Organizational and Individual Outcomes of Health Promotion Strategies—A Review of Empirical Research



Abstract
:1. Introduction
- Q1: In what types of enterprises are the outcomes of WHPI examined and measured most often?
- Q2: What research methods are used to measure the outcomes of WHPI?
- Q3: What types of outcomes of WHPI are reported by organizations?
- Q4: How often has research indicated strong evidence data confirming the effectiveness of WHPI?
2. Literature Review
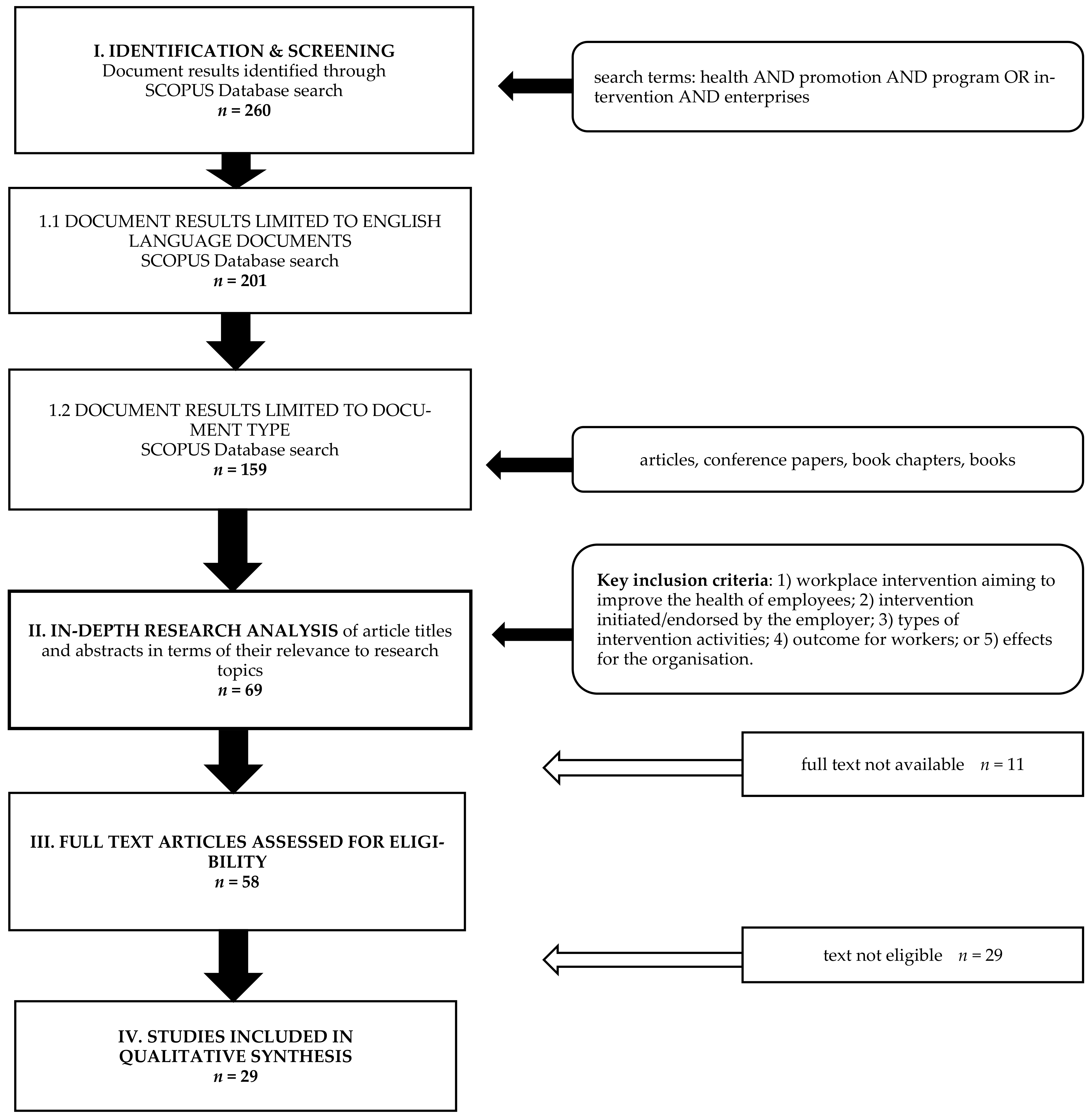
3. Materials and Methods
- The identification of size and type of organization and the country in which the research was conducted.
- The analysis of type and duration of the WHPI.
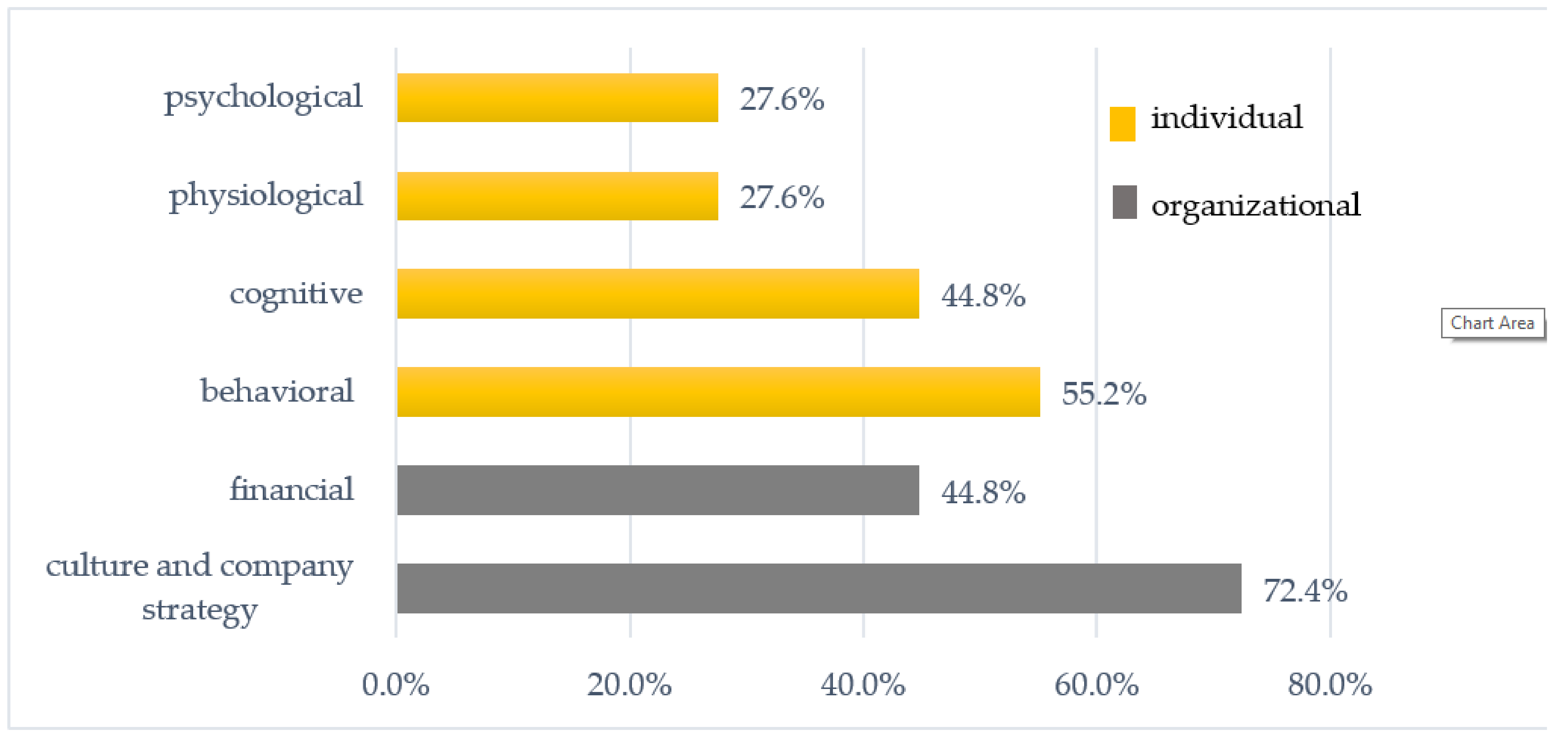
- The identification and classification of outcomes indicated in the tests. Based on Sorensen’s model (see Figure 2), two types of organizational and four types of individual categories of outcome were identified. The categories used are not disjunctive, which means that in one research paper, the same and different types of outcomes could be identified.
- The identification of the research methodology used to present the results of WHPIs. In particular, the method, sample size, tools, and frequency of outcome measurement were considered.
- Level of evaluation carried out: Process, structure, and outcomes were taken into consideration.
- The analysis and evaluation of strong evidence data confirming the effectiveness of WHPIs was conducted based on nine criteria/questions:
- Were quasi-experimental methods or randomly controlled cluster trials or cross-sectorial studies used in the study to confirm the effectiveness of WHPI?
- Was the WHPI effectiveness measurement carried out at least twice (at baseline and after intervention)?
- Was the WHPI effectiveness measurement repeated after a certain period of time after the end of the intervention to check the durability of its effects? After what period of time?
- Were objectified research tools used in the study?
- When assessing the effectiveness of the WHPI, was the structure or process examined in addition to the outcomes as well?
- Was the WHPI effect to modify unhealthy habits and improve the risk profile of employees, especially the highest risk groups?
- Was the WHPI effect an organizational change?
- Did the WHPI result in financial benefits for the organization?
4. Results
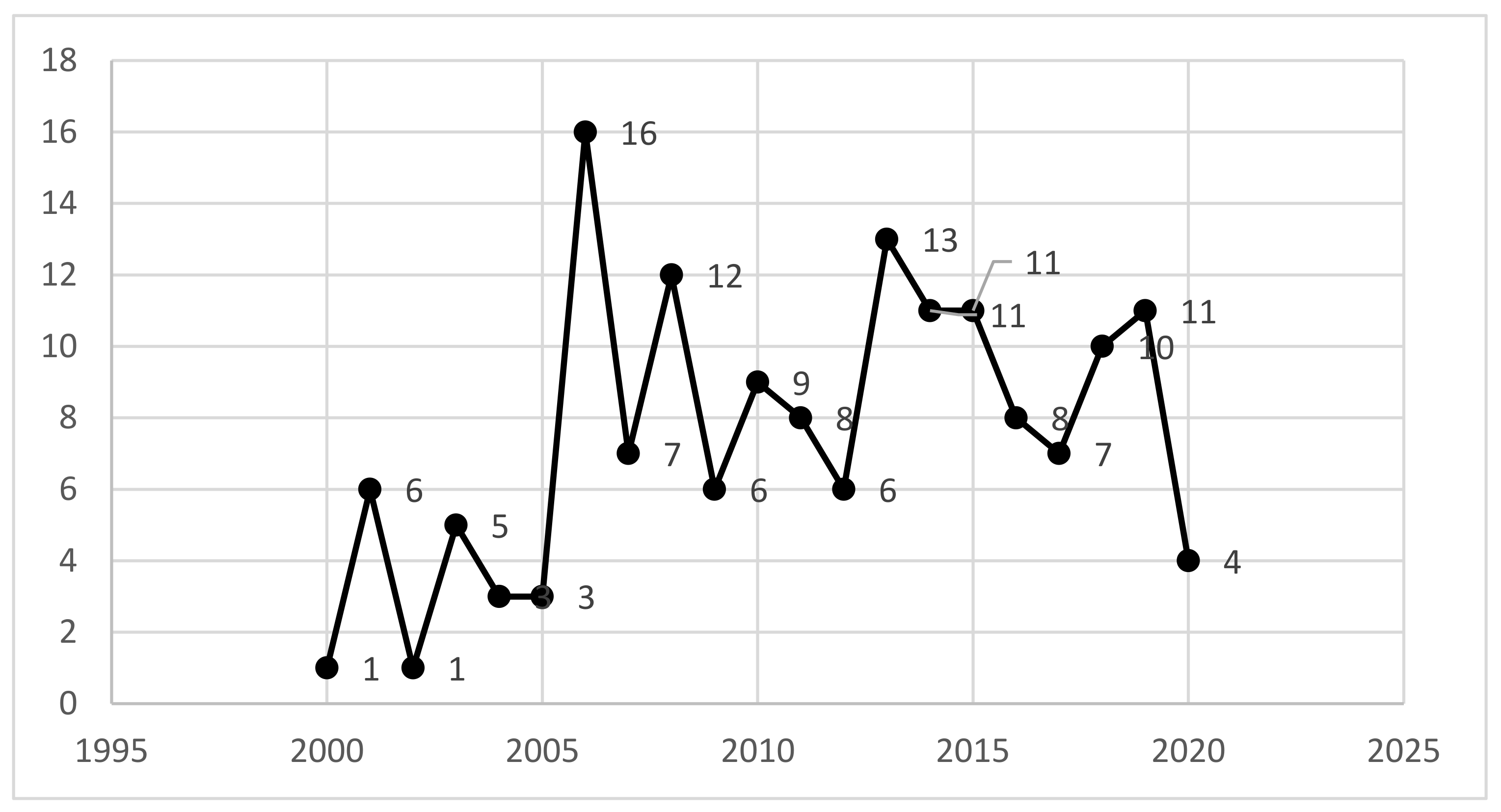
Description of Material Analyzed
- Q1: In What Types of Enterprises are the Outcomes of WHPI Examined and Measured Most Often?
- Q2: What Research Methods are Used to Measure the Outcomes of WHPI?
- Q3: What Types of Outcomes of WHPI Are Reported by Organizations?
- Q4: How Often Has Research Indicated Strong Evidence Data Confirming the Effectiveness of the WHPI?
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hackman, J.R. A new strategy for job enrichment. Calif. Manag. Rev. 1975, XVII, 57–71. [Google Scholar]
- Rab-Przybyłowicz, J. Medical Tourism: Theoretical Considerations. Stud. Perieget. 2016, 2, 13–31. [Google Scholar]
- Kickbusch, I. Responding to the health society. Health Promot. Int. 2007, 22, 89–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kickbusch, I. The health society: Importance of the new policy proposal by the EU Commission on Health and Consumer Affairs. Health Promot. Int. 2005, 20, 101–103. [Google Scholar] [CrossRef] [Green Version]
- Constitution of the World Health Organization. Basic Documents, 45th ed.; Supplement; The World Health Organization (WHO): Geneva, Switzerland, 2006; pp. 1–18. [Google Scholar]
- Puchalski, K.; Korzeniowska, E. (Eds.) Promocja Zdrowia w Zakładzie Pracy: Wsparcie dla Zdrowego Odżywiania się i Aktywności Fizycznej Pracowników; Instytut Medycyny Pracy: Łódź, Poland, 2017. [Google Scholar]
- Organisation for Economic Co-operation and Development (OECD). Hours Worked (Indicator) [Internet]. 2018. Available online: https://data.oecd.org/emp/hours-worked.htm (accessed on 17 April 2020).
- Nienhaus, A.; Skudlik, C.; Seidler, A. Work-related accidents and occupational diseases in veterinarians and their staff. Int. Arch. Occup. Environ. Health 2005, 78, 230–238. [Google Scholar]
- Leplat, J.; Rasmussen, J. Analysis of Human Errors in Industrial Incidents and Accidents for Improvement of Work Safety. Accid. Anal. Prevent. 1984, 16, 77–88. [Google Scholar]
- Umar, T.; Egbu, C. Heat stress, a hidden cause of accidents in construction. Proc. Inst. Civ. Eng. Munic. Eng. 2020, 173, 49–60. [Google Scholar] [CrossRef]
- Karasek, R.A.; Baker, D.; Marxer, F.; Ahlbom, A.; Theorell, T. Job decision latitude, job demands, and cardiovascular disease: A prospective study of Swedish men. Am. J. Public Health 1981, 71, 694–705. [Google Scholar] [CrossRef] [Green Version]
- Potocka, A.; Waszkowska, M. Application of Job Demands-Resources model in research on relationships between job satisfaction, job resources, individual resources and job demands. Med. Pr. 2013, 64, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Häusser, J.A.; Mojzisch, A.; Niesel, M.; Schulz-Hardt, S. Ten years on: A review of recent research on the Job Demand–Control (-Support) model and psychological well-being. Work Stress 2010, 16, 1–35. [Google Scholar]
- Tims, M.; Bakker, A.B.; Derks, D. The Impact of Job Crafting on Job Demands, Job Resources, and Well-Being. J. Occup. Health Psychol. 2013, 18, 230–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, P.; Vainio, H. Well-being at work—Overview and perspective. Scand J. Work Environ. Health 2010, 36, 422–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buffet, M.A.; Gervais, R.L.; Liddle, M.; Eeckelaert, L.; De Jong, T. Well-Being at Work: Creating a Positive Work Environment; Literature Review; European Agency for Safety and Health at Work: Bilbao, Spain, 2013. [Google Scholar]
- Mujtaba, B.G.; Cavico, F.J. Corporate wellness programs: Implementation challenges in the modern American workplace. Int. J. Health Policy Manag. 2013, 1, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Kaspin, L.C.; Gorman, K.M.; Miller, R.M. Systematic review of employer-sponsored wellness strategies and their economic and health-related outcomes. Popul. Health Manag. 2013, 16, 14–21. [Google Scholar] [CrossRef]
- World Health Organization. Work organisation and Stress. Prot. Work Health 2003, 3, 1–27. [Google Scholar]
- Puchalski, K.; Korzeniowska, E. Promocja zdrowia w zakładach pracy w Polsce w 2015 R.- diagnoza na podstawie reprezentatywnego badania firm zatrudniających powyżej 50 pracowników. Med. Pr. 2017, 68, 229–246. [Google Scholar] [PubMed]
- European Network For Workplace Health Promotion (ENWHP). The Luxembourg Declaration on Workplace Health Promotion; WHP: Luxembourg, 2007. [Google Scholar]
- Day, A.; Helson, T. Workplace health promotion. In The Wiley Blackwell Handbook of the Psychology of Occupational Safety and Workplace Health; Clarke, S., Probst, T.M., Passmore, J., Guldenmund, F., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Goetzel, R.Z.; Henke, R.M.; Tabrizi, M.; Pelletier, K.R.; Loeppke, R.; Ballard, D.W.; Grossmeier, J.; Anderson, D.R.; Yach, D.; Kelly, R.K.; et al. Do workplace health promotion (wellness) programs work? J. Occup. Environ. Med. 2014, 56, 927–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulmer, J.; Groeben, F. Work Place Health Promotion: A longitudinal study in companies placed in Hessen and Thueringen. J. Public Health 2005, 13, 144–148. [Google Scholar] [CrossRef]
- Rucker, M.R. Workplace wellness strategies for small businesses. Int. J. Work Health Manag. 2017, 10, 55–68. [Google Scholar] [CrossRef]
- Chu, C.; Breucker, G.; Harris, N.; Stitzel, A.; Gan, X.; Gu, X.; Dwyer, S. Health-promoting workplaces—International settings. Health Promot. Int. 2000, 15, 155–167. [Google Scholar] [CrossRef]
- Graveling, R.A.; Crawford, J.O.; Cowie, H.; Amati, C.; Vohra, S. A Review of Workplace Interventions that Promote Mental Wellbeing in the Workplace; Institute of Occupational Medicine: Edinburgh, Scotland, 2008. [Google Scholar]
- Pich, J. Preventing occupational stress in healthcare workers. Res. Nurs. Health 2018, 41, 408–409. [Google Scholar] [CrossRef]
- Richardson, K.M.; Rothstein, H.R. Effects of Occupational Stress Management Intervention Programs: A Meta-Analysis. J. Occup. Health Psychol. 2008, 13, 69–93. [Google Scholar] [CrossRef] [PubMed]
- Engbers, L.H.; Van Poppel, M.N.M.; Chin APaw, M.J.M.; Van Mechelen, W. Worksite health promotion programs with environmental changes: A systematic review. Am. J. Prev. Med. 2005, 29, 61–70. [Google Scholar] [CrossRef]
- Rongen, A.; Robroek, S.J.W.; Van Lenthe, F.J.; Burdorf, A. Workplace health promotion: A meta-analysis of effectiveness. Am. J. Prev. Med. 2013, 44, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Emmons, K.M. How can we increase translation of research into practice? Types of evidence needed. Annu. Rev. Public Health 2007, 28, 413–433. [Google Scholar] [CrossRef] [Green Version]
- Goetzel, R.; Roemer, E.C.; Kent, K.; Hohlbauch, A.; Tibrizi, M.J.; Smith, K. Health Promotion in the Workplace Program Evaluation. In Health Promotion in the Workplace, 5th ed.; O’Donnell, M.P., Ed.; Art & Science of Health Promotion Institute: Troy, MI, USA, 2017; pp. 197–257. [Google Scholar]
- Van der Vliet, J.A. Occupational health in European member states: A road to organizational health. Int. J. Occup Med. Environ. Health 2001, 14, 13–17. [Google Scholar]
- Korzeniowska, E.; Puchalski, K. (Eds.) Workplace Health Promotion in Europe; The Nofer Institute of Occupational Medicine: Łódź, Poland, 2006. [Google Scholar]
- World Health Organization (WHO). Ottawa Charter for Health Promotion; WHO: Geneva, Switzerland, 1986. [Google Scholar]
- Baicker, K.; Cutler, D.; Song, Z. Workplace wellness programs can generate savings. Health Aff. 2010, 29, 1–8. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Health Promotion Glossary; Vol. WHO/HPR/HE; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Welch, A.; Healy, G.; Straker, L.; Comans, T.; O’Leary, S.; Melloh, M.; Sjøgaard, G.; Pereira, M.; Chen, X.; Johnston, V. Process evaluation of a workplace-based health promotion and exercise cluster-randomised trial to increase productivity and reduce neck pain in office workers: A RE-AIM approach. BMC Public Health 2020, 20, 1–15. [Google Scholar]
- Gomathi, K.; Rajini, G. Organizational ergonomics: Human engineering leading to employee well-being. Int. J. Innov. Technol. Explor. Eng. 2019, 8, 3744–3749. [Google Scholar]
- Caspi, C.E.; Dennerlein, J.T.; Kenwood, C.; Stoddard, A.M.; Hopcia, K.; Hashimoto, D.; Sorensen, G. Results of a pilot intervention to improve health and safety for health care workers. J. Occup. Environ. Med. 2013, 55, 1449–1455. [Google Scholar] [CrossRef] [Green Version]
- Richter, H.O.; Sundin, S.; Long, J. Visually deficient working conditions and reduced work performance in office workers: Is it mediated by visual discomfort? Int. J. Ind. Ergon. 2019, 72, 128–136. [Google Scholar] [CrossRef]
- Kim, S.S.; Okechukwu, C.A.; Dennerlein, J.T.; Boden, L.I.; Hopcia, K.; Hashimoto, D.M.; Sorensen, G. Association between perceived inadequate staffing and musculoskeletal pain among hospital patient care workers. Int. Arch. Occup. Environ. Health 2014, 87, 323–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugdill, L.; Brettle, A.; Hulme, C.; Mccluskey, S.; Long, A.F. Workplace physical activity interventions: A systematic review. Int. J. Work Health Manag. 2008, 1, 20–40. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, G.; McLellan, D.L.; Sabbath, E.L.; Dennerlein, J.T.; Nagler, E.M.; Hurtado, D.A.; Pronk, N.P.; Wagner, G.R. Integrating worksite health protection and health promotion: A conceptual model for intervention and research. Prev. Med. 2016, 91, 188–196. [Google Scholar] [CrossRef] [Green Version]
- Schmitt-Howe, B. Healthy at work: Interdisciplinary perspectives. In Healthy at Work: Interdisciplinary Perspectives; Wiencke, M., Cacace, M., Fischer, S., Eds.; Springer International Publishing: Berlin, Germany, 2016; pp. 217–234. [Google Scholar]
- Anderson, G. Chronic Conditions: Making the Case for Ongoing Care; Partnership for Solutions: London, UK, 2004. [Google Scholar]
- Workplace Health Promotion. Available online: https://www.cdc.gov/workplacehealthpromotion/initiatives/workathealth/index.html (accessed on 12 December 2020).
- Verra, S.E.; Benzerga, A.; Jiao, B.; Ruggeri, K. Health Promotion at Work: A Comparison of Policy and Practice Across Europe. Saf. Health Work. 2019, 10, 21–29. [Google Scholar] [CrossRef]
- Ammendolia, C.; Côté, P.; Cancelliere, C.; Cassidy, J.D.; Hartvigsen, J.; Boyle, E.; Soklaridis, S.; Stern, P.; Amick, B. Healthy and productive workers: Using intervention mapping to design a workplace health promotion and wellness program to improve presenteeism. BMC Public Health 2016, 16, 1190. [Google Scholar] [CrossRef] [Green Version]
- Ory, M.G.; Jordan, P.J.; Bazzarre, T. The Behavior Change Consortium: Setting the stage for a new century of health behavior-change research. Health Educ. Res. 2002, 17, 500–511. [Google Scholar] [CrossRef]
- Xerox. Working Well: A Global Survey of Workforce Wellbeing Strategies, 7th ed.; Survey Report; Xerox: Norwalk, CT, USA, 2016. [Google Scholar]
- Karanika-Murray, M.; Biron, C. Why Do Some Interventions Derail? Deconstructing the Elements of Organizational Interventions for Stress and Well-Being. In Derailed Organizational Interventions for Stress and Well-Being: Confessions of Failure and Solutions for Success; Karanika-Murray, M., Biron, C., Eds.; Springer: New York, NY, USA; London, UK, 2015; pp. 1–21. [Google Scholar]
- Korzeniowska, E.; Puchalski, K. Workplace health promotion program quality evaluation questionnaire. Med. Pr. 2002, 53, 361–368. [Google Scholar]
- Goetzel, R.Z. Research Designs for Workplace Health Programs. Am. J. Health Promot. 2016, 30, 576–578. [Google Scholar]
- Soler, R.E.; Leeks, K.D.; Razi, S.; Hopkins, D.P.; Griffith, M.; Aten, A.; Chattopadhyay, S.K.; Smith, S.C.; Habarta, N.; Goetzel, R.Z.; et al. A Systematic Review of Selected Interventions for Worksite Health Promotion. The Assessment of Health Risks with Feedback. Am. J. Prev. Med. 2010, 38, S237–S262. [Google Scholar] [CrossRef]
- Charrois, T.L. Systematic reviews: What do you need to know to get started? Can. J. Hosp. Pharm. 2015, 68, 144–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancelliere, C.; Cassidy, J.D.; Ammendolia, C.; Côté, P. Are workplace health promotion programs effective at improving presenteeism in workers? A systematic review and best evidence synthesis of the literature. BMC Public Health 2011, 11, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lunde, L.K.; Skare, Ø.; Mamen, A.; Sirnes, P.A.; Aass, H.C.D.; Øvstebø, R.; Goffeng, E.; Matre, D.; Nielsen, P.; Heglum, H.S.A.; et al. Cardiovascular health effects of shift work with long working hours and night shifts: Study protocol for a three-year prospective follow- up study on industrial workers. Int. J. Environ. Res. Public Health 2020, 17, 589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.; Li, T.; Zou, G.; Renzaho, A.M.N.; Li, X.; Shi, L.; Ling, L. Results of a cluster randomized controlled trial to promote the use of respiratory protective equipment among migrant workers exposed to organic solvents in small and medium-sized enterprises. Int. J. Environ. Res. Public Health 2019, 16, 3187. [Google Scholar] [CrossRef] [Green Version]
- Akram, Y.; Al-Khudairy, L.; Hemming, K.; Hofman, J.; Kudrna, L.; Lilford, R.; Nightingale, M.; Prideaux, R.; Russell, S.; Sutherland, A.; et al. Evaluation of a policy intervention to promote the health and wellbeing of workers in small and medium sized enterprises—A cluster randomised controlled trial. BMC Public Health 2019, 19, 493. [Google Scholar]
- Deforche, B.; Mommen, J.; Hublet, A.; De Roover, W.; Huys, N.; Clays, E.; Maes, L.; De Bourdeaudhuij, I.; Van Cauwenberg, J. Evaluation of a brief intervention for promoting mental health among employees in social enterprises: A cluster randomized controlled trial. Int. J. Environ. Res. Public Health 2018, 15, 2107. [Google Scholar] [CrossRef] [Green Version]
- Rohlman, D.S.; Campo, S.; Hall, J.; Robinson, E.L.; Kelly, K.M. What could total worker health® look like in small enterprises? Ann. Work Expo. Heal. 2018, 62, S34–S41. [Google Scholar] [CrossRef]
- Magnavita, N.; Sakowski, P.; Capitanelli, I.; La Milia, D.I.; Moscato, U.; Poscia, A.; Ricciardi, W. Health promotion for the aging workforce in Poland. Int. J. Occup. Med. Environ. Health 2018, 31, 753–761. [Google Scholar]
- Huang, S.J.; Hung, W.C. Policy, environment, and worksite fitness program participation among financial enterprise employees in Taiwan. J. Exerc. Sci. Fit. 2016, 14, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.S.; Veen, R.; Van Der Song, Z. The impact of coping strategies on occupational stress and turnover intentions among hotel employees. J. Hosp. Mark. Manag. 2018, 27, 926–945. [Google Scholar]
- Cadavid, E.; Sáenz, L.M. Physical Activity as a Strategy for Prevention and Health Promotion in the Occupational Context: An Example of Corporate Engagement. Proc. Manuf. 2015, 3, 1140–1147. [Google Scholar]
- Kim, S.A.; Suh, C.; Park, M.H.; Kim, K.; Lee, C.K.; Son, B.C.; Kim, J.H.; Lee, J.T.; Woo, K.H.; Kang, K.H. Effectiveness of a Comprehensive Stress Management Program to Reduce Work-Related Stress in a Medium-Sized Enterprise. Ann. Occup. Environ. Med. 2014, 26, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, M.; Tilford, S.; Branney, P.; Kinsella, K. Championing mental health at work: Emerging practice from innovative projects in the UK. Health Promot. Int. 2014, 29, 583–595. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.L.H. Building human resources management capacity for university research: The case at four leading Vietnamese universities. High. Educ. 2016, 71, 231–251. [Google Scholar] [CrossRef]
- Sun, W.; Wu, H.; Wang, L. Occupational stress and its related factors among university teachers in China. J. Occup. Health 2011, 53, 280–286. [Google Scholar]
- Edmunds, S.; Stephenson, D.; Clow, A. The effects of a physical activity intervention on employees in small and medium enterprises: A mixed methods study. Work 2013, 46, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Haruyama, Y.; Fukuda, H.; Arai, T.; Muto, T. Change in lifestyle through health promotion program without face-to-face intervention in a large-scale Japanese enterprise. J. Occup. Health 2013, 55, 74–83. [Google Scholar] [PubMed]
- Williams, S.J.; Snow, D.M. Promoting health in small and medium-sized enterprises. J. Small Bus. Enterp. Dev. 2012, 19, 729–744. [Google Scholar]
- Tsai, H.H.; Peng, S.M.; Yeh, C.Y.; Chen, C.J.; Chen, R.Y. An effective physical fitness program for small and medium-sized enterprises. Ind. Health 2011, 49, 311–320. [Google Scholar] [CrossRef] [Green Version]
- Moore, A.; Parahoo, K.; Fleming, P. Managers’ understanding of workplace health promotion within small and medium-sized enterprises: A phenomenological study. Health Educ. J. 2011, 70, 92–101. [Google Scholar]
- Kobayashi, Y.; Kaneyoshi, A.; Yokota, A.; Kawakami, N. Effects of a worker participatory program for improving work environments on job stressors and mental health among workers: A controlled trial. J. Occup. Health 2008, 50, 455–470. [Google Scholar] [CrossRef] [Green Version]
- Lie, A. ‘Inclusive Working Life’ in Norway—Experience from ‘Models of Good Practice’ enterprises. Croat. Med. J. 2008, 49, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Nishikido, N.; Matsuda, K.; Fukuda, E.; Motoki, C.; Tsutaki, M.; Kawakami, Y.; Yuasa, A.; Iijima, M.; Tanaka, M.; Hirata, M.; et al. Development and process evaluation of the participatory and action-oriented empowerment model facilitated by occupational health nurses for workplace health promotion in small and medium-sized enterprises. Ind. Health 2007, 45, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Idreis, H.M.; Siqueira, C.E.; Levenstein, C.C. Impact of software and hardware technologies on occupational health and safety policies in Saudi Arabian oil refineries. New Solut. 2006, 16, 193–216. [Google Scholar] [CrossRef] [PubMed]
- Itani, T.; Tachi, N.; Takeyama, H.; Ebara, T.; Takanishi, T.; Murata, K.; Inoue, T.; Suzumura, H.; Kurungkraiong, S.; Khuvasanont, T.; et al. Approaches to occupational health based on participatory methodology in small workplaces. Ind. Health 2006, 44, 17–21. [Google Scholar] [CrossRef] [Green Version]
- Krungkraiwong, S.; Itani, T.; Amornratanapaichit, R. Promotion of a healthy work life at small enterprises in Thailand by participatory methods. Ind. Health 2006, 44, 108–111. [Google Scholar] [CrossRef] [Green Version]
- Fine, A.; Ward, M.; Burr, M.; Tudor-Smith, C.; Kingdon, A. Health promotion in small workplaces—A feasibility study. Health Educ. J. 2004, 63, 334–346. [Google Scholar] [CrossRef]
- Kawakami, T.; Kogi, K. Action-oriented support for occupational safety and health programs in some developing countries in Asia. Int. J. Occup. Saf. Ergon. 2001, 7, 421–434. [Google Scholar] [CrossRef]
- Chen, T.H.; Huang, J.J.; Chang, F.C.; Chang, Y.T.; Chuang, H.Y. Effect of workplace counseling interventions launched by workplace health promotion and tobacco control centers in Taiwan: An evaluation based on the Ottawa charter. PLoS ONE 2016, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Horodyska, K.; Luszczynska, A.; Van Den Berg, M.; Hendriksen, M.; Roos, G.; De Bourdeaudhuij, I.; Brug, J. Good practice characteristics of diet and physical activity interventions and policies: An umbrella review. BMC Public Health 2015, 15, 1–16. [Google Scholar]
- Aburumman, M.; Newnam, S.; Fildes, B. Evaluating the effectiveness of workplace interventions in improving safety culture: A systematic review. Saf. Sci. 2019, 115, 376–392. [Google Scholar] [CrossRef]
- Henke, R.M.; Goetzel, R.Z.; McHugh, J.; Isaac, J. Recent experiences in health promotion at Johnson and Johnson: Lower health spending, strong returns on investment. Health Aff. 2011, 30, 490–499. [Google Scholar]
- Paauwe, J.; Boselie, P. HRM and performance: What next? Hum. Resour. Manag. J. 2005, 15, 68–83. [Google Scholar]
- Paauwe, J. HRM and Performance: Achievements, Methodological Issues and Prospects. J. Manag. Stud. 2009, 1, 129–142. [Google Scholar]
- Alfes, K.; Shantz, A.; Truss, C.; Soane, E. The link between HRM practices, employee engagement and employee behaviors: A moderated mediation model. Int. J. Hum. Resour. Manag. 2013, 24, 330–351. [Google Scholar]
- Heckman, J.J.; Singer, B. Social Science Research Council (U.S.). In Longitudinal Analysis of Labor Market Data; Cambridge University Press: New York, NY, USA, 1985. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Study | Type of Paper | Country | Size of Organization | Sector | Type of Research | Sample Size | |
|---|---|---|---|---|---|---|---|
| Enterprises | Employees | ||||||
| [59] | O | Norway | not indicated | manufacturing | 3 | 125 | |
| [60] | O | China | SMEs | manufacturing | 3 | 60 | 1211 |
| [61] | O | UK | SMEs | varied sectors | 3 | 132 | |
| [62] | O | Belgium | not indicated | social enterprise | 2 | 196 | |
| [63] | O | USA | small | varied sectors | 1 | 19 | |
| [64] | R | Poland | large, medium, and small | varied sectors | 1 | 84 | |
| [25] | O | USA | SMEs | services | 1 | 4 | |
| [45] | O | USA | SMEs, hospitals | varied sectors | 1 | 3 | not indicated |
| [65] | O | Taiwan | SMEs | financial | 3 | 31 | 428 |
| [66] | O | Taiwan | large, medium, and small | varied sectors | 3 | 544 | |
| [67] | O | Colombia | large | public providers, IT and communication services | 3 | 1 | 6000 |
| [68] | O | Korea | medium | metal company | 3 | 211 | |
| [69] | R | UK | not indicated | varied sectors | 1 | 3 | |
| [70] | O | Vietnam | SMEs | varied sectors | 3 | 20 | |
| [71] | O | China | large | retail | 2 | 9 | 2768 |
| [72] | O | UK | SMEs | varied sectors | 3 | 17 | 89 |
| [73] | O | Japan | large | services | 2 | 22429 | |
| [74] | O | Wales (UK) | SMEs | varied sectors | 1 | 5 | |
| [75] | O | Taiwan | SMEs | not indicated | 2 | 133 | |
| [76] | O | Ireland | SMEs | Health and Social Care Trust | 1 | 18 | |
| [77] | O | Japan | large | not indicated | 3 | 1070 | |
| [78] | O | Norway | large, medium, and small | not indicated | 3 | 11 | |
| [79] | O | Japan | SMEs | not indicated | 1 | 80 | |
| [80] | O | Saudi Arabia | large | oil refineries | 1 | 2 | |
| [81] | O | Philippines, Thailand, Japan | small | informal sector | 3 | 8 | |
| [82] | O | Thailand | small | manufacturing | 3 | 7 | |
| [24] | O | Germany | SMEs | varied sectors | 2 | 150 | |
| [83] | O | Wales [UK] | SMEs | varied sectors | 2 | 37 | 531 |
| [84] | O | Philippines, Thailand, Laos, Pakistan, Vietnam | small | workers and farmers, home-based workers | 3 | not indicated | |
| Categories Used in Model Developed by Sorensen | Applied Categories of Outcomes | Outcomes Indicated in the Analyzed Studies | |
|---|---|---|---|
| organizational | Conditions of work (physical environment, organization of work) | Culture and company strategy | Led to implementing a strategy and culture based on health, improved working environment and occupational climate, improved work organization, greater flexibility of the work schedule, creating a workplace free of smoke and excessive noise, improved health awareness of companies, improved CSR |
| Enterprise Outcomes (productivity and quality, turnover and absence, health care costs) | Financial | Led to cost reduction in the long term, reduced sickness absenteeism, active sickness absence, employee expenditure on health care and better health intervention return on investment, reducing medical cost, positive impact on insurance absenteeism, presentism, turnover, preventing early retirement, increased productivity of employees, faster return to work in case of injury, and faster return after disability pension, as well as reducing the frequency of occupational accidents. | |
| individual | Worker proximal outcomes (health and safety behaviors engagement in programs) | Behavioral | Led to reinforcement of teamwork, satisfaction from participating in the program, changed behavior of workers and managers, helping workers to adopt and maintain healthy behavior, lower health risks, improved healthy lifestyle of workers: healthy eating, less stress, more sleep, giving up smoking, physical activity or fitness classes, exercise, improved coping strategies |
| Worker proximal outcomes | Cognitive | Led to enlightenment in terms of health awareness in the workplace, shared information about health issues, initiated thinking about health, improved ability to work, a sense of control over their jobs, and mobility to meet the mental demands of work, improved new skills and minimized skill underutilization | |
| Worker outcomes Injury Illness | Physiological | Led to an improvement in the physical health of workers, improvements in musculoskeletal disorders, pain reduction in neck, wrist pain and upper/lower back pain, chronic illness prevention, e.g., weight, blood pressure, resting heart rate, waistline, BMI, front and back trunk flexibility, abdominal muscle durability and back muscle strength | |
| Worker outcomes Wellbeing | Psychological | Led to improved mental health and wellbeing, reduction of stress-related hazards and consequences, a decreased level of occupational burnout, reduction of somatic symptoms, depressive symptoms, work-related symptoms, job satisfaction and lower job tension. |
| Studies | Characteristics of Intervention or Program | Classification—Type of Intervention Activities * | Duration of Intervention and Measurement Frequency | Type of Indicated Individual (I) and Organizational: (O) Outcomes * | Evaluation Types | Detailed Result of the Assessment of the Effectiveness of the Intervention ** |
|---|---|---|---|---|---|---|
| [59] | A supervised high-intensity interval training intervention focused on cardiovascular health effects | physical activity & fitness intervention | 3 years: 5 times (at baseline, after 3 months of intervention, after 1 year, after 2 and 3 years) | I: physiological; O: not applicable | outcome evaluation | cardiovascular health effects (+) (physical activity level as a moderator between work schedule and cardiovascular disease risk factors) |
| [60] | “Participatory Action-Oriented Training” (PAOT): the use of respiratory protective equipment, different types of intervention | environmental and safety workplace intervention; health education and personalized counseling | 6 months: 3 times (at baseline, at 3 months, at 6 months) | I: 1 cognitive, behavioral; O: not applicable | outcome evaluation | self-reported appropriate respiratory protective equipment, occupational health knowledge (+), attitude (+), and practice e.g., participation in occupational health check-ups (+) |
| [61] | “Thrive at Work”: program focused on mental health, musculoskeletal health and a healthy lifestyle | multi-focused comprehensive program | 6 months: 5 times (at baseline, after randomization, after 3 months, after 6 months and one year since intervention) | I: cognitive; behavioral; physiological; O: financial; corporate culture and strategy | outcome evaluation | sickness absence (+), health and safety compliance of workers (+), productivity and profit of the company (+), culture change in SMSs, happiness of workers, a fitter and more resilient workplace |
| [62] | Mental health promotion at the workplace, provision of mental support, individual and group talks, stress management training, personal development plans | health education and personalized counseling; coping with health problems and skills development | less than 3 months: 3 times (at baseline, at one month, at four months) | I: behavioral, psychological; O: corporate culture and strategy | outcome evaluation | empowerment (0), resilience, palliative behavior (+), determinants of four coping strategies of mental health (+), quality of life, and life satisfaction (+), unjustified worrying (−) |
| [63] | “Total Work Health ®”: occupational health and safety, employee safety | environmental and safety workplace intervention | no information | I: not applicable; O: corporate culture and strategy | process evaluation | smoke-free workplaces, cell phone use, personal protective equipment (PPE), equipment maintenance, flexible schedules, smoking cessation, weight management, physical activity, environmental changes e.g., installing bike racks, providing fitness equipment on site |
| [64] | “WHPOW”: health promotion of senior workers | environmental and safety workplace intervention, coping with health problems and skills development | no data indicated | I: cognitive, behavioral; O: corporate culture and strategy, financial | structure and process evaluation | transfer of knowledge, experience, ideas, and skills from older to younger workers, promoting the employment of older workers and increasing job retention among pre-retirement workers, work climate and attitudes toward older workers, fighting discrimination and exclusion, reducing the gender gap |
| [25] | Workplace wellness program | physical activity & fitness intervention | no data indicated | I: not applicable; O: corporate culture and strategy | structure and process evaluation | corporate culture and strategy of the small business organization; employees oriented towards more effective, viable and thriving wellness programs |
| [45] | Comprehensive integrated program, focused on working conditions, telephone health coaching and web-based resources that included integrated messages on back pain, worksite-wide events for ergonomic and health promotion practices | multi-focused comprehensive program | no data indicated | I: physiological, behavioral, cognitive; O: corporate culture and strategy, financial | structure, process and outcome evaluation | jointly predicted lower back pain (+), sleep (+), physical activity (+); employee-rated health culture and safety culture (+), self-reported back pain (−), safety hazards (-); organizational resources—measured by the CDC Worksite Health Scorecard: related to organizational support (+), physical activity (+) and nutrition (+) |
| [65] | Worksite fitness program, facilities and exercises | physical activity & fitness intervention | no data indicated | I: behavioral; O: corporate culture and strategy | process evaluation | social support and worksite environment (health promotion policy and equipment) affect employee participation in the program (+) |
| [85] | WHP program intervention including health education, diet education, physical fitness classes, smoking cessation classes, a smoke-free workplace | multi-focused comprehensive program | 5 years | I: cognitive, behavioral; O: corporate culture and strategy | structure, process, and outcome evaluation | awareness of health, diet, physical activity, and smoking (+), using external resources and medical consultation (+), follow-up rates of the abnormal results of annual health examinations (+), the announcement of regulations (+), creating budgets specifically for health promotion and tobacco hazard control to improve employees’ physical and mental health conditions (+) |
| [67] | Programs including prevention and treatment of musculoskeletal disorder, promotion of physical activity, intervention in cases of chronic illness and cardiovascular risk factors; and a return-to-work program following injury, sickness or accident | multi-focused comprehensive program | long-term (several years) | I: cognitive, behavioral, physiological; O: corporate culture and strategy, financial | structure and process evaluation | the reduction of errors, increased safety, and performance of the person—machine—environment system, development of healthy lifestyle habits in the community, physical activity program as a strategy for prevention and health promotion for employees and their families (+) |
| [68] | “Participatory Action-Oriented Training [PAOT]”; program focused at improving health and safety at work, organizational and the individual level intervention, conducted to reduce work-related stress | multi-focused comprehensive program | 2 months: 2 times (pre- and post-test) | I: cognitive, psychological, behavioral, physiological; O: corporate culture and strategy | outcome evaluation | blue-collar workers: stress (-), physical environment (+), occupational climate (+), job demands (+), job control (+), interpersonal conflicts (-), organizational system (+), and lack of rewards (-) white-collar: worker stress (0), physical environment (0) and occupational climate (+); job demands (0), job control (0), interpersonal conflicts (0), organizational system (0), and lack of rewards (0) |
| [69] | Intervention consists of engaging workplace-based ‘business champions’, integration, formalization and embedding in organizational environments by means of training and workshops, pedometer challenges and holistic therapy sessions | multi-focused comprehensive program | 3 years: 1 time after intervention | I: cognitive, psychological, O: corporate culture and strategy | process evaluation | confidence building, capacity building and system change at individual and organizational levels, individual outcome knowledge improvement and wellbeing of employees; participatory approaches within interventions is a facilitator of the organizational culture (+) |
| [70] | Participatory Action-Oriented Training [PAOT], improving health and safety at work | multi-focused comprehensive program | 1 year: 2 times (pre- and post-test) | I: not applicable; O: corporate culture and strategy, financial | outcome evaluation | improvements among the intervention factories in terms of work environment (+), number of improvements and health costs (+), productivity of civil engineering, metal, garment, and rice mill industries in the intervention group (+) |
| [71] | “Health Promotion Enterprise Program” psychosocial interventions, mental health promotion, provision of health services to people with mental illness, and professional skills training | multi-focused comprehensive program | 30 months: 2 times (pre- and post-test) | I: psychological, behavioral; O: financial | outcome evaluation | participants’ ability to work (+), their sense of control over their jobs (+), ability to meet the mental demands of work (+), job stress levels (-) probability of absenteeism related to depression (-) |
| [72] | “Workplace Activator“ program promoting PA including access to a web portal with information on the benefits of PA and information on how to begin exercising, 3 months free gym membership, a free pedometer, challenges | physical activity & fitness intervention | 6 months: 2 times (at baseline and after 6 months) | I: behavioral, physiological cognitive, psychological; O: corporate culture and strategy, financial | outcome evaluation | PA level and awareness (+), BMI (-), absenteeism (0), perceived social support for PA from friends (+), perceived social support for PA from family (0), after 6 months: physical activity (+), general health rating (+), satisfaction with life (+) and positive mood states (+), perceived stress (-), negative mood states (-) and presentism (-), absenteeism (0) |
| [73] | WHPP program consisting of four courses connected with lifestyle, Internet and printed material based | health education and personalized counseling | 2–3-month: 2 times (at baseline and after 1 year) | I: behavioral, physiological; O: not applicable | outcome evaluation | change of lifestyle (+), overall prevalence of cardiovascular risk (-), 10% 10-year risk trend (-) |
| [74] | Identification of the enablers and barriers to introducing workplace health-promotion programs for SMEs | environmental and safety workplace intervention | no data indicated | I: not applicable; O: corporate culture and strategy, financial | process evaluation | factors determining the implementation of the program: an internal health champion/coordinator, resources, time, and the longevity of the external support funded by a government initiative |
| [75] | Worksite program consisted of physical fitness exercise for the occupational environment, aerobic exercise and stretching | physical activity & fitness intervention | 3 months: 2 times (pre- and post-test) | I: behavioral, physiological, psychological; O: not applicable | outcome evaluation | weight (+), blood pressure (+), resting heart rate (+), waistline (+), BMI (+), front and back trunk flexibility (+), abdominal muscle durability (+) and back muscle strength (+), musculoskeletal disorders (+), cardiovascular risk factors (+), overall health (+) |
| [76] | Physical fitness program for small and medium-sized enterprises | physical activity & fitness intervention | no data indicated | I: not applicable; O: corporate culture and strategy, financial | structure and process evaluation | factors determining the realization of the strategy for workplace health promotion: ecological approach within the policy of the company, meaningful engagement by managers; protection from harm and opportunities for health improvement and affording protection for the viability and reputation of the business |
| [77] | Intervention using the Mental Health Action Checklist (list consisting of: sharing work planning, work time and organization, ergonomic work methods, workplace environments, mutual support at work, and preparedness and care) on reducing job stressors and psychological distress | multi-focused comprehensive program | 6 months: 2 times (pre- and post-test) | I: psychological, behavioral, cognitive; O: corporate culture and strategy | structure, process, and outcome evaluation | reduction of job stressors (+) and psychological distress (+), skill underutilization (+), supervisor and coworker support (+), and job satisfaction, degree of worker participation and implementation of planned actions heavily influenced the intervention effect |
| [78] | “Inclusive Working Life“ program, reducing sickness absenteeism, promoting an early return to work, preventing early retirement, and promoting employment of functionally impaired persons | multi-focused comprehensive program | 2 years: 2 times (pre- and post-test) | I: behavioral; O: finance | structure, process, outcome evaluation | sickness absenteeism (0), use of early retirement (+) and disability retirement (+), good cooperation with the occupational health service and the empowerment and involvement of the employees is associated with a low sickness absence rate |
| [79] | Empowerment model for workplace health promotion. The model consists of three tools: an action checklist, an information guidebook, and a book of good practices | multi-focused comprehensive program | 1 year, information not clear | I: cognitive, behavioral; O: corporate culture and strategy | process evaluation | empowerment and participatory and action-oriented process of implementation WHPI in SMSs; WHP as part of organizational culture |
| [80] | “PACE’s Triangle of Prevention” health and safety, a comprehensive training program, effective participation, accident investigation and prevention | environmental and safety workplace intervention; health education and personalized counseling | no data indicated | I: not applicable; O: corporate culture and strategy | process evaluation | organizational culture, implementation of safety system |
| [81] | “Work Improvement in small Enterprises” program, improving the workplace environment, reducing the local muscle workloads, and preventing work-related muscle-skeletal disorder | environmental and safety workplace intervention | 3 years: 3 times, at baseline, after implementation and one year after implementation | I: physiological; O: corporate culture and strategy | outcome evaluation | improvement the workplace environment (using the right tools, improving lighting conditions), health outcomes reducing the local muscle workloads and work-related muscle-skeletal disorder |
| [82] | as above | environmental and safety workplace intervention | 2 years; follow up | I: not applicable; O: corporate culture and strategy, financial | outcome evaluation | frequency of occupational accidents (-); conditions of work (+) and working hours (+) |
| [24] | The intervention focused on the diagnosis of occupational health; assessment measures and measures for health-promoting work organization and job design | environmental and safety workplace intervention, coping with health problems and skills development | not applicable | I: not applicable; O: corporate culture and strategy, financial | process evaluation | Factors determining the results of health promotion programs for enterprises were knowledge and attitude, support of external institutions in the process of implementation of WHP |
| [83]. | pro-health education, coronary heart disease or musculoskeletal disorders | health education and personalized counseling | 12 months | I: cognitive; O: not applicable | outcome evaluation | health promotion knowledge (+) attitude (+), subjective assessment of the usefulness of advice (+) |
| [84] | 3 Programs: Work Improvementin Neighborhood Development Program, an action-oriented training program for trade unions. Goal: improve the workplace environment, reduce the local muscle workloads, and prevent work-related muscle-skeletal disorders | multi-focused comprehensive program | two weeks | I: not applicable; O: corporate culture and strategy, financial | outcome evaluation | improvement of ergonomics and working conditions of various groups of employees (+), number of accidents (-), working hours (+), occupational cost (-) |
| Studies | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. |
|---|---|---|---|---|---|---|---|---|
| [59] | Y | Y | Y, after 1 year, after 2 and 3 years | Y | N | Y | Y | N |
| [60] | Y | Y | Y, at 6 months | Y | N | Y | Y | Y |
| [61] | Y | Y | Y, after 1 year | Y | N | Y | Y | Y |
| [62] | Y | Y | Y, after four months | N | Y | Y | N | |
| [63] | N | ND | ND | Y | Y | Y | Y | N |
| [25] | N | ND | ND | N | Y | Y | Y | N |
| [45] | Y | ND | ND | Y | Y | Y | Y | N |
| [65] | N | ND | ND | Y | Y | Y | N | N |
| [66] | Y | ND | ND | Y | Y | Y | Y | N |
| [67] | ND | ND | ND | ND | Y | Y | Y | N |
| [68] | N | Y | N | Y | N | Y | Y | N |
| [70] | Y | Y | N | Y | N | Y | Y | Y |
| [71] | N | Y | N | Y | N | Y | Y | Y |
| [72] | N | Y | N | Y | N | Y | Y | Y |
| [73] | N | Y | N | Y | N | Y | N | N |
| [74] | N | ND | ND | N | Y | N | Y | Y |
| [75] | N | Y | N | Y | N | Y | Y | Y |
| [76] | N | ND | ND | N | Y | Y | Y | Y |
| [77] | N | Y | N | Y | Y | Y | Y | N |
| [78] | N | Y | N | Y | Y | Y | Y | Y |
| [79] | Y | ND | ND | Y | Y | Y | Y | N |
| [80] | N | ND | ND | N | Y | Y | Y | N |
| [81] | N | Y | Y, after 1 year | Y | N | Y | Y | Y |
| [82] | N | ND | ND | Y | N | Y | Y | Y |
| [24] | N | ND | ND | N | Y | Y | N | N |
| [83] | N | ND | ND | N | N | Y | Y | N |
| [84] | N | ND | ND | N | N | Y | Y | N |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basińska-Zych, A.; Springer, A. Organizational and Individual Outcomes of Health Promotion Strategies—A Review of Empirical Research. Int. J. Environ. Res. Public Health 2021, 18, 383. https://doi.org/10.3390/ijerph18020383
Basińska-Zych A, Springer A. Organizational and Individual Outcomes of Health Promotion Strategies—A Review of Empirical Research. International Journal of Environmental Research and Public Health. 2021; 18(2):383. https://doi.org/10.3390/ijerph18020383
Chicago/Turabian StyleBasińska-Zych, Agata, and Agnieszka Springer. 2021. "Organizational and Individual Outcomes of Health Promotion Strategies—A Review of Empirical Research" International Journal of Environmental Research and Public Health 18, no. 2: 383. https://doi.org/10.3390/ijerph18020383
APA StyleBasińska-Zych, A., & Springer, A. (2021). Organizational and Individual Outcomes of Health Promotion Strategies—A Review of Empirical Research. International Journal of Environmental Research and Public Health, 18(2), 383. https://doi.org/10.3390/ijerph18020383