
The Effect of Exercise Compliance on Risk Reduction for Hamstring Strain Injury: A Systematic Review and Meta-Analyses


 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Quality Assessment
2.4. Statistical Analyses
3. Results
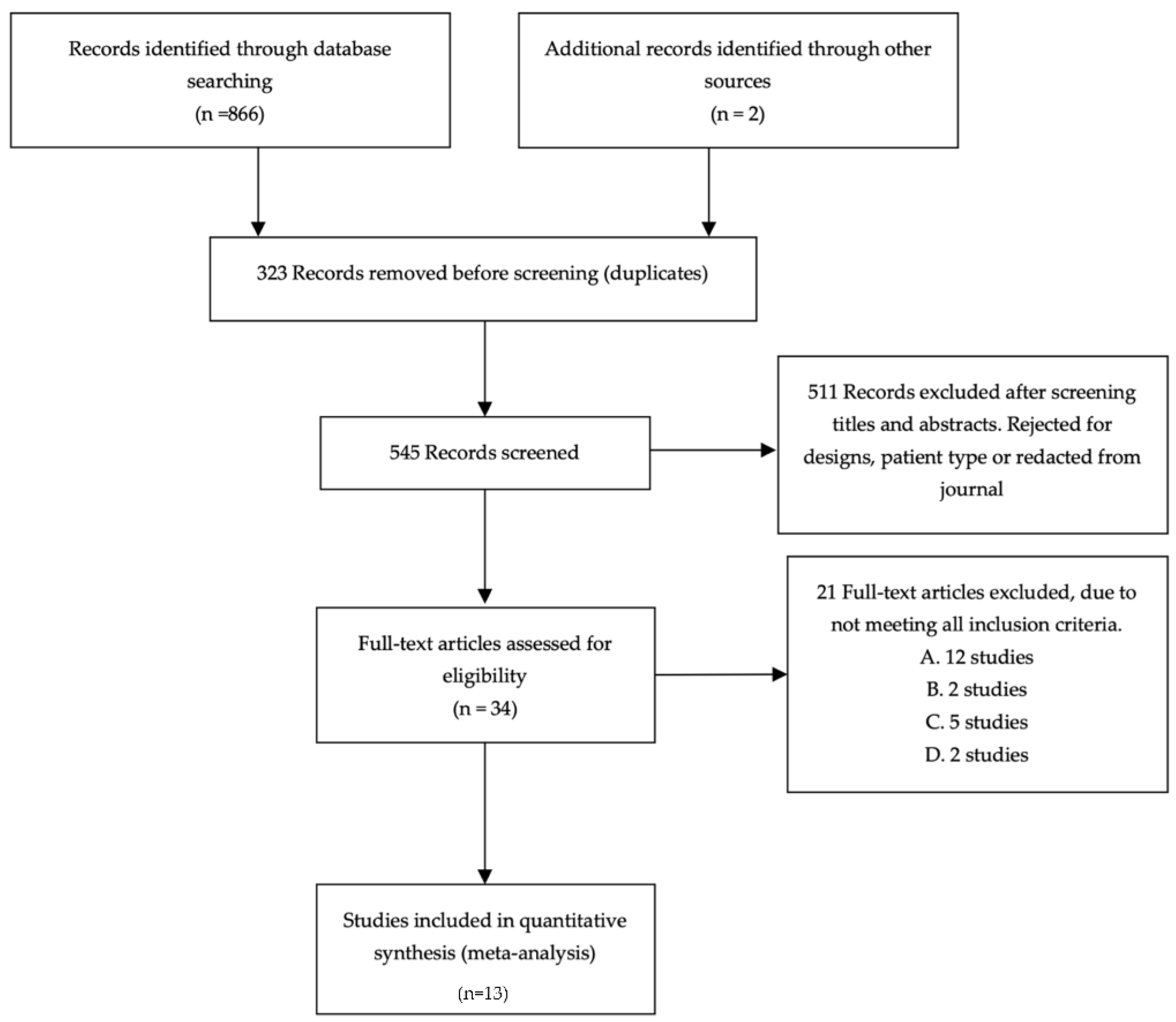
3.1. Search Results
3.2. Characteristics of the Included Studies
3.3. Quality of Studies
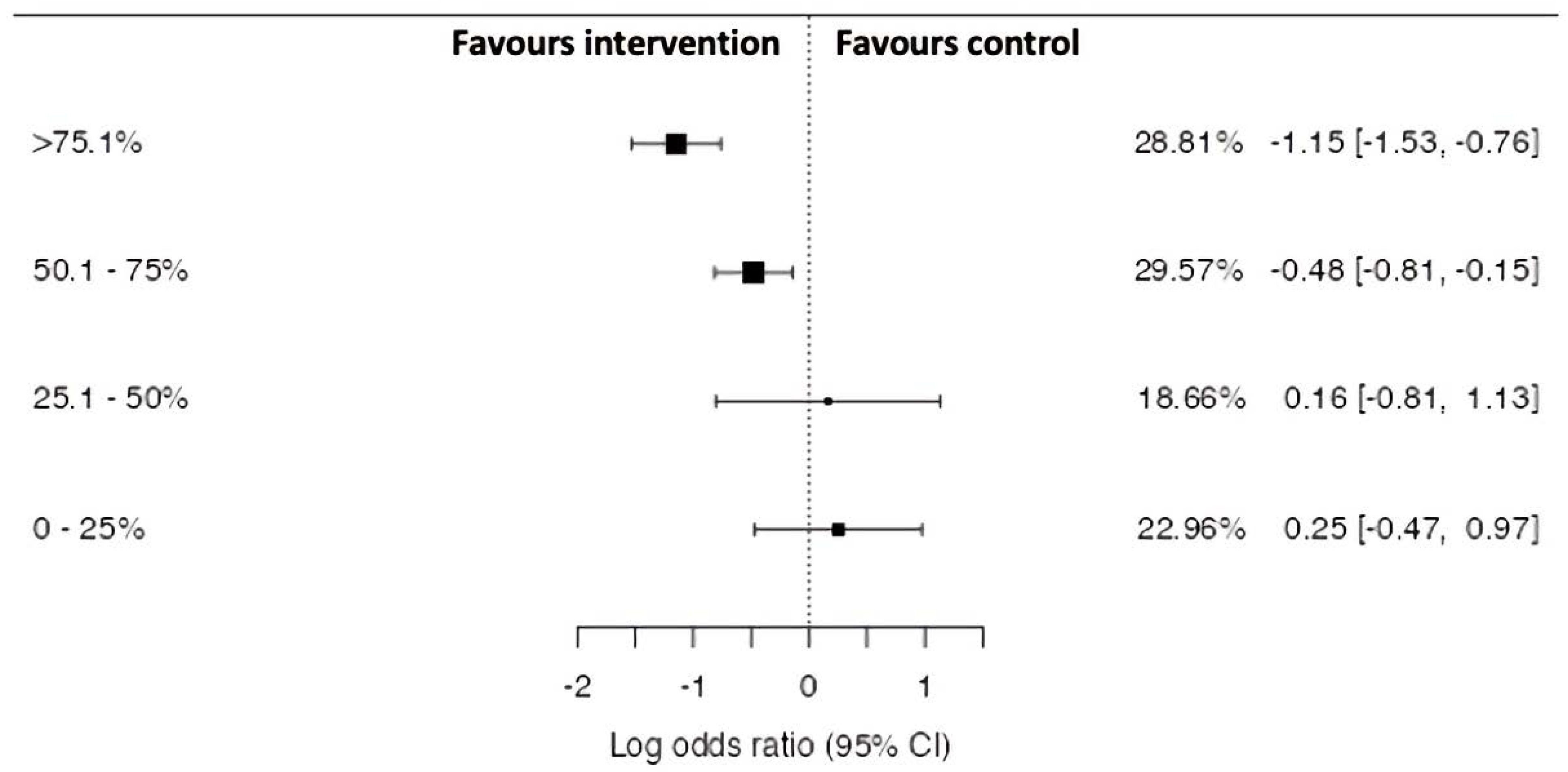
3.4. Meta-Analysis Findings
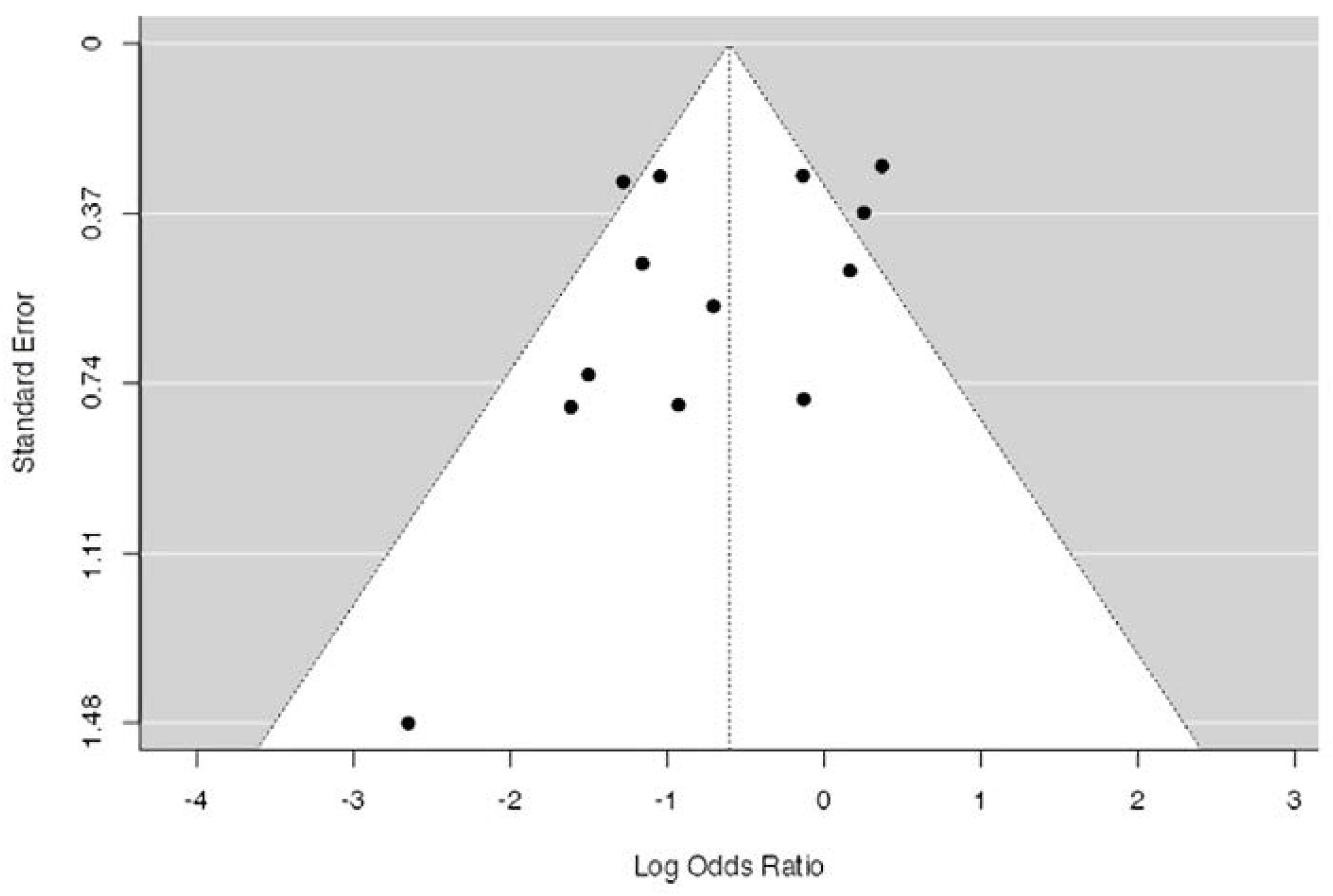
3.5. Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bahr, R.; Thorborg, K.; Ekstrand, J. Evidence-based hamstring injury prevention is not adopted by the majority of Champions League or Norwegian Premier League football teams: The Nordic Hamstring survey. Br. J. Sports Med. 2015, 49, 1466–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Waldén, M.; Hägglund, M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: A 13-year longitudinal analysis of the UEFA Elite Club injury study. Br. J. Sports Med. 2016, 50, 731–737. [Google Scholar] [CrossRef] [Green Version]
- Ekstrand, J. Keeping your top players on the pitch: The key to football medicine at a professional level. Br. J. Sports Med. 2013, 47, 723–724. [Google Scholar] [CrossRef] [Green Version]
- Askling, C.; Karlsson, J.; Thorstensson, A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand. J. Med. Sci. Sports 2003, 13, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Mjolsnes, R.; Árnason, A.; Osthagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmich, P. Preventive Effect of Eccentric Training on Acute Hamstring Injuries in Men’s Soccer: A cluster-randomized controlled trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef] [PubMed]
- Seagrave, I.R.A.; Perez, L.; McQueeney, S.; Toby, E.B.; Key, V.; Nelson, J.D. Preventive effects of eccentric training on acute hamstring muscle injury in professional baseball. Orthop. J. Sports Med. 2014, 2, 1–7. [Google Scholar] [CrossRef]
- Bourne, M.N.; Timmins, R.; Opar, D.; Pizzari, T.; Ruddy, J.D.; Sims, C.; Williams, M.D.; Shield, A. An evidence-based framework for strengthening exercises to prevent hamstring injury. Sports Med. 2018, 48, 251–267. [Google Scholar] [CrossRef]
- Chesterton, P.; Tears, C. The uptake of the Nordic hamstring exercise programme as an injury prevention strategy in professional cricket in the United Kingdom and barriers to implementation. Phys. Ther. Sport 2021, 50, 1–6. [Google Scholar] [CrossRef]
- Chesterton, P.; Tears, C.; Wright, M.; Portas, M. Hamstring injury prevention practices and compliance of the Nordic hamstring program in English professional football. Transl. Sports Med. 2020, 4, 214–222. [Google Scholar] [CrossRef]
- Morgan, D. New insights into the behavior of muscle during active lengthening. Biophys. J. 1990, 57, 209–221. [Google Scholar] [CrossRef] [Green Version]
- Morgan, D.L.; Proske, U. Popping sarcomere hypothesis explains stretch-induced muscle damage. Clin. Exp. Pharmacol. Physiol. 2004, 34, 19–23. [Google Scholar] [CrossRef]
- Šarabon, N.; Marusic, J.; Marković, G.; Kozinc, Ž. Kinematic and electromyographic analysis of variations in Nordic hamstring exercise. PLoS ONE 2019, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Sconce, E.; Heller, B.; Maden-Wilkinson, T.; Hamilton, N. Development of a Novel Nordic Hamstring Exercise Device to Measure and Modify the Knee Flexors’ Torque-Length Relationship. Front. Sports Act. Living 2021, 3, 1–9. [Google Scholar] [CrossRef]
- Howatson, G.; van Someren, K.A. Evidence of a contralateral repeated bout effect after maximal eccentric contractions. Eur. J. Appl. Physiol. 2007, 101, 207–214. [Google Scholar] [CrossRef]
- Green, B.; Bourne, M.N.; Van Dyk, N.; Pizzari, T. Recalibrating the risk of hamstring strain injury (HSI): A 2020 systematic review and meta-analysis of risk factors for index and recurrent HSI in sport. Br. J. Sports Med. 2020, 54, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Silvers-Granelli, H.; Mandelbaum, B.R.; Adeniji, O.; Insler, S.; Bizzini, M.; Pohlig, R.; Junge, A.; Snyder-Mackler, L.; Dvorak, J. Efficacy of the FIFA 11+ Injury Prevention Program in the Collegiate Male Soccer Player. Am. J. Sports Med. 2015, 43, 2628–2637. [Google Scholar] [CrossRef] [Green Version]
- Thorborg, K.; Krommes, K.; Esteve, E.; Clausen, M.B.; Bartels, E.M.; Rathleff, M.S. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: A systematic review and meta-analysis of the FIFA 11 and 11+ programmes. Br. J. Sports Med. 2017, 51, 562–571. [Google Scholar] [CrossRef]
- Alonso-Fernandez, D.; Docampo-Blanco, P.; Martinez-Fernandez, J. Changes in muscle architecture of biceps femoris induced by eccentric strength training with nordic hamstring exercise. Scand. J. Med. Sci. Sports 2018, 28, 88–94. [Google Scholar] [CrossRef]
- Alt, T.; Nodler, Y.T.; Severin, J.; Knicker, A.J.; Strüder, H.K. Velocity-specific and time-dependent adaptations following a standardized Nordic Hamstring Exercise training. Scand. J. Med. Sci. Sports 2018, 28, 65–76. [Google Scholar] [CrossRef]
- Bourne, M.; Duhig, S.; Timmins, R.G.; Williams, M.D.; Opar, D.; Al Najjar, A.; Kerr, G.; Shield, A. impact of the Nordic hamstring and hip extension exercises on hamstring architecture and morphology: Implications for injury prevention. Br. J. Sports Med. 2017, 51, 469–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuthbert, M.; Ripley, N.; McMahon, J.J.; Evans, M.; Haff, G.G.; Comfort, P. The effect of nordic hamstring exercise intervention volume on eccentric strength and muscle architecture adaptations: A systematic review and meta-analyses. Sports Med. 2019, 50, 83–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, B.W.; Young, W.B.; Talpey, S.W.; Smyth, A.M.; Pane, C.L.; Carlon, T.A. The effects of sprint training and the Nordic hamstring exercise on eccentric hamstring strength and sprint performance in adolescent athletes. J. Sports Med. Phys. Fit. 2019, 59, 1119–1125. [Google Scholar] [CrossRef]
- Jakobsen, J.R.; Mackey, A.; Knudsen, A.B.; Koch, M.; Kjaer, M.; Krogsgaard, M.R. Composition and adaptation of human myotendinous junction and neighboring muscle fibers to heavy resistance training. Scand. J. Med. Sci. Sports 2017, 27, 1547–1559. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.W.; Opar, D.A.; Williams, M.D.; Bourne, M.N.; Timmins, R.G. Razor hamstring curl and Nordic hamstring exercise architectural adaptations: Impact of exercise selection and intensity. Scand. J. Med. Sci. Sports 2019, 29, 706–715. [Google Scholar] [CrossRef]
- Presland, J.D.; Timmins, R.; Bourne, M.; Williams, M.D.; Opar, D. The effect of Nordic hamstring exercise training volume on biceps femoris long head architectural adaptation. Scand. J. Med. Sci. Sports 2018, 28, 1775–1783. [Google Scholar] [CrossRef] [PubMed]
- Presland, J.; Opar, D.; Dow, C.L.; Bourne, M.; Williams, M.; Hickey, J.; Timmins, R. Eccentrically overloaded flywheel training increases biceps femoris long head fascicle length. J. Sci. Med. Sport 2017, 20. [Google Scholar] [CrossRef]
- Ripley, N.; Comfort, P.; McMahon, J. Retention of adaptations to eccentric hamstring strength and bicep femoris fascicle length from a seven-week sprint or nordic training intervention. J. Strength Cond. Res. 2021, 35, e3–e288. Available online: https://journals.lww.com/nsca-jscr/Fulltext/2021/04000/2020_NSCA_Research_Abstracts.41.aspx (accessed on 21 October 2021).
- Goode, A.P.; Reiman, M.P.; Harris, L.; DeLisa, L.; Kauffman, A.; Beltramo, D.; Poole, C.; Ledbetter, L.; Taylor, A.B. Eccentric training for prevention of hamstring injuries may depend on intervention compliance: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 349–356. [Google Scholar] [CrossRef] [Green Version]
- Van Dyk, N.; Behan, F.P.; Whiteley, R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: A systematic review and meta-analysis of 8459 athletes. Br. J. Sports Med. 2019, 53, 1362–1370. [Google Scholar] [CrossRef] [Green Version]
- Vatovec, R.; Kozinc, Ž.; Šarabon, N. Exercise interventions to prevent hamstring injuries in athletes: A systematic review and meta-analysis. Eur. J. Sport Sci. 2020, 20, 992–1004. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; McCall, A.; van Smeden, M. Why methods matter in a meta-analysis: A reappraisal showed inconclusive injury preventive effect of Nordic hamstring exercise. J. Clin. Epidemiol. 2021, 140, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Van Reijen, M.; Vriend, I.; Van Mechelen, W.; Finch, C.F.; Verhagen, E.A. Compliance with sport injury prevention interventions in randomised controlled trials: A systematic review. Sports Med. 2016, 46, 1125–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA group preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Valle, X.; Malliaropoulos, N.; Botero, J.D.P.; Bikos, G.; Pruna, R.; Mónaco, M.; Maffulli, N.; Párraga, J.D. Hamstring and other thigh injuries in children and young athletes. Scand. J. Med. Sci. Sports 2018, 28, 2630–2637. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Goldman, E.; Jones, D. Interventions for presenting hamstring injuries. Cochrane Database Syst. Rev. 2010, 1, CD006782. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soligard, T.; Myklebust, G.; Steffen, K.; Holme, I.; Silvers, H.; Bizzini, M.; Junge, A.; Dvorak, J.; Bahr, R.; Andersen, T.E. Comprehensive warm-up programme to prevent injuries in young female footballers: Cluster randomised controlled trial. BMJ 2008, 337, a2469. [Google Scholar] [CrossRef] [Green Version]
- Gabbe, B.; Branson, R.; Bennell, K. A pilot randomised controlled trial of eccentric exercise to prevent hamstring injuries in community-level Australian Football. J. Sci. Med. Sport 2006, 9, 103–109. [Google Scholar] [CrossRef]
- Engebretsen, A.H.; Myklebust, G.; Holme, I.; Engebretsen, L.; Bahr, R. Prevention of injuries among male soccer players: A prospective, randomized intervention study targeting players with previous injuries or reduced function. Am. J. Sports Med. 2008, 36, 1052–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Horst, N.; Smits, D.-W.; Petersen, J.; Goedhart, E.A.; Backx, F.J. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: A randomized controlled trial. Am. J. Sports Med. 2015, 43, 1316–1323. [Google Scholar] [CrossRef]
- Sebelien, C.; Stiller, C.; Maher, S.; Qu, X. Effects of implementing nordic hamstring exercises for semi-professional soccer players in Akershus, Norway. OPTP 2014, 26, 2–14. [Google Scholar]
- Van De Hoef, S.; Huisstede, B.M.A.; Brink, M.S.; De Vries, N.; Goedhart, E.A.; Backx, F.J.G. The preventive effect of the bounding exercise programme on hamstring injuries in amateur soccer players: The design of a randomized controlled trial. BMC Musculoskelet. Disord. 2017, 18, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinosa, G.D.A.; Pöyhönen, T.; Aramendi, J.F.; Samaniego, J.C.; Knörr, J.I.E.; Kyröläinen, H. Effects of an eccentric training programme on hamstring strain injuries in women football players. Biomed. Hum. Kinet. 2015, 7, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Van Beijsterveldt, A.M.C.; Van De Port, I.G.L.; Krist, M.R.; Schmikli, S.L.; Stubbe, J.H.; E Frederiks, J.; Backx, F.J.G. Effectiveness of an injury prevention programme for adult male amateur soccer players: A cluster-randomised controlled trial. Sport Geneeskd 2012, 45, 6–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Attar, W.S.A.; Soomro, N.; Pappas, E.; Sinclair, P.J.; Sanders, R.H. Adding a post-training FIFA 11 + exercise program to the pre-training FIFA 11 + injury prevention program reduces injury rates among male amateur soccer players: A cluster-randomised trial. J. Physiother. 2017, 63, 235–242. [Google Scholar] [CrossRef]
- Hasebe, Y.; Akasaka, K.; Otsudo, T.; Tachibana, Y.; Hall, T.; Yamamoto, M. Effects of nordic hamstring exercise on hamstring injuries in high school soccer players: A randomized cntrolled trial. Int. J. Sports Med. 2020, 41, 154–160. [Google Scholar] [CrossRef]
- Árnason, A.; Andersen, T.E.; Holme, I.; Engebretsen, L.; Bahr, R. Prevention of hamstring strains in elite soccer: An intervention study. Scand. J. Med. Sci. Sports 2008, 18, 40–48. [Google Scholar] [CrossRef]
- Chebbi, S.; Chamari, K.; Van Dyk, N.; Gabbett, T.; Tabben, M. Hamstring injury prevention for elite soccer players: A real-world prevention program showing the effect of players’ compliance on the outcome. J. Strength Cond. Res. 2020. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.K.; Lonsdale, C.; Ho, P.Y.; Yung, P.S.-H.; Chan, K.M. patient motivation and adherence to postsurgery rehabilitation exercise recommendations: The influence of physiotherapists’ autonomy-supportive behaviors. Arch. Phys. Med. Rehabil. 2009, 90, 1977–1982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedrich, M.; Gittler, G.; Halberstadt, Y.; Cermak, T.; Heiller, I. Combined exercise and motivation program: Effect on the compliance and level of disability of patients with chronic low back pain: A randomized controlled trial. Arch. Phys. Med. Rehabil. 1998, 79, 475–487. [Google Scholar] [CrossRef]
- Hayden, J.A.; van Tulder, M.; Tomlinson, G. Systematic review: Strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann. Intern. Med. 2005, 142, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man. Ther. 2010, 15, 220–228. [Google Scholar] [CrossRef]
- McHugh, M.P.; Tyler, T.F.; Greenberg, S.C.; Gleim, G.W. Differences in activation patterns between eccentric and concentric quadriceps contractions. J. Sports Sci. 2002, 20, 83–91. [Google Scholar] [CrossRef]
- Nosaka, K.; Lavender, A.; Newton, M.; Sacco, P. Muscle damage in resistance training - is muscle damage necessary for strength gain and muscle hypertrophy? Int. J. Sport Health Sci. 2003, 1, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Chalker, W.J.; Shield, A.; Opar, D.A.; Rathbone, E.N.; Keogh, J.W. Effect of acute augmented feedback on between limb asymmetries and eccentric knee flexor strength during the Nordic hamstring exercise. PeerJ 2018, 6, e4972. [Google Scholar] [CrossRef] [Green Version]
- Steffen, K.; Emery, C.A.; Romiti, M.; Kang, J.; Bizzini, M.; Dvorak, J.; Finch, C.F.; Meeuwisse, W.H. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: A cluster randomised trial. Br. J. Sports Med. 2013, 47, 794–802. [Google Scholar] [CrossRef] [Green Version]
- Steffen, K.; Meeuwisse, W.H.; Romiti, M.; Kang, J.; McKay, C.; Bizzini, M.; Dvorak, J.; Ao, C.F.; Myklebust, G.; Emery, C.A. Evaluation of how different implementation strategies of an injury prevention programme (FIFA 11+) impact team adherence and injury risk in Canadian female youth football players: A cluster-randomised trial. Br. J. Sports Med. 2013, 47, 480–487. [Google Scholar] [CrossRef]
- Holm, S. What is wrong with compliance? J. Med. Ethics 1993, 19, 108–110. [Google Scholar] [CrossRef] [Green Version]
- Hyldahl, R.D.; Chen, T.C.; Nosaka, K. Mechanisms and Mediators of the Skeletal Muscle Repeated Bout Effect. Exerc. Sport Sci. Rev. 2017, 45, 24–33. [Google Scholar] [CrossRef]
- McHugh, M.P. Recent advances in the understanding of the repeated bout effect: The protective effect against muscle damage from a single bout of eccentric exercise. Scand. J. Med. Sci. Sports 2003, 13, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Ishøi, L.; Hölmich, P.; Aagaard, P.; Thorborg, K.; Bandholm, T.; Serner, A. Effects of the nordic hamstring exercise on sprint capacity in male football players: A randomized controlled trial. J. Sports Sci. 2018, 36, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Alvares, J.B.D.A.R.; Marques, V.B.; Vaz, M.A.; Baroni, B.M. Four weeks of nordic hamstring exercise reduce muscle injury risk factors in young adults. J. Strength Cond. Res. 2018, 32, 1254–1262. [Google Scholar] [CrossRef] [PubMed]
- Van De Hoef, P.S.; Brink, M.; Huisstede, B.B.; van Smeden, M.; De Vries, N.N.; Goedhart, E.E.; Gouttebarge, V.V.; Backx, F.F. Does a bounding exercise program prevent hamstring injuries in adult male soccer players?—A cluster-RCT. Scand. J. Med. Sci. Sports 2019, 29, 515–523. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W. Improving meta-analyses in sport and exercise science. Sportscience 2018, 22, 11–17. [Google Scholar]
- Ripley, N.; Comfort, P.; McMahon, J. The effects of a seven-week sprint vs. nordic training intervention on the modifiable risk factors of hamstring strain injury and performance. J. Strength Cond. Res. 2021, 35, e3–e288. Available online: https://journals.lww.com/nsca-jscr/Fulltext/2021/04000/2020_NSCA_Research_Abstracts.41.aspx (accessed on 21 October 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Injury | Prevention | Training | Study |
|---|---|---|---|
| Hamstring strain injury | Injury prevention | Resistance training | Randomised control trial (RCT) |
| Hamstring injury | Hamstring injury prevention | Strength training | Sport |
| Posterior thigh injury | Primary prevention | Eccentric | Team sport |
| Lower extremity strain | Injury prevention programmes | Eccentric training | Soccer |
| Lower limb injury | Injury risk reduction | Nordic hamstring exercise | |
| Compliance | Nordics | ||
| Warm up | |||
| FIFA 11 | |||
| FIFA 11+ | |||
| Plyometrics | |||
| Sprinting |
| Reference | Population | Intervention Description | Sessions Planned | Compliant Sessions Completed | Weeks per Session | Observation Period | n Intervention | n Control | Number of Injuries Intervention | Number of Injuries Control | Compliance (%) | Log Odds Ratio (95% CI) | Weighted Mean Difference (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gabbe et al. [40] | Male Australian amateur soccer players | NHE training intervention (12 × 6) | 5 | 2.4 | 15.3 | 1 season | 114 | 106 | 10 | 8 | 47.0% | 0.16(−0.81 to 1.13) | 8.10% |
| Engebretsen et al. [41] | Male Norwegian soccer players | 10-week NHE training intervention from Mjølsnes et al. (2004) | 27 | 5.7 | 6.3 | 1 season | 85 | 76 | 23 | 17 | 21.1% | 0.25 (−0.47 to 0.97) | 9.81% |
| Askling, Karlsson and Thorstensson [4] | Male Swedish soccer players | 10-week eccentric training intervention (“Yo-Yo” ergometer) | 16 | 16.0 | 2.9 | 46 weeks | 15 | 15 | 3 | 10 | 100.0% | −1.50 (−2.92 to–0.09) | 5.62% |
| Van der Horst et al. [42] | Male Dutch amateur soccer players | 13-week NHE training intervention from Mjølsnes et al. (2004) | 25 | 22.8 | 2.3 | 12 months | 292 | 287 | 6 | 18 | 91.0% | −1.16 (−2.10 to −0.22) | 8.30% |
| Sebelien et al. [43] | Male Semi-professional soccer players | Progressive NHE training (2 × 5, 1/week–3 × 8–10, 2/week) | 102 | 23.2 | 1.6 | 1 season | 59 | 60 | 0 | 6 | 22.7% | −2.65 (−5.55 to 0.25) | 1.97% |
| Petersen et al. [6] | Male Danish soccer players | 10-week NHE training intervention from Mjølsnes et al. (2004) | 67 | 61.0 | 0.8 | 12 months | 461 | 481 | 15 | 52 | 91.0% | −1.28 (−1.87 to −0.69) | 10.47% |
| Silvers-Granelli et al. [17] | Male NCAA collegiate athletes | FIFA 11+ three times per week. | 60 | 28.2 | 0.7 | 5 months (August–December) | 675 | 850 | 16 | 55 | 47.0% | −1.05 (−1.61 to −0.48) | 10.90% |
| van de Hoef et al. [44] | Male Dutch amateur soccer players | Bounding exercise programme. | 74 | 52.5 | 0.7 | 1 season (9 months) | 229 | 171 | 31 | 26 | 71.0% | 0.14 (−0.70 to 0.43) | 10.92% |
| del ama-espinosa et al. [45] | Female Elite European soccer players | NHE training intervention, 1 × 5 performed once per week for 42 weeks. | 42 | 33.6 | 0.7 | 1 season | 22 | 21 | 3 | 6 | 80.0% | −0.93 (−2.47 to 0.61) | 5.07% |
| Van Beijsterveldt et al. [46] | Male Dutch amateur soccer players | FIFA 11 warm up twice per week. | 74 | 54.0 | 0.7 | 1 season (9 months) | 223 | 233 | 18.4% [38] | 13.4% [29] | 73.0% | 0.37 (−0.15 to 0.89) | 11.20% |
| Saleh et al. [47] | Male Australian amateur soccer players | Additional FIFA 11+ performed post-exercise two-three times per week. | 48 | 39.8 | 0.6 | 6 months | 144 | 136 | 2 | 9 | 83.0% | −1.62 (−3.17 to −0.06) | 5.03% |
| Hasebe et al. [48] | High school male soccer players | Progressive continual NHE training (5 × 2, 1/week–8–10 × 3, 2/week) | 53 | 46.6 | 0.6 | 27 weeks | 156 | 103 | 4 | 3 | 88.0% | −0.13 (−1.65 to 1.39) | 5.17% |
| Soligard et al. [39] | Youth female soccer players | FIFA 11+ warm up, 2/week. | 148 | 87.9 | 0.4 | 1 season | 1055 | 837 | 5 | 8 | 59.4% | −0.71 (−1.83 to 0.41) | 7.16% |
| Reference | 1 * | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Askling, Karlsson and Thorstensson [4] | - | X | - | X | - | - | X | X | X | X | X | 7 |
| Engebretsen et al. [41] | X | X | - | X | - | - | - | X | X | X | X | 6 |
| Petersen et al. [6] | X | X | X | X | - | - | - | X | X | X | X | 7 |
| Van der Horst et al. [42] | X | X | X | X | - | - | - | X | X | X | X | 7 |
| Gabbe et al. [40] | X | X | - | X | - | - | - | - | - | X | X | 4 |
| Sebelien et al. [43] | X | X | X | - | - | - | - | X | X | X | X | 6 |
| del ama-espinosa et al. [45] | X | - | X | - | - | - | X | X | - | X | X | 6 |
| Saleh et al. [47] | X | X | X | - | X | - | - | X | X | - | X | 6 |
| Silvers-Granelli et al. [17] | X | X | X | - | - | - | X | X | - | X | X | 6 |
| Van Beijsterveldt et al. [46] | - | X | X | X | - | - | - | X | - | - | X | 5 |
| Soligard et al. [39] | X | X | X | - | - | - | X | - | - | X | X | 5 |
| van de Hoef et al. [44] | X | X | - | X | - | - | - | - | X | X | X | 5 |
| Hasebe et al. [48] | X | X | X | X | - | - | - | X | X | X | X | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ripley, N.J.; Cuthbert, M.; Ross, S.; Comfort, P.; McMahon, J.J. The Effect of Exercise Compliance on Risk Reduction for Hamstring Strain Injury: A Systematic Review and Meta-Analyses. Int. J. Environ. Res. Public Health 2021, 18, 11260. https://doi.org/10.3390/ijerph182111260
Ripley NJ, Cuthbert M, Ross S, Comfort P, McMahon JJ. The Effect of Exercise Compliance on Risk Reduction for Hamstring Strain Injury: A Systematic Review and Meta-Analyses. International Journal of Environmental Research and Public Health. 2021; 18(21):11260. https://doi.org/10.3390/ijerph182111260
Chicago/Turabian StyleRipley, Nicholas Joel, Matthew Cuthbert, Steven Ross, Paul Comfort, and John James McMahon. 2021. "The Effect of Exercise Compliance on Risk Reduction for Hamstring Strain Injury: A Systematic Review and Meta-Analyses" International Journal of Environmental Research and Public Health 18, no. 21: 11260. https://doi.org/10.3390/ijerph182111260
APA StyleRipley, N. J., Cuthbert, M., Ross, S., Comfort, P., & McMahon, J. J. (2021). The Effect of Exercise Compliance on Risk Reduction for Hamstring Strain Injury: A Systematic Review and Meta-Analyses. International Journal of Environmental Research and Public Health, 18(21), 11260. https://doi.org/10.3390/ijerph182111260