
Intravenous Tranexamic Acid Reduces Blood Loss and Transfusion Volume in Scoliosis Surgery for Spinal Muscular Atrophy: Results of a 20-Year Retrospective Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment
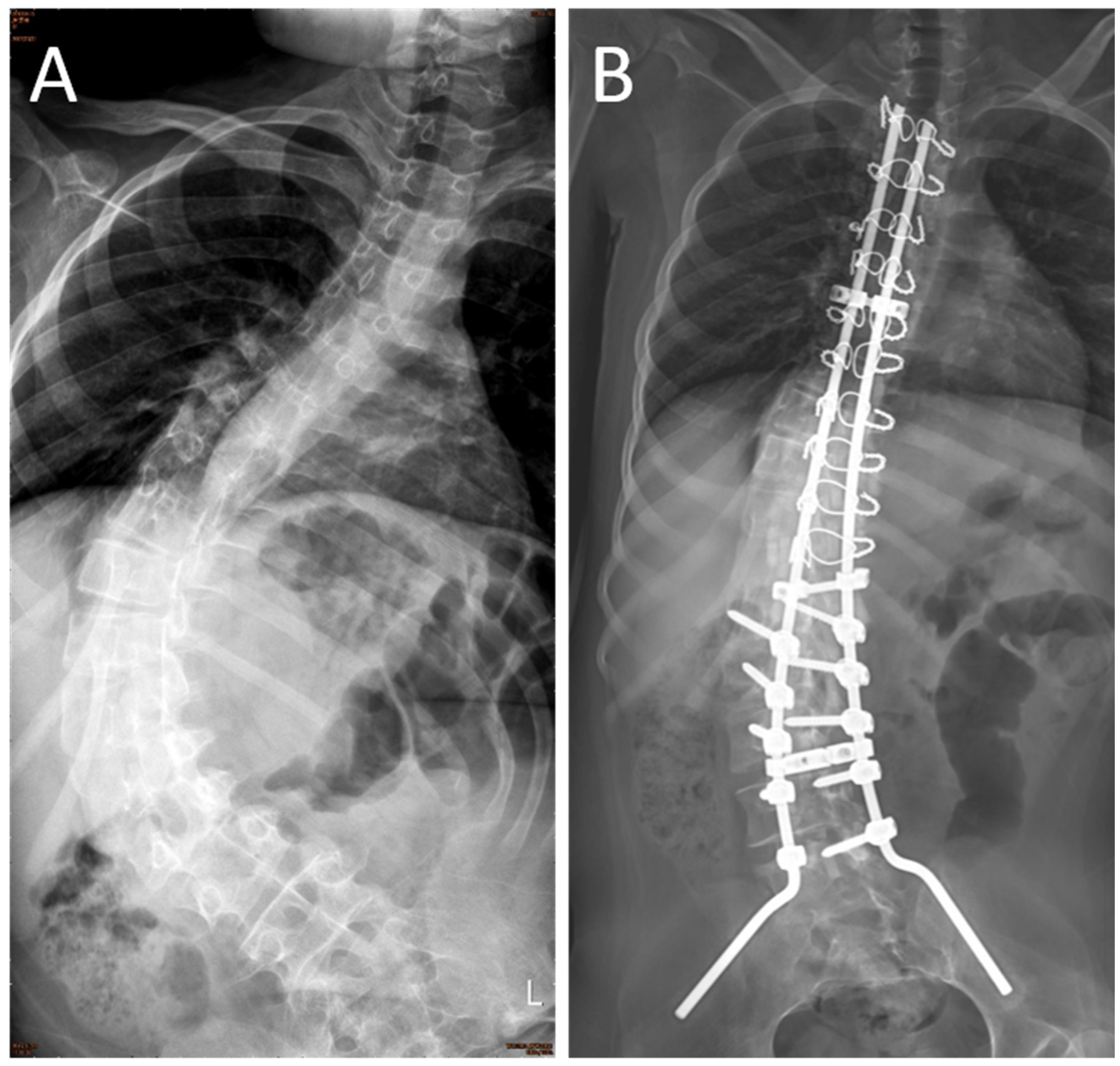
2.3. Surgical Procedure
2.4. Postoperative Course
2.5. Drug Dose
2.6. Statistical Analysis
3. Results
3.1. Intraoperative Blood Loss
3.2. Intraoperative Blood and Fluid Transfusion Volume
3.3. Intubation Time and Pulmonary Complication Rate
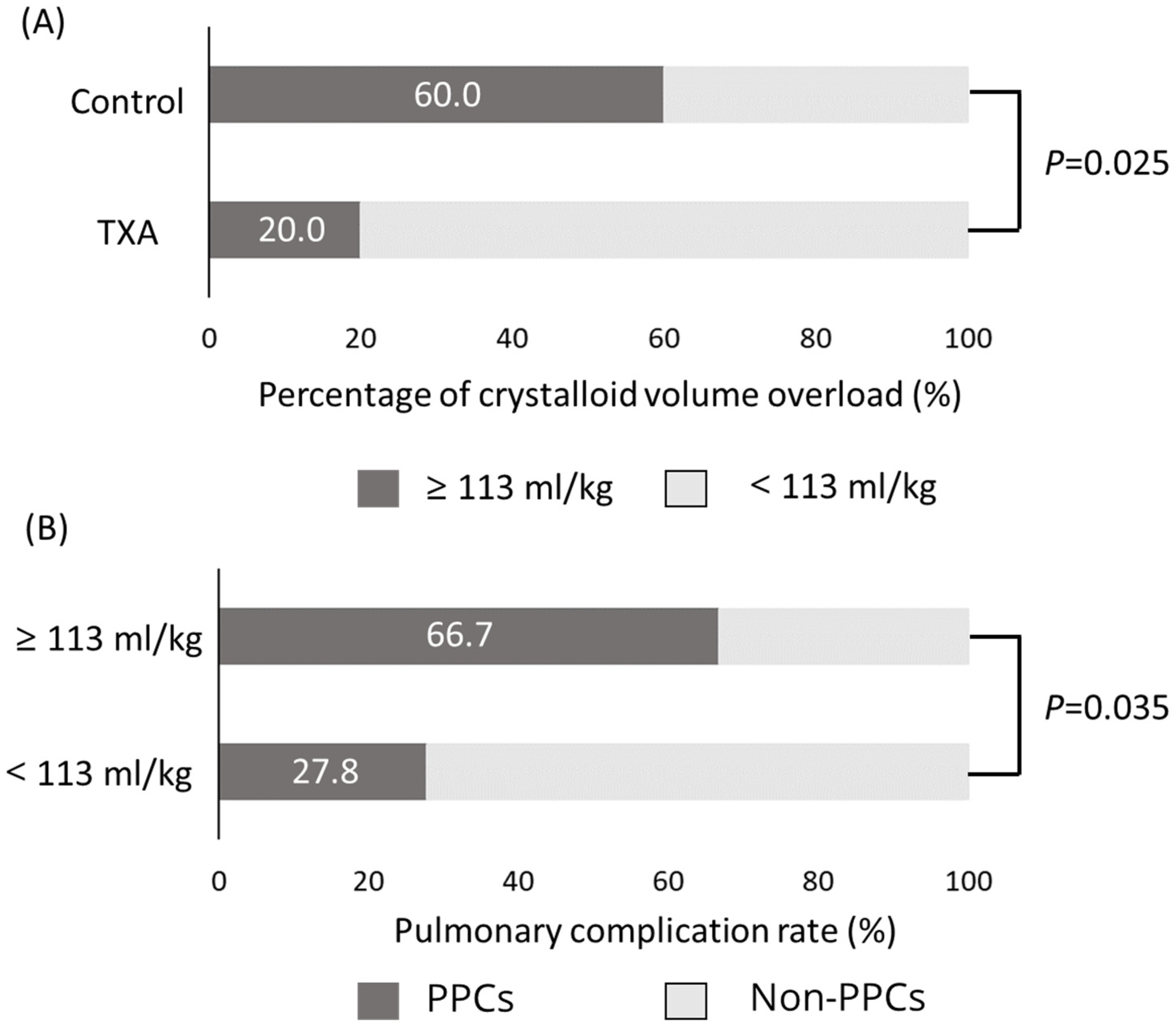
3.4. Crystalloid Volume Overload and Pulmonary Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lunn, M.R.; Wang, C.H. Spinal muscular atrophy. Lancet 2008, 371, 2120–2133. [Google Scholar] [CrossRef]
- Piazzolla, A.; Solarino, G.; De Giorgi, S.; Mori, C.M.; Moretti, L.; De Giorgi, G. Cotrel-Dubousset instrumentation in neuromuscular scoliosis. Eur. Spine J. 2011, 20, S75–S84. [Google Scholar] [CrossRef] [Green Version]
- Garg, S. Management of scoliosis in patients with Duchenne muscular dystrophy and spinal muscular atrophy: A literature review. J. Pediatr. Rehabil. Med. 2016, 9, 23–29. [Google Scholar] [CrossRef]
- Brooks, J.T.; Sponseller, P.D. What’s new in the management of neuromuscular scoliosis. J. Pediatr. Orthop. 2016, 36, 627–633. [Google Scholar] [CrossRef]
- Chou, S.H.; Lin, G.T.; Shen, P.C.; Lue, Y.J.; Lu, C.C.; Tien, Y.C.; Lu, Y.M. The effect of scoliosis surgery on pulmonary function in spinal muscular atrophy type II patients. Eur. Spine J. 2017, 26, 1721–1731. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, F.; Sethna, N. Blood loss in pediatric spine surgery. Eur. Spine J. 2004, 13, S6–S17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannan, S.; Meert, K.L.; Mooney, J.F.; Hillman-Wiseman, C.; Warrier, I. Bleeding and coagulation changes during spinal fusion surgery: A comparison of neuromuscular and idiopathic scoliosis patients. Pediatr. Crit. Care Med. 2002, 3, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Dhawale, A.A.; Shah, S.A.; Sponseller, P.D.; Bastrom, T.; Neiss, G.; Yorgova, P.; Newton, P.O.; Yaszay, B.; Abel, M.F.; Shufflebarger, H.; et al. Are antifibrinolytics helpful in decreasing blood loss and transfusions during spinal fusion surgery in children with cerebral palsy scoliosis? Spine (Phila Pa 1976) 2012, 37, E549–E555. [Google Scholar] [CrossRef] [PubMed]
- McLeod, L.M.; French, B.; Flynn, J.M.; Dormans, J.P.; Keren, R. Antifibrinolytic use and blood transfusions in pediatric scoliosis surgeries performed at US children's hospitals. J. Spinal Disord. Tech. 2015, 28, E460–E466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edler, A.; Murray, D.J.; Forbes, R.B. Blood loss during posterior spinal fusion surgery in patients with neuromuscular disease: Is there an increased risk? Paediatr. Anaesth. 2003, 13, 818–822. [Google Scholar] [CrossRef]
- Jia, R.; Li, N.; Xu, B.Y.; Zhang, W.; Gu, X.P.; Ma, Z.L. Incidence, influencing factors, and prognostic impact of intraoperative massive blood loss in adolescents with neuromuscular scoliosis: A STROBE-compliant retrospective observational analysis. Medicine (Baltim.) 2017, 96, e6292. [Google Scholar] [CrossRef] [PubMed]
- Toll, B.J.; Samdani, A.F.; Janjua, M.B.; Gandhi, S.; Pahys, J.M.; Hwang, S.W. Perioperative complications and risk factors in neuromuscular scoliosis surgery. J. Neurosurg. Pediatr. 2018, 22, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, P.M. Hemostatic drugs. N. Engl. J. Med. 1998, 339, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Li, H.; Wang, D.; He, X.; Zhang, C.; Yang, P. Systematic review and meta-analysis of perioperative intravenous tranexamic acid use in spinal surgery. PLoS ONE 2013, 8, e55436. [Google Scholar]
- Neilipovitz, D.T.; Murto, K.; Hall, L.; Barrowman, N.J.; Splinter, W.M. A randomized trial of tranexamic acid to reduce blood transfusion for scoliosis surgery. Anesth. Analg. 2001, 93, 82–87. [Google Scholar] [CrossRef]
- Lykissas, M.G.; Crawford, A.H.; Chan, G.; Aronson, L.A.; Al-Sayyad, M.J. The effect of tranexamic acid in blood loss and transfusion volume in adolescent idiopathic scoliosis surgery: A single-surgeon experience. J. Child. Orthop. 2013, 7, 245–249. [Google Scholar] [CrossRef] [Green Version]
- Verma, K.; Errico, T.; Diefenbach, C.; Hoelscher, C.; Peters, A.; Dryer, J.; Huncke, T.; Boenigk, K.; Lonner, B.S. The relative efficacy of antifibrinolytics in adolescent idiopathic scoliosis: A prospective randomized trial. J. Bone Joint Surg. Am. 2014, 96, e80. [Google Scholar] [CrossRef]
- Shapiro, F.; Zurakowski, D.; Sethna, N.F. Tranexamic acid diminishes intraoperative blood loss and transfusion in spinal fusions for duchenne muscular dystrophy scoliosis. Spine (Phila Pa 1976) 2007, 32, 2278–2283. [Google Scholar] [CrossRef]
- Sethna, N.F.; Zurakowski, D.; Brustowicz, R.M.; Bacsik, J.; Sullivan, L.J.; Shapiro, F. Tranexamic acid reduces intraoperative blood loss in pediatric patients undergoing scoliosis surgery. Anesthesiology 2005, 102, 727–732. [Google Scholar] [CrossRef]
- Brecher, M.E.; Monk, T.; Goodnough, L.T. A standardized method for calculating blood loss. Transfusion 1997, 37, 1070–1074. [Google Scholar] [CrossRef]
- Meert, K.L.; Kannan, S.; Mooney, J.F. Predictors of red cell transfusion in children and adolescents undergoing spinal fusion surgery. Spine (Phila Pa 1976) 2002, 27, 2137–2142. [Google Scholar] [CrossRef] [PubMed]
- Schuster, J.M.; Rechtine, G.; Norvell, D.C.; Dettori, J.R. The influence of perioperative risk factors and therapeutic interventions on infection rates after spine surgery: A systematic review. Spine (Phila Pa 1976) 2010, 35, S125–S137. [Google Scholar] [CrossRef] [PubMed]
- Leighton, J.L.; You, D.; Schneider, P. Limiting blood loss in orthopaedic trauma. Strategies and effect. Injury 2020, 51, S123–S127. [Google Scholar] [CrossRef] [PubMed]
- Balvers, K.; van Dieren, S.; Basksaas-Asen, K.; Gaarder, C.; Brohi, K.; Eaglestone, S.; Stanworth, S.; Johansson, P.J.; Ostrowski, S.R.; Stensballe, J.; et al. Combined effect of therapeutic strategies for bleeding injury on early survival, transfusion needs and correction of coagulopathy. Br. J. Surg. 2017, 104, 222–229. [Google Scholar] [CrossRef]
- Schrier, R.W.; Wang, W. Acute renal failure and sepsis. N. Engl. J. Med. 2004, 351, 159–169. [Google Scholar] [CrossRef]
- Cordemans, C.; De Laet, I.; Van Regenmortel, N.; Schoonheydt, K.; Dits, H.; Huber, W.; Malbrain, M.L. Fluid management in critically ill patients: The role of extravascular lung water, abdominal hypertension, capillary leak, and fluid balance. Ann. Intensive Care 2012, 2, S1. [Google Scholar] [CrossRef] [Green Version]
- Myburgh, J.A.; Mythen, M.G. Resuscitation fluids. N. Engl. J. Med. 2013, 369, 1243–1251. [Google Scholar] [CrossRef]
- Anastasian, Z.H.; Gaudet, J.G.; Levitt, L.C.; Mergeche, J.L.; Heyer, E.J.; Berman, M.F. Factors that correlate with the decision to delay extubation after multilevel prone spine surgery. J. Neurosurg. Anesthesiol. 2014, 26, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Xiao, H.; Wang, R.; Huang, Y. Prediction of massive blood loss in scoliosis surgery from preoperative variables. Spine (Phila Pa 1976) 2013, 38, 350–355. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control Group (n = 15) | TXA Group (n = 15) | p-Value | |
|---|---|---|---|
| Age (years) | 14.5 ± 5.5 | 12.7 ± 5.6 | 0.233 a |
| Sex (Female: Man) SMA II:SMAIII | 9:6 12:3 | 10:5 12:3 | 0.583 a 1.000 a |
| Height (cm) | 148.6 ± 14.2 | 150.1 ± 12.6 | 0.769 a |
| Weight (kg) | 33.1 ± 8.6 | 39.6 ± 12.8 | 0.171 a |
| Hematocrit (%) | 39.4 ± 3.2 | 41.7 ± 3.5 | 0.067 b |
| Coagulation profile | |||
| Platelet (×103) | 313.7 ± 72.3 | 321.9 ± 58.3 | 0.735 b |
| PT (Sec) | 11.6 ± 0.7 | 11.0 ± 1.0 | 0.071 b |
| aPTT (Sec) | 31.9 ± 4.5 | 29.5 ± 2.4 | 0.077 b |
| INR | 0.96 ± 0.08 | 1.00 ± 0.06 | 0.128 b |
| Scoliosis major curve | |||
| Preoperative Cobb’s | 77.1 ± 29.1 | 70.3 ± 22.8 | 0.595 a |
| Postoperative Cobb’s | 29.6 ± 19.6 | 22.0 ± 14.2 | 0.250 a |
| Correction (°) | 46.3 ± 14.5 | 48.3 ± 14.0 | 0.567 a |
| Correction rate (%) | 60.8 ± 14.0 | 70.0 ± 12.9 | 0.072 b |
| Surgical time (h) | 9.0 ± 1.6 | 8.7 ± 1.3 | 0.461 a |
| Control Group (n = 15) | TXA Group (n = 15) | p-Value | |
|---|---|---|---|
| EBL (mL) | 2023.8 ± 1673.4 | 1327.0 ± 685.2 | 0.174 |
| TBVL (%) | 106.7 ± 95.0 | 52.1 ± 17.8 | 0.011 * |
| Intraoperative supplement | |||
| Blood transfusion | |||
| volume (mL) | 1250.0 ± 1052.2 | 498.7 ± 158.4 | <0.001 * |
| relative volume (mL/kg) | 43.3 ± 40.5 | 13.4 ± 4.2 | <0.001 * |
| Crystalloid | |||
| volume (mL) | 4154.0 ± 1530.9 | 3058.0 ± 836.2 | 0.041 * |
| relative volume (mL/kg) | 144.1 ± 57.5 | 82.2 ± 24.4 | <0.001 * |
| Total transfusion | |||
| volume (mL) | 5404.0 ± 2308.5 | 3523.4 ± 890.2 | 0.005 * |
| relative volume (mL/kg) | 187.4 ± 91.2 | 95.2 ± 26.4 | <0.001 * |
| Postoperative care | |||
| Intubation time (h) | 52.8 ± 58.5 | 19.1 ± 12.9 | 0.106 |
| Postoperative complications | |||
| Wound infection | 0 | 1 | |
| VTE | 0 | 0 | |
| Pulmonary complications | 8 (8/15 = 53.3%) | 5 (5/15 = 33.3%) | 0.269 |
| Pneumonia + pulmonary edema | 6 | 2 # | |
| Pulmonary edema | 1 | 2 | |
| Atelectasis | 1 | 1 | |
| Pulmonary Complication (n = 13) | Non-Pulmonary Complication (n = 17) | p-Value | |
|---|---|---|---|
| EBL (mL) | 1688.62 ± 1596.0 | 1665.3 ± 1085.4 | 0.869 |
| TBVL (%) | 95.2 ± 103.5 | 67.3 ± 34.4 | 0.680 |
| Intraoperative supplement | |||
| Crystalloid | |||
| volume (mL) | 4109.2 ± 1578.4 | 3221.2 ± 997.0 | 0.113 |
| relative volume (mL/kg) | 142.2 ± 62.7 | 90.9 ± 32.4 | 0.003 * |
| Total transfusion | |||
| volume (mL) | 4987.2 ± 2507.3 | 4065.6 ± 1382.4 | 0.263 |
| relative volume (mL/kg) | 176.6 ± 103.7 | 114.3 ± 44.9 | 0.022 * |
| Postoperative care | |||
| Intubation time (h) | 57.5 ± 61.6 | 19.4 ± 12.5 | 0.183 |
| This Study | Neilipovitz et al. [15] | Sethna et al. [19] | Shapiro et al. [18] | Dhawale et al. [8] | |
|---|---|---|---|---|---|
| Disease | SMA | miscellaneous | miscellaneous | DMD | CP |
| Number(s) | 30 | unknown | 22 | 56 | 70 |
| Reduced blood loss | 51% * | 10% | 48% * | 58% * | 51.5% * |
| Reduced blood transfusion | 60% * | 30% * | 42% * | 46% * | 12.5% |
| Reduced crystalloid volume | 26% * | 12.3% | undescribed | undescribed | undescribed |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, S.-H.; Lin, S.-Y.; Wu, M.-H.; Tien, Y.-C.; Jong, Y.-J.; Liang, W.-C.; Lu, Y.-M.; Shih, C.-L.; Lu, C.-C. Intravenous Tranexamic Acid Reduces Blood Loss and Transfusion Volume in Scoliosis Surgery for Spinal Muscular Atrophy: Results of a 20-Year Retrospective Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9959. https://doi.org/10.3390/ijerph18199959
Chou S-H, Lin S-Y, Wu M-H, Tien Y-C, Jong Y-J, Liang W-C, Lu Y-M, Shih C-L, Lu C-C. Intravenous Tranexamic Acid Reduces Blood Loss and Transfusion Volume in Scoliosis Surgery for Spinal Muscular Atrophy: Results of a 20-Year Retrospective Analysis. International Journal of Environmental Research and Public Health. 2021; 18(19):9959. https://doi.org/10.3390/ijerph18199959
Chicago/Turabian StyleChou, Shih-Hsiang, Sung-Yen Lin, Meng-Huang Wu, Yin-Chun Tien, Yuh-Jyh Jong, Wen-Chen Liang, Yen-Mou Lu, Chia-Lung Shih, and Cheng-Chang Lu. 2021. "Intravenous Tranexamic Acid Reduces Blood Loss and Transfusion Volume in Scoliosis Surgery for Spinal Muscular Atrophy: Results of a 20-Year Retrospective Analysis" International Journal of Environmental Research and Public Health 18, no. 19: 9959. https://doi.org/10.3390/ijerph18199959
APA StyleChou, S. -H., Lin, S. -Y., Wu, M. -H., Tien, Y. -C., Jong, Y. -J., Liang, W. -C., Lu, Y. -M., Shih, C. -L., & Lu, C. -C. (2021). Intravenous Tranexamic Acid Reduces Blood Loss and Transfusion Volume in Scoliosis Surgery for Spinal Muscular Atrophy: Results of a 20-Year Retrospective Analysis. International Journal of Environmental Research and Public Health, 18(19), 9959. https://doi.org/10.3390/ijerph18199959