The Prevalence of Virulent and Multidrug-Resistant Enterococci in River Water and in Treated and Untreated Municipal and Hospital Wastewater


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling Sites and Methods
2.2. Determination of Physicochemical Parameters
2.3. Isolation of Enterococci from Samples of River Water and Wastewater
2.4. Identification of Enterococci to Genus and Species Level
2.5. Determination of Enterococcus Susceptibility to Antimicrobial Drugs
2.6. Isolation of Genomic DNA and PCR Conditions
2.7. Identification of Enterococci and Detection of Vancomycin Resistance Genes and Virulence Factors by PCR
2.8. Statistical Analysis
3. Results
3.1. Physicochemical Parameters
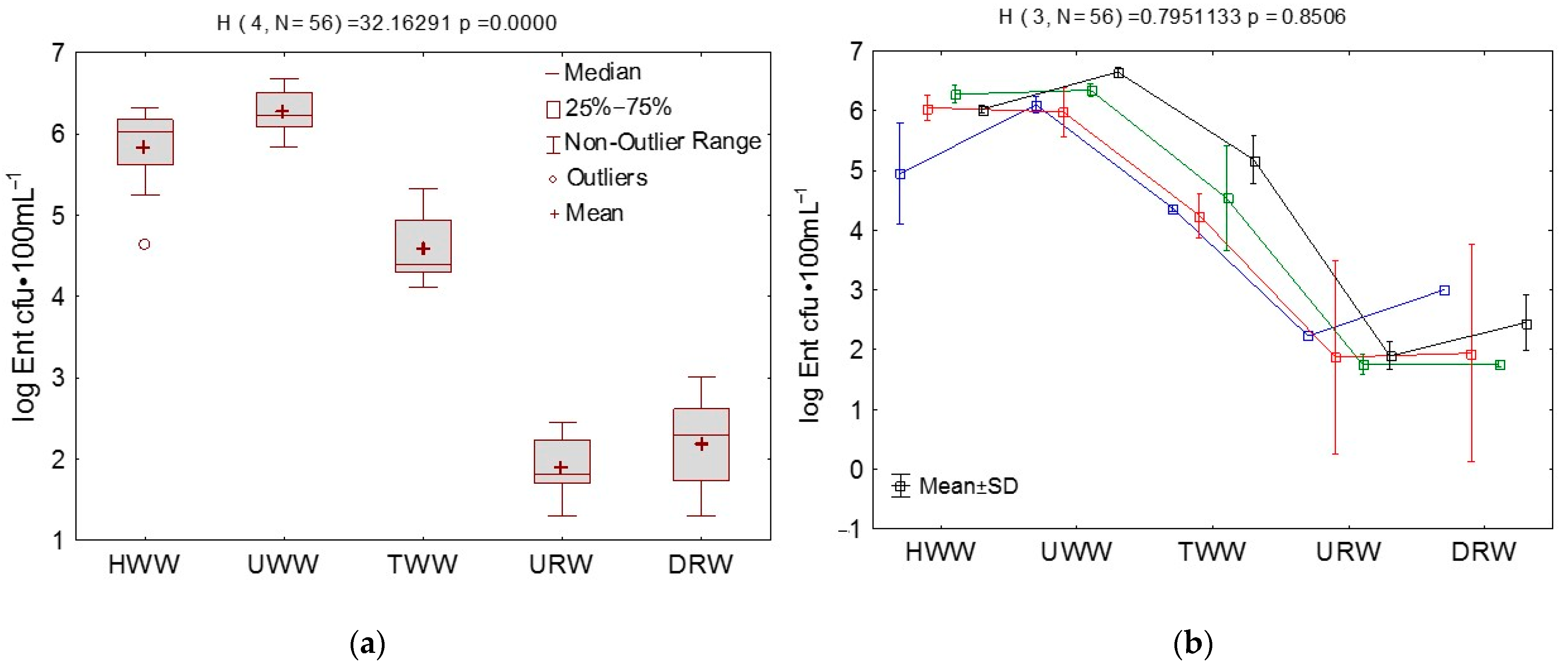
3.2. Microbial Counts in Wastewater and River Water Determined by the Culture-Dependent Method
3.3. Analysis of Correlations between Enterococci, Vancomycin Resistance Genes, Virulence Factors, Physicochemical Parameters, Sampling Site, and Season
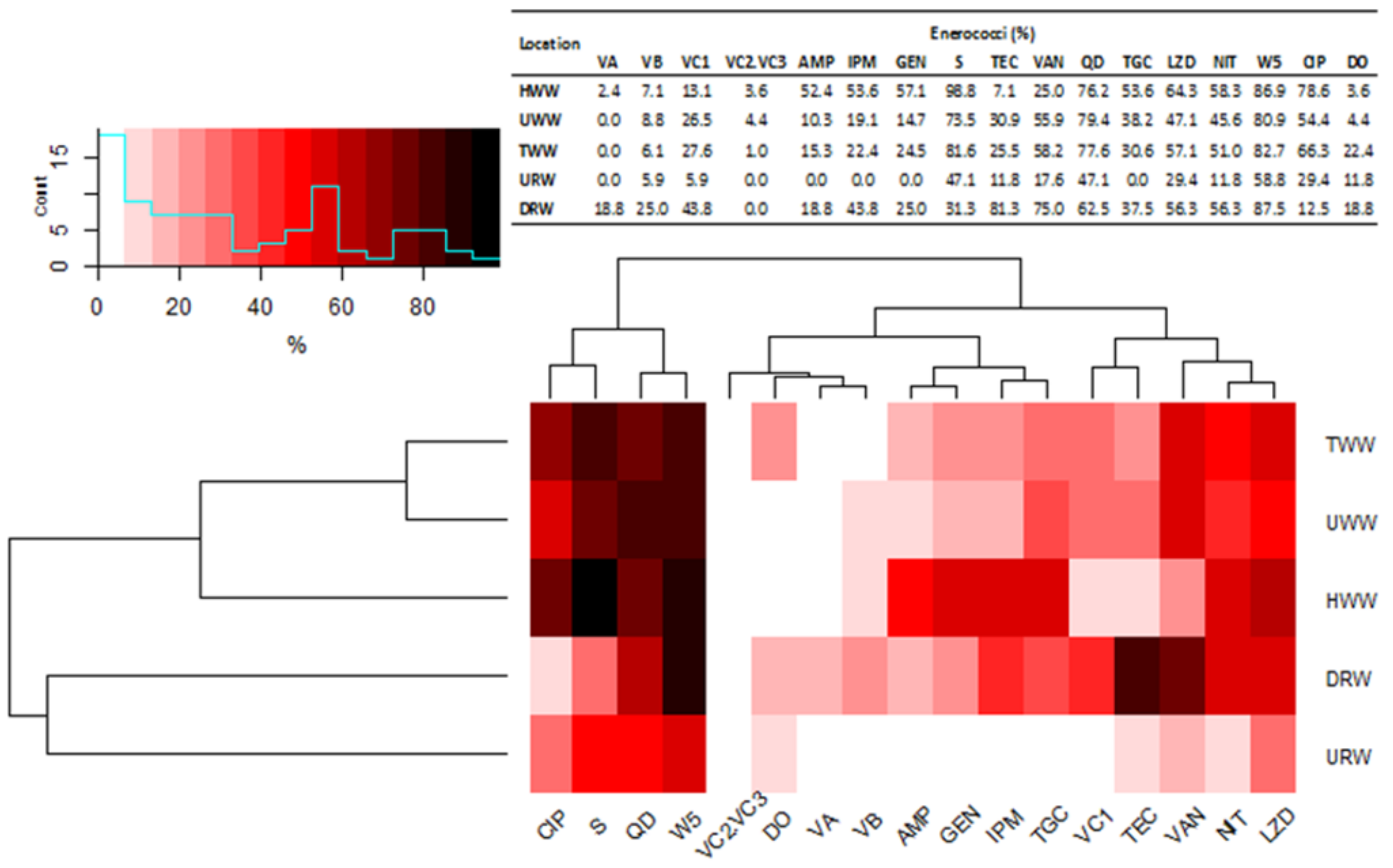
3.4. Species Diversity, Percentage Composition and Multidrug Resistance of Enterococci in Samples of River Water and Wastewater
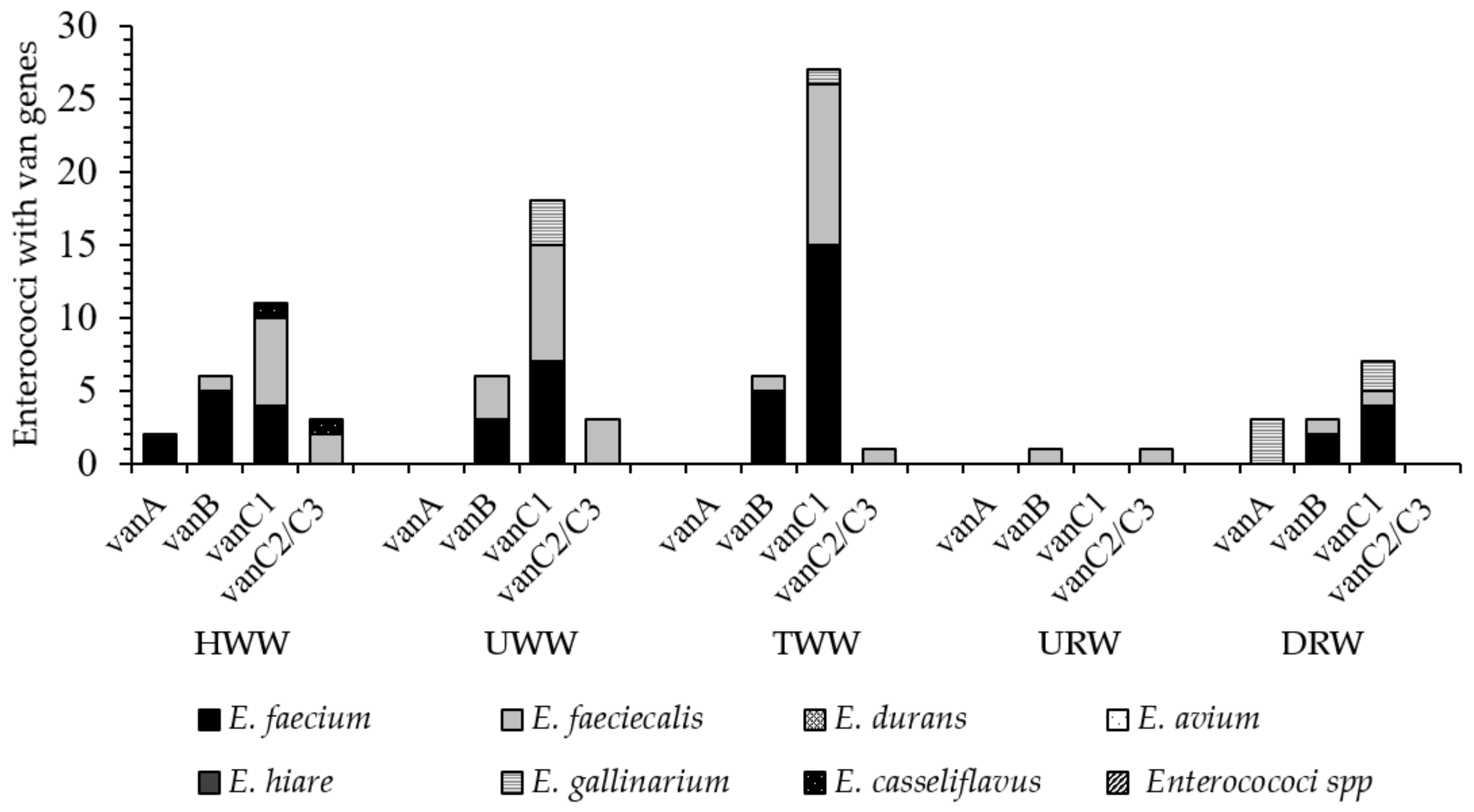
3.5. Identification of Vancomycin Resistance Genes (Van) in Enterococci Isolated from Wastewater and River Water
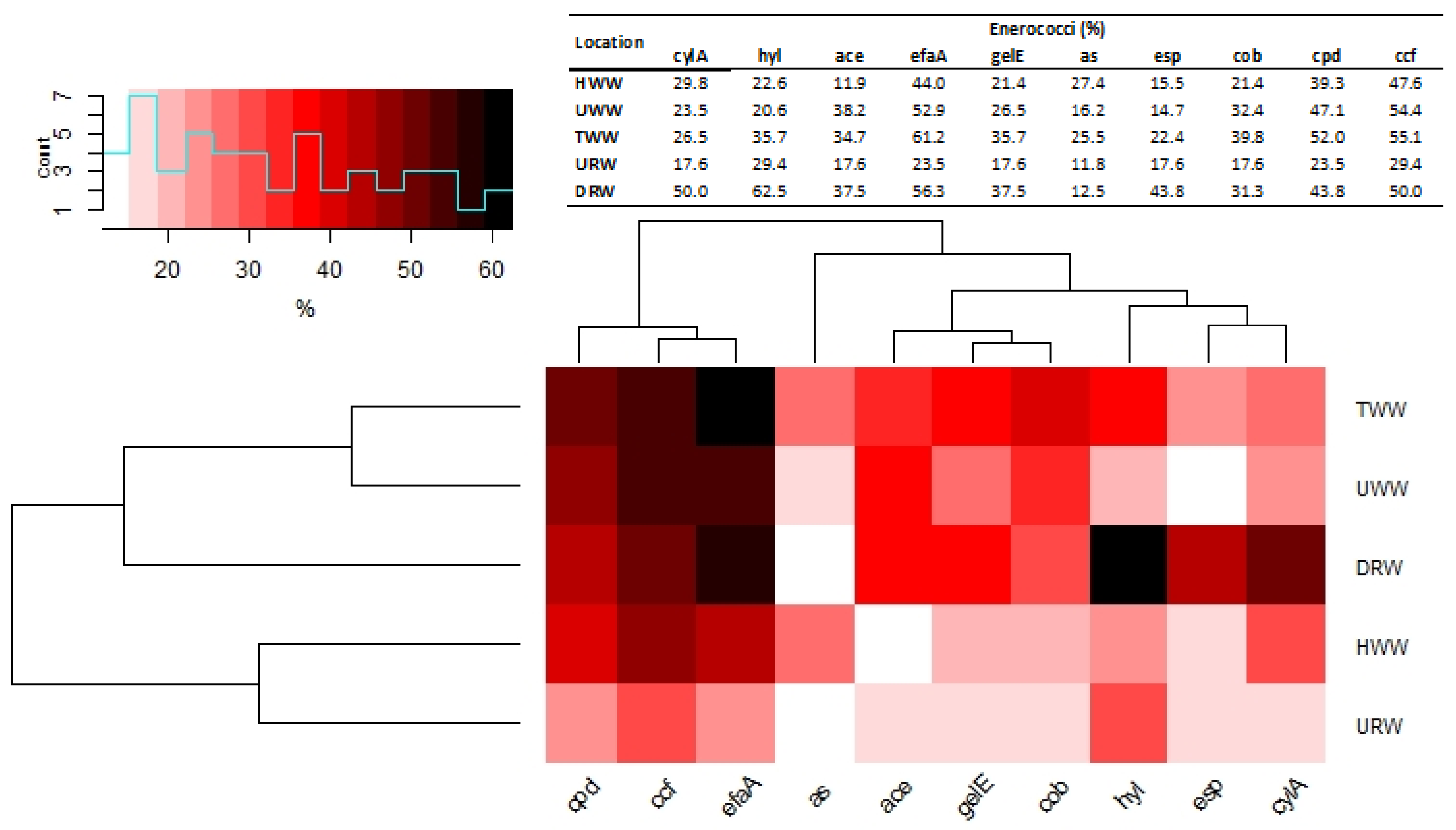
3.6. Identification of Genes Encoding Virulence Factors in Enterococci Isolated from Wastewater and River Water
4. Discussion
4.1. Enterococcus Counts in Wastewater and River Water Samples
4.2. Species Composition, Multidrug Resistance and the Presence of Van Genes in Enterococci Isolated from Water and Wastewater Samples
4.3. Characteristics of Virulent Enterococci in Wastewater and River Water Samples
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harnisz, M.; Kiedrzyńska, E.; Kiedrzyński, M.; Korzeniewska, E.; Czatzkowska, M.; Koniuszewska, I.; Joźwik, A.; Szklarek, S.; Niestępski, S.; Zalewski, M. The impact of WWTP size and sampling season on the prevalence of antibiotic resistance genes in wastewater and the river system. Sci. Total Environ. 2020, 741, 140466. [Google Scholar] [CrossRef] [PubMed]
- Lekunberri, I.; Villagrasa, M.; Balcázar, J.L.; Borrego, C.M. Contribution of bacteriophage and plasmid DNA to the mobilization of antibiotic resistance genes in a river receiving treated wastewater discharges. Sci. Total Environ. 2017, 601–602, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Niestępski, S.; Harnisz, M.; Ciesielski, S.; Korzeniewska, E.; Osińska, A. Environmental fate of Bacteroidetes, with particular emphasis on Bacteroides fragilis group bacteria and their specific antibiotic resistance genes, in activated sludge wastewater treatment plants. J. Hazard. Mater. 2020, 394, 122544. [Google Scholar] [CrossRef] [PubMed]
- Bojarczuk, A.; Jelonkiewicz, Ł.; Lenart-Boroń, A. The effect of anthropogenic and natural factors on the prevalence of physicochemical parameters of water and bacterial water quality indicators along the river Białka, southern Poland. Environ. Sci. Pollut. Res. 2018, 25, 10102–10114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glińska-Lewczuk, K.; Gołaś, I.; Koc, J.; Gotkowska-Płachta, A.; Harnisz, M.; Rochwerger, A. The impact of urban areas on the water quality gradient along a lowland river. Environ. Monit. Assess. 2016, 188, 624–638. [Google Scholar] [CrossRef] [PubMed]
- Gotkowska-Płachta, A.; Gołaś, I.; Korzeniewska, E.; Koc, J.; Rochwerger, A.; Solarski, K. Evaluation of the distribution of fecal indicator bacteria in a river system depending on different types of land use in the southern watershed of the Baltic Sea. Environ. Sci. Pollut. Res. 2016, 23, 4073–4085. [Google Scholar] [CrossRef] [PubMed]
- Byappanahalli, M.N.; Nevers, M.B.; Korajkic, A.; Staley, Z.R.; Harwood, V.J. Enterococci in the environment. Microbiol. Mol. Biol. Rev. 2012, 76, 685–706. [Google Scholar] [CrossRef] [Green Version]
- Staley, C.; Dunny, G.M.; Sadowsky, M.J. Environmental and Animal-associated enterococci. Adv. Appl. Microbiol. 2014, 147–186. [Google Scholar] [CrossRef]
- Kampmeier, S.; Kossow, A.; Clausen, L.M.; Knaack, D.; Ertmer, C.; Gottschalk, A.; Freise, H.; Mellmann, A. Hospital acquired vancomycin resistant enterococci in surgical intensive care patients—A prospective longitudinal study. Antimicrob. Resist. Infect. Control 2018, 7, 103. [Google Scholar] [CrossRef]
- Recreational Water Quality Criteria; Office of Water, United States Environmental Protection Agency: Washington, DC, USA, 2012.
- Zielińska, D.; Kolożyn-Krajewska, D. Food-origin lactic acid bacteria may exhibit probiotic properties: Review. Biomed Res. Int. 2018, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Lata, P.; Ram, S.; Agrawal, M.; Shanker, R. Enterococci in river Ganga surface waters: Propensity of species distribution; dissemination of antimicrobial–resistance and virulence–markers among species along landscape. BMC Microbiol. 2009, 9, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Servais, P.; Passerat, J. Antimicrobial resistance of fecal bacteria in waters of the Seine river watershed (France). Sci. Total Environ. 2009, 408, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Sadowy, E.; Łuczkiewicz, A. Drug–resistant and hospital–associated Enterococcus faecium from wastewater, riverine estuary and anthropogenically impacted marine catchment basin. BMC Microbiol. 2014, 14, 66. [Google Scholar] [CrossRef] [Green Version]
- Boehm, A.B.; Sassoubre, L.M. Enterococci as indicators of environmental fecal contamination. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infections; Gilmore, M.S., Clewell, D.B., Ike, Y., Shankar, N., Eds.; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014; pp. 1–31. [Google Scholar]
- Franz, C.M.A.P.; Huch, M.; Abriouel, H.; Holzapfel, W.; Galvez, A. Enterococci as probiotics and their implications in food safety. Int. J. Food Microbiol. 2011, 151, 125–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, W.; Howden, B.P.; Stinear, T.P. Evolution of virulence in Enterococcus faecium, a hospital–adapted opportunistic pathogen. Curr. Opin. Microbiol. 2018, 41, 76–82. [Google Scholar] [CrossRef]
- Talaga-Ćwiertnia, K.; Bulanda, M. Drug resistance in the genus enterococcus-current problem in humans and animals. Post. Mikrob. Adv. Microbiol. 2018, 57, 244–250. [Google Scholar] [CrossRef]
- O’Driscoll, T.; Crank, C.W. Vancomycin–resistant enterococcal infections: Epidemiology, clinical manifestations, and optimal management. Infect. Drug Resist. 2015, 8, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, U.; Garg, A.; Tiwari, D.; Ayyagiri, A. Emerging vancomycin resistance in enterococci in India. Indian. J. Pathol. Microbiol. 2006, 49, 620–622. [Google Scholar]
- Gordon, S.; Swenson, J.; Hill, B.; Pigott, N.; Facklam, R.; Cooksey, R.; Thornsberry, C.; Jarvis, W.; Tenover, F. Antimicrobial susceptibility patterns of common and unusual species of enterococci causing infections in the United States. J. Clin. Microbiol. 1992, 30, 2373–2378. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, D.M.P.; Forde, B.M.; Kidd, T.J.; Harris, P.N.A.; Schembri, M.A.; Beatson, S.A.; Paterson, D.L.; Walker, M.J. Antimicrobial Resistance in ESKAPE Pathogens. Clin. Microbiol. Rev. 2020, 33, e00181-19. [Google Scholar] [CrossRef]
- Patel, T.; Lewis, M.E.; Niesley, M.L.; Chowdhury, M. Postneurosurgical Central Nervous System Infection Due to Enterococcus faecalis Successfully Treated With Intraventricular Vancomycin. Infect. Dis. Clin. Pract. 2016, 24, 174–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sievert, D.M.; Ricks, P.; Edwards, J.R.; Schneider, A.; Patel, J.; Srinivasan, A.; Kallen, A.; Limbago, B.; Fridkin, S.; National Healthcare Safety Network (NHSN) Team and Participating NHSN Facilities. Antimicrobial-resistant pathogens associated with healthcare-associated infections: Summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect. Control Hosp. Epidemiol. 2013, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Yuen, G.J.; Ausubel, F.M. Enterococcus infection biology: Lessons from invertebrate host models. J. Microbiol. 2014, 52, 200–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levitus, M.; Perera, T.B. Vancomycin-Resistant Enterococci (VRE). In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2019. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513233/ (accessed on 21 July 2020).
- Monticelli, J.; Knezevich, A.; Luzzati, R.; Di Bella, S. Clinical management of non-faecium non-faecalis vancomycin-resistant enterococci infection. Focus on Enterococcus gallinarum and Enterococcus casseliflavus/flavescens. J. Infect. Chemother. 2018, 24, 237–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protonotariou, E.; Dimitroulia, E.; Pournaras, S.; Pitiriga, V.; Sofianou, D.; Tsakris, A. Trends in antimicrobial resistance of clinical isolates of Enterococcus faecalis and Enterococcus faecium in Greece between 2002 and 2007. J. Hosp. Infect. 2010, 75, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.X.; Li, T.; Ning, Y.Z.; Shao, D.H.; Liu, J.; Wang, S.Q.; Liang, G.W. Molecular characterization of resistance, virulence and clonality in vancomycin-resistant Enterococcus faecium and Enterococcus faecalis: A hospital-based study in Beijing, China. Infect. Genet. Evol. 2015, 33, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Alevizakos, M.; Gaitanidis, A.; Nasioudis, D.; Tori, K.; Flokas, M.E.; Mylonakis, E. Colonization With Vancomycin–Resistant Enterococci and Risk for Bloodstream Infection Among Patients With Malignancy: A Systematic Review and Meta–Analysis. Open Forum Infect. Dis. 2017, 4, ofw246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melese, A.; Genet, C.; Andualem, T. Prevalence of Vancomycin resistant enterococci (VRE) in Ethiopia: A systematic review and meta–analysis. BMC Infect. Dis. 2020, 20, 124. [Google Scholar] [CrossRef] [Green Version]
- Barbosa-Ribeiro, M.; De Jesus-Soares, A.; Zaia, A.A.; Ferraz, C.C.; Almeida, J.F.; Gomes, B.P. Antimicrobial susceptibility and characterization of virulence genes of Enterococcus faecalis isolates from teeth with failure of the endodontic treatment. J. Endod. 2016, 42, 1022–1028. [Google Scholar] [CrossRef]
- Comerlato, C.B.; Resende, M.C.; Caierão, J.; d’Azevedo, P.A. Presence of virulence factors in Enterococcus faecalis and Enterococcus faecium susceptible and resistant to vancomycin. Mem. Inst. Oswaldo Cruz 2013, 108, 590–595. [Google Scholar] [CrossRef] [Green Version]
- Strateva, T.; Atanasova, D.; Savov, E.; Petrova, G.; Mitov, I. Incidence of virulence determinants in clinical Enterococcus faecalis and Enterococcus faecium isolates collected in Bulgaria. Braz. J. Infect. Dis. 2016, 20, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, D.M.; Talavera, G.N.; Hernandez, L.A.; Weisberg, S.B.; Ambrose, R.F.; Jay, J.A. Virulence genes among Enterococcus faecalis and Enterococcus faecium isolated from coastal beaches and human and nonhuman sources in Southern California and Puerto Rico. J. Pathog. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lata, P.; Ram, S.; Shanker, R. Multiplex PCR based genotypic characterization of pathogenic vancomycin resistant Enterococcus faecalis recovered from an Indian river along a city landscape. Springer Plus 2016, 5, 1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varela, A.R.; Ferro, G.; Vredenburg, J.; Yanık, M.; Vieira, L.; Rizzo, L.; Lameiras, C.; Manaia, C.M. Vancomycin resistant enterococci: From the hospital effluent to the urban wastewater treatment plant. Sci. Total Environ. 2013, 450–451, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Bartley, P.B.; Schooneveldt, J.M.; Looke, D.F.M.; Morton, A.; Johnson, D.W.; Nimmo, G.R. The relationship of a clonal outbreak of Enterococcus faecium vanA to methicillin-resistant Staphylococcus aureus incidence in a Australian hospital. J. Hosp. Infect. 2001, 48, 43–54. [Google Scholar] [CrossRef]
- Talebi, M.; Sadeghi, J.; Rahimi, F.; Pourshafie, M.R. Isolation and Biochemical Fingerprinting of Vancomycin–Resistant Enterococcus faecium From Meat, Chicken and Cheese. Jundishapur J. Microbiol. 2015, 8, e15815. [Google Scholar] [CrossRef] [Green Version]
- Torres, C.; Alonso, C.A.; Ruiz-Ripa, L.; León-Sampedro, R.; Del Campo, R.; Coque, T.M. Antimicrobial resistance in Enterococcus spp. of animal origin. Microbiol. Spectr. 2018, 6, ARBA-0032-2018. [Google Scholar] [CrossRef]
- Nishiyama, M.; Iguchi, A.; Suzuki, Y. Identification of Enterococcus faecium and Enterococcus faecalis as vanC–type vancomycin–resistant enterococci (VRE) from sewage and river water in the provincial city of Miyazaki, Japan. J. Environ. Sci. Health 2015, 50, 16–25. [Google Scholar] [CrossRef]
- Korzeniewska, E.; Korzeniewska, A.; Harnisz, M. Antibiotic resistant Escherichia coli in hospital and municipal sewage and their emission to the environment. Ecotoxicol. Environ. Saf. 2013, 91, 96–102. [Google Scholar] [CrossRef]
- Polish Standard PN–EN ISO 7899–2:2004. Water Quality—Detection and Enumeration of Intestinal Enterococci—Part 2: Membrane Filtration Method; PKN Warsaw: Płock, Poland, 2004. [Google Scholar]
- Facklam, R.R.; Collins, M.D. Identification of enterococcus species isolated from human infections by a conventional test scheme. J. Clin. Microbiol. 1989, 27, 731–734. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbart, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint Tables for Interpretation of MICs and Zone Diameters. 2012. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Disk_test_documents/EUCAST_breakpoints_v_2.0_120101.pdf (accessed on 20 May 2020).
- CLSI, Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Disk Susceptibility Tests, Approved Standard, 11th ed.; CLSI document M02-A11; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2012. [Google Scholar]
- Council of the European Communities. Council Directive 91/271/ECC of Concerning Urban Waste Water Treatment. Off. J. Eur. Communities 1991, 40–52. [Google Scholar]
- Giebułtowicz, J.; Tyski, S.; Wolinowska, R.; Grzybowska, W.; Zaręba, T.; Drobniewska, A.; Wroczyński, P.; Nałęcz-Jawecki, G. Occurrence of antimicrobial agents, drug–resistant bacteria, and genes in the sewage–impacted Vistula River (Poland). Environ. Sci. Pollut. Res. 2018, 25, 5788–5807. [Google Scholar] [CrossRef] [PubMed]
- Korzeniewska, E.; Harnisz, M. Relationship between modification of activated sludge wastewater treatment and changes in antibiotic resistance of bacteria. Sci. Total Environ. 2018, 639, 304–315. [Google Scholar] [CrossRef]
- Osińska, A.; Korzeniewska, E.; Harnisz, M.; Felis, E.; Bajkacz, S.; Jachimowicz, P.; Niestępski, S.; Konopka, I. Small–scale wastewater treatment plants as a source of the dissemination of antibiotic resistance genes in the aquatic environment. J. Hazard. Mater. 2020, 381, 121221. [Google Scholar] [CrossRef]
- Lipp, E.K.; Farrah, S.A.; Rose, J.B. Assessment and impact of microbial fecal pollution and human enteric pathogens in a coastal community. Mar. Pollut. Bull. 2001, 42, 286–293. [Google Scholar] [CrossRef]
- Hörman, A.; Rimhanen-Finne, R.; Maunula, L.; von Bonsdorff, C.-H.; Torvela, N.; Heikinheimo, A.; Hanninen, M.L. Campylobacter spp., Giardia spp., Cryptosporidium spp., Noroviruses, and indicator organisms in surface water in southwestern Finland, 2000–2001. Appl. Environ. Microbiol. 2004, 70, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Fries, J.S.; Characklis, G.W.; Noble, R.T. Sediment–water exchange of Vibrio sp. and fecal indicator bacteria: Implications for persistence and transport in the Neuse River Estuary, North Carolina. USA. Water Res. 2008, 42, 941–950. [Google Scholar] [CrossRef]
- Wilkes, G.; Edge, T.; Gannon, V.; Jokinen, C.; Lyautey, E.; Medeiros, D.; Neumann, N.; Ruecker, N.; Topp, E.; Lapen, D.R. Seasonal relationships among indicator bacteria, pathogenic bacteria, Cryptosporidium oocysts, Giardia cysts, and hydrological indices for surface waters within an agricultural landscape. Water Res. 2009, 43, 2209–2223. [Google Scholar] [CrossRef]
- Rodrigues, V.; Ramaiah, N.; Kakti, S.; Samant, D. Long–term variations in abundance and distribution of sewage pollution indicator and human pathogenic bacteria along the central west coast of India. Ecol. Indic. 2011, 11, 318–327. [Google Scholar] [CrossRef]
- Giebułtowicz, J.; Nałęcz-Jawecki, G.; Harnisz, M.; Kucharski, D.; Korzeniewska, E.; Płaza, G. Environmental Risk and Risk of Resistance Selection Due to Antimicrobials’ Occurrence in Two Polish Wastewater Treatment Plants and Receiving Surface Water. Molecules 2020, 25, 1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanthier, M.; Scott, A.; Zhang, Y.; Cloutier, M.; Durie, D.; Henderson, V.C.; Wilkes, G.; Lapen, D.R.; Topp, E. Distribution of selected virulence genes and antibiotic resistance in Enterococcus species isolated from the South Nation River drainage basin; Ontario; Canada. J. Appl. Microbiol. 2011, 110, 407–421. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, R.; Oberlé, K.; Galopin, S.; Cattoir, V.; Budzinski, H.; Petit, F. Changes in enterococcal populations and related antibiotic resistance along a medical center–wastewater treatment plant–river continuum. Appl. Environ. Microbiol. 2013, 79, 2428–2434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kühn, I.; Iversen, A.; Burman, L.G.; Olsson-Liljequist, B.; Franklin, A.; Finn, M.; Aarestrup, F.; Seyfarth, A.M.; Blanch, A.R.; Vilanova, X.; et al. Comparison of enterococcal populations in animals; humans; and the environment—A European study. Int. J. Food Microbiol. 2003, 88, 133–145. [Google Scholar] [CrossRef]
- Lebreton, F.; Willems, R.J.L.; Gilmore, M.S. Enterococcus Diversity, Origins in Nature, and Gut Colonization. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Gilmore, M.S., Clewell, D.B., Ike, Y., Shankar, N., Eds.; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014; pp. 5–64. [Google Scholar]
- Layton, B.A.; Walters, S.P.; Lam, L.H.; Boehm, A.B. Enterococcus species distribution among human and animal hosts using multiplex PCR. J. Appl. Microbiol. 2010, 109, 539–547. [Google Scholar] [CrossRef]
- Bonilla, T.D.; Nowosielski, K.; Esiobu, N.; McCorquodale, D.S.; Rogerson, A. Species assemblages of Enterococcus indicate potential sources of fecal bacteria at a south Florida recreational beach. Mar. Pollut. Bull. 2006, 52, 807–810. [Google Scholar] [CrossRef]
- Da Silva, M.F.; Tiago, I.; Veríssimo, A.; Boaventura, R.A.R.; Nunes, O.C.; Manaia, C.M. Antimicrobial resistance patterns in Enterobacteriaceae isolated from an urban wastewater treatment plant. FEMS Microbiol. Ecol. 2007, 60, 166–176. [Google Scholar] [CrossRef]
- Iweriebor, B.C.; Gaqavu, S.; Obi, L.C.; Nwodo, U.U.; Okoh, A.I. Antibiotic susceptibilities of enterococcus species isolated from hospital and domestic wastewater effluents in alice, eastern cape province of South Africa. Int. J. Environ. Res. Public Health 2015, 12, 4231–4246. [Google Scholar] [CrossRef]
- Gotkowska-Płachta, A.; Filipkowska, Z.; Korzeniewska, Z.; Janczukowicz, W.; Dixon, B.; Gołaś, I.; Szwalgin, D. Airborne microorganisms emitted from wastewater treatment plant treating domestic wastewater and meat processing industry wastes. Clean Soil Air Water 2013, 41, 429–436. [Google Scholar] [CrossRef]
- Aarestrup, F.M.; Butaye, P.; Witte, W. Nonhuman reservoirs of enterococci. In The Enterococci: Pathogenesis. Molecular Biology and Antibiotic Resistance; Gilmore, M.S., Clewell, D.B., Courvalin, P., Dunny, G.M., Murray, B.E., Rice, L.B., Eds.; ASM Press: Washington, DC, USA, 2002; pp. 55–99. [Google Scholar]
- Osińska, A.; Korzeniewska, E.; Harnisz, M.; Niestępski, S. The prevalence and characterization of antibiotic–resistant and virulent Escherichia coli strains in the municipal wastewater system and their environmental fate. Sci. Total Environ. 2017, 577, 367–375. [Google Scholar]
- Rosenberg Goldstein, R.E.; Micallef, S.A.; Gibbs, S.G.; George, A.; Claye, E.; Sapkota, A.; Joseph, S.W.; Sapkota, A.R. Detection of vancomycin–resistant enterococci (VRE) at four U.S. wastewater treatment plants that provide effluent for reuse. Sci. Total Environ. 2014, 1, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Kotzamanidis, C.; Zdragas, A.; Kourelis, A.; Moraitou, E.; Papa, A.; Yiantzi, V.; Pantelidou, C.; Yiangou, M. Characterization of vanA–type Enterococcus faecium isolates from urban and hospital wastewater and pigs. J. Appl. Microbiol. 2009, 107, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.; Galvin, S.; Boyle, F.; Hickey, P.; Mulligan, M.; Cormican, M. Enterococcus faecium of the vanA genotype in rural drinking water, effluent, and the aqueous environment. Appl. Environ. Microbiol. 2012, 78, 596–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moura, T.M.; Cassenego, A.P.V.; Campos, F.S.; Ribeiro, A.M.L.; Franco, A.C.; d’Azevedo, P.A.; Frazzon, J.; Frazzon, A.P.G. Detection of vanC1 gene transcription in vancomycin–susceptible Enterococcus faecalis. Mem. Inst. Oswaldo Cruz 2013, 108, 453–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toner, L.; Papa, N.; Aliyu, S.H.; Dev, H.; Lawrentschuk, N.; Al-Hayek, S. Vancomycin resistant enterococci in urine cultures: Antibiotic susceptibility trends over a decade at a tertiary hospital in the United Kingdom. Investig. Clin. Urol. 2016, 57, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Hancock, L.E.; Murray, B.E.; Sillanpää, J. Enterococcal Cell Wall Components and Structures. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Massachusetts Eye and Ear Infirmary: Boston, MA, USA, 2014; pp. 503–546. [Google Scholar]
- Kayaoglu, G.; Orstavik, D. Virulence factors of Enterococcus faecalis: Relationship to endodontic disease. Crit. Rev. Oral Biol. Med. 2004, 15, 308–320. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, A.S.; Omar, N.B.; Abriouel, H.; López, R.L.; Ortega, E.; Cañamero, M.M.; Gálvez, A. Risk factors in enterococci isolated from foods in Morocco: Determination of antimicrobial resistance and incidence of virulence traits. Food Chem. Toxicol. 2008, 46, 2648–2652. [Google Scholar] [CrossRef]
- Shokoohizadeh, L.; Ekrami, A.; Labibzadeh, M.; Ali, L.; Alavi, S.M. Antimicrobial resistance patterns and virulence factors of enterococci isolates in hospitalized burn patients. BMC Res. Notes 2018, 11, 1. [Google Scholar] [CrossRef]
- Creti, R.; Imperi, M.; Bertuccini, L.; Fabretti, F.; Orefici, G.; Di Rosa, R.; Baldassarri, L. Survey for virulence determinants among Enterococcus faecalis isolated from different sources. J. Med. Microbiol. 2004, 53, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Biswas, P.P.; Dey, S.; Sen, A.; Adhikari, L. Molecular Characterization of Virulence Genes in Vancomycin–Resistant and Vancomycin–Sensitive Enterococci. J. Glob. Infect. Dis. 2016, 8, 16–24. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sampling Sites | Parameters | |
|---|---|---|
| pH | Temperature (°C) | |
| HWW | 8.35 ± 0.62 a | 14.37 ± 6.96 |
| (7.60−9.20) b | (7.58−25.89) | |
| UWW | 8.39 ± 0.42 | 14.74 ± 6.60 |
| (8.02−9.22) | (7.58−25.85) | |
| TWW | 8.40 ± 0.35 | 15.55 ± 8.67 |
| (8.02−9.01) | (7.47−26.80) | |
| URW | 7.16 ± 0.41 | 11.76 ± 4.87 |
| (6.40−7.50) | (0.0−21.10) | |
| DRW | 7.21 ± 0.65 | 14.31 ± 6.0 |
| (6.50−8.40) | (9.30−24.70) | |
| p value c | 0.0011 * | 0.8452 |
| Sewage | River | ||||
|---|---|---|---|---|---|
| Species | HWW | UWW | TWW | URW | DRW |
| Strains: number (%) | |||||
| MDR (%) | |||||
| XDR (%) | |||||
| E. faecium | 36 (42.9) | 28 (41.2) | 38 (38.8) | 0 | 4 (25.0) |
| 34 (94.4) | 27 (96.4) | 33 (86.8) | 0 | 4 (100) | |
| 2 (5.6) | 1 (3.57) | 1 (2.6) | 0 | 0 | |
| E. faecalis | 26 (31.0) | 20 (29.4) | 29 (29.6) | 5 (29.4) | 1 (6.3) |
| 23 (88.5) | 19 (95.0) | 28 (96.6) | 3 (60) | 1 (100) | |
| 1(3.8) | 0 | 0 | 0 | 0 | |
| E. durans | 1 (1.2) | 0 | 3 (3.1) | 0 | 0 |
| 1 (100) | 0 | 3 (100) | 0 | 0 | |
| E. avium | 7 (8.3) | 4 (5.9) | 2 (2.0) | 0 | 0 |
| 7 (100) | 4 (100) | 2 100) | 0 | 0 | |
| E. hirae | 2 (2.4) | 1 (1.5) | 4 (4.1) | 0 | 0 |
| 2 (100) | 1 (100) | 4 (100) | 0 | 0 | |
| E. gallinarum | 1 (1.2) | 3 (4.4) | 1 (1.0) | 0 | 5 (31.3) |
| 1 (100) | 3 (100) | 1 (100) | 0 | 4 (80) | |
| E. casseliflavus/ | 1 (1.2) | 0 | 0 | 0 | 0 |
| flawescens | 1 (100) | 0 | 0 | 0 | 0 |
| Other | 10 (11.9) | 12 (17.6) | 21 (21.4) | 12 (70.6) | 6 (37.5) |
| Enterococcus spp. | 10 (100) | 13 (100) | 20 (95.2) | 5 (41.6) | 6 (100) |
| 1 (10.0) | 0 | 0 | 0 | 0 | |
| Number of strains | 84 | 68 | 98 | 17 | 16 |
| MDR (%) | 79 (94.0) | 67 (98.5) | 91 (92.9) | 8 (47.0) | 15 (93.8) |
| XDR (%) | 4 (4.8) | 1(1.5) | 1(1.0) | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gotkowska-Płachta, A. The Prevalence of Virulent and Multidrug-Resistant Enterococci in River Water and in Treated and Untreated Municipal and Hospital Wastewater. Int. J. Environ. Res. Public Health 2021, 18, 563. https://doi.org/10.3390/ijerph18020563
Gotkowska-Płachta A. The Prevalence of Virulent and Multidrug-Resistant Enterococci in River Water and in Treated and Untreated Municipal and Hospital Wastewater. International Journal of Environmental Research and Public Health. 2021; 18(2):563. https://doi.org/10.3390/ijerph18020563
Chicago/Turabian StyleGotkowska-Płachta, Anna. 2021. "The Prevalence of Virulent and Multidrug-Resistant Enterococci in River Water and in Treated and Untreated Municipal and Hospital Wastewater" International Journal of Environmental Research and Public Health 18, no. 2: 563. https://doi.org/10.3390/ijerph18020563
APA StyleGotkowska-Płachta, A. (2021). The Prevalence of Virulent and Multidrug-Resistant Enterococci in River Water and in Treated and Untreated Municipal and Hospital Wastewater. International Journal of Environmental Research and Public Health, 18(2), 563. https://doi.org/10.3390/ijerph18020563