in the neutral range (45° to −45°), +1 was added to the wrist twist score. If the turn of the wrist was close to the terminal range of motion (90° to 45° and −45° to −90°), +2 was added to the wrist twist score. | The RULA score does not show how much the wrists need to be twisted. |
| STEP 6 | Muscle use score of arm and wrist | The score was increased by +1 for static or repetitive muscle work. - Muscle work was classified as static if the difference in angular velocity of the shoulder joint at the beginning and end was ≥7.5 for longer than 10 s [48]. - Muscle work was classified as repetitive if the movement of the joint indicated more than 0.5 Hz mean power frequency [48]. For this purpose, extension and flexion of the wrist, as well as forearm rotation, were taken into account. | The given scores from the RULA table were transformed into continuous recordings. |
| STEP 9 + 10 | Twist trunk and neck | If a rotation of the neck or trunk was deduced to be inferior to −10° or superior to 10°, a score of +1 was added to the ‘neck score’ or ‘trunk score’. | In order to determine the exact extent of the movement, certain scores were added. |
| STEP 9 + 10 | Side bending trunk and neck | If the neck or torso inclination (in the frontal plane) was more than +10° or less than −10°, +1 was added to the neck or torso score. | In order to determine the exact extent of the movement, certain scores were added. |
| STEP 11 | Supported legs and feet | As the legs and feet of the dental students were permanently supported by their sedentary work, +1 was given as the supported leg score. | |
| STEP 13 | Muscle use score of neck, trunk and legs | The score was increased by +1 for static or repetitive muscle work. Muscle work was classified as static if the difference in angular velocity of the neck/cervical spine and lower back/lumbar spine was ≥7.5 at the beginning and at the end for longer than 10 s. - Muscle work was classified as repetitive if the movement in any of the degrees of freedom of the joint indicated above 0.5 Hz mean power frequency. | |
| STEP 14 | Force/load score | Since all dental instruments weighed less than 2 kg, this score was set to 0 [48]. |
| RULA Score | Median (IQR)/Max. Score | Relative Time Score | ERP |
|---|---|---|---|
| Final Score | 7 (0)/7 | 6.67 | 0.95 |
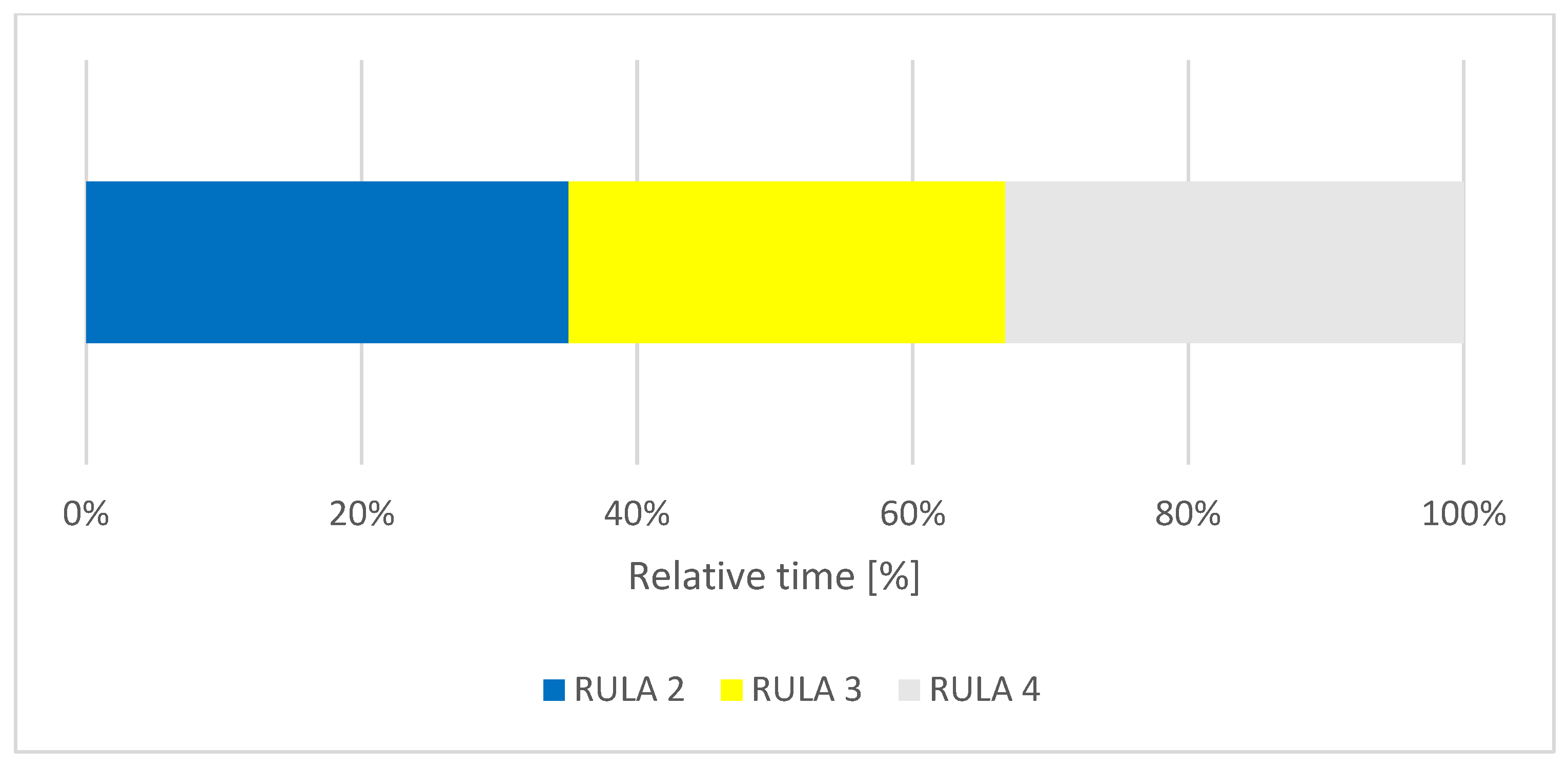
| Trunk Score | 3 (2)/6 | 2.74 | 0.46 |
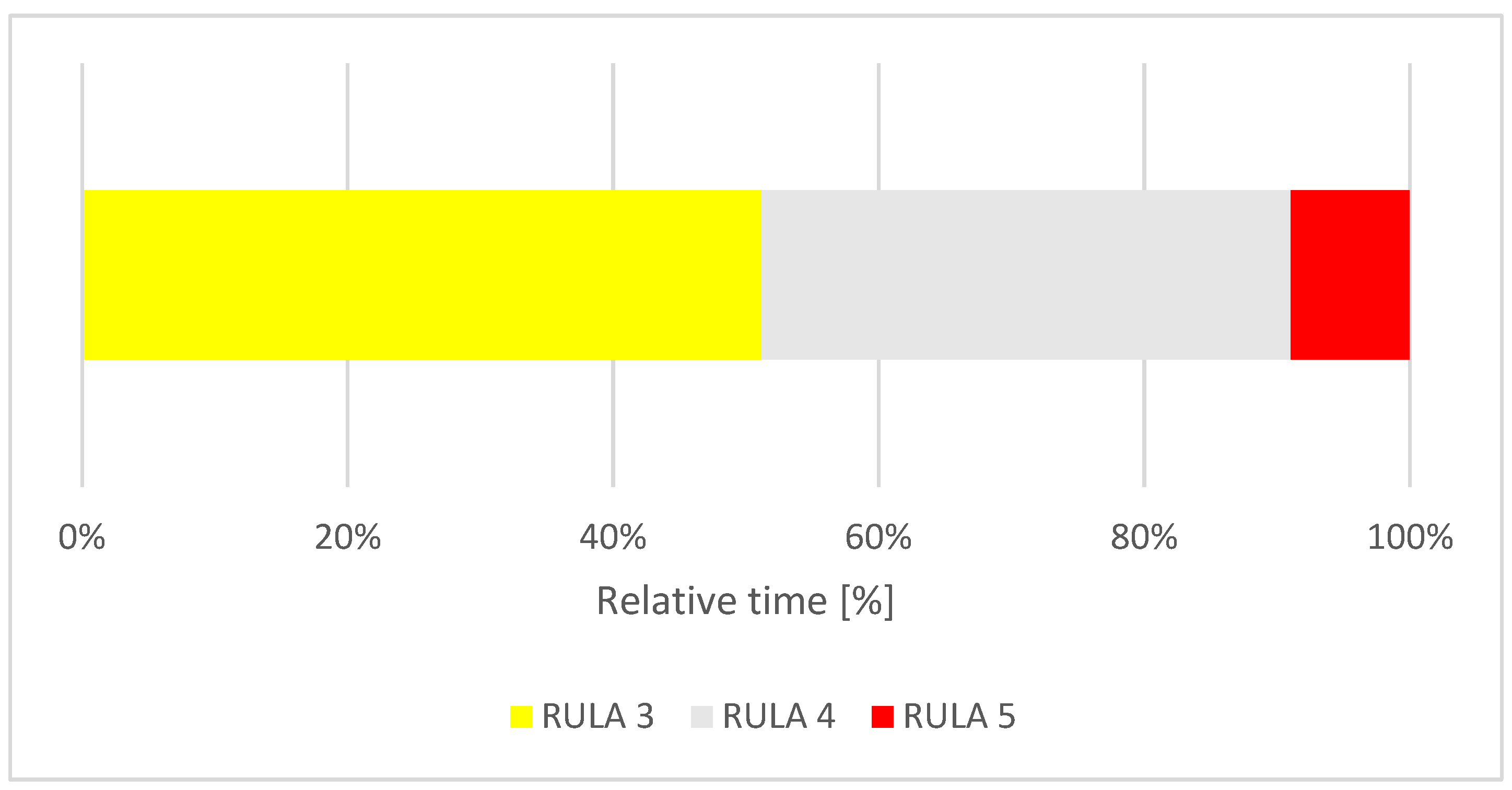
| Neck Score | 4 (1)/6 | 3.15 | 0.53 |
| Right Wrist Score | 4 (1)/6 | 4.06 | 0.68 |
| Right Lower Arm Score | 2 (2)/3 | 1.96 | 0.65 |
| Right Upper Arm Score | 2 (1)/6 | 1.82 | 0.30 |
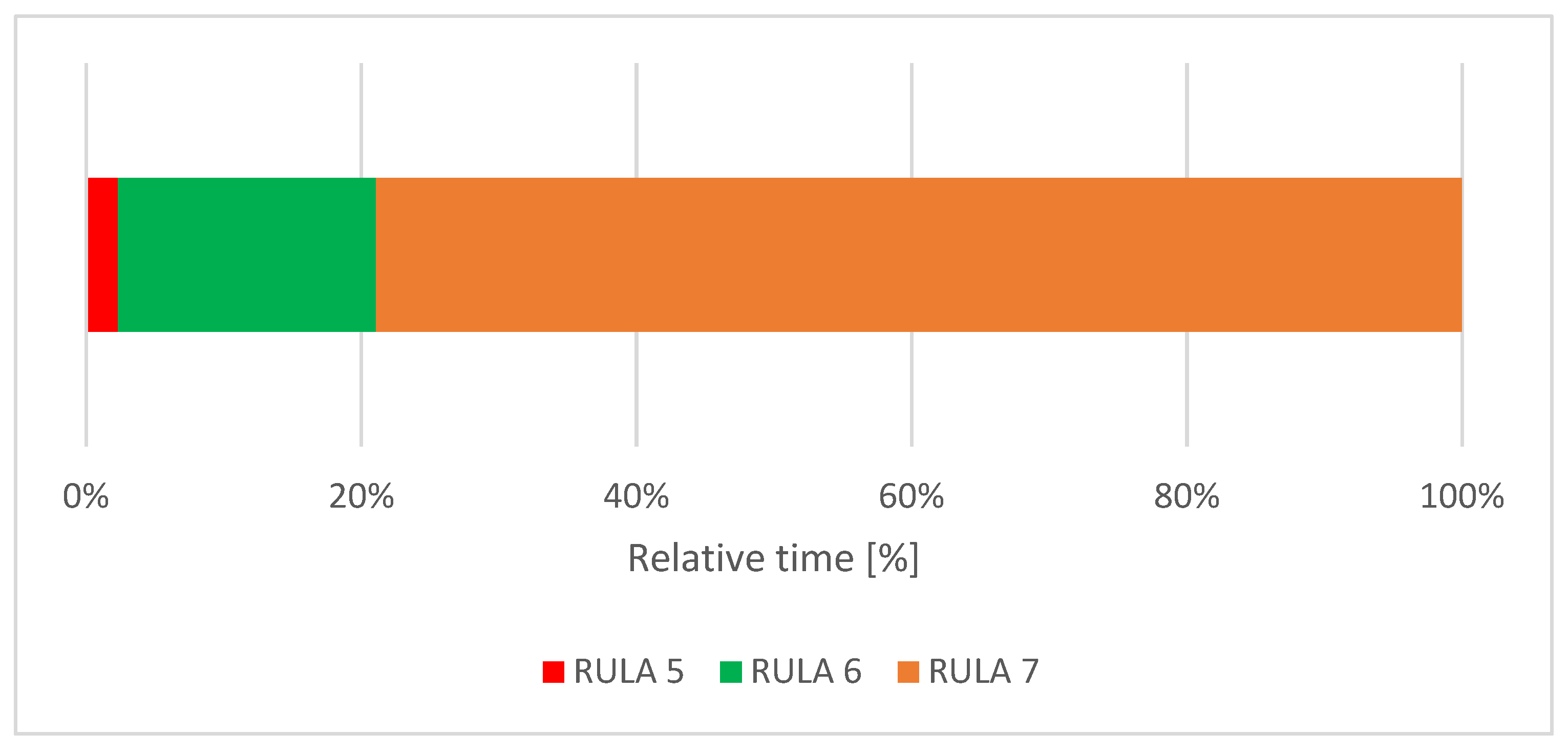
| Left Wrist Score | 5 (1)/6 | 4.66 | 0.78 |
| Left Lower Arm Score | 3 (1)/3 | 2.53 | 0.84 |
| Left Upper Arm Score | 1 (0)/6 | 1.21 | 0.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blume, K.S.; Holzgreve, F.; Fraeulin, L.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; Maurer-Grubinger, C.; Groneberg, D.A.; et al. Ergonomic Risk Assessment of Dental Students—RULA Applied to Objective Kinematic Data. Int. J. Environ. Res. Public Health 2021, 18, 10550. https://doi.org/10.3390/ijerph181910550
Blume KS, Holzgreve F, Fraeulin L, Erbe C, Betz W, Wanke EM, Brueggmann D, Nienhaus A, Maurer-Grubinger C, Groneberg DA, et al. Ergonomic Risk Assessment of Dental Students—RULA Applied to Objective Kinematic Data. International Journal of Environmental Research and Public Health. 2021; 18(19):10550. https://doi.org/10.3390/ijerph181910550
Chicago/Turabian StyleBlume, Kim Sarah, Fabian Holzgreve, Laura Fraeulin, Christina Erbe, Werner Betz, Eileen M. Wanke, Doerthe Brueggmann, Albert Nienhaus, Christian Maurer-Grubinger, David A. Groneberg, and et al. 2021. "Ergonomic Risk Assessment of Dental Students—RULA Applied to Objective Kinematic Data" International Journal of Environmental Research and Public Health 18, no. 19: 10550. https://doi.org/10.3390/ijerph181910550
APA StyleBlume, K. S., Holzgreve, F., Fraeulin, L., Erbe, C., Betz, W., Wanke, E. M., Brueggmann, D., Nienhaus, A., Maurer-Grubinger, C., Groneberg, D. A., & Ohlendorf, D. (2021). Ergonomic Risk Assessment of Dental Students—RULA Applied to Objective Kinematic Data. International Journal of Environmental Research and Public Health, 18(19), 10550. https://doi.org/10.3390/ijerph181910550