
Oral Health of Australian Adults: Distribution and Time Trends of Dental Caries, Periodontal Disease and Tooth Loss



Abstract
:1. Introduction
2. Materials & Methods
2.1. Dental Caries (Coronal Caries)
2.2. Periodontal Disease
3. Results
3.1. Dental Caries
3.2. Gingivitis
3.3. Periodontitis
3.4. Tooth Loss
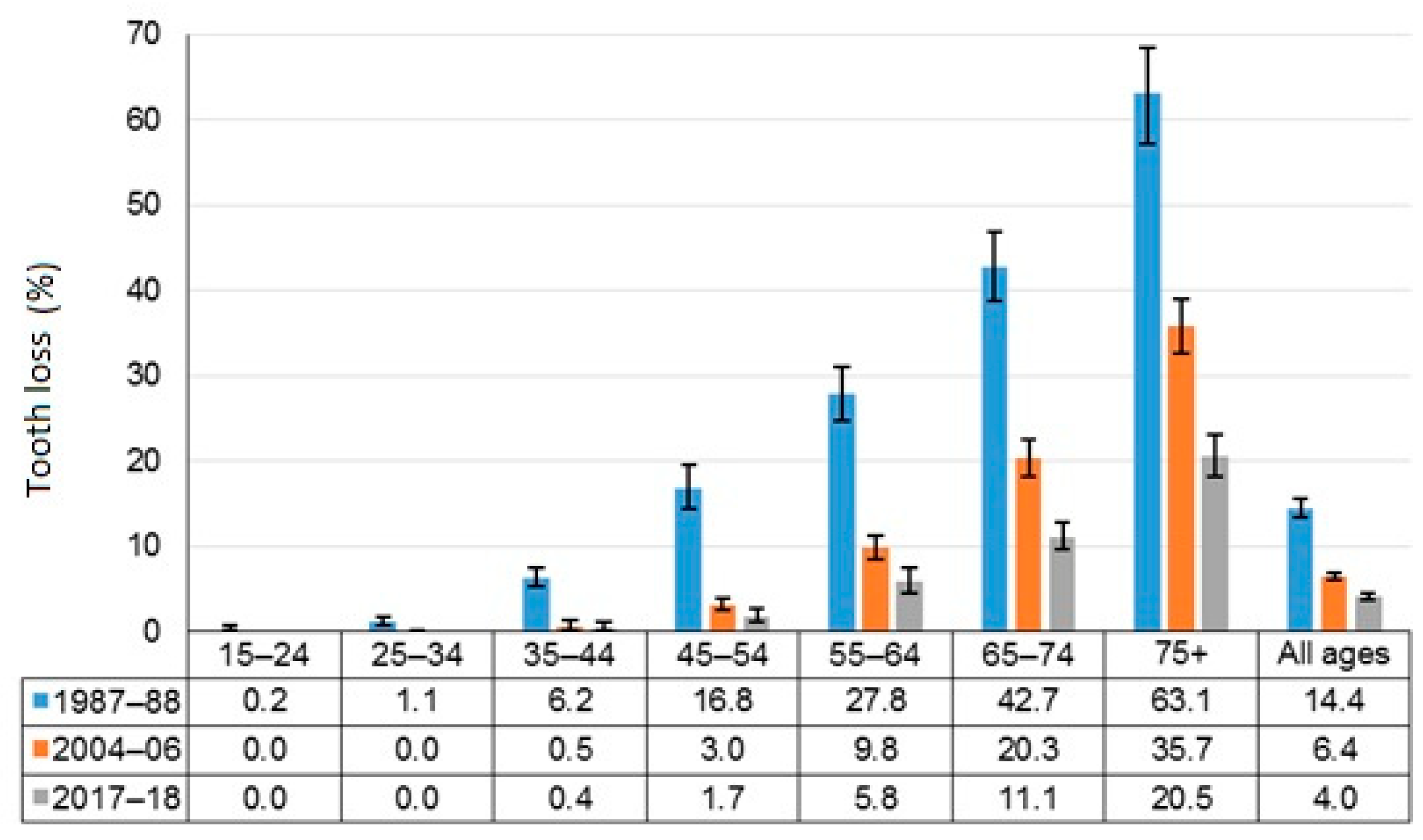
3.5. Time Trends in Oral Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Regional Office for Europe. 2021. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/oral-health (accessed on 4 July 2021).
- Glick, M.; Williams, D.M.; Kleinman, D.V.; Vujicic, M.; Watt, R.G.; Weyant, R.J. A new definition for oral health developed by the FDI World Dental Federation opens the door to a universal definition of oral health. J. Public Health Dent. 2017, 77, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Watt, R.G.; Williams, D.M.; Giannobile, W.V. A New Definition for Oral Health: Implications for Clinical Practice, Policy, and Research. J. Dent. Res. 2017, 96, 125–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, B.; James, Z.; Shroff Karhade, D.; Barrow, J.; Pruneddu, A.; Anderson, N.K.; Mossey, P. Definition of Global Health TFFT. A definition of global oral health: An expert consensus approach by the Consortium of Universities for Global Health’s Global Oral Health Interest Group. Glob Health Action 2020, 13, 1814001. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 6 July 2021).
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Veiga, N.; Aires, D.; Douglas, F.; Pereira, M.; Vaz, A.; Rama, L.; Silva, M.; Miranda, V.; Pereira, F.; Vidal, B.; et al. Dental caries: A review. J. Dent. Oral Health 2016, 2, 1–3. [Google Scholar]
- GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016, a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017, a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990–2010, a systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Oral Health and Dental Care in Australia. Cat. no. DEN 231; AIHW: Canberra, Australia, 2021. Available online: https://www.aihw.gov.au/reports/dental-oral-health/oral-health-and-dental-care-in-australia/contents/healthy-teeth (accessed on 27 July 2021).
- Australian Research Centre for Population Oral Health (ARCPOH). Australia’s Oral Health: The National Study of Adult Oral Health 2017–18; University of Adelaide: Adelaide, Australia, 2019. [Google Scholar]
- Chrisopoulos, S.; Ellershaw, E.; Luzzi, L. National Study of Adult Oral Health 2017–2018, Study design and methods. Aust. Dent. J. 2020, 65, S5–S10. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.F.; Ellershaw, A. Oral Health and Use of Dental Services 2008. Findings from the National Dental Telephone Interview Survey 2008; Dental Statistics and Research Series no. 58. Cat. no. DEN 216; Australian Institute if Health and Welfare: Canberra, Australia, 2012. [Google Scholar]
- Do, L.G.; Peres, K.G.; Ha, D.H.; Roberts-Thomson, K. Oral epidemiological examination—Protocol: The National Study of Adult Oral Health 2017–18. Aust. Dent. J. 2020, 65, S18–S22. [Google Scholar] [CrossRef] [PubMed]
- Loe, H.; Silness, J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- NIDCR. National Health and Nutrition Examination Survey Dental Examiners Procedures Manual; US National Center for Health Statistics: Hyattsville, MD, USA, 2002. [Google Scholar]
- Barnard, P.D. National Oral Health Survey Australia 1987–88; Australian Government Publishing Services: Canberra, Australia, 1993. [Google Scholar]
- Roberts-Thomson, K.; Do, L. Australia’s Dental Generations: The National Survey of Adult Oral Health 2004–2006; Australian Institute of Health and Welfare: Canberra, Australia, 2007. [Google Scholar]
- Australian Institute of Health and Welfare. Australia’s National Oral Health Plan 2015–2024, Performance Monitoring Report in Brief; Cat. no. DEN 234; AIHW: Canberra, Australia, 2020. [Google Scholar]
- Do, L.G. Australian Research Centre for Population Oral Health. Guidelines for use of fluorides in Australia: Update 2019. Aust. Dent. J. 2020, 65, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Spencer, A.J.; Liu, P.; Armfield, J.M.; Do, L.G. Preventive benefit of access to fluoridated water for young adults. J. Public Health Dent. 2017, 77, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Thomson, W.M.; Williams, S.M.; Broadbent, J.M.; Poulton, R.; Locker, D. Long-term dental visiting patterns and adult oral health. J. Dent. Res. 2010, 89, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Amarasena, N.; Kapellas, K.; Skilton, M.R.; Maple-Brown, L.J.; Brown, A.; Bartold, M.; O’Dea, K.; Celermajer, D.; Jamieson, L.M. Factors Associated with Routine Dental Attendance among Aboriginal Australians. J. Health Care Poor Underserved 2016, 27 (Suppl. 1), 67–80. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A.E. Social Determinants of Oral Health: Conditions Linked to Socioeconomic Inequalities in Oral Health and in the Australian Population; Population Oral Health Series No. 7; Australian Institute of Health and Welfare: Canberra, Australia, 2007. [Google Scholar]
- Mejia, G.C.; Elani, H.W.; Harper, S.; Thomson, W.M.; Ju, X.; Kawachi, I.; Kaufman, J.S.; Jamieson, L.M. Socioeconomic status, oral health and dental disease in Australia, Canada, New Zealand and the United States. BMC Oral Health 2018, 18, 176. [Google Scholar] [CrossRef] [PubMed]
- Amarasena, N.; Kapellas, K.; Skilton, M.R.; Maple-Brown, L.J.; Brown, A.; O’Dea, K.; Celermajer, D.; Jamieson, L.M. Associations with dental caries experience among a convenience sample of Aboriginal Australian adults. Aust. Dent. J. 2015, 60, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, L.M.; Elani, H.W.; Mejia, G.C.; Ju, X.; Kawachi, I.; Harper, S.; Thomson, W.M.; Kaufman, J.S. Inequalities in Indigenous Oral Health: Findings from Australia, New Zealand, and Canada. J. Dent. Res. 2016, 95, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, L.; Hedges, J.; Peres, M.A.; Guarnizo-Herreño, C.C.; Bastos, J.L. Challenges in identifying indigenous peoples in population oral health surveys: A commentary. BMC Oral Health 2021, 21, 216. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N | % (95% CI) | Age (Years) | |||||
|---|---|---|---|---|---|---|---|
| Total | 15–34 | 35–54 | 55–74 | ≥75 | |||
| % (95% CI) | |||||||
| All people | 5022 | 32.1 (29.6, 34.7) | 30.3 (25.7, 35.2) | 35.4 (31.1, 40.0) | 32.2 (28.2, 36.6) | 24.5 (18.8, 31.3) | |
| Sex | |||||||
| Male | 2249 | 49.6 (46.9, 52.2) | 34.7 (31.2, 38.4) | 32.1 (25.1, 40.0) | 37.1 (30.9, 43.7) | 38.5 (33.2, 44.2) | 22.3 (14.8, 32.2) |
| Female | 2773 | 50.4 (47.8, 53.1) | 29.5 (26.3, 32.9) | 28.4 (23.2, 24.2) | 33.8 (28.3, 39.8) | 26.0 (20.3, 32.6) | 26.2 (18.3, 36.0) |
| Indigenous identity | |||||||
| Non-Indigenous | 4937 | 98.3 (97.4, 98.9) | 32.1 (29.5, 34.7) | 30.6 (26.0, 35.6) | 35.4 (31.1, 40.0) | 31.6 (27.6, 35.9) | 24.5 (18.8, 31.3) |
| Indigenous | 84 | 1.7 (1.1, 2.6) | * 27.8 (15.0, 45.5) | * 17.6 (6.8, 38.3) | * 36.1(15.5, 63.4) | 72.8 (45.1, 89.7) | * 22.4 (2.6, 75.9) |
| Residential location | |||||||
| Major cities | 2969 | 72.7 (69.1, 76.0) | 31.8 (28.7, 35.1) | 28.0 (23.4, 33.2) | 35.3 (29.9, 41.2) | 34.9 (29.4, 40.7) | 25.7 (18.2, 34.9) |
| Rural/remote | 2053 | 27.3 (24.0, 30.9) | 32.6 (28.4, 37.1) | 35.9 (26.0, 47.1) | 35.6 (29.3, 42.6) | 28.0 (22.4, 34.4) | 22.5 (14.9, 32.5) |
| Year level of schooling | |||||||
| Year 10 or less | 1190 | 25.5 (23.5, 27.8) | 36.9 (32.0, 42.1) | 32.8 (22.4, 45.3) | 51.4 (41.1, 61.6) | 35.0 (28.0, 42.7) | 25.3 (17.7, 34.7) |
| Year 11 or more | 3793 | 74.5 (72.2, 76.5) | 30.2 (27.3, 33.2) | 29.6 (25.0, 34.7) | 31.7 (27.1, 36.8) | 29.7 (25.1, 34.9) | 22.5 (14.3, 33.7) |
| Highest qualification attained | |||||||
| Degree or higher | 2026 | 29.3 (26.9, 31.8) | 30.4 (26.3, 34.8) | 33.1 (26.4, 40.4) | 29.3 (23.6, 35.7) | 27.6 (21.4, 34.7) | * 14.5 (7.7, 25.5) |
| Other/None | 2931 | 70.7 (68.2, 73.1) | 32.6 (29.5, 35.8) | 28.6 (22.9, 35.0) | 39.0 (33.2, 45.1) | 32.6 (27.9, 37.6) | 24.9 (18.7, 32.3) |
| Eligibility for public dental care | |||||||
| Eligible | 1634 | 30.7 (28.3, 33.1) | 34.5 (30.1, 39.1) | 29.3 (18.8, 42.6) | 54.2 (45.5, 62.7) | 32.9 (26.6, 39.8) | 24.1 (18.1, 31.5) |
| Ineligible | 3373 | 69.3 (66.9, 71.7) | 31.1 (28.1, 34.2) | 30.8 (26.0, 36.0) | 31.4 (26.9, 36.3) | 31.4 (26.3, 37.0) | * 26.7 (13.8, 45.4) |
| Dental insurance | |||||||
| Insured | 2548 | 45.3 (42.5, 48.1) | 24.4 (21.3, 27.7) | 22.3 (17.3, 28.4) | 25.1 (19.8, 31.3) | 25.9 (21.3, 31.1) | 24.9 (17.0, 34.8) |
| Uninsured | 2385 | 54.7 (51.9, 57.5) | 38.6 (35.2, 42.1) | 35.9 (29.8, 42.5) | 45.7 (39.9, 51.6) | 37.8 (31.5, 44.5) | 24.3 (16.3, 34.6) |
| Usually visit dentist | |||||||
| For a check-up | 3135 | 61.5 (58.8, 64.1) | 24.3 (21.4, 27.5) | 24.2 (19.3, 29.9) | 25.4 (20.3, 31.3) | 24.4 (19.6, 30.0) | 19.5 (13.1, 28.0) |
| For a dental problem | 1796 | 38.5 (35.9, 41.2) | 43.5 (39.3, 47.9) | 43.7 (35.6, 52.2) | 49.2 (42.5, 56.0) | 39.4 (32.5, 46.7) | 30.9 (20.1, 44.3) |
| N | % (95% CI) | Age (Years) | |||||
|---|---|---|---|---|---|---|---|
| Total | 15–34 | 35–54 | 55–74 | ≥75 | |||
| Mean (95% CI) | |||||||
| All people | 5022 | 1.4 (1.2, 1.6) | 1.3 (0.9, 1.7) | 1.4 (1.1, 1.7) | 1.8 (1.3, 2.3) | 1.1 (0.6, 1.5) | |
| Sex | |||||||
| Male | 2249 | 49.6 (46.9, 52.2) | 1.7 (1.4, 2.0) | 1.3 (0.8, 1.7) | 1.6 (1.1, 2.1) | 2.8 (1.9, 3.6) | 1.1 * (0.3, 1.9) |
| Female | 2773 | 50.4 (47.8, 53.1) | 1.2 (0.9, 1.4) | 1.4 (0.8, 1.9) | 1.3 (0.9, 1.7) | 0.8 (0.5, 1.0) | 1.1 (0.6, 1.6) |
| Indigenous identity | |||||||
| Non-Indigenous | 4937 | 98.3 (97.4, 98.9) | 1.4 (1.2, 1.6) | 1.3 (0.9, 1.6) | 1.4 (1.1, 1.7) | 1.8 (1.3, 2.2) | 1.1 (0.6, 1.6) |
| Indigenous | 84 | 1.7 (1.1, 2.6) | 2.7 * (0.5, 4.9) | 2.5 * (0.0, 5.7) | 3.2 * (0.2, 6.3) | 2.8 * (0.0, 6.5) | 0.9 * (0.0, 2.6) |
| Residential location | |||||||
| Major cities | 2969 | 72.7 (69.1,76.0) | 1.4 (1.1,1.6) | 1.3 (0.8,1.7) | 1.4 (1.0,1.8) | 1.6 (1.0,2.1) | 1.3 (0.6,1.9) |
| Rural/remote | 2053 | 27.3 (24.0,30.9) | 1.6 (1.3,2.0) | 1.4 (0.9,1.9) | 1.5 (1.1,2.0) | 2.2 (1.3,3.2) | 0.7 (0.4,1.0) |
| Year level of schooling | |||||||
| Year 10 or less | 1190 | 25.5 (23.5,27.8) | 2.1 (1.6,2.6) | 2.6 * (1.0,4.2) | 2.2 (1.5,2.9) | 2.2 (1.4,3.0) | 1.3 * (0.6,2.0) |
| Year 11 or more | 3793 | 74.5 (72.2,76.5) | 1.2 (1.0,1.4) | 1.1 (0.8,1.4) | 1.3 (0.9,1.6) | 1.3 (0.9,1.6) | 0.7 (0.4,1.0) |
| Highest qualification attained | |||||||
| Degree or above | 2026 | 29.3 (26.9,31.8) | 0.9 (0.7,1.2) | 0.9 (0.6,1.3) | 0.9 (0.5,1.2) | 1.1 (0.6,1.7) | 0.9 * (0.2,1.7) |
| Other/None | 2931 | 70.7 (68.2,73.1) | 1.7 (1.4,1.9) | 1.5 (0.9,2.1) | 1.7 (1.3,2.2) | 2 (1.4,2.5) | 1.1 (0.5,1.6) |
| Eligibility for public dental care | |||||||
| Eligible | 1634 | 30.7 (28.3,33.1) | 2.1 (1.6,2.5) | 1.8 * (0.6,3.0) | 2.9 (2.1,3.8) | 2.3 (1.4,3.1) | 1.1 (0.6,1.7) |
| Ineligible | 3373 | 69.3 (66.9,71.7) | 1.2 (1.0,1.4) | 1.2 (0.8,1.5) | 1.1 (0.8,1.4) | 1.3 (0.9,1.8) | 0.8 * (0.3,1.3) |
| Dental insurance | |||||||
| Insured | 2548 | 45.3 (42.5,48.1) | 0.8 (0.6,1.0) | 0.7 (0.4,0.9) | 0.8 (0.5,1.1) | 1.1 (0.7,1.6) | 0.6 (0.4,0.9) |
| Uninsured | 2385 | 54.7 (51.9,57.5) | 1.9 (1.6,2.2) | 1.6 (1.1,2.1) | 2 (1.6,2.5) | 2.3 (1.6,3.1) | 1.4 * (0.6,2.3) |
| Usually visit dentist | |||||||
| For a check-up | 3135 | 61.5 (58.8,64.1) | 0.7 (0.6,0.9) | 0.7 (0.5,0.9) | 0.8 (0.5,1.2) | 0.6 (0.5,0.8) | 0.5 (0.3,0.7) |
| For a dental problem | 1796 | 38.5 (35.9,41.2) | 2.3 (1.9,2.6) | 2.4 (1.5,3.3) | 2.1 (1.7,2.6) | 2.4 (1.7,3.2) | 1.8 * (0.7,2.9) |
| N | Weighted % | Age (Years) | |||||
|---|---|---|---|---|---|---|---|
| Total | 15–34 | 35–54 | 55–74 | ≥75 | |||
| Mean (95% CI) | |||||||
| All people | 5022 | 29.7 (28.4, 31.1) | 7.7 (6.9, 8.5) | 24.9 (23.3, 26.5) | 57.1 (54.8, 59.4) | 75.3 (72.2, 78.4) | |
| Sex | |||||||
| Male | 2249 | 49.6 (46.9,52.2) | 27.1 (25.2, 29.1) | 7.3 (6.0, 8.5) | 22.2 (19.8, 24.5) | 53.5 (50.5, 56.4) | 71.5 67.1, 76.0) |
| Female | 2773 | 50.4 (47.8,53.1) | 32.3 (30.5, 34.1) | 8.1 (6.9, 9.4) | 27.6 (25.6, 29.6) | 60.7 (57.3, 64.2) | 78.3 (74.5, 82.1) |
| Indigenous identity | |||||||
| Non-Indigenous | 4937 | 98.3 (97.4,98.9) | 29.9 (28.5, 31.3) | 7.7 (6.9, 8.6) | 24.9 (23.3, 26.5) | 57.1 (54.8, 59.5) | 75.4 (72.3, 78.5) |
| Indigenous | 84 | 1.7 (1.1,2.6) | 18.7 (10.3, 27.1) | * 6.9 (1.1, 12.7) | 27.5 (22.7, 32.3) | 63.9 (54.9, 72.8) | NP |
| Residential location | |||||||
| Major cities | 2969 | 72.7 (69.1,76.0) | 28.5 (26.9, 30.1) | 7.8 (6.8, 8.9) | 24.4 (22.5, 26.3) | 57 (53.6, 60.4) | 77.8 (73.8, 81.7) |
| Rural/remote | 2053 | 27.3 (24.0,30.9) | 32.3 (29.8, 34.8) | 7.3 (5.9, 8.8) | 26 (23.1, 28.9) | 57.2 (54.7, 59.7) | 71.1 (66.9, 75.4) |
| Year level of schooling | |||||||
| Year 10 or less | 1190 | 25.5 (23.5,27.8) | 43.9 (41.1–46.8) | 7.6 (4.6, 10.6) | 29.9 (26.1, 33.8) | 57 (53.4, 60.7) | 75.6 (71.2, 80.0) |
| Year 11 or more | 3793 | 74.5 (72.2,76.5) | 24.8 (23.4, 26.2) | 7.6 (6.8, 8.5) | 23.9 (22.1, 25.6) | 57.3 (54.3, 60.3) | 74.8 (71.2, 78.4) |
| Highest qualification attained | |||||||
| Degree or higher | 2026 | 29.3 (26.9,31.8) | 20.9 (19.2, 22.5) | 8.4 (7.2, 9.6) | 19 (17.1, 20.8) | 55.8 (52.9, 58.7) | 76.3 (72.0, 80.6) |
| Other/None | 2931 | 70.7 (68.2,73.1) | 33.4 (31.8, 35.1) | 7.3 (6.2, 8.4) | 28.3 (26.1, 30.5) | 58 (55.4, 60.5) | 75.7 (72.1, 79.2) |
| Eligibility for public dental care | |||||||
| Eligible | 1634 | 30.7 (28.3,33.1) | 44.8 (42.0, 47.6) | 8.8 (6.8, 10.7) | 32.5 (28.6, 36.4) | 58.9 (55.2, 62.5) | 75.5 (72.0–79.0) |
| Ineligible | 3373 | 69.3 (66.9,71.7) | 23.2 (21.8, 24.5) | 7.5 (6.6, 8.4) | 23.3 (21.6, 25.0) | 55.4 (52.5, 58.3) | 74.1 (69.2, 79.0) |
| Dental insurance | |||||||
| Insured | 2548 | 45.3 (42.5,48.1) | 30.6 (28.8, 32.4) | 7.5 (6.2, 8.7) | 23.2 (21.1, 25.4) | 59.4 (57.0, 61.8) | 76.4 (72.8, 79.9) |
| Uninsured | 2385 | 54.7 (51.9,57.5) | 29.9 (27.9, 31.8) | 7.9 (6.8, 9.1) | 27.1 (24.6, 29.5) | 55.3 (51.6, 59.0) | 74.6 (69.8, 79.3) |
| Usually visit dentist | |||||||
| For a check-up | 3135 | 61.5 (58.8,64.1) | 26.6 (25.0, 28.1) | 6.5 (5.6, 7.3) | 21.9 (19.8, 23.9) | 56.7 (54.3, 59.2) | 75.5 (71.1, 79.8) |
| For a dental problem | 1796 | 38.5 (35.9,41.2) | 35.7 (33.4, 37.9) | 10.8 (8.9, 12.7) | 29.8 (27.2, 32.4) | 57.7 (53.5, 61.9) | 75.3 (71.1, 79.4) |
| N | % (95% CI) | Age (Years) | |||||
|---|---|---|---|---|---|---|---|
| Total | 15–34 | 35–54 | 55–74 | ≥75 | |||
| % (95% CI) | |||||||
| All people | 4401 | 28.8 (26.1, 31.6) | 31.3 (27.1, 35.8) | 29.5 (25.2, 34.2) | 24.4 (20.7, 28.6) | 20.9 (15.0, 28.2) | |
| Sex | |||||||
| Male | 1906 | 48.9 (46.0,51.8) | 34.7 (30.7,39.0) | 34.9 (28.5,41.8) | 35.6 (29.3,42.4) | 34.1 (28.0,40.8) | 27.4 (17.0,41.1) |
| Female | 2496 | 51.1 (48.2,54.0) | 23.1 (20.3,26.1) | 27.6 (22.7,33.0) | 23.7 (18.8,29.3) | 15.7 (12.1,20.3) | 16.7 (10.3,26.0) |
| Indigenous identity | |||||||
| Non-Indigenous | 4330 | 98.4 (97.4,99.0) | 28.7 (26.0,31.5) | 31.3 (27.0,35.9) | 29.1 (24.8,33.8) | 24.6 (20.8,28.9) | 20.9 (15.1,28.2) |
| Indigenous | 71 | 1.6 (1.0,2.6) | 38.6 (19.9,61.4) | 30.5 * (11.1,60.7) | 63.3 (36.2,84.0) | 9.9 * (1.2,49.2) | NP |
| Residential location | |||||||
| Major cities | 2607 | 73.8 (70.3,77.0) | 30.1 (26.8,33.5) | 31.5 (26.8,36.6) | 31.6 (26.2,37.5) | 26.0 (21.0,31.7) | 21.9 (14.9,30.8) |
| Rural/remote | 1795 | 26.2 (23.0,29.7) | 25.2 (20.6,30.4) | 30.4 (21.8,40.6) | 24.2 (18.1,31.4) | 21.1 (16.3,26.9) | 18.2 * (9.2,32.9) |
| Year level of schooling | |||||||
| Year 10 or less | 943 | 23.2 (21.2,25.4) | 28.6 (24.0,33.8) | 40.2 (27.5,54.3) | 30.4 (22.1,40.1) | 23.3 (17.5,30.2) | 18.6 (11.4,28.8) |
| Year 11 or more | 3427 | 76.8 (74.6,78.8) | 28.9 (25.9,32.1) | 29.9 (25.5,34.7) | 29.3 (24.6,34.6) | 25.6 (21.0,30.9) | 24.5 (15.7,36.0) |
| Highest qualification attained | |||||||
| Degree or above | 1865 | 30.6 (28.1,33.3) | 24.0 (20.5,28.0) | 21.3 v | 27.3 (21.2,34.3) | 24.2 (17.5,32.5) | 22.2 * (11.3,39.1) |
| Other/None | 2477 | 69.4 (66.7,71.9) | 31.2 (27.9,34.6) | 36.7 (31.1,42.7) | 31.0 (25.6,37.0) | 25.2 (20.9,30.0) | 20.7 (14.1,29.3) |
| Eligibility for public dental care | |||||||
| Eligible | 1264 | 27.3 (24.9,29.9) | 30.4 (26.0,35.3) | 31.9 (22.8,42.5) | 38.1 (29.1,48.0) | 28.4 (22.2,35.5) | 19.6 (13.5,27.6) |
| Ineligible | 3123 | 72.7 (70.1,75.1) | 28.3 (25.3,31.5) | 31.3 (26.7,36.4) | 27.8 (23.3,32.8) | 21.4 (17.0,26.4) | 29.6 * (14.1,51.8) |
| Dental insurance | |||||||
| Insured | 2261 | 46.1 (43.0,49.2) | 25.2 (22.0,28.8) | 29.9 (24.0,36.5) | 25.0 (19.8,31.1) | 20.4 (16.2,25.3) | 14.9 (9.1,23.6) |
| Uninsured | 2058 | 53.9 (50.8,57.0) | 31.1 (27.5,34.9) | 30.1 (24.6,36.1) | 34.8 (28.6,41.6) | 28.4 (22.5,35.1) | 25.8 (16.9,37.3) |
| Usually visit dentist | |||||||
| For a check-up | 2775 | 62.3 (59.5,65.1) | 25.2 (22.0,28.7) | 27.5 (22.5,33.1) | 25.2 (20.2,31.1) | 20.7 (16.7,25.3) | 20.5 (13.6,29.9) |
| For a dental problem | 1548 | 37.7 (34.9,40.5) | 33.2 (29.3,37.4) | 35.4 (27.9,43.6) | 35.7 (29.3,42.8) | 28.7 (22.6,35.8) | 21.4 * (12.2,34.9) |
| N | % (95% CI) | Age (Years) | |||||
|---|---|---|---|---|---|---|---|
| Total | 15–34 | 35–54 | 55–74 | ≥75 | |||
| % (95% CI) | |||||||
| All people | 4402 | 30.1 (27.9, 32.4) | 12.2 (9.5, 15.6) | 32.7 (28.5, 37.3) | 51.1 (46.2, 56.0) | 69.3 (60.5, 76.9) | |
| Sex | |||||||
| Male | 1906 | 48.9 (46.0,51.8) | 34.9 (31.2,38.8) | 16.6 (11.8,22.8) | 38.9 (32.1,46.3) | 59.5 (53.3,65.4) | 63.1 (48.1,75.9) |
| Female | 2496 | 51.1 (48.2,54.0) | 25.5 (22.7,28.5) | 7.8 (5.3,11.3) | 26.6 (21.7,32.2) | 43.5 (37.1,50.2) | 73.0 (62.3,81.6) |
| Indigenous identity | |||||||
| Non-Indigenous | 4330 | 98.4 (97.4,99.0) | 30.3 (28.1,32.7) | 12.5 (9.7,15.9) | 32.9 (28.6,37.5) | 50.8 (46.0,55.6) | 69.2 (60.4,76.8) |
| Indigenous | 71 | 1.6 (1.0,2.6) | 11.0 * (5.3,21.3) | 3.9 * (0.8,17.2) | 21.0 * (8.2,44.1) | 49.7 * (15.4,84.3) | NP |
| Residential location | |||||||
| Major cities | 2607 | 73.8(70.3,77.0) | 29.4 (26.7,32.2) | 12.2 (9.0,16.4) | 31.6 (26.4,37.2) | 52.9 (46.7,59.1) | 71.1 (60.1,80.0) |
| Rural/remote | 1795 | 26.2 (23.0,29.7) | 32.1 (28.1,36.5) | 12.3 (8.2,18.2) | 35.8 (28.8,43.4) | 47.1 (39.6,54.8) | 64.4 (49.7,76.9) |
| Year level of schooling | |||||||
| Year 10 or less | 943 | 23.2 (21.2,25.4) | 45.0 (39.6,50.5) | 7.7 * (3.3,16.7) | 50.0 (39.8,60.3) | 55.9 (47.8,63.7) | 72.2 (61.0,81.1) |
| Year 11 or more | 3427 | 76.8 (74.6,78.8) | 25.6 (23.2,28.2) | 12.9 (9.8,16.8) | 29.2 (24.8,34.1) | 47.8 (42.3,53.3) | 64.7 (49.2,77.7) |
| Highest qualification attained | |||||||
| Degree or above | 1865 | 23.2 (21.2,25.4) | 21.7 (18.2,25.6) | 11.6 (6.7,19.1) | 22.7 (18.1,28.1) | 49.7 (42.6,56.7) | 59.6 (35.9,79.6) |
| Other/None | 2477 | 69.4 (66.7,71.9) | 33.6 (30.6,36.6) | 12.6 (9.5,16.5) | 38.4 (32.5,44.6) | 50.9 (45.3,56.5) | 69.9 (60.6,77.8) |
| Eligibility for public dental care | |||||||
| Eligible | 1264 | 27.3 (24.9,29.9) | 42.5 (37.9,47.2) | 15.7 (9.0,25.9) | 41.3 (32.1,51.2) | 54.8 (47.5,61.9) | 70.6 (61.5,78.3) |
| Ineligible | 3123 | 72.7 (70.1,75.1) | 25.5 (22.9,28.2) | 11.5 (8.7,14.9) | 30.9 (26.2,36.0) | 47.7 (41.8,53.7) | 59.3 (33.3,80.9) |
| Dental insurance | |||||||
| Insured | 2261 | 46.1 (43.0,49.2) | 25.4 (22.7,28.3) | 8.4 (5.1,13.4) | 24.5 (19.8,30.0) | 45.2 (39.0,51.6) | 67.4 (53.1,79.1) |
| Uninsured | 2058 | 53.9 (50.8,57.0) | 35.0 (31.8,38.4) | 15.7 (11.5,20.9) | 41.1 (34.8,47.7) | 56.9 (49.7,63.8) | 70.7 (59.7,79.8) |
| Usually visit dentist | |||||||
| For a check-up | 2775 | 62.3 (59.5,65.1) | 26.1 (23.4,29.0) | 8.8 (6.0,12.9) | 29.5 (23.9,35.8) | 49.0 (43.0,55.0) | 72.5 (60.4,81.9) |
| For a dental problem | 1548 | 37.7 (34.9,40.5) | 36.8 (32.6,41.3) | 18.8 (13.4,25.8) | 37.2 (30.4,44.5) | 53.0 (45.6,60.2) | 64.3 (50.3,76.2) |
| N | % (95% CI) | Age (Years) | |||||
|---|---|---|---|---|---|---|---|
| Total | 15–34 | 35–54 | 55–74 | ≥75 | |||
| % (95% CI) | |||||||
| All people | 15,731 | 4.0 (3.6, 4.4) | — | 1.1 (0.7, 1.6) | 8.1 (7.0, 9.3) | 20.5 (18.1, 23.1) | |
| Sex | |||||||
| Male | 6781 | 49.2 (48.1,50.4) | 3.4 (2.9,3.9) | — | 1.1 * (0.6,2.0) | 6.5 (5.2,8.1) | 19.1 (15.6,23.2) |
| Female | 8950 | 50.8 (49.6,51.9) | 4.7 (4.1,5.3) | — | 1.0 * (0.6,1.8) | 9.6 (8.0,11.5) | 21.5 (18.4,25.0) |
| Indigenous identity | |||||||
| Non-Indigenous | 15,392 | 97.7 (97.3,98.1) | 4.0 (3.6,4.4) | — | 1.1 (0.7,1.6) | 7.7 (6.7,8.9) | 20.5 (18.1,23.1) |
| Indigenous | 334 | 2.3 (1.9,2.7) | 7.1 (4.3,11.4) | — | 0.8 * (0.2,2.5) | 29.3 (17.8,44.1) | 19.5 * (6.5,45.9) |
| Residential location | |||||||
| Major cities | 9372 | 71.8 (68.6,74.9) | 3.5 (3.0,4.0) | — | 1.0 * (0.6,1.7) | 7.4 (6.0,9.0) | 18.8 (15.9,22.0) |
| Rural/remote | 6359 | 28.2 (25.1,31.4) | 5.4 (4.7,6.2) | — | 1.2 * (0.7,2.0) | 9.5 (8.1,11.2) | 24.2 (20.1,28.7) |
| Year level of schooling | |||||||
| Year 10 or less | 4198 | 28.9 (27.8,30.1) | 9.4 (8.5,10.5) | — | 3.1 * (1.8,5.2) | 11.7 (9.9,13.8) | 24.9 (21.6,28.5) |
| Year 11 or more | 11,355 | 71.1 (69.9,72.2) | 1.8 (1.5,2.1) | — | 0.6 * (0.3,1.1) | 5.3 (4.2,6.7) | 13.1 (10.2,16.6) |
| Highest qualification attained | |||||||
| Degree or higher | 5836 | 26.8 (25.4,28.2) | 0.7 (0.5,1.1) | — | 0.5 * (0.1,1.6) | 2.0 (1.3,3.1) | 5.3 * (3.0,9.0) |
| Other/None | 9584 | 73.2 (71.8,74.6) | 5.1 (4.6,5.7) | — | 1.3 (0.8,2.0) | 9.4 (8.1,10.8) | 22.0 (19.4,24.9) |
| Eligibility for public dental care | |||||||
| Eligible | 4976 | 30.2 (29.0,31.4) | 10.5 (9.5,11.7) | — | 3.1 * (1.7,5.3) | 13.4 (11.5,15.6) | 22.3 (19.6,25.2) |
| Ineligible | 10,686 | 69.8 (68.6,71.0) | 1.2 (1.0,1.5) | — | 0.7 * (0.4,1.2) | 3.7 (2.9,4.9) | 11.3 (7.6,16.5) |
| Dental insurance | |||||||
| Insured | 8238 | 51.1 (49.5,52.8) | 1.7 (1.4,2.0) | — | 0.5 * (0.3,1.1) | 3.6 (2.8,4.5) | 9.2 (7.0,11.9) |
| Uninsured | 7206 | 48.9 (47.2,50.5) | 6.5 (5.8,7.2) | — | 1.8 (1.1,2.8) | 12.7 (10.9,14.8) | 28.3 (24.7,32.3) |
| Usually visit dentist | |||||||
| For a check-up | 9790 | 63.3 (61.9,64.6) | 1.2 (0.9,1.5) | — | 0.3 * (0.2,0.6) | 3.0 (2.1,4.2) | 6.1 (4.4,8.4) |
| For a dental problem | 5620 | 36.7 (35.4,38.1) | 7.9 (7.1,8.8) | — | 2.2 (1.3,3.5) | 13.0 (11.2,15.0) | 32.5 (28.5,36.7) |
| N | % (95% CI) | Age (Years) | |||||
|---|---|---|---|---|---|---|---|
| Total | 15–34 | 35–54 | 55–74 | ≥75 | |||
| Mean (95% CI) | |||||||
| All people | 5022 | 4.4 (4.1, 4.7) | 0.6 (0.4, 0.7) | 3.6 (3.3, 3.9) | 8.8 (8.2, 9.4) | 13.2 (12.2, 14.2) | |
| Sex | |||||||
| Male | 2249 | 49.6 (46.9,52.2) | 4.2 (3.8,4.6) | 0.5 (0.3,0.8) | 3.4 (3.0,3.9) | 8.6 (8.0,9.3) | 13.6 (12.5,14.6) |
| Female | 2773 | 50.4 (47.8,53.1) | 4.6 (4.2,5.0) | 0.7 (0.4,0.9) | 3.8 (3.4,4.2) | 9 (8.0,10.0) | 12.9 (11.3,14.6) |
| Indigenous identity | |||||||
| Non-Indigenous | 4937 | 98.3 (97.4,98.9) | 4.4 (4.1,4.7) | 0.6 (0.4,0.7) | 3.6 (3.3,3.9) | 8.8 (8.2,9.4) | 13.2 (12.2,14.2) |
| Indigenous | 84 | 1.7 (1.1,2.6) | 3.2 (1.6,4.7) | 0.9 * (0.0,1.7) | 4.9 (3.2,6.7) | 11.5 (7.0,16.0) | 14 * (1.9,26.0) |
| Residential location | |||||||
| Major cities | 2969 | 72.7 (69.1,76.0) | 4 (3.7,4.4) | 0.6 (0.4,0.8) | 3.4 (3.0,3.8) | 8.4 (7.6,9.2) | 13.3 (12.0,14.6) |
| Rural/remote | 2053 | 27.3 (24.0,30.9) | 5.4 (4.9,5.9) | 0.7 (0.4,1.0) | 4.3 (3.7,4.8) | 9.6 (8.8,10.3) | 13 (11.6,14.4) |
| Year level of schooling | |||||||
| Year 10 or less Year 11 or more | 1190 3793 | 25.5 (23.5,27.8) 74.5 (72.2, 76.5) | 7.7 (7.1,8.2) 3.3 (3.0, 3.5) | 0.6 * (0.2,1.0) 0.6 (0.4, 0.7) | 4.7 (4.0,5.4) 3.4 (3.0, 3.8) | 10.2 (9.4,11.1) 7.7 (6.8, 8.6) | 14 (12.5,15.6) 11.8 (10.7, 12.9) |
| Highest qualification attained | |||||||
| Degree or above | 2026 | 29.3 (26.9,31.8) | 2.3 (2.0,2.5) | 0.6 (0.3,0.8) | 2.4 (2.0,2.7) | 6 (5.4,6.6) | 11 (9.1,13.0) |
| Other/None | 2931 | 70.7 (68.2,73.1) | 5.3 (4.9,5.6) | 0.6 (0.4,0.8) | 4.3 (3.9,4.8) | 9.4 (8.7,10.1) | 13.4 (12.2,14.5) |
| Eligibility for public dental care | |||||||
| Eligible | 1634 | 30.7 (28.3,33.1) | 7.6 (7.0,8.2) | 1 (0.5,1.4) | 5.2 (4.5,6.0) | 10.1 (9.3,11.0) | 13.6 (12.5,14.7) |
| Ineligible | 3373 | 69.3 (66.9,71.7) | 3 (2.7,3.3) | 0.5 (0.4,0.6) | 3.3 (2.9,3.6) | 7.6 (6.7,8.4) | 10.8 (9.1,12.5) |
| Dental insurance | |||||||
| Insured | 2548 | 45.3 (42.5,48.1) | 3.9 (3.5,4.2) | 0.4 (0.3,0.6) | 3.0 (2.6,3.4) | 7.6 (7.0,8.3) | 10.8 (9.8,11.8) |
| Uninsured | 2385 | 54.7 (51.9,57.5) | 5 (4.6,5.4) | 0.7 (0.5,1.0) | 4.3 (3.8,4.8) | 9.8 (9.0,10.7) | 15 (13.4,16.5) |
| Usually visit dentist | |||||||
| For a check-up | 3135 | 61.5 (58.8,64.1) | 3.5 (3.2,3.8) | 0.5 (0.3,0.7) | 3.1 (2.7,3.5) | 7.3 (6.8,7.9) | 11.3 (10.3,12.3) |
| For a dental problem | 1796 | 38.5 (35.9,41.2) | 6 (5.5,6.5) | 0.8 (0.6,1.1) | 4.5 (4.0,5.0) | 10.6 (9.5,11.7) | 16 (14.2,17.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amarasena, N.; Chrisopoulos, S.; Jamieson, L.M.; Luzzi, L. Oral Health of Australian Adults: Distribution and Time Trends of Dental Caries, Periodontal Disease and Tooth Loss. Int. J. Environ. Res. Public Health 2021, 18, 11539. https://doi.org/10.3390/ijerph182111539
Amarasena N, Chrisopoulos S, Jamieson LM, Luzzi L. Oral Health of Australian Adults: Distribution and Time Trends of Dental Caries, Periodontal Disease and Tooth Loss. International Journal of Environmental Research and Public Health. 2021; 18(21):11539. https://doi.org/10.3390/ijerph182111539
Chicago/Turabian StyleAmarasena, Najith, Sergio Chrisopoulos, Lisa M. Jamieson, and Liana Luzzi. 2021. "Oral Health of Australian Adults: Distribution and Time Trends of Dental Caries, Periodontal Disease and Tooth Loss" International Journal of Environmental Research and Public Health 18, no. 21: 11539. https://doi.org/10.3390/ijerph182111539
APA StyleAmarasena, N., Chrisopoulos, S., Jamieson, L. M., & Luzzi, L. (2021). Oral Health of Australian Adults: Distribution and Time Trends of Dental Caries, Periodontal Disease and Tooth Loss. International Journal of Environmental Research and Public Health, 18(21), 11539. https://doi.org/10.3390/ijerph182111539