
Italian Expert Consensus on Clinical and Therapeutic Management of Multiple Chemical Sensitivity (MCS)

 ,
, 
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scientific Committee
2.2. Study Design
2.2.1. Pre-Delphi Exercise
2.2.2. Delphi Rounds
2.2.3. Statistics
3. Results and Discussion
3.1. Pre-Delphi and eDelphi Exercises
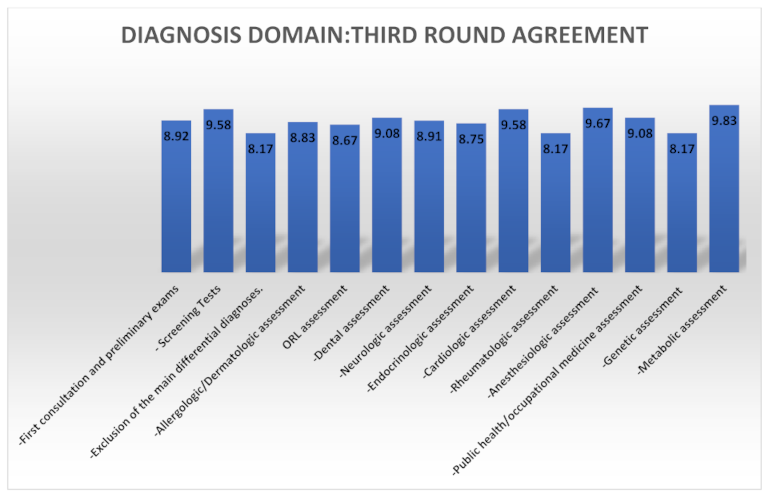
3.2. Diagnosis
3.2.1. First Consultation Exam to Prescribe
- Serum protein electrophoresis;
- Ferritin serum;
- Sodium (Na), magnesium (Mg), zinc (Zn) serum;
- Creatine phosphokinase (CPK) serum;
- Cholinesterase serum/plasma/erythrocyte;
- Erythrocyte sedimentation rate (ESR);
- C-reactive protein (CRP) serum;
- Immunoglobulin E (Total IgE) serum;
- Interleukin-2 receptor (sIL2r) serum;
- Basal serum cortisol;
- Basophil activation test on chemicals known for adverse reactions.
3.2.2. Screening Tests
3.2.3. Main Diagnoses to Exclude
3.2.4. Specialist Evaluations in Patients with MCS
Allergologic/Dermatologic Assessment (I Level)
- Total immunoglobulin E (IgE) dosage and, only in the case of a clinical suspect, specific or recombinant IgE assays (Immuno Solid-Phase Allergen Chip (ISAC®) and in vitro multiplex allergy (i.e., Allergy Explorer-ALEX® and ALEX2®) tests).
- Patch tests are regarded as a second choice as they can cause MCS flares to the patients.
- A lymphocyte transformation test (LTT) is optimal only for testing metal allergies and has approval/approbatory medical–legal validity only for metal allergies.
Otorhinolaryngology (ORL) Assessment (I Level)
Dental Assessment (I Level)
- Mercury (Hg) whole blood.
- Lead (Pb) whole blood.
- Aluminum (Al) whole blood/serum.
- Cadmium (Cd) whole blood.
- Nickel (Ni) whole blood.
- Mercury (Hg) 24 h urine specimens.
- Arsenic (As) 24 h urine specimens.
Neurological Assessment (I Level)
Endocrinologic assessment (I Level)
Cardiological assessment (I Level)
Rheumatologic Assessment (I Level)
Anesthesiologic Assessment (I Level)
Public Health/Occupational Medicine Assessment (I Level)
Genetic Assessment (II Level)
Metabolic Assessment (II Level)
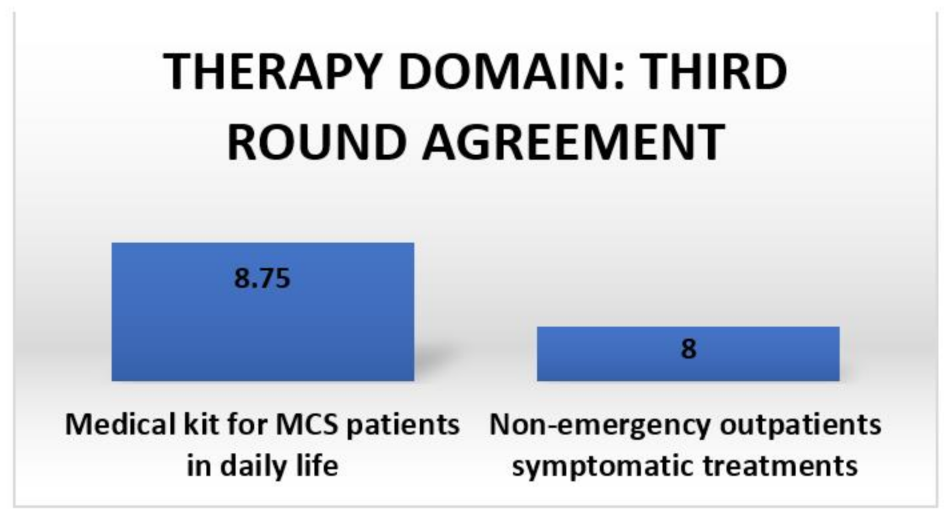
3.3. Therapy Domain
3.3.1. Medical Kit for MCS Patients in Daily Life
- Masks (latex-free paper face masks or cotton masks and filters and/or masks with a high-efficiency particulate absorbing filter (HEPA) and activated carbon filters).
- Air purifiers (portable household air in metal with HEPA filters with activated carbon and a percentage of rubber gaskets < 3% and relative filters and/or air purifiers for cars in metal with HEPA filters with activated carbon and a percentage of rubber gaskets < 3% and relative filters. Air filters should be supplied with an oxygen tank and a glass oxygen bubbler and be phthalate-free and flexible with an oxygen tube with a ceramic mask and latex-free glasses).
- Water purifiers (an active carbon water purifier with a percentage of rubber gaskets < 3%).
3.3.2. Symptomatic Treatments for Non-Emergency Outpatients
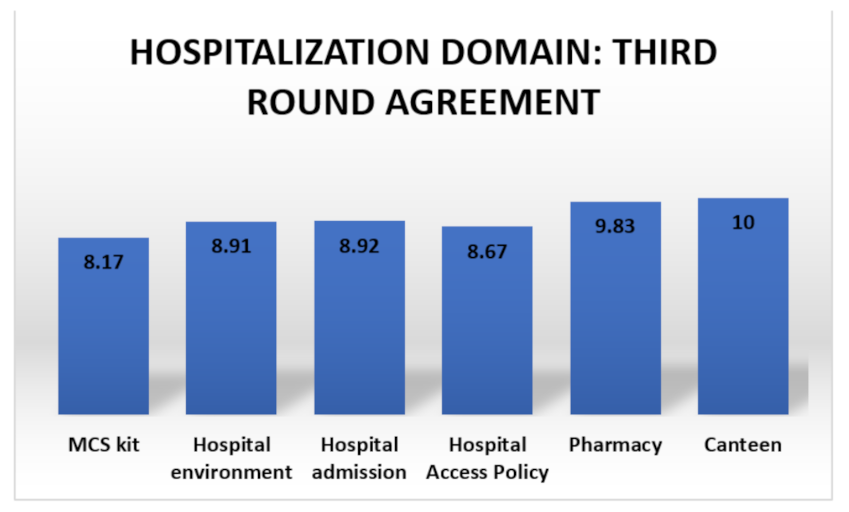
3.4. Hospitalization Domain
- Latex-free surgical gloves;
- Cleaning products without perfumes and hydrogen peroxide;
- Hydrogen peroxide for disinfection;
- 5% dextrose (glucose-intravenous) in a 1000 cc 0.9% NaCl glass drip;
- Porcelain oxygen mask;
- Phthalate-free, flexible oxygen tube;
- Latex-free glasses;
- Inverted sugar solution in a 1000 cc 0.9% NaCl glass drip;
- Sodium bicarbonate solution in glass vials (500 cc);
- Intravenous administration kit in glass;
- Sheets, pillowcases, tablecloths, sterile cotton towels, washed cotton pillows with non-perfumed detergents and without softener (not dry-cleaned);
- Disposable cotton tunics washed with fragrance-free detergents;
- Disposable headgear, shoe covers and tunics;
- Latex-free paper plasters;
- Intravenous butterfly valve;
- Velcro tourniquet/cuff sphygmomanometer;
- Fragrance-free soap for healthcare workers in contact with MCS patients;
- Latex-free paper masks for healthcare workers in contact with MCS patients;
- A 0.9% NaCl 1000 cc solution drip in glass.
3.4.1. Hospital Environment
3.4.2. Hospital Admission
- Arrange MCS patients in a private room marked with a dedicated color (i.e., the MCS kit) with advice prohibiting the access of any person with perfumes;
- Prioritize the arrangement in ventilated rooms far from sources of MCS-recognized triggers (i.e., streets);
- Decontaminate the room in advance (>6 h before the admission);
- Clean the room with water, bicarbonate and fragrance-free detergents;
- Use sheets, pillowcases and 100% cotton towels;
- Mark in the clinical history any allergies, previous drug reactions and tolerated drugs with particular attention paid to antibiotics, anesthetics and disease-modifying antirheumatic drugs (DMARDs);
- Pre-alert the hospital pharmacy, healthcare workers and the canteen service;
- Provide water only in glass bottles with glass cups.
3.4.3. Hospital Access Policy
- Avoid any perfumes, spray or hair products;
- Wash hands with fragrance-free soap or white soap;
- Change their clothes in a dedicated pre-entrance vestibule or a locker room, disinfected and cleaned as an MCS room;
- Have a dedicated MCS kit that contains shirts, gloves (powder-free vinyl or nitrile), latex-free and phthalate-free oxygen tubes and a latex-free oxygen mask.
3.4.4. Pharmacy
- Use only glass bottles for intravenous solutions;
- Do not replace tolerated drugs with generic pharmaceutical products or even with biosimilars (for target therapies);
- Galenic preparations are preferred to packaged drugs due to their lower concentration of preservatives;
- Carefully monitor the drug intake of MCS patients.
3.4.5. Canteen
- Pre-alert the canteen;
- Refer previous food reactions to the canteen;
- Do not cook in aluminum or copper pots;
- Use only glasses, iron cutlery and glass transparent plates (no colored glassware);
- Report any adverse events in the medical history regarding food or beverages.
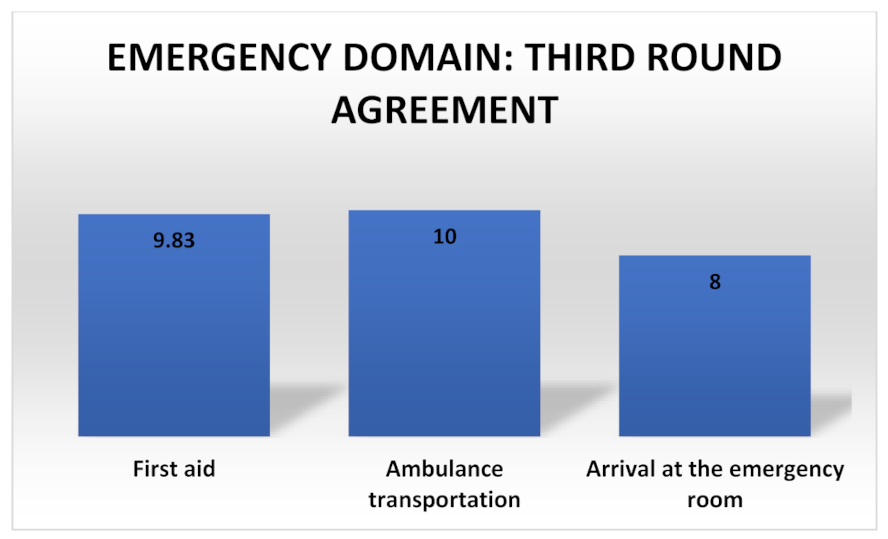
3.5. Emergency Domain
3.5.1. First Aid
- Latex-free and powder-free gloves;
- Latex-free materials for healthcare workers;
- Latex-free oxygen glasses for the patient;
- Hydrogen peroxide solution to decontaminate;
- Glass drip bottles;
- Aluminum roll to seal off any parts of medical equipment (i.e., tubes, rubber gaskets) potentially contaminated by MCS-recognized triggers;
- Ice gown;
- Headgear;
- Disposable paper shoe covers.
3.5.2. Ambulance Transportation
- Avoid environmental deodorants;
- Healthcare workers should avoid smoke, perfumes, hair gel or deodorants 6 h before an ambulance shift;
- Use the emergency kit for MCS.
3.5.3. Arrival at the Emergency Room
- Isolate MCS patients from the other patients and place visitors into a separate room;
- Decontaminate the separate room and remove all potential MCS triggers (i.e., solvents, rubber parts);
- Assign a priority code to the MCS patients;
- Use the MCS kit.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Azuma, K.; Uchiyama, I.; Tanigawa, M.; Bamba, I.; Azuma, M.; Takano, H.; Yoshikawa, T.; Sakabe, K. Chemical intolerance: Involvement of brain function and networks after exposure to extrinsic stimuli perceived as hazardous. Environ. Health Prev. Med. 2019, 24, 61. [Google Scholar] [CrossRef] [PubMed]
- Randolph, T.G. Human ecology and susceptibility to the chemical environment. Ann. Allergy 1961, 19, 779–799. [Google Scholar] [PubMed]
- Cullen, M.R. The worker with multiple chemical sensitivities: An overview. Occup. Med. 1987, 2, 655–661. [Google Scholar] [PubMed]
- Bartha, L.; Baumzweiger, W.; Buscher, D.S.; Callender, T.; Dahl, K.A.; Davidoff, A.; Donnay, A.; Edelson, S.B.; Elson, B.D.; Elliot, E.; et al. Multiple chemical sensitivity: A 1999 consensus. Arch Environ. Health 1999, 54, 147–149. [Google Scholar]
- Lacour, M.; Zunder, T.; Schmidtke, K.; Vaith, P.; Scheidt, C. Multiple chemical sensitivity syndrome: Suggestions for an extension of the US. MCS case definition. Int. J. Hyg. Environ. Health 2005, 208, 141–151. [Google Scholar] [CrossRef]
- Hausteiner, C.; Bornschein, S.; Hansen, J.; Zilker, T.; Forstl, H. Self-reported chemical sensitivity in Germany: A population-based survey. Int. J. Hyg. Environ. Health 2005, 208, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Pigatto, P.D.; Guzzi, G. Prevalence and risk factors for multiple chemical sensitivity in Australia. Prev. Med. Rep. 2019, 14, 100856. [Google Scholar] [CrossRef]
- Caress, S.M.; Steinemann, A.C. A national population study of the prevalence of multiple chemical sensitivity. Arch Environ. Health 2005, 59, 300–305. [Google Scholar] [CrossRef]
- Miller, C.S. Toxicant-induced loss of tolerance. Addiction 2001, 96, 115–137. [Google Scholar] [CrossRef] [PubMed]
- Bell, I.R.; Hardin, E.E.; Baldwin, C.M.; Schwartz, G.E. Increased limbic system symptomatology and sensitizability of young adults with chemical and noise sensitivities. Environ. Res. 1995, 70, 84–97. [Google Scholar] [CrossRef]
- Viziano, A.; Micarelli, A.; Alessandrini, M. Noise sensitivity and hyperacusis in patients affected by multiple chemical sensitivity. Int. Arch Occup. Environ. Health 2017, 90, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Heinonen-Guzejev, M.; Koskenvuo, M.; Mussalo-Rauhamaa, H.; Vuorinen, H.S.; Heikkilä, K.; Kaprio, J. Noise sensitivity and multiple chemical sensitivity scales: Properties in a population based epidemiological study. Noise Health 2012, 14, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Emmett, E.A. Parosmia and hyposmia induced by solvent exposure. Br. J. Ind. Med. 1976, 33, 196–198. [Google Scholar] [CrossRef] [Green Version]
- Doty, R.L.; Deems, D.A.; Frye, R.E.; Pelberg, R.; Shapiro, A. Olfactory sensitivity, nasal resistance, and autonomic function in patients with multiple chemical sensitivities. Arch. Otolaryngol. Head Neck Surg. 1988, 114, 1422–1427. [Google Scholar] [CrossRef]
- Fernandez, M.; Schwartz, G.E.; Bell, I.R. Subjective ratings of odorants by women with chemical sensitivity. Toxicol. Ind. Health 1999, 15, 577–581. [Google Scholar] [CrossRef]
- Mazzatenta, A.; Pokorski, M.; Di Giulio, C. Real time analysis of volatile organic compounds (VOCs) in centenarians. Respir. Physiol. Neurobiol. 2015, 209, 47–51. [Google Scholar] [CrossRef]
- Yunus, M.B. Central sensitivity syndromes: A new paradigm and group nosology for fibromyalgia and overlapping conditions, and the related issue of disease versus illness. Semin. Arthritis Rheum. 2008, 37, 339–352. [Google Scholar] [CrossRef]
- Pigatto, P.D.; Minoia, C.; Ronchi, A.; Brambilla, L.; Ferruci, S.M.; Spadari, F.; Passoni, M.; Somalvico, F.; Bombeccari, G.P.; Guzzi, G. Allergological and toxicological aspects in a multiple chemical sensitivity cohort. Oxid. Med. Cell Longev. 2013, 2013, 356235. [Google Scholar] [CrossRef] [Green Version]
- Gibson, P.R.; Lindberg, A. Physicians’ perceptions and practices regarding patient reports of multiple chemical sensitivity. ISRN Nurs. 2011, 2011, 838930. [Google Scholar] [CrossRef] [Green Version]
- Wiesmuller, G.A.; Hornberg, C. [Environmental medical syndromes]. Bundesgesundheitsblatt Gesundh. Gesundh. 2017, 60, 597–604. [Google Scholar]
- Pall, M.L. Elevated nitric oxide/peroxynitrite theory of multiple chemical sensitivity: Central role of N-methyl-D-aspartate receptors in the sensitivity mechanism. Environ. Health Perspect. 2003, 111, 1461–1464. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, A.; Thrasher, J.D.; Madison, R.A.; Gray, M.R.; Heuser, G.; Campbell, A.W. Antibodies to molds and satratoxin in individuals exposed in water-damaged buildings. Arch. Environ. Health 2004, 58, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Rea, W.J. A Large Case-series of Successful Treatment of Patients Exposed to Mold and Mycotoxin. Clin. Ther. 2018, 40, 889–893. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, A.; Rea, W.; Curtis, L. Adverse health effects of indoor mold exposure. J. Allergy Clin. Immunol. 2006, 118, 763. [Google Scholar] [CrossRef]
- Hyvönen, S.; Poussa, T.; Lohi, J.; Tuuminen, T. High prevalence of neurological sequelae and multiple chemical sensitivity among occupants of a Finnish police station damaged by dampness microbiota. Arch. Environ. Occup. Health 2021, 76, 145–151. [Google Scholar] [CrossRef]
- Hyvönen, S.; Lohi, J.; Tuuminen, T. Moist and Mold Exposure is Associated with High Prevalence of Neurological Symptoms and MCS in a Finnish Hospital Workers Cohort. Saf. Health Work 2020, 11, 173–177. [Google Scholar] [CrossRef]
- Meggs, W.J. The Role of Neurogenic Inflammation in Chemical Sensitivity. Ecopsychology 2017, 9, 83–89. [Google Scholar] [CrossRef]
- Miller, C.S.; Mitzel, H.C. Chemical sensitivity attributed to pesticide exposure versus remodeling. Arch. Environ. Health 1995, 50, 119–129. [Google Scholar] [CrossRef]
- Stejskal, V.D.; Danersund, A.; Lindvall, A.; Hudecek, R.; Nordman, V.; Yaqob, A.; Mayer, W.; Bieger, W.; Lindh, U. Metal-specific lymphocytes: Biomarkers of sensitivity in man. NeuroEndocrinol. Lett. 1999, 20, 289–298. [Google Scholar] [PubMed]
- Sterzl, I.; Prochazkova, J.; Hrda, P.; Bartova, J.; Matucha, P.; Stejskal, V.D.M. Mercury and nickel allergy: Risk factors in fatigue and autoimmunity. NeuroEndocrinol. Lett. 1999, 20, 221–228. [Google Scholar] [PubMed]
- Watai, K.; Fukutomi, Y.; Hayashi, H.; Kamide, Y.; Sekiya, K.; Taniguchi, M. Epidemiological association between multiple chemical sensitivity and birth by caesarean section: A nationwide case-control study. Environ. Health 2018, 17, 89. [Google Scholar] [CrossRef] [Green Version]
- Rainville, P.; Bushnell, M.C.; Duncan, G.H. Representation of acute and persistent pain in the human CNS: Potential implications for chemical intolerance. Ann. N.Y. Acad. Sci. 2001, 933, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Bell, I.R.; Miller, C.S.; Schwartz, G.E. An olfactory-limbic model of multiple chemical sensitivity syndrome: Possible relationships to kindling and affective spectrum disorders. Biol. Psychiatry 1992, 32, 218–242. [Google Scholar] [CrossRef]
- Bell, I.R.; Schwartz, G.E.; Peterson, J.M.; Amend, D. Self-reported illness from chemical odors in young adults without clinical syndromes or occupational exposures. Arch. Environ. Health 1993, 48, 6–13. [Google Scholar] [CrossRef]
- Bell, I.R.; Schwartz, G.E.; Peterson, J.M.; Amend, D.; Stini, W.A. Possible time-dependent sensitization to xenobiotics: Self-reported illness from chemical odors, foods, and opiate drugs in an older adult population. Arch. Environ. Health 1993, 48, 315–327. [Google Scholar] [CrossRef]
- Albright, J.F.; Goldstein, R.A. Is there evidence of an immunologic basis for multiple chemical sensitivity? Toxicol. Ind. Health 1992, 8, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Broughton, A.; Thrasher, J.D.; Gard, Z. Immunological evaluation of four arc welders exposed to fumes from ignited polyurethane (isocyanate) foam: Antibodies and immune profiles. Am. J. Ind. Med. 1988, 13, 463–472. [Google Scholar] [CrossRef]
- Levin, A.S.; Byers, V.S. Multiple chemical sensitivities: A practicing clinician’s point of view. Clinical and immunologic research findings. Toxicol. Ind. Health 1992, 8, 95–109. [Google Scholar] [CrossRef]
- Ziem, G.E.; Davidoff, L.L. Illness from chemical "odors": Is the health significance understood? Arch Environ. Health 1992, 47, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Galland, L. Biochemical abnormalities in patients with multiple chemical sensitivities. Occup. Med. 1987, 2, 713–720. [Google Scholar] [PubMed]
- Johnson, A.; Rea, W.J. Review of 200 cases in the environmental control unit. In Proceedings of the 7th International Symposium on Man and His Environment in Health and Disease, Dallas, TX, USA, 23–26 February 1989. [Google Scholar]
- Levine, S.A.; Reinhardt, J.H. Biochemical-pathology initiated by free radicals, oxidant chemicals, and therapeutic drugs in the etiology of chemical hypersensitivity disease. Orthomol. Psych. 1983, 12, 166–183. [Google Scholar]
- De Luca, C.; Scordo, M.G.; Cesareo, E.; Pastore, S.; Mariani, S.; Maiani, G.; Stancato, A.; Loreti, B.; Valacchi, G.; Lubrano, C.; et al. Biological definition of multiple chemical sensitivity from redox state and cytokine profiling and not from polymorphisms of xenobiotic-metabolizing enzymes. Toxicol. Appl. Pharmacol. 2010, 248, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Mazzatenta, A.; Di Giulio, C.; Pokorski, M. Pathologies currently identified by exhaled biomarkers. Respir. Physiol. Neurobiol. 2013, 187, 128–134. [Google Scholar] [CrossRef]
- Mazzatenta, A.; Pokorski, M.; Cozzutto, S.; Barbieri, P.; Veratti, V.; Di Giulio, C. Non-invasive assessment of exhaled breath pattern in patients with multiple chemical sensibility disorder. Adv. Exp. Med. Biol. 2013, 756, 179–188. [Google Scholar] [PubMed]
- Fisherman, E.W.; Cohen, G. Chemical intolerance to butylated-hydroxyanisole (BHA) and butylated-hydroxytoluene (BHT) and vascular response as an indicator and monitor of drug intolerance. Ann. Allergy. 1973, 31, 126–133. [Google Scholar]
- Black, D.W. The relationship of mental disorders and idiopathic environmental intolerance. Occup. Med. 2000, 15, 557–570. [Google Scholar]
- Staudenmayer, H.; Binkley, K.E.; Leznoff, A.; Phillips, S. Idiopathic environmental intolerance: Part 1: A causation analysis applying Bradford Hill’s criteria to the toxicogenic theory. Toxicol. Rev. 2004, 22, 235–246. [Google Scholar] [CrossRef]
- Miller, C.S.; Prihoda, T.J. The environmental exposure and sensitivity inventory (EESI): A standardized approach for measuring chemical intolerances for research and clinical applications. Toxicol. Ind. Health 1999, 15, 370–385. [Google Scholar] [CrossRef]
- Hojo, S.; Kumano, H.; Yoshino, H.; Kakuta, K.; Ishikawa, S. Application of Quick Environment Exposure Sensitivity Inventory (QEESI) for Japanese population: Study of reliability and validity of the questionnaire. Toxicol. Ind. Health 2003, 19, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Eis, D.; Helm, D.; Mühlinghaus, T.; Birkner, N.; Dietel, A.; Eikmann, T.; Gieler, U.; Herr, C.; Lacour, M.; Nowak, D.; et al. The German Multicentre study on multiple chemical sensitivity (MCS). Int. J. Hyg. Environ. Health 2008, 211, 658–681. [Google Scholar] [CrossRef]
- Andersson, L.; Johansson, A.; Millqvist, E.; Nordin, S.; Bende, M. Prevalence and risk factors for chemical sensitivity and sensory hyperreactivity in teenagers. Int. J. Hyg. Environ. Health 2008, 211, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Österberg, K.; Persson, R.; Karlson, B.; Carlsson Eek, F.; Orbaek, P. Personality, mental distress, and subjective health complaints among persons with environmental annoyance. Hum. Exp. Toxicol. 2007, 26, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Palmer, R.F.; Jaén, C.R.; Perales, R.B.; Rincon, R.; Forster, J.N.; Miller, C.S. Three questions for identifying chemically intolerant individuals in clinical and epidemiological populations: The Brief Environmental Exposure and Sensitivity Inventory (BREESI). PLoS ONE 2020, 15, e0238296. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.S.; Prihoda, T.J. A controlled comparison of symptoms and chemical intolerances reported by Gulf War veterans, implant recipients and persons with multiple chemical sensitivity. Toxicol. Ind. Health 1999, 15, 386–397. [Google Scholar] [CrossRef]
- Stölzel, U.; Doss, M.O.; Schuppan, D. Clinical Guide and Update on Porphyrias. Gastroenterology 2019, 157, 365–381.e4. [Google Scholar] [CrossRef] [Green Version]
- Pardanani, A. Systemic mastocytosis in adults: 2019 update on diagnosis, risk stratification and management. Am. J. Hematol. 2019, 94, 363–377. [Google Scholar] [CrossRef] [Green Version]
- Pigatto, P.D.; Guzzi, G. Contact allergy to metals and multiple chemical sensitivity. Contact Dermat. 2019, 81, 79. [Google Scholar] [CrossRef]
- Pigatto, P.D.; Rossi, V.; Guzzi, G. Dietary factors and endocrine consequences of multiple chemical sensitivity. Endocrinol. Diabetes Nutr. 2020, 67, 353–354. [Google Scholar] [CrossRef]
- Viziano, A.; Micarelli, A.; Pasquantonio, G.; Della-Morte, D.; Alessandrini, M. Perspectives on multisensory perception disruption in idiopathic environmental intolerance: A systematic review. Int. Arch. Occup. Environ. Health 2018, 91, 923–935. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, M.; Micarelli, A.; Chiaravalloti, A.; Bruno, E.; Danieli, R.; Pierantozzi, M.; Genovesi, G.; Öberg, J.; Pagani, M.; Schillaci, O. Involvement of Subcortical Brain Structures During Olfactory Stimulation in Multiple Chemical Sensitivity. Brain Topogr. 2016, 29, 243–252. [Google Scholar] [CrossRef] [Green Version]
- Chiaravalloti, A.; Pagani, M.; Micarelli, A.; Di Pietro, B.; Genovesi, G.; Alessandrini, M.; Schillaci, O. Cortical activity during olfactory stimulation in multiple chemical sensitivity: A (18)F-FDG PET/CT study. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 733–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alessandrini, M.; Micarelli, A.; Bruno, E.; Ottaviani, F.; Conetta, M.; Cormano, A.; Genovesi, G. Intranasal administration of hyaluronan as a further resource in olfactory performance in multiple chemical sensitivity syndrome. Int. J. Immunopathol. Pharmacol. 2013, 26, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, M.; Micarelli, A.; Chiaravalloti, A.; Candidi, M.; Bruno, E.; Di Pietro, B.; Schillaci, O.; Pagani, M. Cortico-subcortical metabolic correlates of olfactory processing in healthy resting subjects. Sci. Rep. 2014, 4, 5146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micarelli, A.; Viziano, A.; Bruno, E.; Micarelli, E.; Alessandrini, M. Vestibular impairment in Multiple Chemical Sensitivity: Component analysis findings. J. Vestib. Res. 2016, 26, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Micarelli, A.; Viziano, A.; Genovesi, G.; Bruno, E.; Ottaviani, F.; Alessandrini, M. Lack of contralateral suppression in transient-evoked otoacoustic emissions in multiple chemical sensitivity: A clinical correlation study. Noise Health 2016, 18, 143–149. [Google Scholar]
- Guzzi, G.; Grandi, M.; Guzzi, G.; Cattaneo, C.; Calza, S.; Minoia, C.; Ronchi, A.; Gatti, A.; Severi, G. Dental amalgam and mercury levels in autopsy tissues: Food for thought. Am. J. Forensic Med. Pathol. 2006, 27, 42–45. [Google Scholar]
- Daunderer, M. Handbuch der Amalgam-Vergiftung; Ecomed: Landsberg/Lech, Germany, 1992. [Google Scholar]
- Pigatto, P.D.; Ferrucci, S.; Brambilla, L. Toxic metals screening in MCS patients. In Proceedings of the 16th Euro-Global Summit on Toxicology and Applied Pharmacology, Valencia, Spain, 4–5 July 2019. [Google Scholar]
- Guzzi, G.; Pigatto, P.D.; Legori, A.; Ferrucci, S.; Brambilla, L. Multiple sensitization to metals in MCS. Contact Dermat. 2018, 79 (Suppl. 1), 79. [Google Scholar]
- Guzzi, G.; Ronchi, A.; Barbaro, M.; Spadari, F.; Bombeccari, G.; Brambilla, L.; Ferrucci, S.; Pigatto, P.D. Multiple chemical sensitivity and toxic metals. Toxicol. Lett. 2016, 258, s113. [Google Scholar] [CrossRef]
- Guzzi, G.; Pigatto, P.D.; Ronchi, A.; Dolcetta, D.; Brambilla, L.; Ferrucci, S.; Passoni, M. Exposure to metals, multiple chemical sensitivity, and neurogenic inflammation. J. Clin. Toxicol. 2018, 8, 1. [Google Scholar]
- Pigatto, P.; Arancio, L.; Guzzi, G.; Severi, G. Metals from amalgam in saliva: Association with lichenoid lesions, leukoplakia, burning mouth syndrome. Toxicol. Lett. 2005, 158S, 169. [Google Scholar]
- Pigatto, P.D.; Minoia, C.; Ronchi, A.; Guzzi, G. Mercury in saliva: Immunotoxic and allergenic metal. All. Asthma. Proc. 2009, 64 (Suppl. 90), 537. [Google Scholar]
- Shirakawa, S.R.; Ishikawa, S.; Johnson, A.R. Evaluation of the autonomic nervous system response by pupillographical study in the chemically sensitive patient. Environ. Med. 1991, 8, 121–127. [Google Scholar]
- Weiss, B. Experimental strategies for research on multiple chemical sensitivity. Environ. Health Perspect. 1997, 105 (Suppl. 2), 487–494. [Google Scholar]
- Kilburn, K.H. Chemical Brain Injury (Environmental Health); Van Nostrand Reinhold: New York, NY, USA, 1998. [Google Scholar]
- Anger, W.K.; Letz, R.; Chrislip, D.W.; Frumkin, H.; Hudnell, K.; Russo, J.M.; Chappell, W.; Hutchinson, L. Neurobehavioral test methods for environmental health studies of adults. Neurotoxicol. Teratol. 1994, 16, 489–497. [Google Scholar] [CrossRef]
- Hudnell, H.K.; Benignus, V.A. Carbon monoxide exposure and human visual detection thresholds. Neurotoxicol. Teratol. 1989, 11, 363–371. [Google Scholar] [CrossRef]
- Hudnell, H.K.; Boyes, W.K.; Otto, D.A.; Frumkin, H.; Hudnell, K.; Russo, J.M.; Chappell, W.; Hutchinson, L. Battery of neurobehavioral tests recommended to ATSDR: Solvent-induced deficits in microelectronic workers. Toxicol. Ind. Health. 1996, 12, 235–243. [Google Scholar] [CrossRef]
- Hudnell, H.K.; Otto, D.A.; House, D.E. The influence of vision on computerized neurobehavioral test scores: A proposal for improving test protocols. Neurotoxicol. Teratol. 1996, 18, 391–400. [Google Scholar] [CrossRef]
- Seppalainen, A.M.; Raitta, C.; Huuskonen, M.S. n-Hexane-induced changes in visual evoked potentials and electroretinograms of industrial workers. Electroencephalogr. Clin. Neurophysiol. 1979, 47, 492–498. [Google Scholar] [CrossRef]
- Callender, T.J.; Morrow, L.; Subramanian, K. Evaluation of chronic neurological sequelae after acute pesticide exposure using SPECT brain scans. J. Toxicol. Environ. Health 1994, 41, 275–284. [Google Scholar] [CrossRef]
- Callender, T.J.; Morrow, L.; Subramanian, K.; Duhon, D.; Ristovv, M. Three-dimensional brain metabolic imaging in patients with toxic encephalopathy. Environ. Res. 1993, 60, 295–319. [Google Scholar] [CrossRef] [PubMed]
- Heuser, G.; Mena, I.; Alamos, F. NeuroSPECT findings in patients exposed to neurotoxic chemicals. Toxicol. Ind. Health 1994, 10, 561–571. [Google Scholar] [CrossRef]
- Hillert, L.; Musabasic, V.; Berglund, H.; Ciumas, C.; Savic, I. Odor processing in multiple chemical sensitivity. Hum. Brain Mapp. 2006, 28, 172–182. [Google Scholar] [CrossRef]
- Belpomme, D.; Campagnac, C.; Irigaray, P. Reliable disease biomarkers characterizing and identifying electrohypersensitivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev. Environ. Health 2015, 30, 251–271. [Google Scholar] [CrossRef] [PubMed]
- Guzzi, G.; Ronchi, A.; Bolengo, I.; Pontillo, M.; Soldini, L.; Soldarini, A.; Pigatto, P.D. NSE: Marker of the Clinical Toxicity of Mercury. Toxicol. Lett. 2015, 238 (Suppl. 2), S162. [Google Scholar] [CrossRef]
- Pigatto, P.; Ronchi, A.; Guzzi, G. NSE as a biomarker of mercury exposure. Clin. Toxicol. 2014, 52, 444. [Google Scholar] [CrossRef] [Green Version]
- Wade, M.G.; Parent, S.; Finnson, K.W.; Foster, W.; Younglai, E.; McMahon, A.; Cyr, D.G.; Hughes, C. Thyroid toxicity due to subchronic exposure to a complex mixture of 16 organochlorines, lead, and cadmium. Toxicol. Sci. 2002, 67, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Baines, C.J.; McKeown-Eyssen, G.E.; Riley, N.; Cole, D.E.; Marshall, L.; Loescher, B.; Jazmaji, V. Case-control study of multiple chemical sensitivity, comparing haematology, biochemistry, vitamins and serum volatile organic compound measures. Occup. Med. 2004, 5, 408–418. [Google Scholar] [CrossRef] [Green Version]
- Bell, I.R.; Bootzin, R.R.; Davis, T.P.; Hau, V.; Ritenbaugh, C.; Johnson, K.A.; Schwartz, G.E. Time-dependent sensitization of plasma beta-endorphin in community elderly with self-reported environmental chemical odor intolerance. Biol. Psychiatry 1996, 40, 134–143. [Google Scholar] [CrossRef]
- Haumann, K.; Kiesswetter, E.; van Thriel, C.; Blaszkewicz, M.; Golka, K.; Seeber, A. Breathing and heart rate during experimental solvent exposure of young adults with self-reported multiple chemical sensitivity (sMCS). Neurotoxicology 2003, 24, 179–186. [Google Scholar] [CrossRef]
- Ziem, G.; McTamney, J. Profile of patients with chemical injury and sensitivity. Environ. Health Perspect. 1997, 105 (Suppl. 2), 417–436. [Google Scholar] [PubMed]
- Bell, I.R.; Schwartz, G.E.; Hardin, E.E.; Baldwin, C.M.; Kline, J.P. Differential resting quantitative electroencephalographic alpha patterns in women with environmental chemical intolerance, depressives, and normals. Biol. Psychiatry 1998, 43, 376–388. [Google Scholar] [CrossRef]
- Baldwin, C.M.; Bell, I.R. Increased cardiopulmonary disease risk in a community-based sample with chemical odor intolerance: Implications for women’s health and health-care utilization. Arch. Environ. Health 1998, 53, 347–353. [Google Scholar] [CrossRef]
- Rea, W.J. Environmentally triggered thrombophlebitis. Ann. Allergy 1976, 37, 101–109. [Google Scholar]
- Rea, W.J. Environmentally triggered small vessel vasculitis. Ann. Allergy 1977, 38, 245–251. [Google Scholar]
- Slotkoff, A.T.; Radulovic, D.A.; Clauw, D.J. The relationship between fibromyalgia and the multiple chemical sensitivity syndrome. Scand. J. Rheumatol. 1997, 2, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Migliore, A.; Bizzi, E.; Massafra, U.; Capuano, A.; Martin Martin, L.S. Multiple chemical sensitivity syndrome in Sjogren’s syndrome patients: Casual association or related diseases? Arch. Environ. Occup. Health 2007, 61, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.R.; Elms, A.N.; Ruding, L.A. Perceived treatment efficacy for conventional and alternative therapies reported by persons with multiple chemical sensitivity. Environ Health Perspect. 2003, 111, 1498–1504. [Google Scholar] [CrossRef] [Green Version]
- Skovbjerg, S.; Brorson, S.; Rasmussen, A.; Johansen, J.D.; Elberling, J. Impact of self-reported multiple chemical sensitivity on everyday life: A qualitative study. Scand. J. Public Health 2009, 37, 621–626. [Google Scholar] [CrossRef] [PubMed]
- Piroli, A.; Ciccozzi, A.; Petrucci, E.; Paladini, A.; Marsili, I.; Panella, L.; Santucci, C.; Coaccioli, S.; Marinangeli, F. Anaesthesia management in patients with multiple chemical sensitivity syndrome. Int. J. Immunopathol. Pharmacol. 2013, 26, 961–964. [Google Scholar] [CrossRef] [Green Version]
- Fisher, M.M.; Rose, M. Anaesthesia for patients with idiopathic environmental intolerance and chronic fatigue syndrome. Br. J. Anaesth. 2008, 101, 486–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKeown-Eyssen, G.; Baines, C.; Cole, D.E.; Riley, N.; Tyndale, R.F.; Marshall, L.; Jazmaji, V. Case-control study of genotypes in multiple chemical sensitivity: CYP2D6, NAT1, NAT2, PON1, PON2 and MTHFR. Int. J. Epidemiol. 2004, 33, 971–978. [Google Scholar] [CrossRef]
- Berg, N.D.; Rasmussen, H.B.; Linneberg, A.; Brasch-Andersen, C.; Fenger, M.; Dirksen, A.; Vesterhauge, S.; Werge, T.; Elberling, J. Genetic susceptibility factors for multiple chemical sensitivity revisited. Int. J. Hyg. Environ. Health 2010, 213, 131–139. [Google Scholar] [CrossRef]
- Fujimori, S.; Hiura, M.; Yi, C.X.; Xi, L.; Katoh, T. Factors in genetic susceptibility in a chemical sensitive population using QEESI. Environ. Health Prev. Med. 2012, 17, 357–363. [Google Scholar] [CrossRef] [Green Version]
- Cui, X.; Lu, X.; Hiura, M.; Oda, M.; Miyazaki, W.; Katoh, T. Evaluation of genetic polymorphisms in patients with multiple chemical sensitivity. PLoS ONE 2013, 8, e73708. [Google Scholar] [CrossRef] [Green Version]
- Caccamo, D.; Cesareo, E.; Mariani, S.; Raskovic, D.; Ientile, R.; Currò, M.; Korkina, L.; De Luca, C. Xenobiotic sensor- and metabolism-related gene variants in environmental sensitivity-related illnesses: A survey on the Italian population. Oxid. Med. Cell Longev. 2013, 2013, 831969. [Google Scholar] [CrossRef]
- Micarelli, A.; Cormano, A.; Caccamo, D.; Alessandrini, M. Olfactory-Related Quality of Life in Multiple Chemical Sensitivity: A Genetic-Acquired Factors Model. Int. J. Mol. Sci. 2019, 21, 156. [Google Scholar] [CrossRef] [Green Version]
- De Luca, C.; Gugliandolo, A.; Calabrò, C.; Currò, M.; Ientile, R.; Raskovic, D.; Korkina, L.; Caccamo, D. Role of polymorphisms of inducible nitric oxide synthase and endothelial nitric oxide synthase in idiopathic environmental intolerances. Mediat. Inflamm. 2015, 2015, 245308. [Google Scholar] [CrossRef]
- Gugliandolo, A.; Gangemi, C.; Calabrò, C.; Vecchio, M.; Di Mauro, D.; Renis, M.; Ientile, R.; Currò, M.; Caccamo, D. Assessment of glutathione peroxidase-1 polymorphisms, oxidative stress and DNA damage in sensitivity-related illnesses. Life Sci. 2016, 145, 27–33. [Google Scholar] [CrossRef]
- Dantoft, T.M.; Skovbjerg, S.; Andersson, L.; Claeson, A.S.; Engkilde, K.; Lind, N.; Nordin, S.; Hellgren, L.I. Gene expression profiling in persons with multiple chemical sensitivity before and after a controlled n-butanol exposure session. BMJ Open. 2017, 7, e013879. [Google Scholar] [CrossRef]
- Cannata, A.; De Luca, C.; Korkina, L.G.; Ferlazzo, N.; Ientile, R.; Currò, M.; Andolina, G.; Caccamo, D. The SNP rs2298383 reduces ADORA2A gene transcription and positively associates with cytokine production by peripheral blood mononuclear cells in patients with Multiple Chemical Sensitivity. Int. J. Mol. Sci. 2020, 21, 1858. [Google Scholar] [CrossRef] [Green Version]
- Ross, G.H. Treatment options in multiple chemical sensitivity. Toxicol. Ind. Health 1992, 8, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Driesen, L.; Patton, R.; John, M. The impact of multiple chemical sensitivity on people’s social and occupational functioning; a systematic review of qualitative research studies. J. Psychosom. Res. 2020, 132, 109964. [Google Scholar] [CrossRef]
- Damiani, G.; Gironi, L.; Pacifico, A.; Cristaudo, A.; Malagoli, P.; Allocco, F.; Bragazzi, N.L.; Linder, D.M.; Santus, P.; Buja, A.; et al. Masks use and facial dermatitis during COVID-19 outbreak: Is there a difference between CE and non-CE approved masks? G Ital. Dermatol. Venereol. 2021, 156, 220–225. [Google Scholar]
- Damiani, G.; Gironi, L.C.; Grada, A.; Kridin, K.; Finelli, R.; Buja, A.; Bragazzi, N.L.; Pigatto, P.D.M.; Savoia, P. COVID-19 related masks increase severity of both acne (maskne) and rosacea (mask rosacea): Multi-center, real-life, telemedical, and observational prospective study. Dermatol. Ther. 2021, 34, e14848. [Google Scholar] [CrossRef]
- Damiani, G.; Gironi, L.C.; Kridin, K.; Pacifico, A.; Buja, A.; Bragazzi, N.L.; Spalkowska, M.; Pigatto, P.D.M.; Santus, P.; Young Dermatologists Italian Network; et al. Mask-induced Koebner phenomenon and its clinical phenotypes: A multicenter, real-life study focusing on 873 dermatological consultations during COVID-19 pandemics. Dermatol. Ther. 2021, 34, e14823. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathogenetic Hypotheses | Clinical Manifestations * | Screening Questionnaires | Subjects at Risk | Triggers * |
|---|---|---|---|---|
| Limbic dysfunction [34,35,36,37] | Neurological disorders [1,12,13,14,15,16,17]: headache, migraine, trigeminal neuralgia, convulsions, attention deficit disorder, neurocognitive deficits, hyperacusis, insomnia, myalgic encephalomyelitis | Environmental Exposure and Sensitivity Intolerance (EESI) [49] | Industrial workers acutely or chronically exposed to recognized triggers [30] | Organic solvents and related compounds [23] |
| Immune disorders [36,37,38] | ORL disorders [1]: sinusitis, polyps, non-allergic rhinitis with eosinophilic syndrome, tinnitus, recurrent otitis, allergic rhinitis | Quick Environmental Exposure and Sensitivity Inventory (QEESI) [50] | Other workers exposed to recognized triggers (farmers, hairdressers, radiologists, anesthesiologists) [30] | Insecticides, pesticides, herbicides [23] |
| Biochemical mechanisms [40,41,42,43] | Cardiovascular disorders [1]: arrhythmia, tachycardia, hypotension, hypertension, Raynaud’s phenomenon, lipothymia | Huppe Questionnaire [51] | Office workers [30] | Different gases (i.e., hydrogen sulfide (H2S) or carbon monoxide (CO) [23] |
| Neurogenic inflammation [39] | Respiratory disorders [1]: asthma, tracheitis, bronchospasms, chronic tonsillitis, hyper-reactive airway syndrome, toluene diisocyanate hypersensitivity | Chemical Sensitivity Scale for Sensory Hyper-Reactivity (CSS-SHR) [52] | Residents in contaminated areas [30] | Metals (i.e., mercury) [23,30] |
| Neurophysiological and respiratory mechanisms [44,45] | Gastroenterological disorders [1]: irritable colon, colitis, gastroesophageal reflux (GERD), celiac disease, gluten sensitivity, food intolerances, food allergies | German Questionnaire on Chemical and Environmental Sensitivity (CGES) [53] | Gulf War veterans [30] | Molds and mycotoxins [24,25,26,27,28] |
| Vascular dysfunction [46] | Rheumatological disorders: fibromyalgia, carpal tunnel syndrome, dysfunction of the temporomandibular joint (TMJ), arthritis, connective tissue disease, systemic lupus erythematosus (SLE) [1] | Brief Environmental Exposure and Sensitivity Inventory (BREESI) [54] | Silicon or prosthesis implants carriers [10,31] | Xenobiotics in foods and beverages (i.e., sulfites) [29] |
| Psychiatric disorders [47,48] | Dermatological/allergic disorders [1]: eczema, systemic dermatitis, rash, urticaria/angioedema, photosensitivity, skin photosensitivity, dermographism | Patients born by Caesarean section [33] | Combusted products (diesel exhaust, tobacco, wood) [29] | |
| N-Methyl-D-aspartic acid or N-Methyl-D-aspartate (NMDA) sensitization and stimulation by reactive oxygen species and peroxynitrite [21] | Endocrinological disorders [1,18]: diabetes, dysthyroidism, adrenal gland disorders, pituitary disorders | Other substances (natural psoralens, terpenes) [29] | ||
| Psychological/psychiatric disorders: anxiety, depression, manic depression, bipolar disorder, mood swings, panic attacks | ||||
| Others [19,20]: Chronic Fatigue Syndrome, Gulf War Syndrome, Sick Building Syndrome |
| Demographics and Characteristics | Pre-Delphi Exercise (N = 7) | Delphi Rounds (N = 12) |
|---|---|---|
| Dermatologists, N (%) | 1 (14.3) | 1 (8.3) |
| Dentists, N (%) | 1 (14.3) | 2 (16.6) |
| Otorhinolaryngologist, N (%) | 1 (14.3) | 1 (8.3) |
| Anesthesiologists, N (%) | - | 1 (8.3) |
| Allergists/Allergologists, N (%) | 1 (14.3) | 1 (8.3) |
| Rheumatologists | - | 1 (8.3) |
| Alternative Medicine Doctors | - | 1 (8.3) |
| Biologists, N (%) | 2 (28.6) | 2 (16.6) |
| Representatives of Patients, N (%) | 1 (14.3) | 1 (8.3) |
| Male, N (%) | 5 (71.4) | 9 (75.0) |
| Age, Median (IQR), Years | 52 (50–57.5) | 55 (47–59) |
| Clinical/Research Experience, Median (IQR), Years | 25.5 (21.3–27.5) | 26 (15.5–34.5) |
| Academic Experience, N (%) * | 5 (71.4) | 5 (41.7) |
| Hospital or Private Practice Experience, N (%) | 4 (57.1) | 9 (75.0) |
| Both, N (%) | 6 (85.7) | 11 (91.7) |
| Screening and Diagnosis (Level 0) | 1st Level Assessments | 2nd Level Assessments |
|---|---|---|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damiani, G.; Alessandrini, M.; Caccamo, D.; Cormano, A.; Guzzi, G.; Mazzatenta, A.; Micarelli, A.; Migliore, A.; Piroli, A.; Bianca, M.; et al. Italian Expert Consensus on Clinical and Therapeutic Management of Multiple Chemical Sensitivity (MCS). Int. J. Environ. Res. Public Health 2021, 18, 11294. https://doi.org/10.3390/ijerph182111294
Damiani G, Alessandrini M, Caccamo D, Cormano A, Guzzi G, Mazzatenta A, Micarelli A, Migliore A, Piroli A, Bianca M, et al. Italian Expert Consensus on Clinical and Therapeutic Management of Multiple Chemical Sensitivity (MCS). International Journal of Environmental Research and Public Health. 2021; 18(21):11294. https://doi.org/10.3390/ijerph182111294
Chicago/Turabian StyleDamiani, Giovanni, Marco Alessandrini, Daniela Caccamo, Andrea Cormano, Gianpaolo Guzzi, Andrea Mazzatenta, Alessandro Micarelli, Alberto Migliore, Alba Piroli, Margherita Bianca, and et al. 2021. "Italian Expert Consensus on Clinical and Therapeutic Management of Multiple Chemical Sensitivity (MCS)" International Journal of Environmental Research and Public Health 18, no. 21: 11294. https://doi.org/10.3390/ijerph182111294
APA StyleDamiani, G., Alessandrini, M., Caccamo, D., Cormano, A., Guzzi, G., Mazzatenta, A., Micarelli, A., Migliore, A., Piroli, A., Bianca, M., Tapparo, O., & Pigatto, P. D. M. (2021). Italian Expert Consensus on Clinical and Therapeutic Management of Multiple Chemical Sensitivity (MCS). International Journal of Environmental Research and Public Health, 18(21), 11294. https://doi.org/10.3390/ijerph182111294