Evolution of Malaria Incidence in Five Health Districts, in the Context of the Scaling up of Seasonal Malaria Chemoprevention, 2016 to 2018, in Mali




 , ,
, ,
Abstract
:1. Introduction
2. Method
2.1. Study Location and Population
2.2. Data and Sources
2.3. Data Analysis
2.4. Software and Packages
3. Results
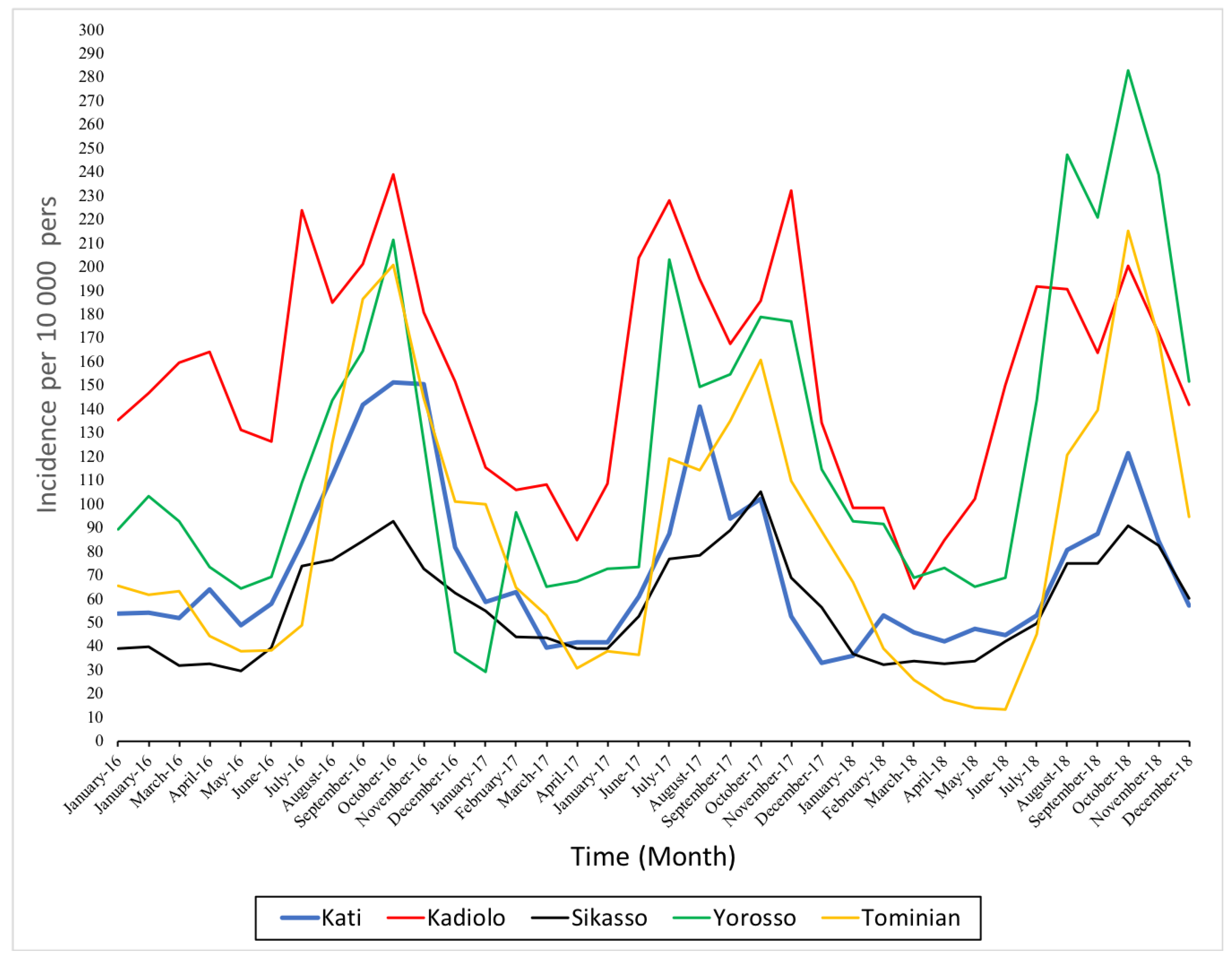
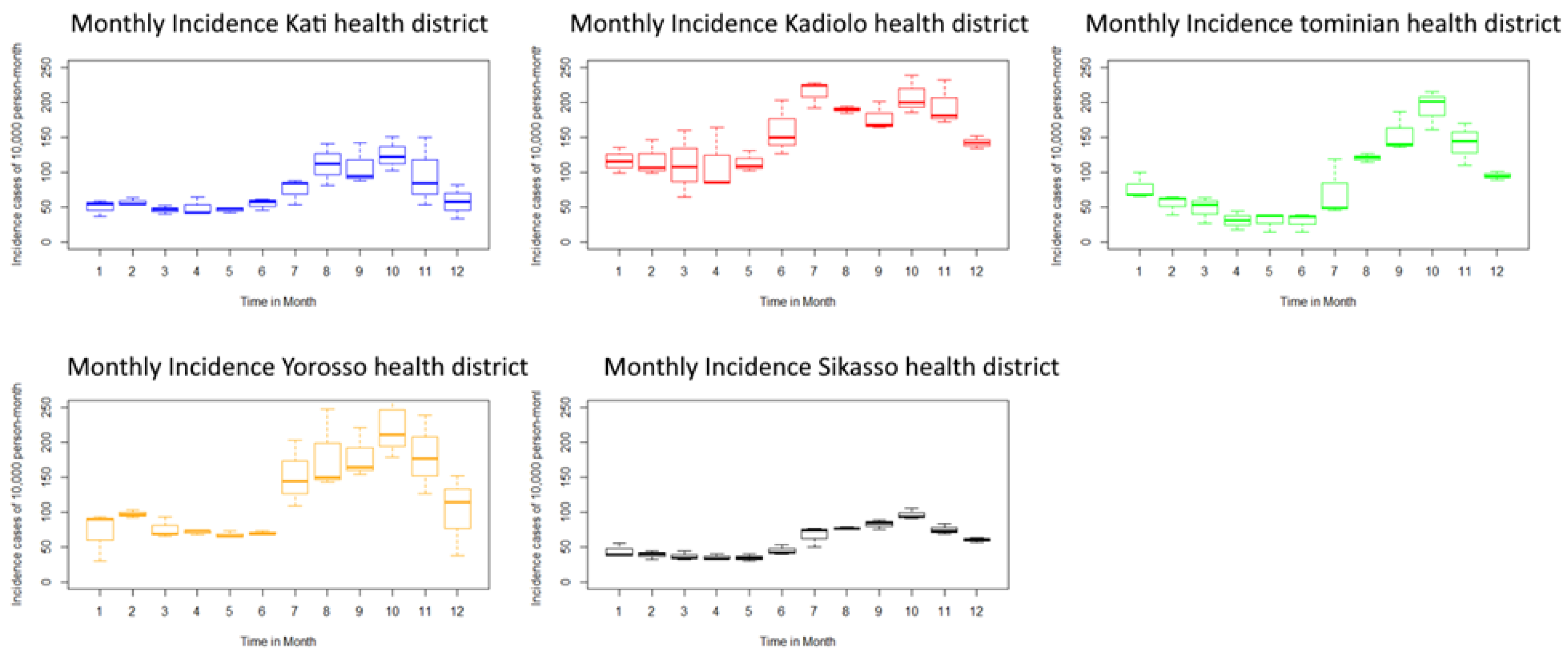
3.1. Evolution of Malaria Incidence in the Five Health Districts
3.2. Estimated Monthly Incidence in Under-Fives and Five or Over Five Years Olds and SMC
3.3. Analysis of the Meteorological Variables into the Five Health Districts
3.3.1. Univariate Analysis of Overall Meteorological Variables between the Health Districts
3.3.2. Miltivariiate Analysis of Overall Malaria Incidence and Meteorological Variables
4. Discussion
The Comparison between Meteorological Variables in the Health Districts
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO: World Health Organization. World Malaria Report; WHO: Geneva, Switzerland, 2018; p. 210. [Google Scholar]
- DGSHP. Mali Annuaire Statistique Du Système Local Information Saniatire 2018 (SLIS); DGSHP: Bamako, Mali, 2018. [Google Scholar]
- WHO. Global Technical Strategy for Malaria 2016–2030; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- AOOS P/MTN—Paludisme et Maladies Tropicales Négligées(MTN) Au Sahel|Organisation Ouest Africaine de La Santé. Available online: https://www.wahooas.org/web-ooas/fr/projets/pmtn-paludisme-et-maladies-tropicales-negligeesmtn-au-sahel (accessed on 29 October 2020).
- World Health Organization. Chimioprévention du Paludisme Saisonnier par L’administration de la Sulfadoxine Pyrimethamine et L’amodiaqune: Guide de Terrain; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Wagman, J.; Gogue, C.; Tynuv, K.; Mihigo, J.; Bankineza, E.; Bah, M.; Diallo, D.; Saibu, A.; Richardson, J.H.; Kone, D.; et al. An Observational Analysis of the Impact of Indoor Residual Spraying with Non-Pyrethroid Insecticides on the Incidence of Malaria in Ségou Region, Mali: 2012–2015. Malar. J. 2018, 17, 19. [Google Scholar] [CrossRef] [Green Version]
- Wragge, S.-E.; Toure, D.; Coetzee, M.; Gilbert, A.; Christian, R.; Segoea, G.; Hunt, R.H.; Coetzee, M. Malaria Control at a Gold Mine in Sadiola District, Mali, and Impact on Transmission over 10 Years. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 755–762. [Google Scholar] [CrossRef]
- WHO. Malaria Consortium—Seasonal Malaria Chemoprevention. 2020. Available online: https://www.malariaconsortium.org/pages/preventive_treatments/seasonal-malaria-chemoprevention.htm (accessed on 29 October 2020).
- Guo-Ding, Z.; Jun, C. Progress and challenges of global malaria elimination. Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi 2019, 31, 19–22. [Google Scholar] [CrossRef]
- Attaher, O.; Zaidi, I.; Kwan, J.L.; Issiaka, D.; Samassekou, M.B.; Cisse, K.B.; Coulibaly, B.; Keita, S.; Sissoko, S.; Traore, T.; et al. Effect of Seasonal Malaria Chemoprevention on Immune Markers of Exhaustion and Regulation. J. Infect. Dis. 2020, 221, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Cissé, B.; Ba, E.H.; Sokhna, C.; NDiaye, J.L.; Gomis, J.F.; Dial, Y.; Pitt, C.; NDiaye, M.; Cairns, M.; Faye, E.; et al. Effectiveness of Seasonal Malaria Chemoprevention in Children under Ten Years of Age in Senegal: A Stepped-Wedge Cluster-Randomised Trial. PLoS Med. 2016, 13, e1002175. [Google Scholar] [CrossRef] [Green Version]
- Diawara, F.; Steinhardt, L.C.; Mahamar, A.; Traore, T.; Kone, D.T.; Diawara, H.; Kamate, B.; Kone, D.; Diallo, M.; Sadou, A.; et al. Measuring the Impact of Seasonal Malaria Chemoprevention as Part of Routine Malaria Control in Kita, Mali. Malar. J. 2017, 16, 325. [Google Scholar] [CrossRef]
- Druetz, T. Evaluation of Direct and Indirect Effects of Seasonal Malaria Chemoprevention in Mali. Sci. Rep. 2018, 8, 8104. [Google Scholar] [CrossRef] [Green Version]
- Konaté, D.; Diawara, S.I.; Touré, M.; Diakité, S.A.S.; Guindo, A.; Traoré, K.; Diarra, A.; Keita, B.; Thiam, S.; Keita, M.; et al. Effect of Routine Seasonal Malaria Chemoprevention on Malaria Trends in Children under 5 Years in Dangassa, Mali. Malar. J. 2020, 19, 137. [Google Scholar] [CrossRef]
- Cairns, M.E.; Sagara, I.; Zongo, I.; Kuepfer, I.; Thera, I.; Nikiema, F.; Diarra, M.; Yerbanga, S.R.; Barry, A.; Tapily, A.; et al. Evaluation of Seasonal Malaria Chemoprevention in Two Areas of Intense Seasonal Malaria Transmission: Secondary Analysis of a Household-Randomised, Placebo-Controlled Trial in Houndé District, Burkina Faso and Bougouni District, Mali. PLoS Med. 2020, 17, e1003214. [Google Scholar] [CrossRef]
- Mahamar, A.; Issiaka, D.; Barry, A.; Attaher, O.; Dembele, A.B.; Traore, T.; Sissoko, A.; Keita, S.; Diarra, B.S.; Narum, D.L.; et al. Effect of Seasonal Malaria Chemoprevention on the Acquisition of Antibodies to Plasmodium Falciparum Antigens in Ouelessebougou, Mali. Malar. J. 2017, 16, 289. [Google Scholar] [CrossRef]
- CPS/SSDSPF; Institut National de la Statistique (INSTAT); Centre d’Études et d’Information Statistiques (INFO-STAT). Bamako, Mali Report: Enquête Démographique et de Santé (EDSM VI) Mali; CPS/SSDSPF: Calverton, MD, USA, 2018. [Google Scholar]
- DGSHP. Carte Saniatire Revisée Du Mali Bamako Mali; DGSHP: Bamako, Mali, 2019. [Google Scholar]
- François, H.; Lê, S.; Pagès, J. Analyse de Données Avec R, 2nd ed.; Presses Universitaires de Rennes: Rennes, France, 2009; ISBN 978-2-7535-4869-5. [Google Scholar]
- Simon, N. Wood Generalized Additive Models: An introduction with R; Chapman and Hall/CRC: Boca Raton, FL, USA, 2017; p. 392. [Google Scholar]
- Abiodun, G.J.; Makinde, O.S.; Adeola, A.M.; Njabo, K.Y.; Witbooi, P.J.; Djidjou-Demasse, R.; Botai, J.O. A Dynamical and Zero-Inflated Negative Binomial Regression Modelling of Malaria Incidence in Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2019, 16, 2000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaudart, J.; Poudiougou, B.; Dicko, A.; Ranque, S.; Toure, O.; Sagara, I.; Diallo, M.; Diawara, S.; Ouattara, A.; Diakite, M.; et al. Space-Time Clustering of Childhood Malaria at the Household Level: A Dynamic Cohort in a Mali Village. BMC Public Health 2006, 6, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sissoko, M.S.; Sissoko, K.; Kamate, B.; Samake, Y.; Goita, S.; Dabo, A.; Yena, M.; Dessay, N.; Piarroux, R.; Doumbo, O.K.; et al. Temporal Dynamic of Malaria in a Suburban Area along the Niger River. Malar. J. 2017, 16, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO|Malaria in Children under Five. Available online: http://www.who.int/malaria/areas/high_risk_groups/children/en/ (accessed on 10 September 2020).
- Hamidou, R.L.; Moustapha, L.M.; Maiga, M.A.; Djibo, Y.H.; Mouhaimouni, M.; Boubacar, A.; Ibrahim, M.L. Influence des facteurs climatiques sur la morbidité palustre à Tillabéry au Niger. Médecine d’Afrique Noire 2018, 65, 389. [Google Scholar]
- Saugeon, C.; Baldet, T.; Akogbeto, M.; Henry, M.C. Will climate and demography have a major impact on malaria in sub-Saharan Africa in the next 20 years. Med. Trop. (Mars) 2009, 69, 203–207. [Google Scholar]
- Park, J.W.; Cheong, H.K.; Honda, Y.; Ha, M.; Kim, H.; Kolam, J.; Inape, K.; Mueller, I. Time Trend of Malaria in Relation to Climate Variability in Papua New Guinea. Environ. Health Toxicol. 2016, 31. [Google Scholar] [CrossRef] [Green Version]
- Matubi, E.M.; Bukaka, E.; Luemba, T.B.; Situakibanza, H.; Sangaré, I.; Mesia, G.; Ngoyi, D.M.; Maniania, N.K.; Akikwa, C.N.; Kanza, J.P.B.; et al. Détermination Des Paramètres Bioécologiques et Entomologiques d’Anopheles Gambiae Sl Dans La Transmission Du Paludisme à Bandundu-Ville, République Démocratique de Congo. Pan. Afr. Med. J. 2015, 22. [Google Scholar] [CrossRef]
- Wu, D.F.; Löhrich, T.; Sachse, A.; Mundry, R.; Wittig, R.M.; Calvignac-Spencer, S.; Deschner, T.; Leendertz, F.H. Seasonal and Inter-Annual Variation of Malaria Parasite Detection in Wild Chimpanzees. Malar. J. 2018, 17, 38. [Google Scholar] [CrossRef] [Green Version]
- Ouedraogo, B.; Inoue, Y.; Kambiré, A.; Sallah, K.; Dieng, S.; Tine, R.; Rouamba, T.; Herbreteau, V.; Sawadogo, Y.; Ouedraogo, L.S.L.W.; et al. Spatio-Temporal Dynamic of Malaria in Ouagadougou, Burkina Faso, 2011–2015. Malar. J. 2018, 17. [Google Scholar] [CrossRef] [Green Version]
- Reid, H.L.; Haque, U.; Roy, S.; Islam, N.; Clements, A.C. Characterizing the Spatial and Temporal Variation of Malaria Incidence in Bangladesh, 2007. Malar. J. 2012, 11, 170. [Google Scholar] [CrossRef] [Green Version]
- Dicko, A.; Sagara, I.; Sissoko, M.S.; Guindo, O.; Diallo, A.I.; Kone, M.; Toure, O.B.; Sacko, M.; Doumbo, O.K. Impact of Intermittent Preventive Treatment with Sulphadoxine-Pyrimethamine Targeting the Transmission Season on the Incidence of Clinical Malaria in Children in Mali. Malar. J. 2008, 7, 123. [Google Scholar] [CrossRef] [Green Version]
- Coulibaly, D.; Rebaudet, S.; Travassos, M.; Tolo, Y.; Laurens, M.; Kone, A.K.; Traore, K.; Guindo, A.; Diarra, I.; Niangaly, A.; et al. Spatio-Temporal Analysis of Malaria within a Transmission Season in Bandiagara, Mali. Malar. J. 2013, 12, 82. [Google Scholar] [CrossRef] [Green Version]
- Cissoko, M.; Sagara, I.; Sankaré, M.H.; Dieng, S.; Guindo, A.; Doumbia, Z.; Allasseini, B.; Traore, D.; Fomba, S.; Bendiane, M.K.; et al. Geo-Epidemiology of Malaria at the Health Area Level, Dire Health District, Mali, 2013–2017. Int. J. Environ. Res. Public Health 2020, 17, 3982. [Google Scholar] [CrossRef]
- Touré, M.; Sanogo, D.; Dembele, S.; Diawara, S.I.; Oppfeldt, K.; Schiøler, K.L.; Haidara, D.B.; Traoré, S.F.; Alifrangis, M.; Konradsen, F.; et al. Seasonality and Shift in Age-Specific Malaria Prevalence and Incidence in Binko and Carrière Villages Close to the Lake in Selingué, Mali. Malar. J. 2016, 15, 219. [Google Scholar] [CrossRef] [Green Version]
- Diakité, S.A.S.; Traoré, K.; Sanogo, I.; Clark, T.G.; Campino, S.; Sangaré, M.; Dabitao, D.; Dara, A.; Konaté, D.S.; Doucouré, F.; et al. A Comprehensive Analysis of Drug Resistance Molecular Markers and Plasmodium Falciparum Genetic Diversity in Two Malaria Endemic Sites in Mali. Malar. J. 2019, 18, 361. [Google Scholar] [CrossRef] [Green Version]
- Mouchet, J.; Carnevale, P.; Coosemans, M.; Fontenille, D.; Ravaonjanahary, C.; Richard, A.; Robert, V. Typologie du paludisme en Afrique. Cahier Santé 1993, 3, 20. [Google Scholar]
- Gaudart, J.; Touré, O.; Dessay, N.; lassane Dicko, A.; Ranque, S.; Forest, L.; Demongeot, J.; Doumbo, O.K. Modelling Malaria Incidence with Environmental Dependency in a Locality of Sudanese Savannah Area, Mali. Malar. J. 2009, 8, 61. [Google Scholar] [CrossRef]
- Gaudart, J.; Dessay, N.; Touré, O.; Fané, M.; Sabatier, P.; Doumbo, O. Rapport, Analyse du Changement Climatique et de ses Impacts sur l’eau et la Santé: Développement d’une Méthodologie Appliquée à l’évaluation du Risque Palustre; GICC-ACCIES, Aix Marseille Université: Bamako, Mali, 2017. [Google Scholar]
- Tandina, F.; Doumbo, O.; Yaro, A.S.; Traoré, S.F.; Parola, P.; Robert, V. Mosquitoes (Diptera: Culicidae) and Mosquito-Borne Diseases in Mali, West Africa. Parasites Vectors 2018, 11, 467. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, J.G.; Touré, M.B.; Sogoba, N.; Doumbia, S.O.; Gomis, J.F.; Ndiaye, M.; Ndiaye, D.; Diarra, A.; Abubakar, I.; Ahmad, A.; et al. Clustering of Asymptomatic Plasmodium Falciparum Infection and the Effectiveness of Targeted Malaria Control Measures. Malar. J. 2020, 19, 33. [Google Scholar] [CrossRef] [Green Version]
- Magombedze, G.; Ferguson, N.M.; Ghani, A.C. A Trade-off between Dry Season Survival Longevity and Wet Season High Net Reproduction Can Explain the Persistence of Anopheles Mosquitoes. Parasit Vectors 2018, 11, 576. [Google Scholar] [CrossRef]
- Krajacich, B.J.; Sullivan, M.; Faiman, R.; Veru, L.; Graber, L.; Lehmann, T. Induction of Long-Lived Potential Aestivation States in Laboratory An. Gambiae Mosquitoes. Parasit Vectors 2020, 13, 412. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Health District | Average Annual Rainfall (mm) | Average Annual Temperature (°C) |
|---|---|---|
| Kati | 789.6 | 30 |
| Kadiolo | 1000 | 27.6 |
| Sikasso | 1100 | 27 |
| Tominian | 500 | 30 |
| Yorosso | 681.7 | 28 |
| Health District | Sum of Annual Cases | Rate Variation (%) | ||
|---|---|---|---|---|
| 2016 | 2017 | 2018 | ||
| Kati | 66,781 | 53,276 | 50,660 | 24.14 |
| Kadiolo | 62,314 | 58,614 | 53,522 | 14.11 |
| Sikasso | 41,720 | 47,620 | 42,206 | −1.16 |
| Tominian | 31,096 | 30,033 | 28,325 | 8.91 |
| Yorosso | 34,511 | 38,274 | 49,692 | −43.99 |
| Variables | p-Value | Test |
|---|---|---|
| Average monthly rainfall | 0.296 | ANOVA |
| Average monthly temperature | 0.686 | ANOVA |
| Average monthly relative humidity | <0.001 | Kruskal–Wallis |
| Nonparametric Part | p-Value | Deviance |
|---|---|---|
| Dim-1 (Northern Sudan and Sahel Zone) | <0.001 | |
| Dim-2 (Northern Sudan and Sahel Zone) | <0.001 | 74% |
| Dim-1 (Sudano-Guinean) | <0.001 | |
| Dim-2 (Sudano-Guinean) | 0.006 | 50% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacko, A.; Sagara, I.; Berthé, I.; Diarra, M.; Cissoko, M.; Diarra, S.S.; Coulibaly, D.; Sanogo, M.; Dicko, A. Evolution of Malaria Incidence in Five Health Districts, in the Context of the Scaling up of Seasonal Malaria Chemoprevention, 2016 to 2018, in Mali. Int. J. Environ. Res. Public Health 2021, 18, 840. https://doi.org/10.3390/ijerph18020840
Sacko A, Sagara I, Berthé I, Diarra M, Cissoko M, Diarra SS, Coulibaly D, Sanogo M, Dicko A. Evolution of Malaria Incidence in Five Health Districts, in the Context of the Scaling up of Seasonal Malaria Chemoprevention, 2016 to 2018, in Mali. International Journal of Environmental Research and Public Health. 2021; 18(2):840. https://doi.org/10.3390/ijerph18020840
Chicago/Turabian StyleSacko, Aissata, Issaka Sagara, Ibrahima Berthé, Modibo Diarra, Mady Cissoko, Souleymane S. Diarra, Drissa Coulibaly, Moussa Sanogo, and Alassane Dicko. 2021. "Evolution of Malaria Incidence in Five Health Districts, in the Context of the Scaling up of Seasonal Malaria Chemoprevention, 2016 to 2018, in Mali" International Journal of Environmental Research and Public Health 18, no. 2: 840. https://doi.org/10.3390/ijerph18020840
APA StyleSacko, A., Sagara, I., Berthé, I., Diarra, M., Cissoko, M., Diarra, S. S., Coulibaly, D., Sanogo, M., & Dicko, A. (2021). Evolution of Malaria Incidence in Five Health Districts, in the Context of the Scaling up of Seasonal Malaria Chemoprevention, 2016 to 2018, in Mali. International Journal of Environmental Research and Public Health, 18(2), 840. https://doi.org/10.3390/ijerph18020840