
Cross-Sectional and Longitudinal Association between Neighborhood Environment and Perceived Control in Older Adults: Findings from HRS


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Frame
2.2. Measurement
2.3. Analysis
3. Results
3.1. Descriptive Statistics and Correlation Test
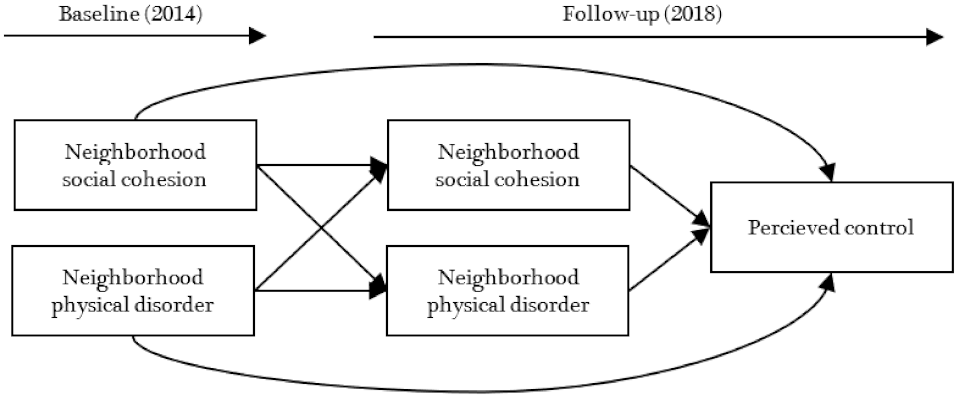
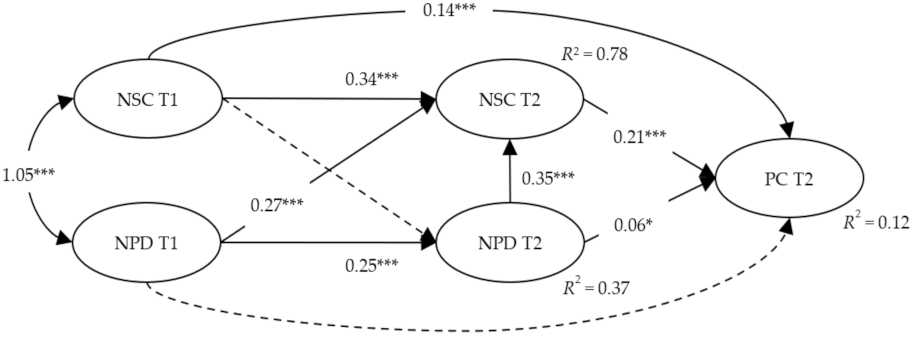
3.2. Structural Model Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| % | ||
| Gender | Female | 59.1 |
| Age | Mean = 71.74 years, SD = 7.76 | |
| Education | No degree | 18.1 |
| General Educational Development (GED) | 4.5 | |
| High school diploma | 47.3 | |
| Two-year college degree | 4.9 | |
| Four-year college degree | 13.6 | |
| Master’s degree | 8.1 | |
| Professional degree | 2.6 | |
| Race/ethnicity | White/Caucasian | 75.4 |
| Black/African American | 17.7 | |
| Other (American Indian, Alaskan Native, Asian, Native Hawaiian, and Pacific Islander) | 6.9 | |
| Hispanicity type | Hispanic, Mexican | 7.6 |
| Hispanic, other | 4.9 | |
| Hispanic, type unknown | 0.2 | |
| Non-Hispanic | 87.2 | |
| Marital status | Married | 57.9 |
| Separated/divorced | 15.7 | |
| Widowed | 23.0 | |
| Never married | 3.3 | |
| Living arrangement | Married/partnered, | |
| living with partner | 61.0 | |
| not living with spouse/partner | 2.5 | |
| Not married/partnered, | ||
| living with another unrelated adult | 1.1 | |
| living with relative (e.g., children) | 11.2 | |
| living alone | 24.0 |
Appendix B
| Construct | Items |
|---|---|
| neighborhood environment—Physical disorder | There are no vacant or deserted houses or storefronts in this area. |
| There is no problem with vandalism and graffiti in this area. | |
| This area is kept very clean. | |
| People feel safe walking alone in this area after dark. | |
| neighborhood environment—Social cohesion | I really feel part of this area. |
| Most people in this are friendly. | |
| Most people in this area can be trusted. | |
| If you were in trouble, there are lots of people in this area who would help you. | |
| Perceived control | I often feel helpless in dealing with the problems of life. |
| Other people determine most of what I can and cannot do. | |
| What happens in my life is often beyond my control. | |
| I have little control over the things that happen to me. | |
| There is really no way I can solve the problems I have. |
References
- Choi, Y.J.; Matz-Costa, C. Perceived neighborhood safety, social cohesion, and psychological health of older adults. Gerontologist 2018, 58, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Cramm, J.M.; Van Dijk, H.M.; Nieboer, A.P. The importance of neighborhood social cohesion and social capital for the well being of older adults in the community. Gerontologist 2013, 53, 142–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonyea, J.G.; Burnes, K. Aging well at home: Evaluation of a neighborhood-based pilot project to “put connection back into community”. J. Hous. Elder. 2013, 27, 333–347. [Google Scholar] [CrossRef]
- Lee, S. Perceived neighborhood environment associated with older adults’ walking and positive affect: Results from the health and retirement study. J. Aging Phys. Act. 2020, 29, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Schorr, A.V.; Khalaila, R. Aging in place and quality of life among the elderly in Europe: A moderated mediation model. Arch. Gerontol. Geriatr. 2018, 77, 196–204. [Google Scholar] [CrossRef]
- Won, J.; Lee, C.; Forjuoh, S.N.; Ory, M.G. Neighborhood safety factors associated with older adults’ health-related outcomes: A systematic literature review. Soc. Sci. Med. 2016, 165, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Baranyi, G.; Sieber, S.; Cullati, S.; Pearce, J.R.; Dibben, C.J.; Courvoisier, D.S. The longitudinal associations of perceived neighborhood disorder and lack of social cohesion with depression among adults aged 50 years or older: An individual-participant-data meta-analysis from 16 high-income countries. Am. J. Epidemiol. 2020, 189, 343–353. [Google Scholar] [CrossRef] [Green Version]
- Kowitt, S.D.; Aiello, A.E.; Callahan, L.F.; Fisher, E.B.; Gottfredson, N.C.; Jordan, J.M.; Muessig, K.E. Associations among neighborhood poverty, perceived neighborhood environment, and depressed mood are mediated by physical activity, perceived individual control, and loneliness. Health Place 2020, 62, 102278. [Google Scholar] [CrossRef]
- Norstrand, J.A.; Glicksman, A.; Lubben, J.; Kleban, M. The role of the social environment on physical and mental health of older adults. J. Hous. Elder. 2012, 26, 290–307. [Google Scholar] [CrossRef]
- Rios, R.; Aiken, L.S.; Zautra, A.J. Neighborhood contexts and the mediating role of neighborhood social cohesion on health and psychological distress among Hispanic and non-Hispanic residents. Ann. Behav. Med. 2012, 43, 50–61. [Google Scholar] [CrossRef]
- Ruiz, M.; Malyutina, S.; Pajak, A.; Kozela, M.; Kubinova, R.; Bobak, M. Congruent relations between perceived neighbourhood social cohesion and depressive symptoms among older European adults: An East-West analysis. Soc. Sci. Med. 2019, 237, 112454. [Google Scholar] [CrossRef]
- Thierry, A.D.; Sherman-Wilkins, K.; Armendariz, M.; Sullivan, A.; Farmer, H.R. Perceived neighborhood characteristics and cognitive functioning among diverse older adults: An intersectional approach. Int. J. Environ. Res. Public Health 2021, 18, 2661. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Cheung, O.; Lau, K.; Woo, J. Associations between perceived neighborhood walkability and walking time, wellbeing, and loneliness in community-dwelling older Chinese people in Hong Kong. Int. J. Environ. Res. Public Health 2017, 14, 1199. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, J.; Zhou, M.; Yu, N.X. Neighborhood characteristics and older adults’ well-being: The roles of sense of community and personal resilience. Soc. Indic. Res. 2018, 137, 949–963. [Google Scholar] [CrossRef]
- Jacelon, C.S. Theoretical perspectives of perceived control in older adults: A selective review of the literature. J. Adv. Nurs. 2007, 59, 1–10. [Google Scholar] [CrossRef]
- Lachman, M.E. Perceived control over aging-related declines: Adaptive beliefs and behaviors. Curr. Dir. Psychol. Sci. 2006, 15, 282–286. [Google Scholar] [CrossRef]
- Lachman, M.E.; Weaver, S.L. The sense of control as a moderator of social class differences in health and well-being. J. Personal. Soc. Psychol. 1998, 74, 763. [Google Scholar] [CrossRef]
- Andrew, N.; Meeks, S. Fulfilled preferences, perceived control, life satisfaction, and loneliness in elderly long-term care residents. Aging Ment. Health 2018, 22, 183–189. [Google Scholar] [CrossRef]
- Boehlen, F.H.; Herzog, W.; Schellberg, D.; Maatouk, I.; Saum, K.U.; Brenner, H.; Wild, B. Self-perceived coping resources of middle-aged and older adults–results of a large population-based study. Aging Ment. Health 2017, 21, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Seetai, S.; Morris, R.; Ebrahim, S. Quality of life among older people with poor functioning. The influence of perceived control over life. Age Ageing 2007, 36, 310–315. [Google Scholar] [CrossRef] [Green Version]
- de Quadros-Wander, S.; McGillivray, J.; Broadbent, J. The influence of perceived control on subjective wellbeing in later life. Soc. Indic. Res. 2014, 115, 999–1010. [Google Scholar] [CrossRef]
- Fry, P.S.; Debats, D.L. Self-efficacy beliefs as predictors of loneliness and psychological distress in older adults. Int. J. Aging Hum. Dev. 2002, 55, 233–269. [Google Scholar] [CrossRef] [PubMed]
- Curtis, R.G.; Windsor, T.D.; Luszcz, M.A. Perceived control moderates the effects of functional limitation on older adults’ social activity: Findings from the Australian longitudinal study of ageing. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2017, 72, 571–581. [Google Scholar] [CrossRef] [Green Version]
- Mooney, C.J.; Elliot, A.J.; Douthit, K.Z.; Marquis, A.; Seplaki, C.L. Perceived control mediates effects of socioeconomic status and chronic stress on physical frailty: Findings from the health and retirement study. J. Gerontol. Ser. B 2018, 73, 1175–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruthig, J.C.; Chipperfield, J.G.; Newall, N.E.; Perry, R.P.; Hall, N.C. Detrimental effects of falling on health and well-being in later life: The mediating roles of perceived control and optimism. J. Health Psychol. 2007, 12, 231–248. [Google Scholar] [CrossRef] [PubMed]
- Turiano, N.A.; Chapman, B.P.; Agrigoroaei, S.; Infurna, F.J.; Lachman, M. Perceived control reduces mortality risk at low, not high, education levels. Health Psychol. 2014, 33, 883. [Google Scholar] [CrossRef] [Green Version]
- Faul, J.D.; Smith, J. Health and Retirement Study: Genetic Data Consortia Collaboration; Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Servais, M.A. An Elementary Cookbook of Data Management Using HRS Data with SPSS, SAS, and Stata Examples; Technical Report; Survey Research Center, Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2009. [Google Scholar]
- Smith, J.; Ryan, L.; Fisher, G.; Sonnega, A.; Weir, D. HRS Psychosocial and Lifestyle Questionnaire 2006–2016: Documentation Report; Survey Research Center, Institute for Social Research, University of Michigan: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Cagney, K.A.; Glass, T.A.; Skarupski, K.A.; Barnes, L.L.; Schwartz, B.S.; Mendes de Leon, C.F. Neighborhood-level cohesion and disorder: Measurement and validation in two older adult urban populations. J. Gerontol. Ser. B 2009, 64, 415–424. [Google Scholar] [CrossRef]
- Mendes de Leon, C.F.; Cagney, K.A.; Bienias, J.L.; Barnes, L.L.; Skarupski, K.A.; Scherr, P.A.; Evans, D.A. Neighborhood social cohesion and disorder in relation to walking in community-dwelling older adults: A multilevel analysis. J. Aging Health 2009, 21, 155–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Bromell, L.; Cagney, K.A. Companionship in the neighborhood context: Older adults’ living arrangements and perceptions of social cohesion. Res. Aging 2014, 36, 228–243. [Google Scholar] [CrossRef] [Green Version]


| Mean (SD) | Cronbach’s a | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|---|
| 1.NPD (T1) | 2.52 (1.43) | 0.841 | - | ||||
| 2.NSC (T1) | 2.59 (1.40) | 0.869 | 0.777 ** | - | |||
| 3.NPD (T2) | 2.40 (1.38) | 0.848 | 0.404 ** | 0.324 ** | - | ||
| 4.NSC (T2) | 2.52 (1.35) | 0.874 | 0.298 ** | 0.403 ** | 0.758 ** | - | |
| 5.PC (T2) | 4.74 (1.12) | 0.860 | 0.143 ** | 0.204 ** | 0.186 ** | 0.239 ** | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S. Cross-Sectional and Longitudinal Association between Neighborhood Environment and Perceived Control in Older Adults: Findings from HRS. Int. J. Environ. Res. Public Health 2021, 18, 11344. https://doi.org/10.3390/ijerph182111344
Lee S. Cross-Sectional and Longitudinal Association between Neighborhood Environment and Perceived Control in Older Adults: Findings from HRS. International Journal of Environmental Research and Public Health. 2021; 18(21):11344. https://doi.org/10.3390/ijerph182111344
Chicago/Turabian StyleLee, Sunwoo. 2021. "Cross-Sectional and Longitudinal Association between Neighborhood Environment and Perceived Control in Older Adults: Findings from HRS" International Journal of Environmental Research and Public Health 18, no. 21: 11344. https://doi.org/10.3390/ijerph182111344
APA StyleLee, S. (2021). Cross-Sectional and Longitudinal Association between Neighborhood Environment and Perceived Control in Older Adults: Findings from HRS. International Journal of Environmental Research and Public Health, 18(21), 11344. https://doi.org/10.3390/ijerph182111344