
Development of a Model Care Pathway for Myasthenia Gravis

 , , , ,
, , , , 
Abstract
:1. Introduction
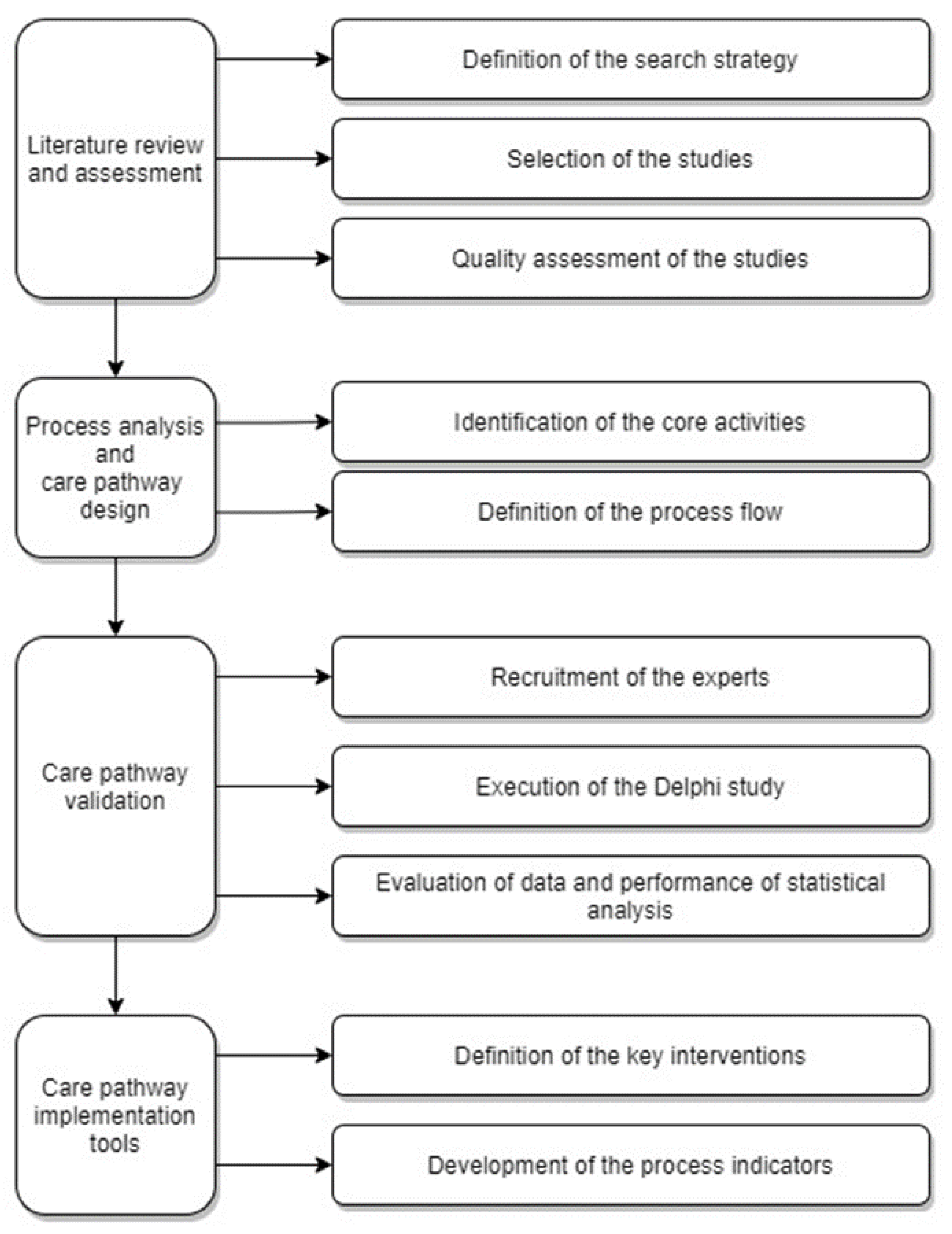
2. Materials and Methods
2.1. Literature Review and Assessment
2.1.1. Definition of the Search Strategy
- (i)
- Websites of international scientific societies: Myasthenia Gravis Foundation of America (MGFA) [https://myasthenia.org/], (accessed on 27 July 2020); Association of British Neurologists (ABN) [https://www.theabn.org (accessed on 27 July 2020)]; European Myasthenia Gravis Association (EuMGA) [http://www.eumga.eu (accessed on 27 July 2020)]; European academy of neurology (EAN)/ European Federation of Neurological Societies (EFNS) [https://www.ean.org (accessed on 27 July 2020)]; American Board of Electrodiagnostic Medicine (ABEM) [https://www.aanem.org]; American Association of Neuroscience Nurses (AANN) [https://aann.org]; American Academy of Neurology [https://www.aan.com (accessed on 27 July 2020)]; Japanese Society for Neuroimmunology (JSN) [http://www.neuroimmunology.jp (accessed on 27 July 2020)]; European Reference Network for Rare Neuromuscular Diseases (EURO-NMD) [https://ern-euro-nmd.eu (accessed on 27 July 2020)].
- (ii)
- Public resources for evidence-based clinical practice guidelines: Guidelines international interwork (GIN) [www.g-i-n.net (accessed on 28 July 2020)]; National Institute for Health and Care Excellence (NICE) [https://www.nice.org.uk/ (accessed on 28 July 2020)]; Scottish Intercollegiate Guidelines Network [https://www.sign.ac.uk/ (accessed on 28 July 2020)]; Canadian clinical practice guidelines [https://joulecma.ca/cpg/ (accessed on 28 July 2020)]; Australian clinical practice guidelines [https://www.clinicalguidelines.gov.au/ (accessed on 28 July 2020)].
- (iii)
- Electronic databases: PubMed [https://pubmed.ncbi.nlm.nih.gov]; UpToDate [https://www.uptodate.com/]; Cochrane library [https://www.cochranelibrary.com/ (accessed on 30 July 2020)]; EMBASE [https://www-embase.com/ (accessed on 30 July 2020)]; EBSCO CINHAL [https://www.ebsco.com/products/research-databases/cinahl-database (accessed on 30 July 2020)].
- (iv)
- Public resources for quality improvement indicators in healthcare: The Joint Commission [https://www.jointcommission.org/ (accessed on 31 July 2020)]; Agency for Health Care Research and Quality [https://www.qualitymeasures.ahrq.gov (accessed on 31 July 2020)]; Australian commission on safety and quality in health care [https://www.safetyandquality.gov.au/ (accessed on 31 July 2020)]; Canadian institute for health information [https://www.cihi.ca/ (accessed on 31 July 2020)]; Health quality Ontario [https://www.hqontario.ca/ (accessed on 31 July 2020)].
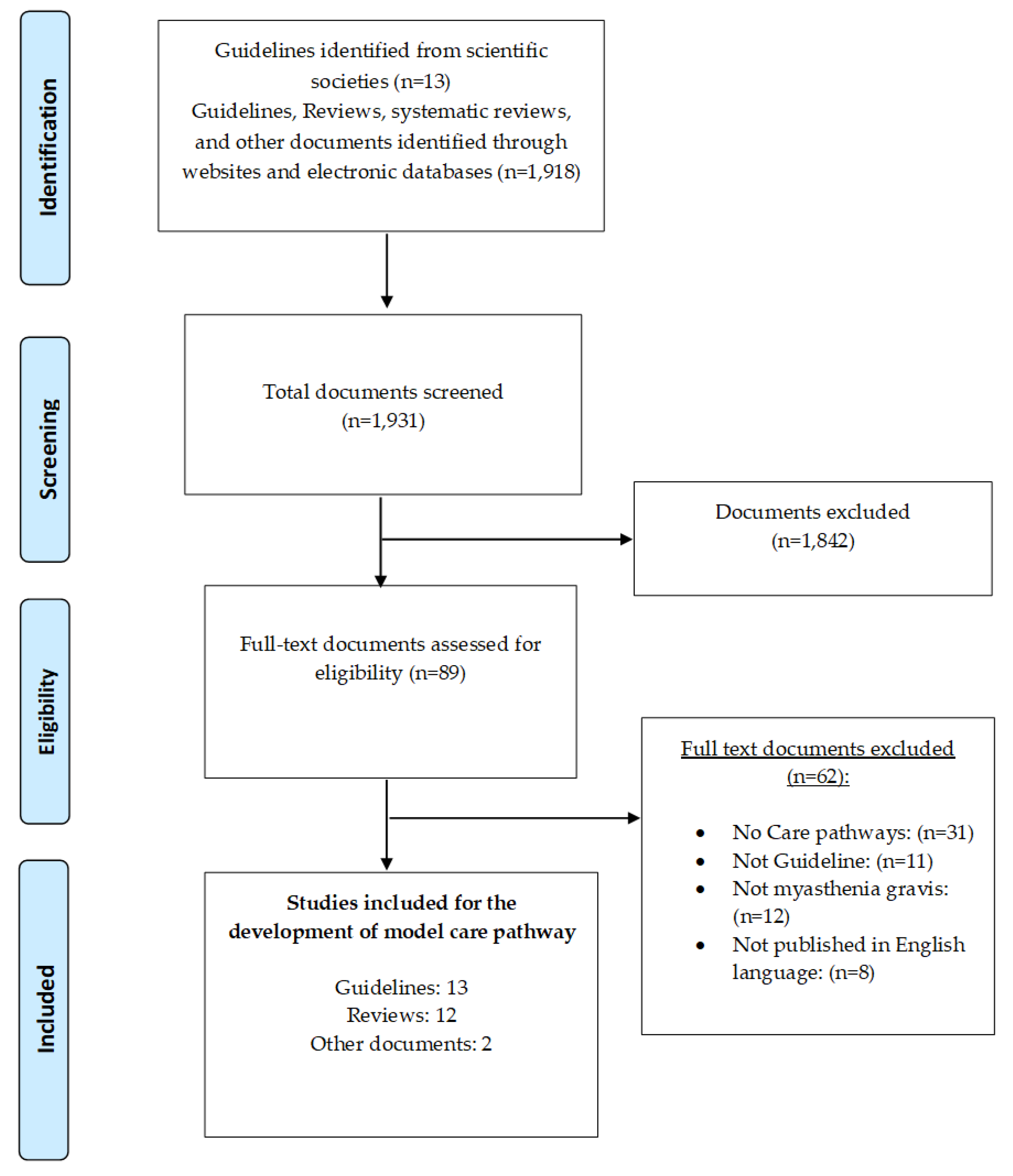
2.1.2. Selection of the Studies
2.1.3. Quality Assessment of the Studies
2.2. Process Analysis and Care Pathway (CP) Design
2.2.1. Identification of the Core Activities
- Class-A: evidence provided by a systematic review (SR) or randomized controlled trial (RCT).
- Class-B: evidence provided by a review or observational study (prospective, retrospective, case-control) or controlled trial or RCT with limitations.
- Class-C: evidence provided by an expert opinion (EO) or consensus or good practice point (GPP).
2.2.2. Definition of the Process-Flow
2.3. Care Pathway Validation
2.3.1. Recruitment of the Experts
2.3.2. Execution of the Delphi Study
2.3.3. Evaluation of Data and Performance of Statistical Analysis
2.4. Care Pathway Implementation Tools
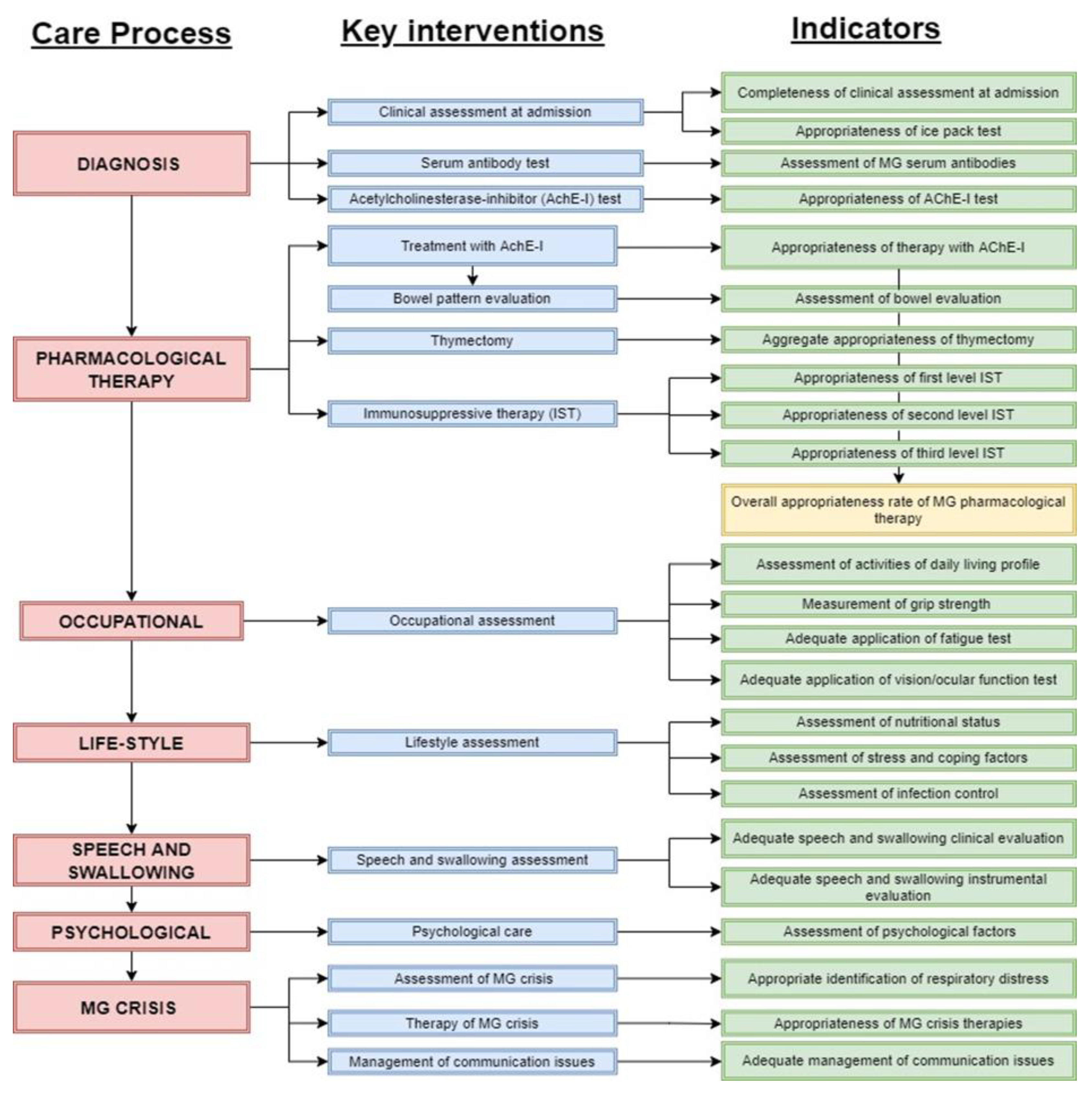
2.4.1. Definition of the Key Interventions
2.4.2. Development of the Process Indicators
3. Results
3.1. Literature Review and Assessment
3.2. Process Analysis and CP Design
3.3. CP Validation
3.4. CP Implementation Tools
4. Discussion
- Model CP: The model care pathway is based on the available international and national evidence. It is not specific to any organization.
- Operational/Local CP: The operational pathway is the pathway developed by a specific organization based on the information from the model care pathway and specific organization characteristics (available competences, resources, etc.) Because of the differences between organizations, this pathway is organization specific.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kinsman, L.; Rotter, T.; James, E.; Snow, P.; Willis, J. What is a clinical pathway? Development of a definition to inform the debate. BMC Med. 2010, 8, 8–10. [Google Scholar] [CrossRef] [Green Version]
- Vanhaecht, K.; Panella, M.; van Zelm, R.; Sermeus, W. An overview on the history and concept of care pathways as complex interventions. Int. J. Care Pathw. 2010, 14, 117–123. [Google Scholar] [CrossRef]
- Vanhaecht, K. The Impact of Clinical Pathways on the Organisation of Care Processes. Ph.D. Dissertation, The Katholieke Universiteit Leuven (KU Leuven), Leuven, Belgium, 2007. [Google Scholar]
- Schrijvers, G.; van Hoorn, A.; Huiskes, N. The Care Pathway: Concepts and Theories: An introduction. Int. J. Integr. Care 2012. (Published Online First: 2011). [Google Scholar] [CrossRef]
- Grol, R.; Grimshaw, J. From best evidence to best practice: Effective implementation of change in patients’ care. Lancet 2003, 362, 1225–1230. [Google Scholar] [CrossRef]
- Teisberg, E.; Wallace, S.; O’Hara, S. Defining and implementing value-based health care: A strategic framework. Acad. Med. 2020, 95, 682–685. [Google Scholar] [CrossRef]
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Seys, D.; Bruyneel, L.; Deneckere, S.; Kul, S.; Veken, L.V.D.; Zelm, R.V.; Sermeus, W.; Panella, M.; Vanhaecht, K. Better organized care via care pathways: A multicenter study. PLoS ONE 2017, 12, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutman, L.; Klein, E.J.; Brown, J.C. Clinical pathway produces sustained improvement in acute gastroenteritis care. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, S.-G.A.; Devitt, K.S.; Kagedan, D.J.; Barretto, B.; Tung, S.; Gallinger, S.; Wei, A.C. The impact of a clinical pathway on patient postoperative recovery following pancreaticoduodenectomy. HPB 2017, 19, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Pound, C.M.; Gelt, V.; Akiki, S.; Eady, K.; Moreau, K.; Momoli, F.; Murchison, B.; Zemek, R.; Mulholland, B.; Kovesi, T. Nurse-driven clinical pathway for inpatient asthma: A randomized controlled trial. Hosp. Pediatr. 2017, 7, 204–213. [Google Scholar] [CrossRef] [Green Version]
- Rotter, T.; Kinsman, L.; James, E.L.; Machotta, A.; Gothe, H.; Willis, J.; Snow, P.; Kugler, J. Clinical pathways: Effects on professional practice, patient outcomes, length of stay and hospital costs. Int. J. Evid. Based Healthc. 2011, 9, 191–192. [Google Scholar] [CrossRef]
- Kalmet, P.H.S.; Koc, B.B.; Hemmes, B.; Ten Broeke, R.H.M.; Dekkers, G.; Hustinx, P.M.D.; Schotanus, M.G.; Tilman, P.; Janzing, H.M.J.; Verkeyn, J.M.A.; et al. Effectiveness of a multidisciplinary clinical pathway for elderly patients with hip fracture. Geriatr. Orthop. Surg. Rehabil. 2016, 7, 81–85. [Google Scholar] [CrossRef] [Green Version]
- Barbieri, A.; Vanhaecht, K.; Van, H.P.; Sermeus, W.; Faggiano, F.; Marchisio, S.; Panella, M. Effects of clinical pathways in the joint replacement: A meta-analysis. BMC Med. 2009, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Hughes, D.; Richter, T.; Nestler-Parr, S.; Babela, R.; Khan, Z.M.; Tesoro, T.; Molsen, E.; Hughes, D.A. Rare disease terminology and definitions-A systematic global review: Report of the ISPOR rare disease special interest group. Value Health 2015, 18, 906–914. [Google Scholar] [CrossRef] [Green Version]
- Dunand, M.; Botez, S.A.; Borruat, F.X.; Roux-Lombard, P.; Spertini, F.; Kuntzer, T. Unsatisfactory outcomes in myasthenia gravis: Influence by care providers. J. Neurol. 2010, 257, 338–343. [Google Scholar] [CrossRef] [Green Version]
- Clinical Overview of MG. Available online: https://myasthenia.org/Professionals/Clinical-Overview-of-MG (accessed on 22 July 2021).
- Carr, A.S.; Cardwell, C.R.; McCarron, P.O.; Conville, J.M. A systematic review of population based epidemiological studies in Myasthenia Gravis. BMC Neurol. 2010, 10. [Google Scholar] [CrossRef] [Green Version]
- Boldingh, M.I.; Maniaol, A.H.; Brunborg, C.; Dekker, L.; Heldal, A.T.; Lipka, A.F.; Popperud, T.H.; Niks, E.H.; Verschuuren, J.J.G.M.; Tallaksen, C.M.E. Geographical distribution of myasthenia gravis in northern Europe—Results from a population-based study from two countries. Neuroepidemiology 2015, 44, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, A.; Clover, L.; Buckley, C.; Evans, J.G.; Rothwell, P.M. Evidence of underdiagnosis of myasthenia gravis in older people. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1105–1108. [Google Scholar] [CrossRef] [Green Version]
- Al-Asmi, A.; Nandhagopal, R.; Jacob, P.C.; Gujjar, A. Misdiagnosis of myasthenia gravis and subsequent clinical implication: A case report and review of literature. Sultan Qaboos Univ. Med. J. 2012, 12, 654–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshal, M.; Mustafa, M.; Crowley, P.; McGovern, R.; Ahern, E.; Ragab, I. Misdiagnosis of myasthenia gravis presenting with tongue and palatal weakness. Oxf. Med. Case Rep. 2018, 2018, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Alshekhlee, A.; Miles, J.D.; Katirji, B.; Preston, D.C.; Kaminski, H.J. Incidence and mortality rates of myasthenia gravis and myasthenic crisis in US hospitals. Neurology 2009, 72, 1548–1554. [Google Scholar] [CrossRef]
- Heatwole, C.; Johnson, N.; Holloway, R.; Noyes, K. Plasma exchange versus intravenous immunoglobulin for myasthenia gravis crisis: An acute hospital cost comparison study. J. Clin. Neuromuscul. Dis. 2011, 13, 85–94. [Google Scholar] [CrossRef]
- Kerty, E.; Elsais, A.; Argov, Z.; Evoli, A.; Gilhus, N.E. EFNS/ENS Guidelines for the treatment of ocular myasthenia. Eur. J. Neurol. 2014, 21, 687–693. [Google Scholar] [CrossRef]
- Sussman, J.; Farrugia, M.E.; Maddison, P.; Hill, M.; Leite, M.I.; Jones, D.H. Myasthenia gravis: Association of british neurologists’ management guidelines. Pract. Neurol. 2015, 15, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Stetefeld, H.; Schroeter, M. SOP myasthenic crisis. Neurol. Res. Pract. 2019, 1, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Mantegazza, R.; Antozzi, C. When myasthenia gravis is deemed refractory: Clinical signposts and treatment strategies. Ther. Adv. Neurol. Disord. 2018, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. Can. Med. Assoc. J. 2010, 182, 839–842. [Google Scholar] [CrossRef] [Green Version]
- AGREE II Training Tools. Available online: https://www.agreetrust.org/resource-centre/agree-ii/agree-ii-training-tools/ (accessed on 1 September 2020).
- Brainin, M.; Barnes, M.P.; Baron, J.C.; Gilhus, N.E.; Hughes, R.; Selmaj, K.; Waldemar, G. Guidance for the preparation of neurological management guidelines by EFNS scientific task forces: Revised recommendations 2004. Eur. J. Neurol. 2004, 9, 577–581. [Google Scholar] [CrossRef]
- io.draw. Available online: https://app.diagrams.net/ (accessed on 30 November 2020).
- M3 Global Research. Available online: https://www.m3globalresearch.com/ (accessed on 5 September 2020).
- Grime, M.M.; Wright, G. Delphi Method. In Wiley StatsRef: Statistics Reference Online; Balakrishnan, N., Colton, T., Everitt, B., Piegorsch, W., Ruggeri, F., Teugels, J.L., Eds.; Wiley—Blackwell: Hoboken, NJ, USA, 2014. [Google Scholar]
- Non-Response Bias: A Bias That Occurs Due to Systematic Differences between Responders and Non-Responders. Available online: https://catalogofbias.org/biases/non-response-bias/ (accessed on 24 October 2021).
- SoGoSurvey. Available online: https://www.sogosurvey.com/help/how-to-calculate-overall-score-in-omni/ (accessed on 6 April 2021).
- Vanhaecht, K.; Gerven, E.V.; Deneckere, S.; Lodewijckx, C.; Janssen, I.; Zelm, R.V.; Boto, P.; Mendes, R.V.; Panella, M.; Biringer, E.; et al. The 7-phase method to design, implement and evaluate care pathways. Int. J. Pers. Cent. Med. 2012, 2, 341–351. [Google Scholar]
- Lodewijckx, C.; Decramer, M.; Sermeus, W.; Panella, M.; Deneckere, S.; Vanhaecht, K. Eight-step method to build the clinical content of an evidence-based care pathway: The case for COPD exacerbation. Trials 2012, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- European Pathway Association. Available online: https://e-p-a.org/ (accessed on 1 March 2021).
- The Joint Commission. Available online: https://manual.jointcommission.org/releases/TJC2022A/MIF0344.html (accessed on 5 November 2020).
- Agency for Healthcare Research and Quality. Available online: https://qualityindicators.ahrq.gov/ (accessed on 2 November 2020).
- Sanders, D.B.; Wolfe, G.I.; Benatar, M.; Evoli, A.; Gilhus, N.E.; Illa, I.; Kuntz, N.; Massey, J.M.; Melms, A.; Murai, H.; et al. International consensus guidance for management of myasthenia gravis. Neurology 2016, 87, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Freeman, C. Evidence-based guideline update: Plasmapheresis in neurologic disorders. Neurology 2011, 77, 294–301. [Google Scholar] [CrossRef]
- Patwa, H.S.; Chaudhry, V.; Katzberg, H.; Rae-Grant, A.D.; So, Y.T. Evidence-based guideline: Intravenous immunoglobulin in the treatment of neuromuscular disorders. Neurology 2012, 78, 1009–1015. [Google Scholar] [CrossRef] [Green Version]
- Chiou-Tan, F.Y.; Gilchrist, J.M. Repetitive nerve stimulation and single-fiber electromyography in the evaluation of patients with suspected myasthenia gravis or Lambert-Eaton myasthenic syndrome. Muscle Nerve 2015, 52, 455–462. [Google Scholar] [CrossRef]
- Gronseth, G.S.; Barohn, R.J. Practice parameter: Thymectomy for autoimmune myasthenia gravis (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000, 55, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Fowler, S.B. Care of The Patient with Myasthenia Gravis; American Association of Neuroscience Nurses: Chicago, IL, USA, 2014. [Google Scholar]
- Skeie, G.O.; Apostolski, S.; Evoli, A.; Gilhus, N.E.; Illa, I.; Harms, L.; Hilton-Jones, D.; Melms, A.; Verschuuren, J.; Horge, H.W. Guidelines for treatment of autoimmune neuromuscular transmission disorders. Eur. J. Neurol. 2010, 17, 893–902. [Google Scholar] [CrossRef]
- Elovaara, I.; Apostolski, S.; Van, D.P.; Gilhus, N.E.; Hietaharju, A.; Honkaniemi, J.; Schaik, I.N.V.; Scolding, N.; Soelberg, P.; Sørensen, N.; et al. EFNS guidelines for the use of intravenous immunoglobulin in treatment of neurological diseases. Eur. J. Neurol. 2008, 15, 893–908. [Google Scholar] [CrossRef]
- Norwood, F.; Dhanjal, M.; Hill, M.; James, N.; Jungbluth, H.; Kyle, P.; O’Sullivan, G.; Palace, J.; Robb, S.; Williamson, C.; et al. Myasthenia in pregnancy: Best practice guidelines from a UK multispecialty working group. J. Neurol. Neurosurg. Psychiatry 2014, 85, 538–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donofrio, P.D.; Berger, A.; Brannagan, T.H.; Bromberg, M.B.; Howard, J.F.; Latov, N.; Quick, A.; Tandan, R. Consensus statement: The use of intravenous immunoglobulin in the treatment of neuromuscular conditions. Muscle Nerve 2009, 40, 890–900. [Google Scholar] [CrossRef]
- Murai, H. Japanese clinical guidelines for myasthenia gravis: Putting into practice. Clin. Exp. Neuroimmunol. 2015, 6, 21–31. [Google Scholar] [CrossRef]
- Godoy, D.A.; de Mello, L.J.V.; Masotti, L.; Napoli, D.I.M. The myasthenic patient in crisis: An update of the management in Neurointensive care unit. Arq. Neuropsiquiatr. 2013, 71, 627–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farmakidis, C.; Pasnoor, M.; Dimachkie, M.M.; Barohn, R.J. Treatment of myasthenia gravis. Neurol. Clin. 2018, 36, 311–337. [Google Scholar] [CrossRef]
- Gilhus, N.E.; Verschuuren, J.J. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015, 14, 1023–1036. [Google Scholar] [CrossRef]
- Gilhus, N.E. Myasthenia gravis. N. Engl. J. Med. 2016, 375, 2570–2581. [Google Scholar] [CrossRef]
- Gilhus, N.E.; Tzartos, S.; Evoli, A.; Palace, J.; Burns, T.M.; Verschuuren, J.J.G.M. Myasthenia gravis. Nat. Rev. Dis. Prim. 2019, 5, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Sathasivam, S. Diagnosis and management of myasthenia gravis. Prog. Neurol. Psychiatry 2014, 18, 6–14. [Google Scholar] [CrossRef]
- Jacob, S. Myasthenia gravis—A review of current therapeutic options. Eur. Neurol. Rev. 2018, 13, 86–92. [Google Scholar] [CrossRef]
- Kim, J.Y.; Park, K.D.; Richman, D.P. Treatment of myasthenia gravis based on its immunopathogenesis. J. Clin. Neurol. 2011, 7, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Meriggioli, M.N.; Sanders, D.B. Autoimmune myasthenia gravis: Emerging clinical and biological heterogeneity. Lancet Neurol. 2009, 8, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Muppidi, S. Outcome measures in myasthenia gravis: Incorporation into clinical practice. J. Clin. Neuromuscul. Dis 2017, 18, 135–146. [Google Scholar] [CrossRef]
- Howard, J.F. Myasthenia Gravis: A Manual for the Health Care Provider, 1st ed.; Myasthenia Gravis Foundation of America: New York, NY, USA, 2009. [Google Scholar]
- Evoli, A. Myasthenia gravis: New developments in research and treatment. Curr. Opin. Neurol. 2017, 30, 464–470. [Google Scholar] [CrossRef]
- Myasthenia Gravis: Delphi Study. Available online: https://www.sogosurvey.com/preview.aspx?k=YsQUWYUsUV&status=preview (accessed on 2 November 2020).
- De Luc, K. Developing Care Pathways, National Pathways Association; Radcliffe Medical Press: Oxford, MS, USA, 2000. [Google Scholar] [CrossRef]
- Miravitlles, M.; Vogelmeier, C.; Roche, N.; Halpin, D.; Cardoso, J.; Chuchalin, A.G.; Kankaanranta, H.; Sandström, T.; Śliwiński, P.; Zatloukal, J.; et al. A review of national guidelines for management of COPD in Europe. Eur. Respir. J. 2016, 47, 625–637. [Google Scholar] [CrossRef] [Green Version]
- Greengold, N.L.; Weingarten, S.R. Developing evidence-based practice guidelines and pathways: The Experience at the local hospital level. Jt. Comm. J. Qual. Improv. 1996, 22, 391–402. [Google Scholar] [CrossRef]
- Vanhaecht, K.; De, W.K.; Sermeus, W. The care process organization triangle: A framework to better understand how clinical pathways work. J. Integr. Care Pathw. 2007, 11, 54–61. [Google Scholar] [CrossRef]
- Montalban, X.; Gold, R.; Thompson, A.J.; Otero-Romero, S.; Amato, M.P.; Chandraratna, D.; Clanet, M.; Comi, G.; Derfuss, T.; Fazekas, F.; et al. ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis. Eur. J. Neurol. 2018, 25, 215–237. [Google Scholar] [CrossRef] [Green Version]
- Perry, M.; Swain, S.; Kemmis-Betty, S.; Cooper, P. Multiple sclerosis: Summary of NICE guidance. BMJ 2014, 349, 6–11. [Google Scholar] [CrossRef]
- Rotter, T.; Kinsman, L.; James, E.; Machotta, A.; Steyerberg, E.W. The Quality of the evidence base for clinical pathway effectiveness: Room for improvement in the design of evaluation trials. BMC Med. 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Ramos, M.; Ratliff, C. The development and implementation of an integrated multidisciplinary clinical pathway. J. Wound Ostomy Cont. Nurs. 1997, 24, 66–71. [Google Scholar] [CrossRef]
- Ridic, G.; Gleason, S.; Ridic, O. Comparisons of health care systems in the United States, Germany and Canada. Mater Socio Medica 2012, 24, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakubowski, E.; Busse, R. Health Care Systems in the EU: A Comparative Study; European Parliament: Luxembourg, 1998. [Google Scholar]
- Landfeldt, E.; Pogoryelova, O.; Sejersen, T.; Zethraeus, N.; Breiner, A.; Lochmüller, H. Economic costs of myasthenia gravis: A Systematic Review. Pharmacoeconomics 2020, 38, 715–728. [Google Scholar] [CrossRef]
- Newton, L. Allocation of health care resources: Principles for decision-making. Pediatr. Rev. 2017, 38, 320–329. [Google Scholar] [CrossRef]
- Abrahams, E.; Balch, A.; Goldsmith, P.; Kean, M.; Miller, A.M.; Omenn, G.; Sonet, E.; Sprandio, J.; Tyne, C.; Westrich, K. Clinical pathways: Recommendations for putting patients at the center of value-based care. Clin. Cancer Res. 2017, 23, 4545–4549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deneckere, S.; Euwema, M.; Van, H.P.; Lodewijckx, C.; Panella, M.; Sermeus, W.; Vanhaecht, K. Care pathways lead to better teamwork: Results of a systematic review. Soc. Sci. Med. 2012, 75, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Deneckere, S.; Euwema, M.; Lodewijckx, C.; Panella, M.; Mutsvari, T.; Sermeus, W.; Vanhaecht, K. Better interprofessional teamwork, higher level of organized care, and lower risk of burnout in acute health care teams using care pathways: A cluster randomized controlled trial. Med. Care 2013, 51, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Aeyels, D.; Bruyneel, L.; Seys, D.; Sinnaeve, P.R.; Sermeus, W.; Panella, M.; Vanhaecht, K. Better hospital context increases success of care pathway implementation on achieving greater teamwork: A multicenter study on STEMI care. Int. J. Qual. Health Care 2019, 31, 442–448. [Google Scholar] [CrossRef]
- Vanhaecht, K.; Panella, M.; Zelm, R.V.; Sermeus, W. What about care pathways? In Care of the Dying: A Pathway to Excellence; Ellershaw, J., Wilkinson, S., Eds.; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Talarico, R.; Cannizzo, S.; Lorenzoni, V.; Marinello, D.; Palla, I.; Pirri, S.; Ticciati, S.; Trieste, L.; Triulzi, I.; Terol, E.; et al. RarERN Path: A methodology towards the optimisation of patients’ care pathways in rare and complex diseases developed within the European Reference Networks. Orphanet J. Rare Dis. 2020, 15, 1–10. [Google Scholar] [CrossRef]
- Tumiene, B.; Graessner, H. Rare disease care pathways in the EU: From odysseys and labyrinths towards highways. J. Community Genet. 2021, 12, 231–239. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sub Process | Clinical Activities (n = 60) | LOE | Expert Opinions | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Completeness Rates | Appropriateness Rates | |||||||||||
| A | B | C | Overall (n = 85) | USA (n = 43) | EU (n = 35) | JPN (n = 7) | Overall (n = 85) | USA (n = 43) | EU (n = 35) | JPN (n = 7) | ||
| (1) Diagnostic process | 10 | - | 3 | 7 | 95.3% | 95.3% | 97.1% | 85.7% | 84.7% | 88.4% | 80.0% | 85.7% |
| (2) Pharmacological management process | 12 | 6 | 3 | 3 | 90.6% | 88.4% | 97.1% | 71.4% | 83.5% | 83.7% | 82.9% | 85.7% |
| (3) Speech, Swallowing and Dental management process | 6 | - | 2 | 4 | 90.6% | 93.0% | 94.3% | 57.1% * | 88.2% | 88.4% | 91.4% | 71.4% |
| (4) Occupational, Physical and Respiratory management process | 13 | - | 2 | 11 | 92.9% | 95.3% | 91.4% | 85.7% | 89.4% | 88.4% | 91.4% | 85.7% |
| (5) Psychological management process | 8 | - | - | 8 | 85.9% | 81.4% | 88.6% | 100.0% | 88.2% | 86.0% | 91.4% | 85.7% |
| (6) Life-style management process | 6 | - | 2 | 4 | 90.6% | 88.4% | 94.3% | 85.7% | 89.4% | 90.7% | 88.6% | 85.7% |
| (7) MG crisis management process | 5 | 2 | 2 | 1 | 89.4% | 90.7% | 91.4% | 71.4% | 89.4% | 93.0% | 85.7% | 85.7% |
| Average of sub processes | 90.8% | 90.4% | 93.5% | 79.6% | 87.6% | 88.4% | 87.3% | 83.7% | ||||
| Sub Process | Setting | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ambulatory Care | Hospital Day Care | Hospital in-Patient | LTC (Nursing Home) | LTC (Rehabilitation) | ||||||||||||||||
| Overall (n = 85) | USA (n = 43) | EU (n = 35) | JPN (n = 7) | Overall (n = 85) | USA (n = 43) | EU (n = 35) | JPN (n = 7) | Overall (n = 85) | USA (n = 43) | EU (n = 35) | JPN (n = 7) | Overall (n = 85) | USA (n = 43) | EU (n = 35) | JPN (n = 7) | Overall (n = 85) | USA (n = 43) | EU (n = 35) | JPN (n = 7) | |
| (1) Dx | 51.8% | 72.1% | 22.9% 1 | 71.4% | 15.8% | 16.3% | 17.1% | 0.0% | 45.9% | 30.2% | 68.6% 2 | 28.6% | 2.4% | 4.7% | 0.0% | 0.0% | 4.7% | 7.0% | 2.9% | 0.0% |
| (2) Ph Tx | 55.3% | 81.4% | 22.9% 3 | 57.1% | 20.0% | 14.0% | 31.4% | 0.0% | 41.2% | 23.3% 4 | 60.0% | 57.1% | 5.9% | 9.3% | 2.9% | 0.0% | 3.5% | 4.7% | 2.9% | 0.0% |
| (3) SSD | 56.5% | 65.1% | 45.7% | 57.1% | 22.4% | 18.6% | 25.7% | 28.6% | 41.2% | 30.2% | 51.4% | 57.1% | 20.0% | 27.9% | 8.6% | 28.6% | 18.8% | 18.6% | 14.3% | 42.9% |
| (4) OPR | 63.5% | 74.4% | 54.3% | 42.9% | 22.4% | 16.3% | 25.7% | 42.9% | 23.5% | 18.6% | 28.6% | 28.6% | 17.6% | 25.6% | 5.7% 5 | 28.6% | 20.0% | 23.3% | 11.4% | 42.9% |
| (5) PAM | 72.9% | 79.1% | 62.9% | 85.7% | 18.8% | 14.0% | 25.7% | 14.3% | 25.9% | 20.9% | 34.3% | 14.3% | 17.6% | 23.3% | 8.6% | 28.6% | 14.1% | 14.0% | 14.3% | 14.3% |
| (6) LAM | 72.9% | 83.7% | 57.1% 6 | 85.7% | 21.2% | 14.0% | 28.6% | 28.6% | 24.7% | 25.6% | 25.7% | 14.3% | 22.4% | 30.2% | 11.4% | 28.6% | 17.6% | 16.3% | 20.0% | 14.3% |
| (7) M crisis | 24.7% | 25.6% | 20.0% | 42.9% | 15.3% | 14.0% | 20.0% | 0.0% | 72.9% | 72.1% | 74.3% | 71.4% | 5.9% | 7.0% | 2.9% | 14.3% | 4.7% | 2.3% | 5.7% | 14.3% |
| Average | 56.8% | 68.8% | 40.8% | 63.3% | 19.3% | 15.3% | 24.9% | 16.3% | 39.3% | 31.6% | 49.0% | 38.8% | 13.1% | 18.3% | 5.7% | 18.4% | 11.9% | 12.3% | 10.2% | 18.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Payedimarri, A.b.; Ratti, M.; Rescinito, R.; Vasile, A.; Seys, D.; Dumas, H.; Vanhaecht, K.; Panella, M. Development of a Model Care Pathway for Myasthenia Gravis. Int. J. Environ. Res. Public Health 2021, 18, 11591. https://doi.org/10.3390/ijerph182111591
Payedimarri Ab, Ratti M, Rescinito R, Vasile A, Seys D, Dumas H, Vanhaecht K, Panella M. Development of a Model Care Pathway for Myasthenia Gravis. International Journal of Environmental Research and Public Health. 2021; 18(21):11591. https://doi.org/10.3390/ijerph182111591
Chicago/Turabian StylePayedimarri, Anil babu, Matteo Ratti, Riccardo Rescinito, Alessandra Vasile, Deborah Seys, Hervé Dumas, Kris Vanhaecht, and Massimiliano Panella. 2021. "Development of a Model Care Pathway for Myasthenia Gravis" International Journal of Environmental Research and Public Health 18, no. 21: 11591. https://doi.org/10.3390/ijerph182111591
APA StylePayedimarri, A. b., Ratti, M., Rescinito, R., Vasile, A., Seys, D., Dumas, H., Vanhaecht, K., & Panella, M. (2021). Development of a Model Care Pathway for Myasthenia Gravis. International Journal of Environmental Research and Public Health, 18(21), 11591. https://doi.org/10.3390/ijerph182111591