An Update on Resources, Procedures and Healthcare Provision in Pain Units: A Survey of Spanish Practitioners


 , ,
, , 
Abstract
:1. Introduction
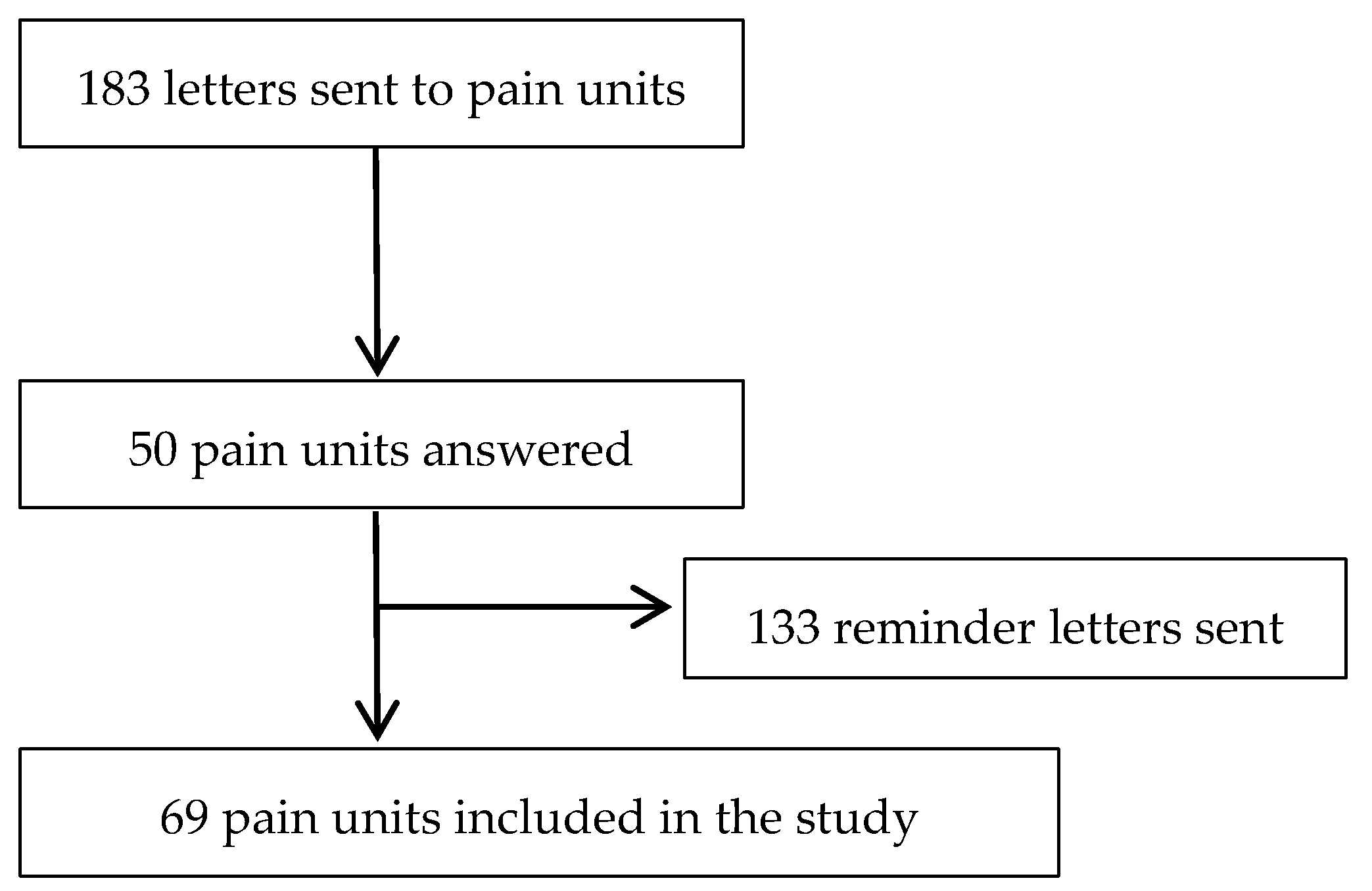
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
2.3. Statistical Analysis
2.4. Compliance with Spanish Standards
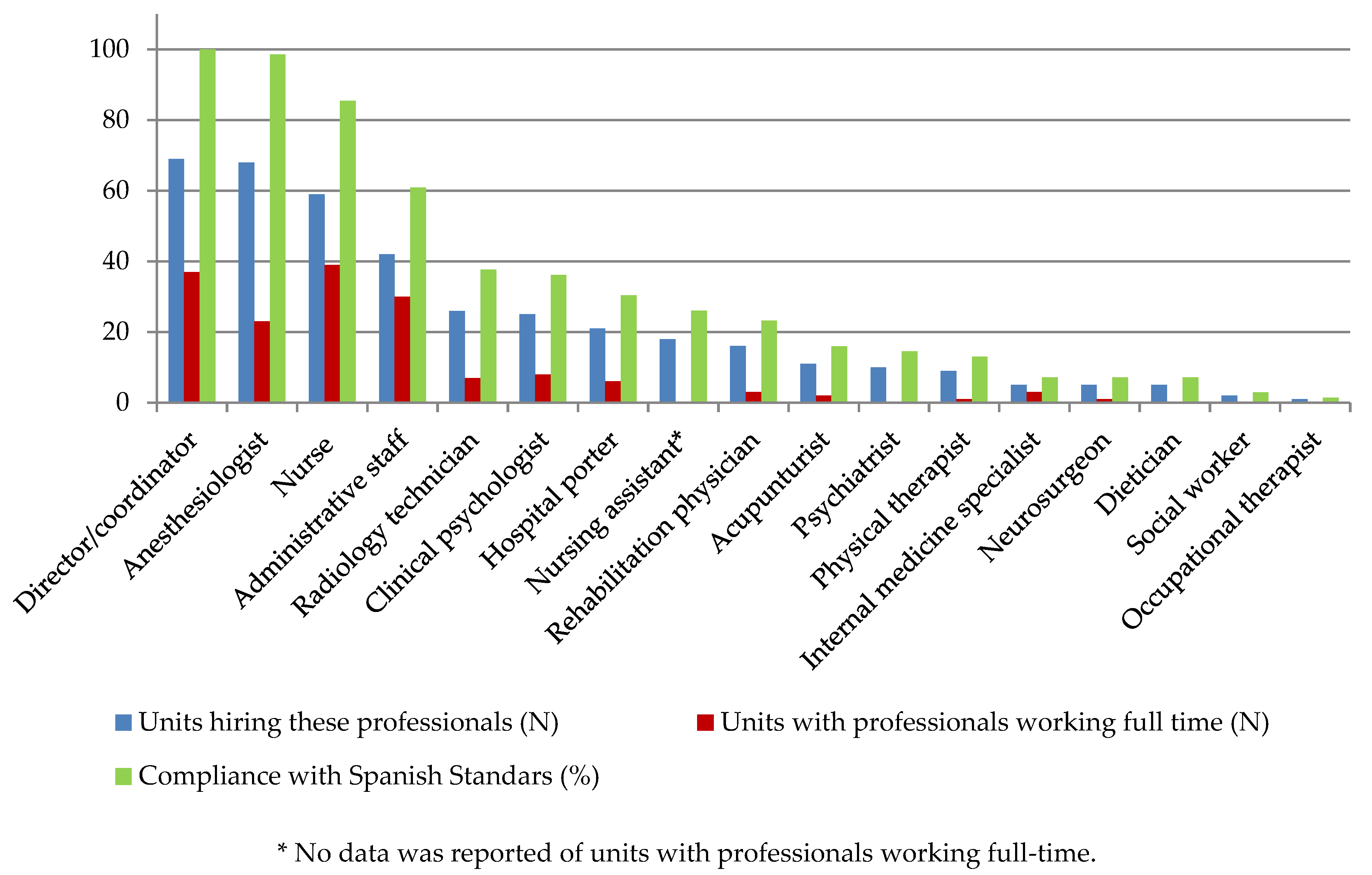
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Association for the Study of Pain. Classification of Chronic Pain, Second Edition (Revised). Available online: https://www.iasp-pain.org/PublicationsNews/Content.aspx?ItemNumber=1673 (accessed on 26 October 2020).
- Engel, L.G. The clinical application of the biopsychosocial model. J. Med. Philos. 1981, 6, 101–123. [Google Scholar] [CrossRef] [PubMed]
- Gatchel, R.J.; McGeary, D.D.; McGeary, C.A.; Lippe, B. Interdisciplinary chronic pain management: Past, present, and future. Am. Psychol. 2014, 69, 119–130. [Google Scholar] [CrossRef] [PubMed]
- GBD; Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadística. Encuesta Nacional de Salud 2017. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=resultados&idp=1254735573175#!tabs-1254736195650 (accessed on 26 October 2020).
- Alonso-García, M.; Sarría-Santamera, A. The Economic and Social Burden of Low Back Pain in Spain: A National Assessment of the Economic and Social Impact of Low Back Pain in Spain. Spine 2020, 45, E1026–E1032. [Google Scholar] [CrossRef] [PubMed]
- Palanca-Sánchez, I.; Puig-Riera, M.M.; Elola-Somoza, J.; Bernal-Sobrino, J.L.; Paniagua-Caparrós, J.L. Grupo de Expertos. In Unidad De Tratamiento De Dolor: Estándares Y Recomendaciones; Política Social e Igualdad, Ministerio de Sanidad: Madrid, Spain, 2011. [Google Scholar]
- Barutell, C. Pain units in Spain. Survey of the Spanish Society of Pain, Pain Day 2007. Rev. Soc. Esp. Dolor 2009, 16, 421–428. [Google Scholar]
- Zapata, M.M.; Catalá, E.; Rigola, M. Análisis descriptivo en el año 2001 de las Unidades de Tratamiento del Dolor Crónico en España. Rev. Esp. Anestesiol. Reanim. 2005, 52, 141–148. [Google Scholar]
- González-Escalada, J.R.; Camba, A.; Sánchez, I. Censo de las Unidades del Dolor en España: Análisis de la estructura organizativa, dotación, cartera de servicios e indicadores de calidad y buenas prácticas. Rev. Soc. Esp. Dolor 2014, 21, 149–161. [Google Scholar] [CrossRef] [Green Version]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC.: College Station, TX, USA, 2017. [Google Scholar]
- Documento Marco Para La Mejora Del Abordaje Del Dolor En el SNS. Plan de Implementación. In Estrategia Para El Abordaje De La Cronicidad En El SNS; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2014. [Google Scholar]
- International Association for the Study of Pain. Recommendations for Wait-Times for Treatment of Pain. Available online: https://www.iasp-pain.org/SearchResults.aspx (accessed on 26 October 2020).
- Gyani, A.; Shafran, R.; Layard, R.; Clark, D.M. Enhancing recovery rates: Lessons from year one or IAPT. Behav. Res. Ther. 2013, 51, 597–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, P.; Owens, T.; Harmon, D. A survey of acute pain services in teaching hospitals in the Republic of Ireland. Ir. J. Med. Sci. 2007, 176, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Erlenwein, J.; Koschwitz, R.; Pauli-Magnus, D.; Quintel, M.; Meißner, W.; Petzke, F.; Stamer, U.M. A follow-up on Acute Pain Services in Germany compared to international survey data. Eur. J. Pain 2016, 20, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Rockett, M.; Vanstone, R.; Chand, J.; Waeland, D. A survey of acute pain services in the UK. Anaesthesia 2017, 72, 1237–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boekel, R.L.M.; Steegers, M.A.H.; Verbeek Noord, I.; Sande, R.; Vissers, K.C.P. Acute pain services and postsurgical pain management in the Netherlands: A survey. Pain Pract. 2015, 15, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.C.; Martins, C.S. A survey of acute pain services in Portuguese hospitals: Are we on the right track? Eur. J. Anaesthesiol 2015, 32, 277–278. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Units n (%) 95%CI | Compliance with Spanish Standards | |
|---|---|---|
| FACILITIES (n = 69) | ||
| Which facilities are available at the pain clinic? | ||
| Consultation/treatment rooms for ambulatory visits | 69 (100) |  |
| Waiting room | 62 (89.9) (0.83–0.97) | |
| Operating theater | 50 (72.5) (0.62–0.83) |  |
| Access to block rooms | 49 (71.0) (0.60–0.82) | |
| Independent management of inpatient beds | 46 (66.7) (0.56–0.78) | |
| Room for clinic sessions/meetings/library | 36 (52.2) (0.40–0.64) | |
| Staff area (office, wardrobe, etc.) | 36 (52.2) (0.40–0.64) | |
| Administrative area | 35 (50.7) (0.39–0.63) | |
| Nursing station | 35 (50.7) (0.39–0.63) | |
| Own day hospital | 24 (34.8) (0.24–0.46) |  |
| EQUIPMENT AND SERVICES | ||
| Which material resources are available in the pain unit? (n = 69) | ||
| Patient basic monitoring equipment | 62 (89.9) (0.83–0.97) | |
| Life support and emergency resuscitative equipment | 58 (84.1) (0.75–0.93) | |
| Internet access | 67 (97.1) (0.96–0.99) | |
| Access to electronic records | 65 (94.2) (0.02–0.15) | |
| Integrated information systems to register their activity | 64 (92.8) (0.87–0.99) | |
| Direct telephonic access | 61 (88.4) (0.81–0.96) | |
| Access to physical and online resources from library databases | 55 (79.7) (0.70–0.89) | |
| Computerized records for chronic pain management with exclusive access for the pain unit | 34 (49.3) (0.38–0.61) | |
| Which material resources are available in the operating theater of the pain unit? (n = 50) | ||
| Patient monitoring equipment | 50 (100) | |
| Instrumentation for nerve blocks | 50 (100) | |
| X-ray image intensifier | 50 (100) | |
| Radiology personal protective equipment | 50 (100) | |
| Local imaging facilities (ultrasound) | 48 (96.0) (0.38–0.61) | |
| Anesthesia equipment: respirator | 46 (92.0) (0.01–0.16) | |
| Radiofrequency devices | 45 (90.0) (0.82–0.98) | |
≥75%; ≥50%–<75%; <50% of compliance with Spanish Standards.| Median (IQR) | n (%) (95%CI) | Compliance with Spanish Standards | |
|---|---|---|---|
| HEALTHCARE SERVICES PROVIDED | |||
| Number of first-time appointments | 700 (400–1334) | ||
| Number of follow-up appointments | 1987.5 (940.5–3724) | ||
| Number of diagnostic techniques applied | 216 (15–650) | ||
| Number of outpatient intervention techniques applied | 300 (24–1041) | ||
| Number of surgical intervention techniques applied | 426 (74.5–750) | ||
| Number of radiological intervention techniques applied | 0 (0–300) | ||
| CONSULTATION AND WAITING TIMES | |||
| Consultation time for standard first appointment (minutes) | 30 (30–45) | ||
| Consultation time for standard follow-up appointment (minutes) | 15 (15–20) | ||
| Consultation time for non-interventional pain treatment (minutes) | 20 (15–30) | ||
| Consultation time for interventional pain treatment (minutes) a | 30 (22.5–45) | ||
| Actual maximum waiting time for first patient appointment: | |||
| Oncologic patients (days) b | 7 (4–15) | ||
| Urgent appointments (days) c | 15 (7–30) | ||
| Non-urgent appointments (days) d | 60 (30–180) | ||
| Actual maximum waiting time for successive patient appointment: | |||
| Oncologic patients (days) b | 15 (7–30) | ||
| Urgent appointments (days) c | 25 (7–40) | ||
| Non-urgent appointments (days) d | 90 (21–180) | ||
| SHARING OF INFORMATION WITH PATIENTS | |||
| The patients receive written recommendations about their pathology | 44 (63.8) (0.52–0.75) | | |
| The patients are provided with a direct telephone number to ask questions | 53 (76.8) (0.67–0.87) | | |
| A written informed consent is requested for all interventions performed | 69 (100) | | |
| The patients are surveyed about the perceived quality of healthcare | 16 (23.2) (0.13–0.33) | | |
≥75%; of compliance with Spanish Standards.| Units n (%) (95%CI) | Median (IQR) | Compliance with Spanish Standards | |
|---|---|---|---|
| Presentations to congresses within the last 5 years (2014–2018) | |||
| National | 60 (87.0) (0.79–0.95) | 4 (3–6) | |
| International | 44 (63.8) (0.52–0.75) | 2 (1–3) | |
| Publications within the last 5 years (2014–2018) | |||
| National | 47 (68.1) (0.57–0.79) | 2 (1–2) | |
| International | 39 (56.5) (0.45–0.68) | 1 (1–6) | |
| Research projects within the last 5 years (2014–2018) | |||
| National | 48 (69.6) (0.59–0.80) | 1.5 (1–2) | |
| International | 29 (42.0) (0.30–0.54) | 1 (1–2) | |
| Rotating physicians during the last year (2018) | 46 (66.7) (0.56–0.78) | | |
| Resident physicians | N.R. | 4 (2–8) | |
| Non-resident physicians | N.R. | 2 (0–6) | |
| Training activities during the last year (2018) | 55 (79.7) (0.70–0.89) | N.R. | |
| Hospital general sessions (n = 55) | 45 (81.8) (0.72–0.92) | N.R. | |
| Courses to physicians from other departments of the hospital (n = 55) | 50 (90.9) (0.83–0.99) | N.R. | |
| Courses to primary care physicians (n = 55) | 48 (87.3) (0.79–0.96) | N.R. | |
≥75%; ≥50%–<75%; <50% of compliance with Spanish Standards.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polo-Santos, M.; Videla-Cés, S.; Pérez-Hernández, C.; Mayoral-Rojals, V.; Ribera-Canudas, M.V.; Sarría-Santamera, A. An Update on Resources, Procedures and Healthcare Provision in Pain Units: A Survey of Spanish Practitioners. Int. J. Environ. Res. Public Health 2021, 18, 451. https://doi.org/10.3390/ijerph18020451
Polo-Santos M, Videla-Cés S, Pérez-Hernández C, Mayoral-Rojals V, Ribera-Canudas MV, Sarría-Santamera A. An Update on Resources, Procedures and Healthcare Provision in Pain Units: A Survey of Spanish Practitioners. International Journal of Environmental Research and Public Health. 2021; 18(2):451. https://doi.org/10.3390/ijerph18020451
Chicago/Turabian StylePolo-Santos, Mar, Sebastián Videla-Cés, Concha Pérez-Hernández, Víctor Mayoral-Rojals, Mª Victoria Ribera-Canudas, and Antonio Sarría-Santamera. 2021. "An Update on Resources, Procedures and Healthcare Provision in Pain Units: A Survey of Spanish Practitioners" International Journal of Environmental Research and Public Health 18, no. 2: 451. https://doi.org/10.3390/ijerph18020451
APA StylePolo-Santos, M., Videla-Cés, S., Pérez-Hernández, C., Mayoral-Rojals, V., Ribera-Canudas, M. V., & Sarría-Santamera, A. (2021). An Update on Resources, Procedures and Healthcare Provision in Pain Units: A Survey of Spanish Practitioners. International Journal of Environmental Research and Public Health, 18(2), 451. https://doi.org/10.3390/ijerph18020451