Participation Profile of Children and Youth, Aged 6–14, with and without ADHD, and the Impact of Environmental Factors



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Instruments
2.3.1. A demographic Questionnaire
2.3.2. The Attention Deficit and Hyperactivity Screening Questionnaire
2.3.3. The Participation and Environment Measure for Children and Youth (PEM-CY)
2.4. Procedure
2.5. Data Analysis
3. Results
3.1. Comparison of Participation and the Overall Environmental Support between Groups in the Different Settings
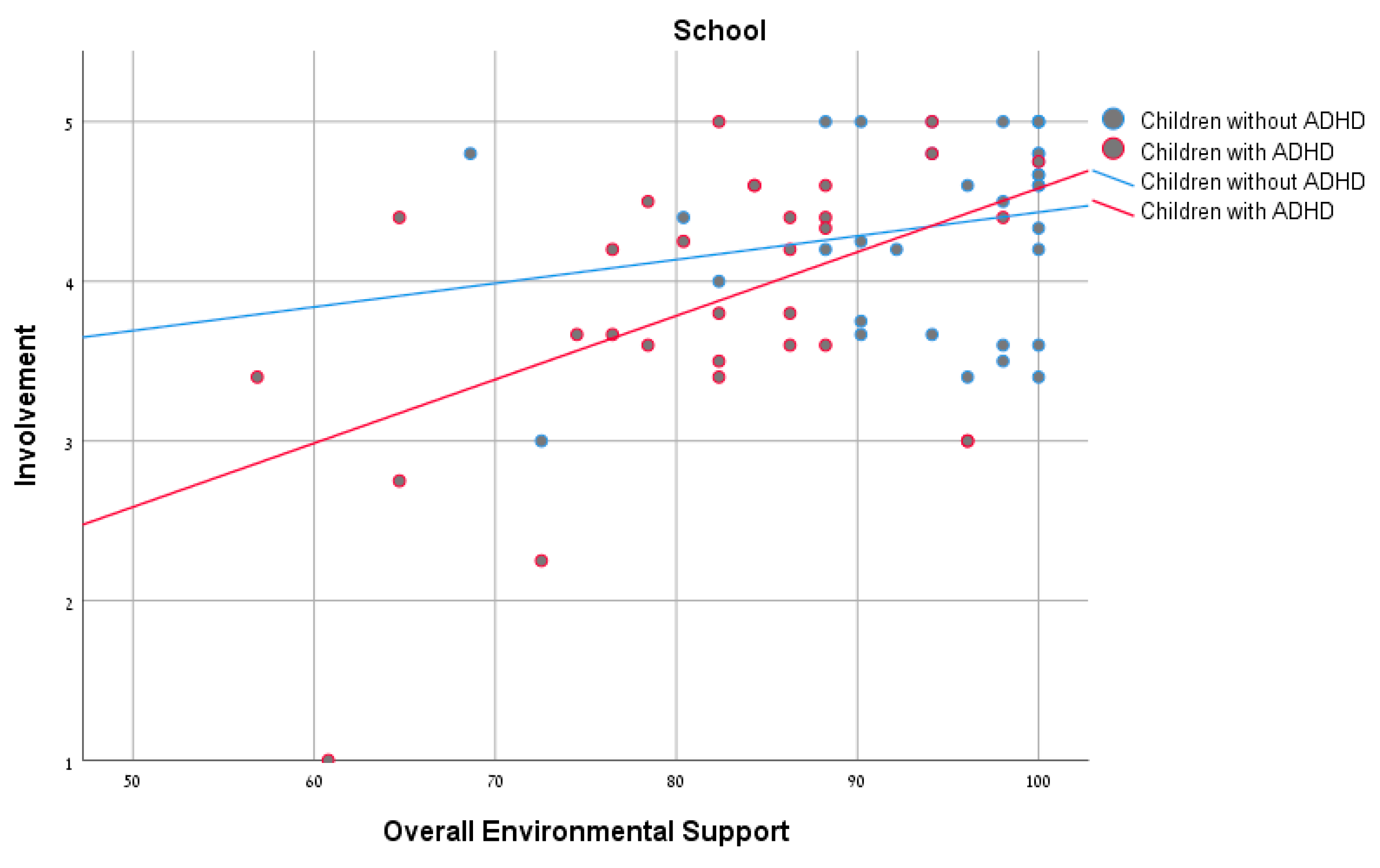
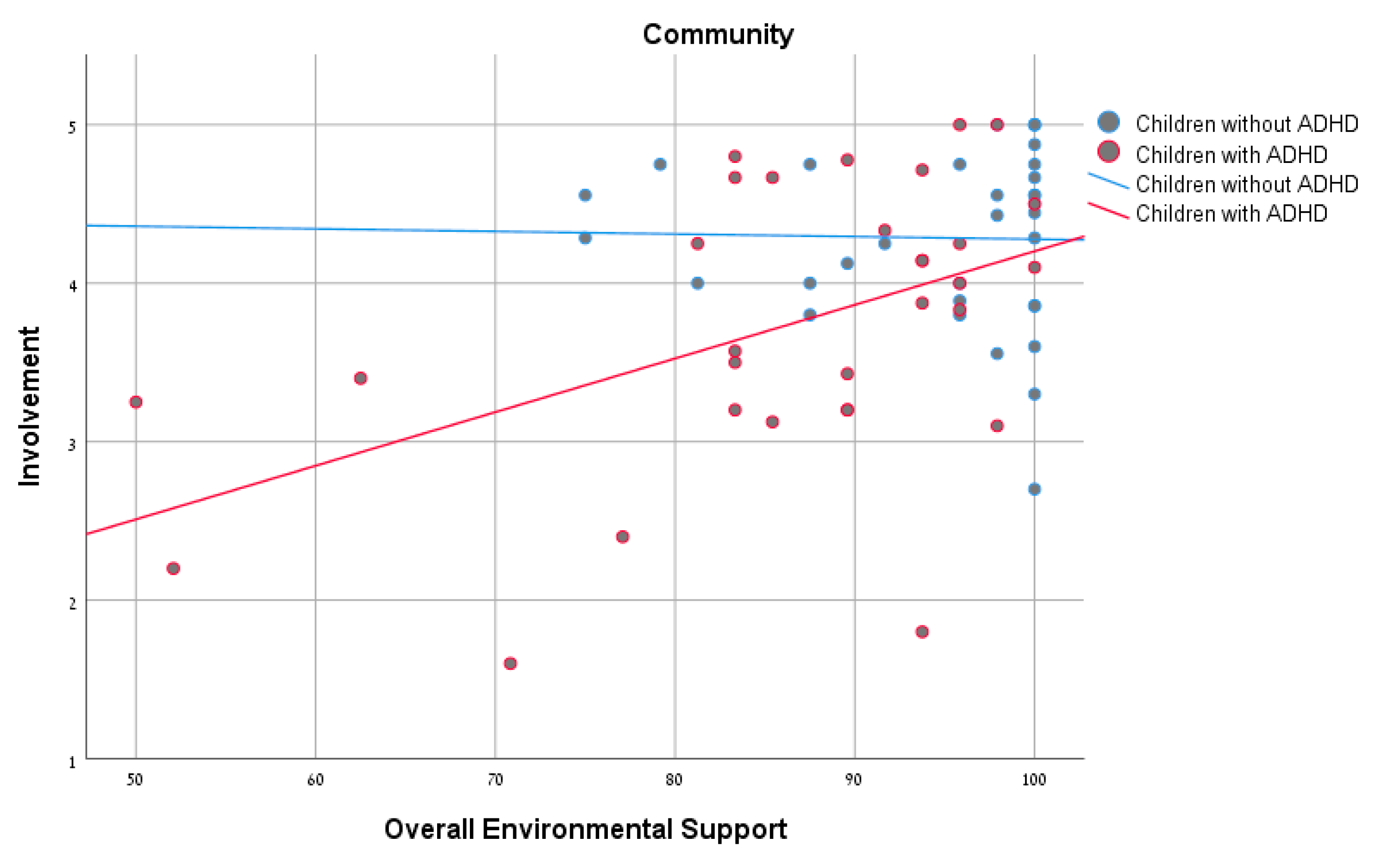
3.2. Correlation between Overall Environmental Support and Participation Patterns in all Settings and for Each of the Groups
3.3. Differences in Participation Patterns and Prevalence of Environmental Factors Impacting the ADHD Group
4. Discussion
4.1. Comparison of Participation Patterns, Desire for Change, and Overall Environmental Supports
4.2. Relationship between Overall Environmental Support and Participation Patterns
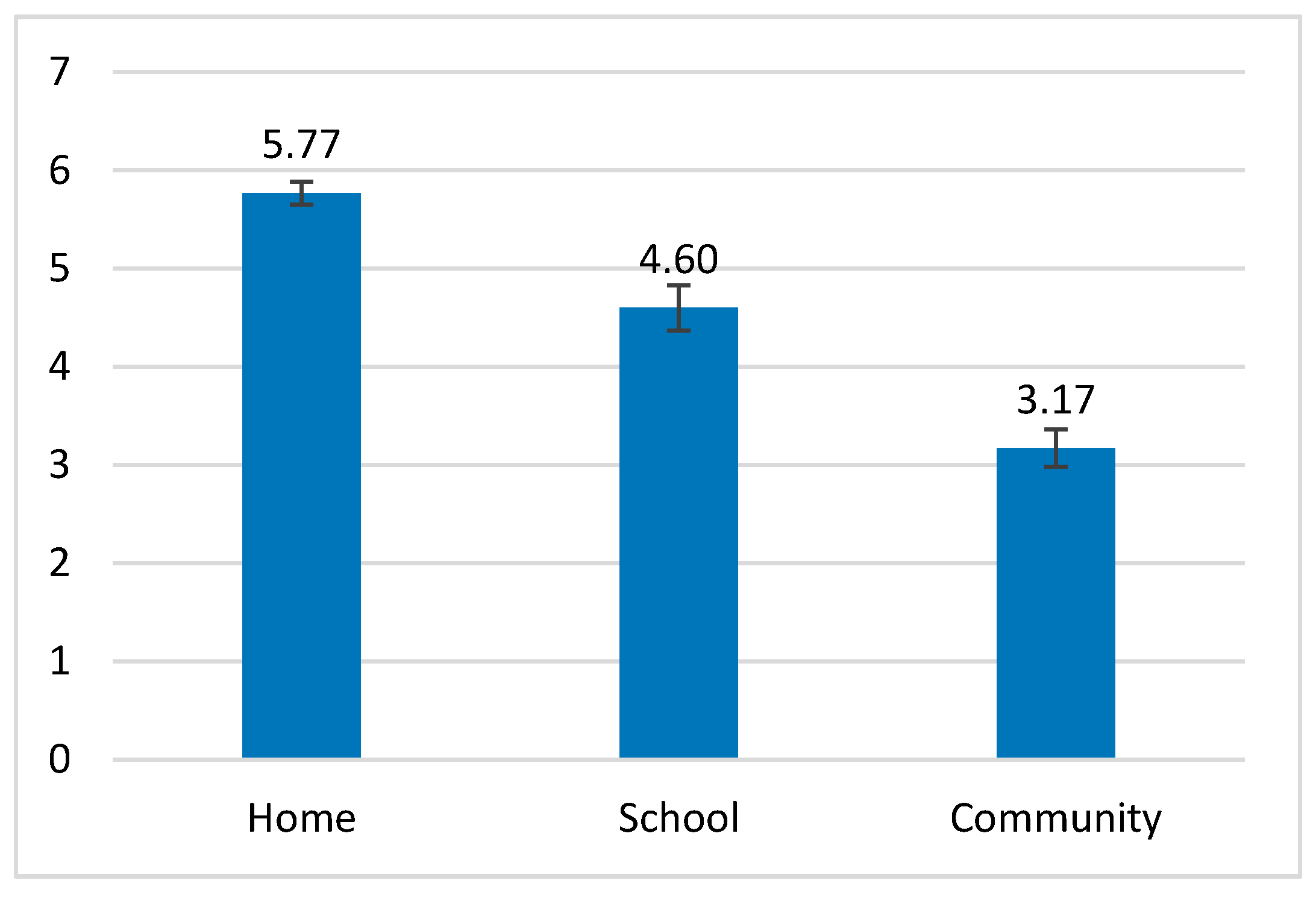
4.3. Comparison of Frequency and Involvement between the Different Settings and a Description of the Environmental Factors
4.4. Research Limitations and Recommendations for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); WHO: Geneva, Switzerland, 2001. [Google Scholar]
- Rainey, L.; van Nispen, R.; van der Zee, C.; van Rens, G. Measurement properties of questionnaires assessing participation in children and adolescents with a disability: A systematic review. Qual. Life Res. 2014, 23, 2793–2808. [Google Scholar] [CrossRef] [PubMed]
- American Occupational Therapy Association (AOTA). Occupational therapy practice framework: Domain and process, 4th ed. Am. J. Occup. Ther. 2020, 74, 7412410010p1–7412410010p87. [Google Scholar] [CrossRef]
- Law, M. Participation in the occupations of everyday life. Am. J. Occup. Ther. 2002, 56, 640–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodger, S.; Ziviani, J. Occupational Therapy with Children: Understanding Children’s Occupations and Enabling Participation; Blackwell: Oxford, UK, 2006. [Google Scholar]
- Law, M.; Anaby, D.; DeMatteo, C.; Hanna, S. Participation patterns of children with acquired brain injury. Brain Inj. 2011, 25, 587–595. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.; Khetani, M.; Cousins, M.; Teplicky, R. Development of the participation and environment measure for children and youth: Conceptual basis. Disabil. Rehabil. 2012, 34, 238–246. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.M. Participation and Environment Measure for Children and Youth (PEM-CY); Boston University: Boston, MA, USA, 2010. [Google Scholar]
- Granlund, M. Participation–challenges in conceptualization, measurement and intervention. Child Care Health Dev. 2013, 39, 470–473. [Google Scholar] [CrossRef]
- Imms, C.; Adair, B.; Keen, D.; Ullenhag, A.; Rosenbaum, P.; Granlund, M. ‘Participation’: A systematic review of language, definitions, and constructs used in intervention research with children with disabilities. Dev. Med. Child Neurol. 2016, 58, 29–38. [Google Scholar] [CrossRef]
- Anaby, D.; Law, M.; Coster, W.; Bedell, G.; Khetani, M.; Avery, L.; Teplicky, R. The mediating role of the environment in explaining participation of children and youth with and without disabilities across home, school, and community. Arch. Phys. Med. Rehabil. 2014, 95, 908–917. [Google Scholar] [CrossRef]
- Coster, W.; Bedell, G.; Law, M.; Khetani, M.A.; Teplicky, R.; Liljenquist, K.; Gleason, K.; Kao, Y.C. Psychometric evaluation of the Participation and Environment Measure for Children and Youth. Dev. Med. Child Neurol. 2011, 53, 1030–1037. [Google Scholar] [CrossRef]
- Jeong, Y.; Law, M.; Stratford, P.; DeMatteo, C.; Missiuna, C. Measuring participation of children and environmental factors at home, school, and in community: Construct validation of the Korean PEM-CY. Phys. Occup. Ther. Pediatr. 2017, 37, 541–554. [Google Scholar] [CrossRef]
- Bedell, G.; Coster, W.; Law, M.; Liljenquist, K.; Kao, Y.C.; Teplicky, R.; Anaby, D.; Khetani, M.A. Community participation, supports, and barriers of school-age children with and without disabilities. Arch. Phys. Med. Rehabil. 2013, 94, 315–323. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.; Liljenquist, K.; Kao, Y.C.; Khetani, M.; Teplicky, R. School participation, supports and barriers of students with and without disabilities. Child Care Health Dev. 2013, 39, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Anaby, D.; Teplicky, R.; Khetani, M.A.; Coster, W.; Bedell, G. Participation in the home environment among children and youth with and without disabilities. Br. J. Occup. Ther. 2013, 76, 58–66. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, USA, 2013. [Google Scholar]
- Faraone, S.; Asherson, P.; Banaschewski, T.; Biederman, J.; Buitelaar, J.K.; Ramos-Quiroga, J.A.; Rohde, L.A.; Sonuga-Barke, E.J.S.; Tannock, R.; Barbara, F. Attention-deficit/hyperactivity disorder. Nature Rev. Dis. Prim. 2015, 1, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Shimoni, M.A.; Engel-Yeger, B.; Tirosh, E. Participation in leisure activities among boys with attention deficit hyperactivity disorder. Res. Dev. Disabil. 2010, 31, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Engel-Yeger, B.; Ziv-On, D. The relationship between sensory processing difficulties and leisure activity preference of children with different types of ADHD. Res. Dev. Disabil. 2011, 32, 1154–1162. [Google Scholar] [CrossRef]
- García-Castellar, R.; Jara-Jiménez, P.; Sánchez-Chiva, D.; Mikami, A.Y. Social skills deficits in a virtual environment among Spanish children with ADHD. J. Atten. Disor. 2018, 22, 776–786. [Google Scholar] [CrossRef]
- Ros, R.; Graziano, P.A. Social functioning in children with or at risk for attention deficit/hyperactivity disorder: A meta-analytic review. J. Clin. Child Adol. Psych. 2018, 47, 213–235. [Google Scholar] [CrossRef]
- Daley, D.; Birchwood, J. ADHD and academic performance: Why does ADHD impact on academic performance and what can be done to support ADHD children in the classroom? Child Care Health Dev. 2010, 36, 455–464. [Google Scholar] [CrossRef]
- Frazier, T.W.; Youngstrom, E.A.; Glutting, J.J.; Watkins, M.W. ADHD and achievement: Meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. J. Learn. Disabil. 2007, 40, 49–65. [Google Scholar] [CrossRef] [Green Version]
- Birchwood, J.; Daley, D. Brief report: The impact of attention deficit hyperactivity disorder (ADHD) symptoms on academic performance in an adolescent community sample. J. Adol. 2012, 35, 225–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, K.M.; Pelham, W.E.; Molina, B.S.; Sibley, M.H.; Waschbusch, D.A.; Yu, J.; Gnagy, E.M.; Biswas, A.; Badinski, D.E.; Karch, K.M. The academic experience of male high school students with ADHD. J. Abnorm. Child Psych. 2011, 39, 451–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harpin, V.A. The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch. Dis. Child. 2005, 90, i2–i7. [Google Scholar] [CrossRef] [PubMed]
- Lavi, G.; Maeir, A.; Traub Bar-Ilan, R.; Levanon-Erez, N. The relationship between executive functions and participation among adolescents with and without attention deficit hyperactivity disorder (ADHD). Isr. J. Occup. Ther. 2017, 26, H250–H266. [Google Scholar]
- Hammel, J.; Magasi, S.; Heinemann, A.; Gray, D.B.; Stark, S.; Kisala, P.; Carlozzi, N.E.; Tulsky, D.; Garcia, S.F.; Hahn, E.A. Environmental barriers and supports to everyday participation: A qualitative insider perspective from people with disabilities. Arch. Phys. Med. Rehabil. 2015, 96, 578–588. [Google Scholar] [CrossRef]
- Rosenberg, L.; Ratzon, N.Z.; Jarus, T.; Bart, O. Perceived environmental restrictions for the participation of children with mild developmental disabilities. Child Care Health Dev. 2012, 38, 836–843. [Google Scholar] [CrossRef]
- Bedell, G.M.; Khetani, M.A.; Cousins, M.A.; Coster, W.J.; Law, M.C. Parent perspectives to inform development of measures of children’s participation and environment. Arch. Phys. Med. Rehabil. 2011, 92, 765–773. [Google Scholar] [CrossRef]
- Anaby, D.; Hand, C.; Bradley, L.; DiRezze, B.; Forhan, M.; DiGiacomo, A.; Law, M. The effect of the environment on participation of children and youth with disabilities: A scoping review. Disabil. Rehabil. 2013, 35, 1589–1598. [Google Scholar] [CrossRef]
- Egilson, S.T.; Jakobsdóttir, G.; Ólafsson, K.; Leósdóttir, T. Community participation and environment of children with and without autism spectrum disorder: Parent perspectives. Scand. J. Occup. Ther. 2017, 24, 187–196. [Google Scholar] [CrossRef]
- Izadi-Najafabadi, S.; Ryan, N.; Ghafooripoor, G.; Gill, K.; Zwicker, J.G. Participation of children with developmental coordination disorder. Res. Dev. Disabil. 2019, 84, 75–84. [Google Scholar] [CrossRef]
- De Schipper, E.; Lundequist, A.; Wilteus, A.L.; Coghill, D.; De Vries, P.J.; Granlund, M.; Holtmann, M.; Jonsson, U.; Karande, S.; Levy, F.; et al. Comprehensive scoping review of ability and disability in ADHD using the International Classification of Functioning, Disability and Health-Children and Youth Version (ICF-CY). Euro. Child Adol. Psych. 2015, 24, 859–872. [Google Scholar] [CrossRef] [PubMed]
- Mahdi, S.; Viljoen, M.; Massuti, R.; Selb, M.; Almodayfer, O.; Karande, S.; de Vries, P.J.; Rohde, L.; Bölte, S. An international qualitative study of ability and disability in ADHD using the WHO-ICF framework. Euro. Child Adol. Psych. 2017, 26, 1219–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lasky, A.K.; Weisner, T.S.; Jensen, P.S.; Hinshaw, S.P.; Hechtman, L.; Arnold, L.E.; Murray, D.E.; Swanson, J.M. ADHD in context: Young adults’ reports of the impact of occupational environment on the manifestation of ADHD. Soc. Sci. Med. 2016, 161, 160–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dvorsky, M.R.; Langberg, J.M. A review of factors that promote resilience in youth with ADHD and ADHD symptoms. Clin. Child Fam. Psych. Rev. 2016, 19, 368–391. [Google Scholar] [CrossRef]
- IBM. SPSS Statistics for Macintosh; Version 25.0; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- Stevens, J. Applied Multivariate Statistics for the Social Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2002. [Google Scholar]
- Wehmeier, P.M.; Schacht, A.; Barkley, R.A. Social and emotional impairment in children and adolescents with ADHD and the impact on quality of life. J. Adol. Health 2010, 46, 209–217. [Google Scholar] [CrossRef]
- Guimarães Mendes, C.; Cotta Mancini, M.; Marques Miranda, D. Household task participation of children and adolescents with ADHD: A systematic review. Brazil. J. Occup. Ther. 2018, 26, 658–667. [Google Scholar]
- Dunn, L.; Coster, W.J.; Orsmond, G.I.; Cohn, E.S. Household task participation of children with and without attentional problems. Phys. Occup. Ther. Pediatr. 2009, 29, 258–273. [Google Scholar] [CrossRef]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.E. ADD/ADHD and impaired executive function in clinical practice. Curr. Atten. Disabil. Rep. 2009, 1, 37–41. [Google Scholar] [CrossRef]
- Mangeot, S.D.; Miller, L.J.; McIntosh, D.N.; McGrath-Clarke, J.; Simon, J.; Hagerman, R.J.; Goldson, E. Sensory modulation dysfunction in children with attention-deficit-hyperactivity disorder. Dev. Med. Child Neurol. 2001, 43, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Pfeifer, L.I.; Terra, L.N.; dos Santos, J.L.F.; Stagnitti, K.E.; Panúncio-Pinto, M.P. Play preference of children with ADHD and typically developing children in Brazil: A pilot study. Austr. Occup. Ther. J. 2001, 58, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Larson, K.; Russ, S.A.; Kahn, R.S.; Halfon, N. Patterns of comorbidity, functioning, and service use for US children with ADHD, 2007. Pediatrics 2011, 127, 462–470. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Children and Youth with ADHD | Children and Youth without ADHD | ||||||
|---|---|---|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | ||||
| Age | 31 | 10.37 (1.83) | 34 | 9.48 (1.83) | t(63) = −1.95 a | p = 0.056 | |
| n | % | n | % | ||||
| Gender | male | 20 | 64.52 | 22 | 64.71 | χ2(1) = 0.0 b | p = 0.987 |
| female | 11 | 35.48 | 12 | 35.29 | |||
| Socioeconomic status | below average | 3 | 9.68 | 0 | - | χ2(2) = 3.50 b | p = 0.174 |
| average | 14 | 45.16 | 16 | 47.06 | |||
| above average | 14 | 45.16 | 18 | 52.94 | |||
| Measure | Setting | With ADHD (n = 31) | Without ADHD (n = 34) | F(1, 63) | η2 |
|---|---|---|---|---|---|
| mean (SD) | mean (SD) | ||||
| Frequency (8-point scale) | Home | 5.77 (0.66) | 6.08 (0.45) | 5.10 * | 0.08 |
| School | 4.60 (1.28) | 4.35 (0.93) | 0.85 | 0.01 | |
| Community | 3.17 (1.06) | 3.61 (0.80) | 3.60 | 0.05 | |
| Involvement (5-point scale) | Home | 3.50 (0.60) | 4.30 (0.39) | 41.55 *** | 0.40 |
| School | 3.89 (0.86) | 4.35 (0.59) | 6.40 ** | 0.09 | |
| Community | 3.74 (0.91) | 4.30 (0.54) | 9.12 ** | 0.13 | |
| mean in percent (SD) | mean in percent (SD) | ||||
| Desire for change | Home | 68.92 (24.21) | 47.35 (23.23) | 13.43 *** | 0.18 |
| School | 47.58 (33.59) | 32.45 (30.45) | 3.63 | 0.05 | |
| Community | 42.90 (24.56) | 27.64 (22.47) | 6.85 ** | 0.10 | |
| Overall environmental support | Home | 83.78 (8.58) | 94.11 (6.38) | 27.52 *** | 0.31 |
| School | 82.54 (10.67) | 94.89 (6.76) | 30.98 *** | 0.33 | |
| Community | 96.42 (12.66) | 94.82 (7.67) | 10.45 ** | 0.14 |
| Overall Environmental Support | ||
|---|---|---|
| Children with ADHD (n = 31) | Children without ADHD (n = 34) | |
| Frequency | ||
| Home | 0.06 | 0.23 |
| School | 0.27 | 0.3 |
| Community | 0.03 | 0.24 |
| Involvement | ||
| Home | 0.38 * | 0.37 * |
| School | 0.49 ** | 0.2 |
| Community | 0.47 ** | −0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shabat, T.; Fogel-Grinvald, H.; Anaby, D.; Golos, A. Participation Profile of Children and Youth, Aged 6–14, with and without ADHD, and the Impact of Environmental Factors. Int. J. Environ. Res. Public Health 2021, 18, 537. https://doi.org/10.3390/ijerph18020537
Shabat T, Fogel-Grinvald H, Anaby D, Golos A. Participation Profile of Children and Youth, Aged 6–14, with and without ADHD, and the Impact of Environmental Factors. International Journal of Environmental Research and Public Health. 2021; 18(2):537. https://doi.org/10.3390/ijerph18020537
Chicago/Turabian StyleShabat, Tair, Haya Fogel-Grinvald, Dana Anaby, and Anat Golos. 2021. "Participation Profile of Children and Youth, Aged 6–14, with and without ADHD, and the Impact of Environmental Factors" International Journal of Environmental Research and Public Health 18, no. 2: 537. https://doi.org/10.3390/ijerph18020537
APA StyleShabat, T., Fogel-Grinvald, H., Anaby, D., & Golos, A. (2021). Participation Profile of Children and Youth, Aged 6–14, with and without ADHD, and the Impact of Environmental Factors. International Journal of Environmental Research and Public Health, 18(2), 537. https://doi.org/10.3390/ijerph18020537