Burnout and Depression in Portuguese Healthcare Workers during the COVID-19 Pandemic—The Mediating Role of Psychological Resilience





Abstract
:1. Introduction
Psychological Resilience as a Factor for Protecting from Burnout and Depression
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey Questionnaire
2.3. Statistical Analysis
3. Results
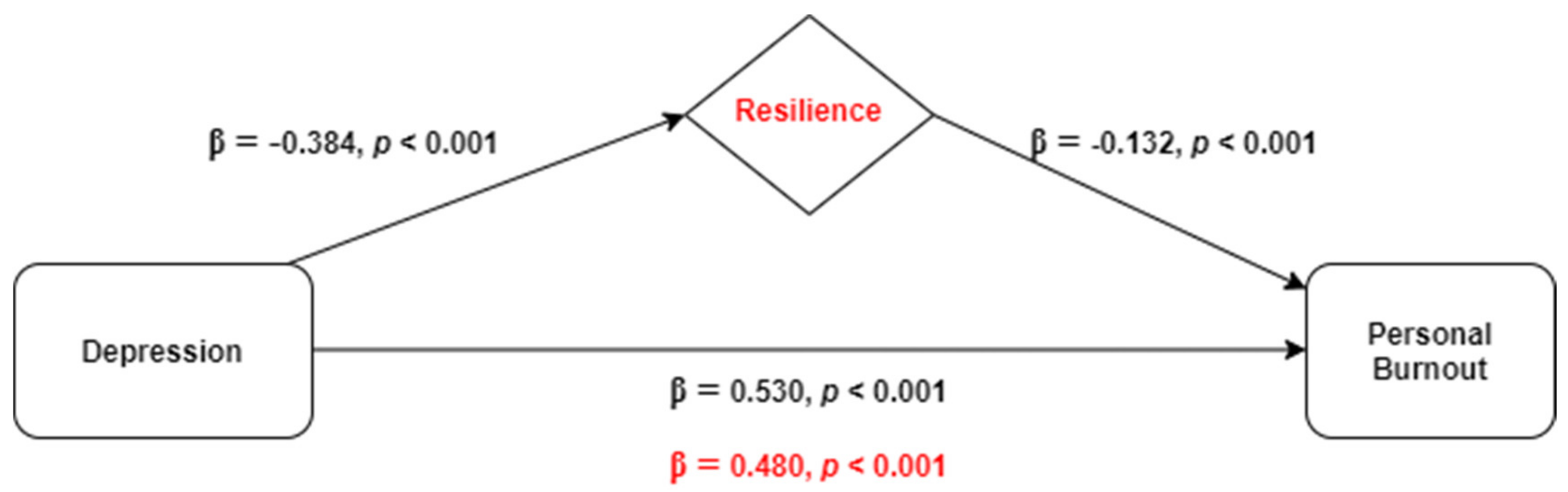
3.1. The Mediating Role of Resilience in the Relationship between Depression and Personal Burnout
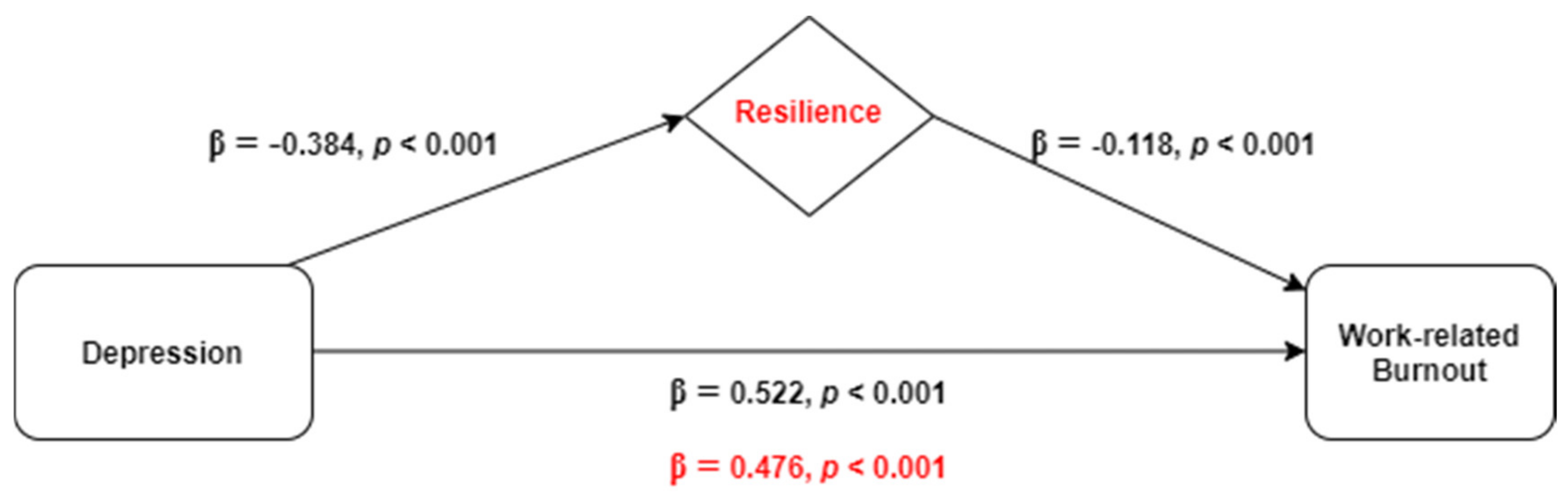
3.2. The Mediating Role of Resilience in the Relationship between Depression and Work-Related Burnout
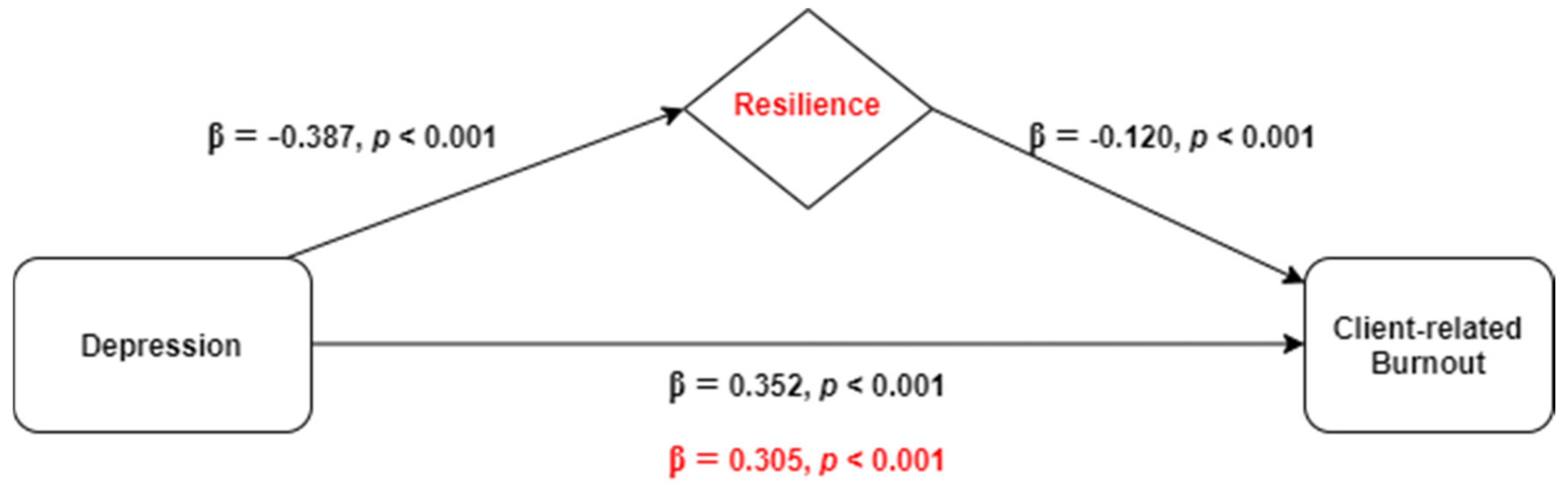
3.3. The Mediating Role of Resilience in the Relationship between Depression and Client-Related Burnout
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centre Disease Prevention and Control (ECDC). Communicable Disease Threats Report. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Communicable-disease-threatsreport-13-june-2020.pdf (accessed on 27 November 2020).
- Albott, C.S.; Wozniak, J.R.; McGlinch, B.P.; Wall, M.H.; Gold, B.S.; Vinogradov, S. Battle Buddies: Rapid Deployment of a Psychological Resilience Intervention for Health Care Workers During the COVID-19 Pandemic. Anesth. Analg. 2020, 131, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Walton, M.; Murray, E.; Christian, M.D. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Marôco, J.; Maroco, A.L.; Leite, E.; Bastos, C.; Vazão, M.J.; Campos, J. Burnout em profissionais da saúde portugueses: Uma análise a nível nacional. Acta Med. Port. 2016, 29, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Reis, C. Prevalência de Síndrome de Burnout em Médicos de Família da Secção Regional do Norte da Ordem dos Médicos. Rev. Port. Med. Geral. Fam. 2019, 35, 176–184. [Google Scholar] [CrossRef]
- WHO. Burn-Out an “Occupational Phenomenon”: International Classification of Diseases. Available online: https://www.who.int/mental_health/evidence/burn-out/en/ (accessed on 1 August 2020).
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Greenglass, E.R. Introduction to special issue on burnout and health. Psychol. Health 2001, 16, 501–510. [Google Scholar] [CrossRef]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Drapeau, A.; Marchand, A.; Beaulieu-Prévost, D. Epidemiology of Psychological Distress. In Mental Illnesses—Understanding, Prediction and Control; L’Abate, L., Ed.; Intech Open: London, UK, 2012; pp. 105–133. Available online: https://www.intechopen.com/books/mental-illnesses-understanding-prediction-and-control/epidemiology-of-psychological-distress (accessed on 21 November 2020).
- Gasparro, R.; Scandurra, C.; Maldonato, N.M.; Dolce, P.; Bochicchio, V.; Valletta, A.; Sammartino, G.; Sammartino, P.; Mariniello, M.; di Lauro, A.E.; et al. Perceived Job Insecurity and Depressive Symptoms among Italian Dentists: The Moderating Role of Fear of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5338. [Google Scholar] [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of Posttraumatic Stress, Anxiety, Depression, Levels of Resilience and Burnout in Spanish Health Personnel during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef]
- Wankowicz, P.; Szylińska, A.; Rotter, I. Assessment of mental health factors among health professionals depending on their contact with COVID-19 patients. Int. J. Environ. Res. Public Health 2020, 17, 5849. [Google Scholar] [CrossRef] [PubMed]
- Weilenmann, S.; Ernst, J.; Petry, H.; Sazpinar, O.; Pfaltz, M.C.; Gehrke, M.; Paolercio, F.; Kaenel, R.; Spiller, T.R. Health care workers mental health during the first weeks of the SARS-CoV-2 Pandemic in Switzerland: A cross-sectional Study. medRxiv 2020. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanafelt, T.D.; Bradley, K.A.; Wipf, J.E.; Back, A.L. Burnout and self-reported patient care in an internal medicine residency program. Ann. Intern. Med. 2002, 136, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Gemignani, A.; Conversano, C. Psychological resources against the traumatic experience of COVID-19. Clin. Neuropsychiatry 2020, 17, 85–87. [Google Scholar] [CrossRef]
- Cooke, G.P.; Doust, J.A.; Steele, M.C. A survey of resilience, burnout, and tolerance of uncertainty in Australian general practice registrars. BMC Med. Educ. 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Rushton, C.H.; Batcheller, J.; Schroeder, K.; Donohue, P. Burnout and Resilience Among Nurses Practicing in High-Intensity Settings. Am. J. Crit. Care 2015, 24, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Gao, T.; Ding, X.; Chai, J.; Zhang, Z.; Zhang, H.; Kong, Y.; Mei, S. The influence of resilience on mental health: The role of general well-being. Int. J. Nurs. Pract. 2017, 23, e12535. [Google Scholar] [CrossRef]
- McKinley, N.; McCain, R.S.; Convie, L.; Clarke, M.; Dempster, M.; Campbell, W.J.; Kirk, S.J. Resilience, burnout and coping mechanisms in UK doctors: A cross-sectional study. BMJ Open 2020, 10, e031765. [Google Scholar] [CrossRef] [Green Version]
- Keeton, K.; Fenner, D.E.; Johnson, T.R.; Hayward, R.A. Predictors of physician career satisfaction, work-life balance, and burnout. Obstet. Gynecol. 2007, 109, 949–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychological Association Building Your Resilience. Available online: https://www.apa.org/topics/resilience (accessed on 21 August 2020).
- Serrão, C.; Castro, L.; Teixeira, A.; Rodrigues, A.R.; Duarte, I. Resiliência em médicos: Contributos para a validação da versão portuguesa da Escala de Resiliência. Acta Med. Port. 2021, in press. [Google Scholar]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: Psychological, behavioral, and biological determinants. Annu. Rev. Clin. Psychol. 2005, 1, 607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luthans, F. The need for and meaning of positive organizational behavior. J. Organ. Behav. 2002, 23, 695–706. [Google Scholar] [CrossRef] [Green Version]
- Dunn, L.B.; Iglewicz, A.; Moutier, C. A conceptual model of medical student well-being: Promoting resilience and preventing burnout. Acad. Psychiatry 2008, 32, 44–53. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Sinsky, C.; Trockel, M.; Tutty, M.; Nedelec, L.; Carlasare, L.E.; Shanafelt, T.D. Resilience and Burnout Among Physicians and the General US Working Population. JAMA Netw. Open 2020, 3, e209385. [Google Scholar] [CrossRef]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Arrogante, O.; Aparicio-Zaldivar, E. Burnout and health among critical care professionals: The mediational role of resilience. Intensive Crit. Care Nurs. 2017, 42, 110–115. [Google Scholar] [CrossRef]
- Arrogante, Ó. Mediación de la resiliencia entre burnout y salud en el personal de Enfermería [Mediator effect of resilience between burnout and health in nursing staff]. Enferm. Clin. 2014, 24, 283–289. (In Spanish) [Google Scholar] [CrossRef]
- Treglown, L.; Palaiou, K.; Zarola, A.; Furnham, A. The Dark Side of Resilience and Burnout: A Moderation-Mediation Model. PLoS ONE 2016, 11, e0156279. [Google Scholar] [CrossRef]
- Papathanasiou, I.V. Work-related Mental Consequences: Implications of Burnout on Mental Health Status Among Health Care Providers. Acta Inform. Med. 2015, 23, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The Relationship Between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 10, 284. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Burnout–depression overlap: A review. Clin. Psychol. Rev. 2015, 36, 28–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joyce, S.; Shand, F.; Tighe, J.; Laurent, S.J.; Bryant, R.A.; Harvey, S.B. Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open 2018, 8, e017858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PORDATA. SNS: Recursos Humanos [NHS: Human Resources]. Available online: https://www.pordata.pt/Subtema/Portugal/Recursos+Humanos-36 (accessed on 27 November 2020).
- Oliveira, M.F.; Machado, T.S. Tradução e validação da Escala de Resiliência para Estudantes do Ensino Superior. Anál. Psicol. 2011, 29, 579–591. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Pais-Ribeiro, J.L.; Honrado, A.; Leal, I. Contribuição para o Estudo da Adaptação Portuguesa das Escalas de Ansiedade, Depressão e Stress (EADS) de 21 itens de Lovibond e Lovibond. Psicol. Saúde Doenças 2004, 5, 229–239. [Google Scholar]
- Fonte, C.M.S. Adaptação e Validação para Português do Questionário de Copenhagen Burnout Inventory (CBI). Master’s Thesis, Universidade de Coimbra, Coimbra, Portugal, 2011. Available online: https://estudogeral.sib.uc.pt/handle/10316/18118 (accessed on 2 October 2020).
- Tan, B.Y.Q.; Chew, N.W.S.; Lee, G.K.H.; Jing, M.; Goh, Y.; Yeo, L.L.L.; Ka, Z.; Chin, H.; Ahmas, A.; Khan, F.; et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Xiao, X.; Zhu, X.; Fu, S.; Hu, Y.; Li, X.; Xiao, J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: A multi-center cross-sectional survey investigation. J. Affect. Disord. 2020, 274, 405–410. [Google Scholar] [CrossRef]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. E Clin. Med. 2020, 24, 100424. [Google Scholar] [CrossRef]
- Khasne, R.W.; Dhakulkar, B.S.; Mahajan, H.C.; Kulkarni, A.P. Burnout among healthcare workers during COVID-19 pandemic in India: Results of a questionnaire-based Survey. Indian J. Crit. Care Med. 2020, 24, 664–671. [Google Scholar] [CrossRef]
- Lin, J.; Ren, Y.; Gan, H.; Chen, Y.; Huang, Y.; You, X. Factors influencing resilience of medical workers from other provinces to Wuhan fighting against 2019 Novel Coronavirus Pneumonia. BMC Psychiatry 2020. [Google Scholar] [CrossRef]
- Connor, K.M.; Zhang, W. Recent advances in the understanding and treatment of anxiety disorders. Resilience: Determinants, measurement, and treatment responsiveness. CNS Spectr. 2006, 11 (Suppl. 12), 5. [Google Scholar] [CrossRef] [PubMed]
- Hjemdal, O.; Vogel, P.A.; Solem, S.; Hagen, K.; Stiles, T.C. The relationship between resilience and levels of anxiety, depression, and obsessive-compulsive symptoms in adolescents. Clin. Psychol. Psychother. 2011, 18, 314. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Sex | |
| Female | 1678 (83.6) |
| Male | 330 (16.4) |
| Parents | |
| Yes | 975 (48.6) |
| No | 1033 (51.4) |
| Lives with a person at risk for COVID-19 infection | |
| Yes | 681 (33.9) |
| No | 1327 (66.1) |
| Death of relative or friend during the pandemic period | |
| Yes | 118 (5.9) |
| No | 1890 (94.1) |
| Professional experience | |
| Five years or less | 504 (25.1) |
| From 6 years to 15 years | 745 (37.1) |
| More than 15 years | 759 (37.8) |
| Frontline working position a | |
| Yes | 1398 (69.7) |
| No | 609 (30.3) |
| Direct contact with infected people | |
| Yes | 552 (27.5) |
| No | 1456 (72.5) |
| Salary reduction | |
| Yes | 710 (35.4) |
| No | 1298 (64.6) |
| Diagnosed health problem | |
| Yes | 524 (26.1) |
| No | 1484 (73.9) |
| COVID-19 Tested | |
| Yes | 504 (25.1) |
| No, but I’d like to do it | 983 (49.0) |
| No, I have no interest | 521 (25.9) |
| Mean (SD) | |
| Personal burnout | 49.3 (20.7) |
| Work-related burnout | 50.2 (19.3) |
| Client-related burnout | 38.9 (22.6) |
| Mdn (Q1; Q3) | |
| Resilience | 137 (123; 146) |
| Depression | 2 (1; 5) |
| Variables | Step 1 (β) | Step 2 (β) | Step 3 (β) |
|---|---|---|---|
| Sex | 0.382 ** | 0.291 ** | 0.283 ** |
| Marital status | |||
| Married/nonmarital partnership | Reference | ||
| Single | −0.018 | −0.104 * | −0.107 * |
| Divorced or separated | 0.012 | −0.046 | −0.057 |
| Widowed | −0.228 | −0.222 | −0.238 |
| Children ≤12y | 0.196 ** | 0.214 ** | 0.208 ** |
| Frontline working position | 0.243 ** | 0.252 ** | 0.242 ** |
| Diagnosed health problem | 0.303 ** | 0.161 ** | 0.156 ** |
| COVID-19 tested | |||
| Yes | Reference | ||
| No, but I’d like to do it | 0.031 | 0.013 | 0.015 |
| No, I have no interest | −0.216 ** | −0.168 ** | −0.169 ** |
| Direct contact with infected people | 0.274 ** | 0.205 ** | 0.202 ** |
| Depression | 0.530 ** | 0.480 ** | |
| Resilience | −0.132 ** | ||
| F | 21.2 ** | 105.6 ** | 103.0 ** |
| R2 | 0.096 | 0.368 | 0.383 |
| ΔR2 | 0.096 | 0.272 | 0.015 |
| Variables | Step 1 (β) | Step 2 (β) | Step 3 (β) |
|---|---|---|---|
| Sex | 0.198 ** | 0.117 * | 0.109 * |
| Children ≤ 12y | 0.096 | 0.130 ** | 0.125 ** |
| Educational level | |||
| High school and below | Reference | ||
| University degree | 0.305 * | 0.185 | 0.198 |
| Postgraduate | 0.473 * | 0.329 * | 0.346 * |
| Master’s | 0.391 ** | 0.313 ** | 0.327 ** |
| PhD | 0.284 | 0.192 | 0.234 |
| Professional experience | |||
| Five years or less | Reference | ||
| From 6 years to 15 years | 0.072 | 0.174 ** | 0.183 ** |
| More than 15 years | 0.004 | 0.100 | 0.103 * |
| Frontline working position | 0.177 ** | 0.185 ** | 0.176 ** |
| Diagnosed health problem | 0.296 ** | 0.154 ** | 0.149 ** |
| COVID-19 tested | |||
| Yes | Reference | ||
| No, but I’d like to do it | 0.036 | 0.015 | 0.017 |
| No, I have no interest | −0.128 * | −0.086 | −0.088 |
| Direct contact with infected people | 0.272 ** | 0.199 ** | 0.196 ** |
| Depression | 0.522 ** | 0.476 ** | |
| Resilience | −0.118 ** | ||
| F | 10.4 ** | 68.8 ** | 67.7 ** |
| R2 | 0.064 | 0.326 | 0.338 |
| ΔR2 | 0.064 | 0.263 | 0.012 |
| Variables | Step 1 (β) | Step 2 (β) | Step 3 (β) |
|---|---|---|---|
| Professional experience | |||
| Five years or less | Reference | ||
| From 6 years to 15 years | 0.114 * | 0.187 ** | 0.194 ** |
| More than 15 years | −0.081 | −0.026 | −0.026 |
| Direct contact with infected people | 0.153 ** | 0.111 * | 0.106 * |
| Death of relative or friend during the pandemic period | −0.163 | −0.189 * | −0.175 * |
| Depression | 0.352 ** | 0.305 ** | |
| Resilience | −0.120 ** | ||
| F | 7.1 ** | 63.3 ** | 58.2 ** |
| R2 | 0.014 | 0.137 | 0.149 |
| ΔR2 | 0.014 | 0.122 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrão, C.; Duarte, I.; Castro, L.; Teixeira, A. Burnout and Depression in Portuguese Healthcare Workers during the COVID-19 Pandemic—The Mediating Role of Psychological Resilience. Int. J. Environ. Res. Public Health 2021, 18, 636. https://doi.org/10.3390/ijerph18020636
Serrão C, Duarte I, Castro L, Teixeira A. Burnout and Depression in Portuguese Healthcare Workers during the COVID-19 Pandemic—The Mediating Role of Psychological Resilience. International Journal of Environmental Research and Public Health. 2021; 18(2):636. https://doi.org/10.3390/ijerph18020636
Chicago/Turabian StyleSerrão, Carla, Ivone Duarte, Luísa Castro, and Andreia Teixeira. 2021. "Burnout and Depression in Portuguese Healthcare Workers during the COVID-19 Pandemic—The Mediating Role of Psychological Resilience" International Journal of Environmental Research and Public Health 18, no. 2: 636. https://doi.org/10.3390/ijerph18020636
APA StyleSerrão, C., Duarte, I., Castro, L., & Teixeira, A. (2021). Burnout and Depression in Portuguese Healthcare Workers during the COVID-19 Pandemic—The Mediating Role of Psychological Resilience. International Journal of Environmental Research and Public Health, 18(2), 636. https://doi.org/10.3390/ijerph18020636