
Virtual Reality in the Treatment of Adults with Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomized Clinical Trials


 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Methodological Quality of Included Studies
2.6. Risk of Bias of Included Studies
2.7. Statistical Analysis
3. Results
3.1. Search Selection
3.2. Characteristics of Included Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) [Ref.] | Country | Sample Size | Age (Years) Mean ± SD | Gender (% Males) | Outcome Measures | Measuring Instrument | Time Points Assessment | Quality |
|---|---|---|---|---|---|---|---|---|
| Park et al. (2013) [26] | South Korea | n = 24 EG1:8 EG2: 8 CG: 8 | EG1: 44.12 ± 5.48 EG2: 43.37 ± 5.42 CG: 45.50 ± 5.34 | 100 | Pain intensity Back strength Functional balance Health status | VAS Isometric lifting strength One-legged stand test RAND-36 | Pre-intervention Post-intervention | 16 |
| Oh et al. (2014) [27] | South Korea | n = 37 EG1: 10 EG2: 9 EG3: 9 CG: 9 | EG1: 20.56 ± 0.69 EG2: 20.33 ± 0.52 EG3: 20.44 ± 0.27 CG: 20.70 ± 0.37 | 100 | Pain intensity Body composition Isokinetic trunk flexion/extension Isokinetic hip flexion/extension and ABD/ADD | VAS Bioelectrical impedance analysis method and anthropometer Isokinetic dynamometer Isokinetic dynamometer | Pre-intervention Post-intervention | 15 |
| Yoo et al. (2014) [28] | South Korea | n = 47 EG: 24 CG: 23 | EG: 20.44 ± 1.33 CG: 20.70 ± 1.45 | 100 | Pain intensity Body composition Isokinetic trunk flexion/extension | VAS Bioelectrical impedance analysis method Isokinetic dynamometer | Pre-intervention Post-intervention | 17 |
| Monteiro-Junior et al. (2015) [32] | Brazil | n = 30 EG: 16 CG: 14 | 68 ± 4 | 0 | Pain intensity Static balance Functional capacity Mood | 11-NPRS Wii balance board Sit-to-stand test POMS | Pre-intervention Post-intervention | 21 |
| Chen et al. (2016) [29] | South Korea | n = 19 EG: 10 CG: 9 | 19-30 | - | Pain intensity Disability associated with low back pain Dynamic balance | VAS KODI LoS test with Biorescue | Pre-intervention Post-intervention | 13 |
| Zadro et al. (2019) [7] | Australia | n = 60 EG: 30 CG: 30 | EG: 68.8 ± 5.5 CG: 67.8 ± 6 | EG: 20 CG: 28.3 | Pain self-efficacy Care-seeking Physical activity Pain intensity Function changes Severity of disability Kinesiophobia Falls efficacy | 10-PSEQ 3-items questionnaire The Rapid Assessment of Physical Activity Questionnaire 11-NPRS PSFS RMDQ 17-TSK FEQ-I | Pre-intervention Post-intervention 3 months follow-up 6 months follow-up | 26 |
| Kim et al. (2020) [30] | South Korea | n = 48 EG: 24 CG: 24 | EG: 26 ± 3.82 CG: 28.79 ± 9.05 | EG: 68.2 CG: 42.3 | Pain intensity Disability associated with low back pain Severity of disability Fear and avoidance beliefs | 11-NPRS ODI RMDQ FABQ | Pre-intervention 4 weeks Post-intervention 6 months follow-up | 22 |
| Nambi et al. (2020) A [34] | Saudi Arabia | n = 45 EG1: 15 EG2: 15 CG: 15 | EG1: 21.25 ± 1.2 EG2: 20.23 ± 1.6 CG: 20.78 ± 1.6 | 100 | Pain intensity Player wellness Sprint performance: - 40 m sprint and 4 × 5 m sprint - Submaximal shuttle running Jump performance: CJ and SJ | VAS Player wellness questionnaire Photocell timer MEMS device Optical timing system | Pre-intervention Post-intervention 8 weeks follow-up 6 months follow-up | 25 |
| Nambi et al. (2020) B [35] | Saudi Arabia | n = 60 EG1: 20 EG2:20 CG:20 | EG1: 23.2 ± 1.5 EG2: 22.8 ± 1.6 CG: 23.3 ± 1.5 | 100 | Pain intensity Kinesiophobia Blood serum levels of stress hormones | VAS 17-TSK 20 ml venous blood sample | Pre-intervention Post-intervention 6 months follow-up | 24 |
| Park et al. (2020) [31] | South Korea | n = 80 EG: 40 CG:40 | EG: 71.50 ± 6.34 CG: 72.05 ± 6.82 | 0 | Pain intensity Disability associated with low back pain Isokinetic trunk flexion/extension Body composition Spinal alignment | VAS ODI Isokinetic dynamometer Bioelectrical impedance analysis method Raster stereography | Pre-intervention Post-intervention | 21 |
| Tomruk et al. (2020) [37] | Turkey | n = 42 EG: 21 CG: 21 | Median (IQR) EG: 46 (40.05-50.50) CG: 45 (44-48) | - | Pain intensity Disability associated with low back pain Postural control Physical activity | 11-NPRS ODI LoS PS tests by Biodex Balance System SenseWear Armband | Pre-intervention Post-intervention | 18 |
| García et al. (2021) [33] | USA | n = 179 EG: 89 CG: 90 | EG: 51.5 ± 13.5 CG: 51.4 ± 12.9 | EG: 25 CG: 21 | Pain intensity Pain interference Patient’s global impression of change Physical function and sleep disturbances Pain catastrophizing Pain self-efficacy Chronic pain acceptance Satisfaction with treatment VR device use System usability Over-the-counter analgesic medication use Opioid use data | DVPRS DVPRS-II Question and 7-point scale ranging PROMIS PCS PSEQ-2 CPAG-8 6-point scale Device SUS Question yes/no Self-reported | Pre-intervention During intervention Post-intervention | 27 |
| Nambi et al. (2021) [36] | Saudi Arabia | n = 54 EG1: 18 EG2:18 CG:18 | EG1: 22.3 ± 1.6 EG2: 21.4 ± 1.8 CG: 21.9 ± 1.8 | 100 | Pain intensity Kinesiophobia Blood serum levels of hormones | VAS 17-TSK 20 ml venous blood sample | Pre-intervention Post-intervention 6 months follow-up | 24 |
| Sato et al. (2021) [38] | Japan | n = 40 EG: 20 CG: 20 | EG: 49.31 ± 12.59 CG: 55.61 ± 10.96 | EG: 45 CG: 40 | Pain intensity Buttock pain Leg numbness Body composition Left and right GS Pain self-efficacy Pain catastrophizing Kinesiophobia | VAS VAS VAS Bioelectrical impedance analysis method Dynamometer 10-PSEQ PCS 17-TSK | Pre-intervention Post-intervention | 22 |
3.3. Characteristics of Interventions
3.4. Methodological Quality of Included Studies
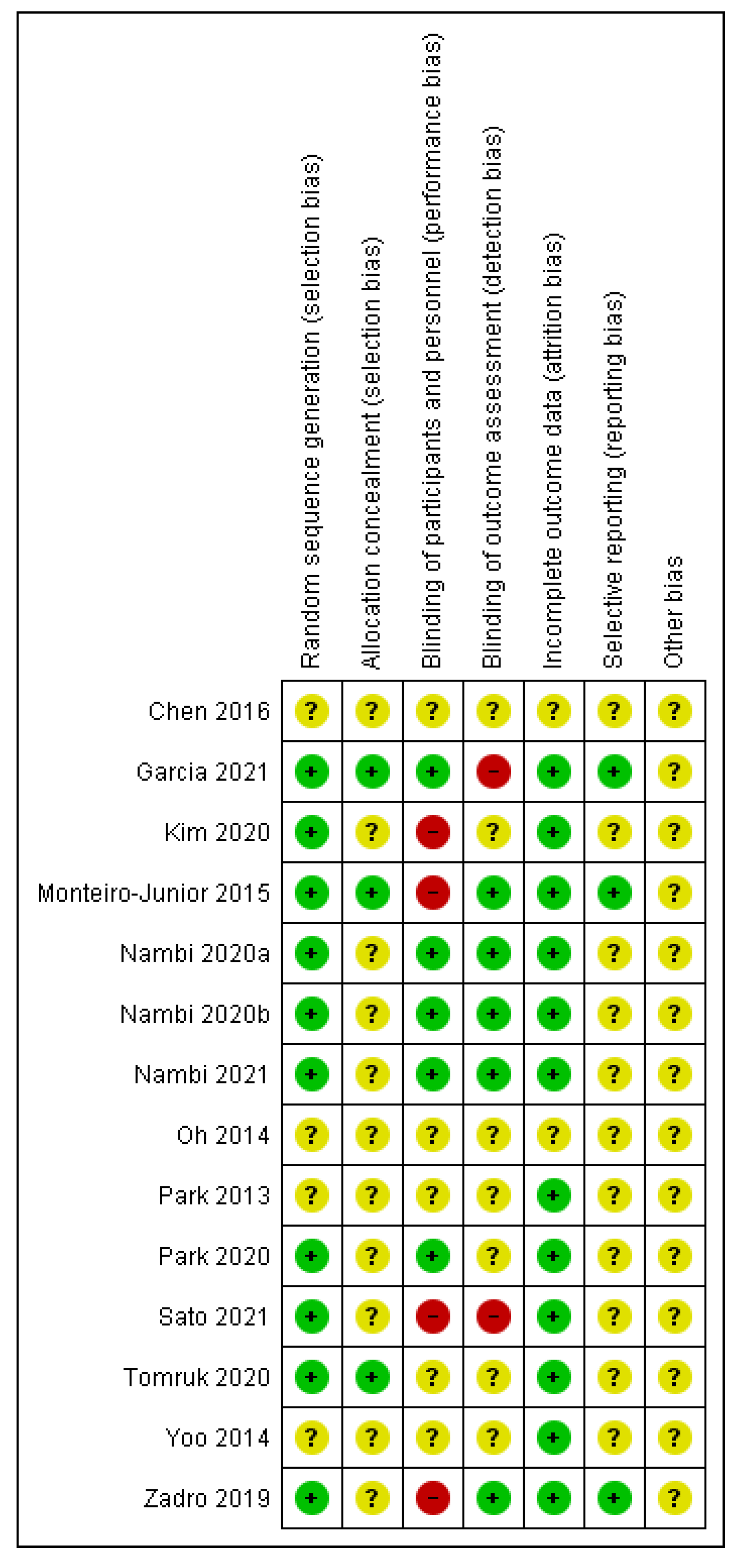
3.5. Risk of Bias of Included Studies
3.6. Effects of Virtual Reality vs. No Virtual Reality in Chronic Low Back Pain
3.6.1. Subgroup Based on Intervention Comparisons: Virtual Reality Alone or Combined with Physiotherapy vs. Control Group Interventions
3.6.2. Subgroups Based on Virtual Reality Interventions
3.6.3. Subgroups Based on the Duration of the Intervention
4. Discussion
4.1. Pain Intensity
4.2. Disability
4.3. Kinesiophobia
4.4. Virtual Reality in Other Populations
4.5. Discussion with Other Reviews
4.6. Strengths and Limitations
4.7. Clinical Implications for Practice
4.8. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Database | PubMed |
|---|---|
| Date | 05/08/2021 |
| Strategy | #1 AND #2 |
| #1 | (“back pain”[Mesh] OR “back pain” OR “low back pain”[Mesh] OR “backache” OR “spine pain” OR “spinal pain” OR “lumbago” OR “sciatica”) |
| #2 | (“Video Games”[Mesh] OR “video game*” OR “videogame*” OR “Gaming” OR “Game” OR “games” OR “Wii” OR “Nintendo” OR “Kinect” OR “Xbox” OR “PlayStation” OR “Virtual Reality”[Mesh] OR “virtual reality” OR “Virtual Reality Exposure Therapy”[Mesh] OR “exergame*” OR “gamification” OR “virtual” OR “computer-based” OR “augmented reality” OR “horse riding” OR “horseback” OR “hippotherapy simulator” OR “equine simulator”) |
| Database | Web of Science |
| Date | 05/08/2021 |
| Strategy | #1 AND #2 |
| #1 | TS = (“back pain”[Mesh] OR “back pain” OR “low back pain”[Mesh] OR “backache” OR “spine pain” OR “spinal pain” OR “lumbago” OR “sciatica”) |
| #2 | TS = (“Video Games”[Mesh] OR “video game*” OR “videogame*” OR “Gaming” OR “Game” OR “games” OR “Wii” OR “Nintendo” OR “Kinect” OR “Xbox” OR “PlayStation” OR “Virtual Reality”[Mesh] OR “virtual reality” OR “Virtual Reality Exposure Therapy”[Mesh] OR “exergame*” OR “gamification” OR “virtual” OR “computer-based” OR “augmented reality” OR “horse riding” OR “horseback” OR “hippotherapy simulator” OR “equine simulator”) |
| Database | Scopus |
| Date | 07/08/2021 |
| Strategy | #1 AND #2 |
| #1 | TITLE-ABS-KEY (“back pain” OR “low back pain” OR “backache” OR “spine pain” OR “spinal pain” OR “lumbago” OR “sciatica”) |
| #2 | TITLE-ABS-KEY (“video game*” OR “videogame*” OR “Gaming” OR “Game” OR “games” OR “Wii” OR “Nintendo” OR “Kinect” OR “Xbox” OR “PlayStation” OR “virtual reality” OR “Virtual Reality Exposure Therapy” OR “exergame*” OR “gamification” OR “virtual” OR “computer-based” OR “augmented reality” OR “horse riding” OR “horseback” OR “hippotherapy simulator” OR “equine simulator”) |
| Database | Cinahl |
| Data | 06/08/2021 |
| Strategy | #1 AND #2 |
| #1 | AB (“back pain”[Mesh] OR “back pain” OR “low back pain”[Mesh] OR “backache” OR “spine pain” OR “spinal pain” OR “lumbago” OR “sciatica”) |
| #2 | AB (“Video Games”[Mesh] OR “video game*” OR “videogame*” OR “Gaming” OR “Game” OR “games” OR “Wii” OR “Nintendo” OR “Kinect” OR “Xbox” OR “PlayStation” OR “Virtual Reality”[Mesh] OR “virtual reality” OR “Virtual Reality Exposure Therapy”[Mesh] OR “exergame*” OR “gamification” OR “virtual” OR “computer-based” OR “augmented reality” OR “horse riding” OR “horseback” OR “hippotherapy simulator” OR “equine simulator”) |
Appendix B
| Database | ClinicalTrials.gov |
|---|---|
| Date | 17/08/2021 |
| Strategy | (“back pain” OR “low back pain”) AND (“video games” OR “virtual reality” OR “virtual reality exposure therapy”) Filter: study type → interventional (clinical trial) |
| Database | ISRCTN registry |
| Date | 17/08/2021 |
| Strategy | “back pain” AND “virtual reality” “back pain” AND “virtual reality exposure therapy” “back pain” AND “video games” “low back pain” AND “virtual reality” “low pain” AND “virtual reality exposure therapy” “low back pain” AND “video games” |
| Database | ICTRP |
| Date | 28/08/2021 |
| Strategy | “back pain” AND “virtual reality” “back pain” AND “virtual reality exposure therapy” “back pain” AND “video games” “low back pain” AND “virtual reality” “low back pain” AND “virtual reality exposure therapy” “low back pain” AND “video games” |
Appendix C
| Article | Reason for Exclusion |
|---|---|
| Virtual Environment Rehabilitation for Patients with Motor Neglect Trial (VERMONT): A Single-Center Randomized Controlled Feasibility Trial | No chronic low back pain |
| Home-Based Balance Training Using the Wii Balance Board | No chronic low back pain |
| Interactive Sections of an Internet-Based Intervention Increase Empowerment of Chronic Back Pain Patients: Randomized Controlled Trial | No chronic low back pain |
| Response latencies to postural disturbances when using a virtual reality balance trainer or wobble board in persons with low back pain | No chronic low back pain treatment |
| Feasibility, Acceptability and Effects of a Home-Based Exercise Program Using a Gerontechnology on Physical Capacities After a Minor Injury in Community-Living Older Adults: A Pilot Study | No chronic low back pain |
| Effectiveness of Trunk Balance Exercises and Wii Fit TM Balance Exercises in Managing Disability and Pain in Patients with Chronic Low Back Pain | Not randomized trial |
| Serious Gaming During Multidisciplinary Rehabilitation for Patients With Chronic Pain or Fatigue Symptoms: Mixed Methods Design of a Realist Process Evaluation | Not randomized trial |
| Examining virtual reality gaming for pain-related fear and disability in chronic low back pain | Meeting abstract |
| Using Virtual Reality to Treat Chronic Pain: Virtual Graded Exposure for Chronic Low Back Pain and Virtual Walking for Persistent Neuropathic Pain in Spinal Cord Injury | Meeting abstract |
| Cost effectiveness of virtual reality game versus clinic based mckenzie extension therapy for chronic non specific low back pain | Meeting abstract |
| Modulating body-image in people with chronic back pain using virtual reality | Meeting abstract |
| Preliminary Feasibility of a Graded, Locomotor-Enabled, Whole-Body Virtual Reality Intervention for Individuals with Chronic Low Back Pain | Not randomized trial |
| RabbitRun: An Immersive Virtual Reality Game for Promoting Physical Activities Among People with Low Back Pain dagger | Not randomized trial |
| Virtual Reality Serious Game for Musculoskeletal Disorder Prevention | Not randomized trial |
| Exploring the role of pain-related fear and catastrophizing in response to a virtual reality gaming intervention for chronic low back pain | Meeting abstract |
| Effects of a Nintendo Wii exercise program versus Tai Chi Chuan on standing balance in older adults: a preliminary study | Not randomized trial |
| A novel, web-enabled multimedia approach, with 3D virtual reality internal and external human body tours, to support low back pain diagnosis | Not randomized trial |
| Low Back Pain Attenuation Employing Virtual Reality Physiotherapy | Not randomized trial |
| Mindfulness-based cognitive-behavior therapy (MCBT) versus virtual reality (VR) enhanced CBT, versus treatment as usual for chronic back pain. A clinical trial | Not randomized trial |
| A Portable Wireless Solution for Back Pain Telemonitoring: A 3D-Based, Virtual Reality Approach | Not randomized trial |
| Assessing the Perception of Trunk Movements in Military Personnel with Chronic Non-Specific Low Back Pain Using a Virtual Mirror | Not randomized trial |
| ALFRED Back Trainer: Conceptualization of a Serious Game-Based Training System for Low Back Pain Rehabilitation Exercises | Not randomized trial |
| A Virtual Reality Lower-Back Pain Rehabilitation Approach: System Design and User Acceptance Analysis | Not randomized trial |
| Efficacy of virtual reality to reduce chronic low back pain: Proof-of-concept of a non-pharmacological approach on pain, quality of life, neuropsychological and functional outcome | Not randomized trial |
| Proposed Game for Promoting Physical Activities among People with Low Back Pain using Virtual Reality | Not randomized trial |
| The influence of a biopsychosocial educational internet-based intervention on pain, dysfunction, quality of life, and pain cognition in chronic low back pain patients in primary care: a mixed methods approach | Not randomized trial |
| Tailored, multimedia versus traditional educational interventions for patients with low back pain: a randomized clinical trial. | No virtual reality intervention |
| Seeing It Helps: Movement-related Back Pain Is Reduced by Visualization of the Back During Movement | No virtual reality intervention |
| New exercise system for waist and back and its effect detection | No virtual reality intervention |
| Tele-rehabilitation for back pain in Korean farmers | No virtual reality intervention |
| Body schema acuity training and Feldenkrais RTM movements compared to core stabilization biofeedback and motor control exercises: Comparative effects on chronic non-specific low back pain in an outpatient clinical setting: A randomized controlled comparative study | No virtual reality intervention |
| Effect of Motor Control Training on Muscle Size and Football Games Missed from Injury | No virtual reality intervention |
| Randomized trial comparing interferential therapy with motorized lumbar traction and massage in the management of low back pain in a primary care setting | No virtual reality intervention |
| Self-Administered Skills-Based Virtual Reality Intervention for Chronic Pain: Randomized Controlled Pilot Study | Not only spinal pain |
| Effects of physiotherapy associated to virtual games in pain perception and heart rate variability in cases of low back pain | No chronic low back pain |
| Adherence to home exercises in non-specific low back pain. A randomised controlled pilot trial. | No chronic low back pain |
| Radiological (Magnetic Resonance Image and Ultrasound) and biochemical effects of virtual reality training on balance training in football players with chronic low back pain: A randomized controlled study. | No variables related to pain |
| The Effects of VR-based Wii Fit Yoga on PhysicalFunction in Middle-aged Female LBP Patients | No chronic low back pain |
| Evaluation of biofeedback based bridging exercises on older adults with low back pain: A randomized controlled trial | No chronic low back pain |
| Is physiotherapy integrated virtual walking effective on pain, function, and kinesiophobia in patients with non-specific low-back pain? Randomied controlled trial | No chronic low back pain |
| Effect of hippotherapy simulator on pain, disability and range of motion of the spinal column in subjects with mechanical low back pain: A randomized single-blind clinical trial | No chronic low back pain |
| A change in the size of the abdominal muscles and balance ability after virtual reality exercise in the elderly with chronic low back pain | No variables related to pain |
| Feasibility and Safety of a Virtual Reality Dodgeball Intervention for Chronic Low Back Pain: A Randomized Clinical Trial | Intervention duration < 4 weeks |
| Virtual reality distraction induces hypoalgesia in patients with chronic low back pain: a randomized controlled trial | Intervention duration < 4 weeks |
Appendix D
| Number | Article | Recruitment Status |
|---|---|---|
| NCT02125968 | Therapeutic Effects of Video Game Play Therapy on Patients With Chronic Low Back Pain | Unknown status |
| NCT03819907 | The Use of Virtual Reality for Lumbar Pain Management in an Outpatient Spine Clinic | Completed |
| NCT04468074 | Virtual Reality Treatment for Adults With Chronic Back Pain | Completed |
| NCT04042090 | The Efficacy, Acceptability, Tolerability and Feasibility of a Therapeutic Virtual Reality Application | Active, not recruiting |
| NCT04273919 | Virtual Reality for the Treatment of Chronic Low Back Pain | Recruiting |
| NCT04236804 | Implementing TMC-CP01 Treatment Based on the Virtual Autonomic Neuromodulation Induced Systemic Healing System in Reducing Pain and Opioid Requirement in Subjects Suffering From Chronic Low Back Pain | Recruiting |
| NCT04307446 | Immersive Virtual Reality and Chronic Back Pain | Recruiting |
| NCT04139564 | EaseVRx for the Reduction of Chronic Pain and Opioid Use | Recruiting |
| NCT04225884 | Digital Therapeutics (DTx) for Pain: Pilot Study of a Virtual Reality Software for Chronic Pain | Recruiting |
| NCT04609787 | Immersive Virtual Reality and Central Sensitization in People With Chronic Pain | Recruiting |
| NCT03909048 | Chronic Low Back Pain Graded - Exposure Psychoeducation Intervention | Completed |
| PACTR202010569932287 | Comparative effects of augmented, virtual and mixed reality on pain characteristics and health-related quality of life of patients with chronic non-specific low-back pain. | Not recruiting |
| PACTR202007533977502 | Comparative effects of clinic and virtual reality-based McKenzie extension therapy in chronic non-specific low-back pain. | Not recruiting |
| IRCT20200330046895N1 | Effects of virtual reality exercises on clinical outcomes in patients with chronic low back pain: a randomized controlled trial. | Recruiting |
| ACTRN12619001776190 | Altering body image in chronic low back pain using virtual reality: A proof of concept randomised clinical trial. | Not recruiting |
| PACTR201907749053096 | Effects of Core Stability Exercise Combined with Virtual Reality in Collegiate Athletes with Nonspecific Low Back Pain: A Randomized Clinical Trial. | Not recruiting |
| JPRN-UMIN000035505 | Effect of exercise by Virtual Reality in patients with chronic low back pain. | Not recruiting |
Appendix E
| Study Quality | External Validity | Study Bias | Confounding and Selection Bias | Study Power | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author (Year) [Ref.] | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | Total | Quality |
| Park et al. (2013) [26] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 16 | FAIR |
| Oh et al. (2014) [27] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 15 | FAIR |
| Yoo et al. (2014) [28] | 1 | 1 | 1 | 1 | 2 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 17 | FAIR |
| Monteiro-Junior et al. (2015) [32] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 21 | GOOD |
| Chen et al. (2016) [29] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 13 | POOR |
| Zadro et al. (2019) [7] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 26 | EXCELLENT |
| Kim et al. (2020) [30] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 22 | GOOD |
| Nambi et al. A (2020) [34] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 25 | GOOD |
| Nambi et al. B (2020) [35] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 24 | GOOD |
| Park et al. (2020) [31] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 21 | GOOD |
| Tomruk et al. (2020) [37] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 18 | FAIR |
| Garcia et al. (2021) [33] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 27 | EXCELLENT |
| Nambi et al. (2021) [36] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 24 | GOOD |
| Sato et al. (2021) [38] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 22 | GOOD |
References
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The Epidemiology of low back pain. Best Pr. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Delitto, A.; George, S.Z.; Van Dillen, L.R.; Whitman, J.M.; Sowa, G.; Shekelle, P.; Denninger, T.R.; Godges, J.J. Low back pain. J. Orthop. Sports Phys. Ther. 2012, 42, 1–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, R.; Qaseem, A.; Snow, V.; Casey, D.; Cross, J.T.; Shekelle, P.; Owens, D.K. American Pain Society Low Back Pain Guidelines for the Clinical Efficacy Assessment Subcommittee of the American College of Physicians and the American College of Physicians/American Pain Society Low Back Pain Guidelines Panel. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann. Intern. Med. 2007, 147, 478–491. [Google Scholar] [CrossRef]
- Zadro, J.; Shirley, D.; Simic, M.; Mousavi, S.J.; Ceprnja, D.; Maka, K.; Sung, J.; Ferreira, P. Video-Game–Based Exercises for Older People with Chronic Low Back Pain: A Randomized Controlledtable Trial (GAMEBACK). Phys. Ther. 2018, 99, 14–27. [Google Scholar] [CrossRef]
- Kato, P.M. Video Games in Health Care: Closing the Gap. Rev. Gen. Psychol. 2010, 14, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Pereira, M.F.; Prahm, C.; Kolbenschlag, J.; Oliveira, E.; Rodrigues, N.F. Application of AR and VR in hand rehabilitation: A systematic review. J. Biomed. Inform. 2020, 111, 103584. [Google Scholar] [CrossRef]
- De Miguel-Rubio, A.; Rubio, M.D.; Alba-Rueda, A.; Salazar, A.; Moral-Munoz, J.A.; Lucena-Anton, D. Virtual Reality Systems for Upper Limb Motor Function Recovery in Patients with Spinal Cord Injury: Systematic Review and Meta-Analysis. JMIR mHealth uHealth 2020, 8, e22537. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Linton, S.J. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain 2012, 153, 1144–1147. [Google Scholar] [CrossRef]
- Matheve, T.; Bogaerts, K.; Timmermans, A. Virtual reality distraction induces hypoalgesia in patients with chronic low back pain: A randomized controlled trial. J. Neuroeng. Rehabil. 2020, 17, 1–12. [Google Scholar] [CrossRef]
- Li, L.; Yu, F.; Shi, D.; Shi, J.; Tian, Z.; Yang, J.; Wang, X.; Jiang, Q. Application of virtual reality technology in clinical medicine. Am. J. Transl. Res. 2017, 9, 3867–3880. [Google Scholar]
- Gumaa, M.; Youssef, A.R. Is Virtual Reality Effective in Orthopedic Rehabilitation? A Systematic Review and Meta-Analysis. Phys. Ther. 2019, 99, 1304–1325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahern, M.M.; Dean, L.V.; Stoddard, C.C.; Agrawal, A.; Kim, K.; Cook, C.E.; Garcia, A.N. The Effectiveness of Virtual Reality in Patients with Spinal Pain: A Systematic Review and Meta-Analysis. Pain Pr. 2020, 20, 656–675. [Google Scholar] [CrossRef] [PubMed]
- Bordeleau, M.; Stamenkovic, A.; Tardif, P.-A.; Thomas, J. The Use of Virtual Reality in Back Pain Rehabilitation: A Systematic Review and Meta-Analysis. J. Pain 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Furlan, A.; Malmivaara, A.; Chou, R.; Maher, C.; A Deyo, R.; Schoene, M.L.; Bronfort, G.; van Tulder, M. 2015 Updated Method Guideline for Systematic Reviews in the Cochrane Back and Neck Group. Spine 2015, 40, 1660–1673. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomized intervention studies. Health Technol. Assess. 2003, 7, iii-173. [Google Scholar] [CrossRef] [Green Version]
- Saunders, L.D.; Soomro, G.M.; Buckingham, J.; Jamtvedt, G.; Raina, P. Assessing the Methodological Quality of Nonrandomized Intervention Studies. West. J. Nurs. Res. 2003, 25, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, I.T.; Salmerón, Y.M.; López, L.L.; Ortiz-Rubio, A.; Torres, J.R.; Valenza, M.C. Videogames in the Treatment of Obstructive Respiratory Diseases: A Systematic Review. Games Health J. 2019, 8, 237–249. [Google Scholar] [CrossRef]
- Silverman, S.R.; Schertz, L.A.; Yuen, H.K.; Lowman, J.D.; Bickel, C.S. Systematic review of the methodological quality and outcome measures utilized in exercise interventions for adults with spinal cord injury. Spinal Cord 2012, 50, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Hooper, P.; Jutai, J.; Strong, G.; Russell-Minda, E. Age-related macular degeneration and low-vision rehabilitation: A systematic review. Can. J. Ophthalmol. 2008, 43, 180–187. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-H.; Lee, S.-H.; Ko, D.-S. The Effects of the Nintendo Wii Exercise Program on Chronic Work-related Low Back Pain in Industrial Workers. J. Phys. Ther. Sci. 2013, 25, 985–988. [Google Scholar] [CrossRef] [Green Version]
- Oh, H.-W.; Lee, M.-G.; Jang, J.-Y.; Jin, J.-J.; Cha, J.-Y.; Jin, Y.-Y.; Jee, Y.-S. Time-effects of horse simulator exercise on psychophysiological responses in men with chronic low back pain. Isokinet. Exerc. Sci. 2014, 22, 153–163. [Google Scholar] [CrossRef]
- Yoo, J.-H.; Kim, S.-E.; Lee, M.-G.; Jin, J.-J.; Hong, J.; Choi, Y.-T.; Kim, M.-H.; Jee, Y.-S. The effect of horse simulator riding on visual analogue scale, body composition and trunk strength in the patients with chronic low back pain. Int. J. Clin. Pr. 2014, 68, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-Y.; Kim, S.-K.; Kim, K.-H.; Lee, I.-S.; Hwangbo, G. Effects of Horse Riding Simulator on Pain, Oswestry Disability Index and Balance in Adults with Nonspecific Chronic Low Back Pain. J. Korean Soc. Phys. Med. 2016, 11, 79–84. [Google Scholar] [CrossRef]
- Kim, T.; Lee, J.; Oh, S.; Kim, S.; Yoon, B. Effectiveness of Simulated Horseback Riding for Patients with Chronic Low Back Pain: A Randomized Controlled Trial. J. Sport Rehabil. 2020, 29, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Park, S.; Min, S.; Kim, C.-J.; Jee, Y.-S. A Randomized Controlled Trial Investigating the Effects of Equine Simulator Riding on Low Back Pain, Morphological Changes, and Trunk Musculature in Elderly Women. Medicina 2020, 56, 610. [Google Scholar] [CrossRef]
- Monteiro-Junior, R.S.; De Souza, C.P.; Lattari, E.; Rocha, N.; Mura, G.; Machado, S.; Da Silva, E.B. Wii-Workouts on Chronic Pain, Physical Capabilities and Mood of Older Women: A Randomized Controlled Double Blind Trial. CNS Neurol. Disord. Drug Targets 2015, 14, 1157–1164. [Google Scholar] [CrossRef]
- Garcia, L.M.; Birckhead, B.J.; Krishnamurthy, P.; Sackman, J.; Mackey, I.G.; Louis, R.G.; Salmasi, V.; Maddox, T.; Darnall, B.D. An 8-Week Self-Administered At-Home Behavioral Skills-Based Virtual Reality Program for Chronic Low Back Pain: Double-Blind, Randomized, Placebo-Controlled Trial Conducted During COVID-19. J. Med Internet Res. 2021, 23, e26292. [Google Scholar] [CrossRef] [PubMed]
- Nambi, G.; AbdelBasset, W.K.; Elsayed, S.H.; Alrawaili, S.M.; Abodonya, A.M.; Saleh, A.K.; Elnegamy, T.E. Comparative Effects of Isokinetic Training and Virtual Reality Training on Sports Performances in University Football Players with Chronic Low Back Pain-Randomized Controlled Study. Evid. Based Complement. Altern. Med. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Nambi, G.; Abdelbasset, W.K.; Alrawaili, S.M.; Alsubaie, S.F.; Abodonya, A.M.; Saleh, A.K. Virtual reality or isokinetic training; its effect on pain, kinesiophobia and serum stress hormones in chronic low back pain: A randomized controlled trial. Technol. Health Care 2021, 29, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Nambi, G.; Abdelbasset, W.K.; Alsubaie, S.F.; Saleh, A.K.; Verma, A.; Abdelaziz, M.A.; Alkathiry, A.A. Short-Term Psychological and Hormonal Effects of Virtual Reality Training on Chronic Low Back Pain in Soccer Players. J. Sport Rehabil. 2021, 30, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Tomruk, M.S.; Kara, B.; Erbayraktar, R.S. The Effect of Computer-Based Training on Postural Control in Patients with Chronic Low Back Pain: A Randomized Controlled Trial. J. Basic Clin. Health Sci. 2020, 4, 329–334. [Google Scholar] [CrossRef]
- Sato, T.; Shimizu, K.; Shiko, Y.; Kawasaki, Y.; Orita, S.; Inage, K.; Shiga, Y.; Suzuki, M.; Sato, M.; Enomoto, K.; et al. Effects of Nintendo Ring Fit Adventure Exergame on Pain and Psychological Factors in Patients with Chronic Low Back Pain. Games Health J. 2021, 10, 158–164. [Google Scholar] [CrossRef]
- Bahat, H.S.; Croft, K.; Carter, C.; Hoddinott, A.; Sprecher, E.; Treleaven, J. Remote kinematic training for patients with chronic neck pain: A randomized controlled trial. Eur. Spine J. 2018, 27, 1309–1323. [Google Scholar] [CrossRef]
- Rezaei, I.; Razeghi, M.; Ebrahimi, S.; Kayedi, S.; Zadeh, A.R. A Novel Virtual Reality Technique (Cervigame®) Compared to Conventional Proprioceptive Training to Treat Neck Pain: A Randomized Controlled Trial. J. Biomed. Phys. Eng. 2019, 9, 355–366. [Google Scholar] [CrossRef]
- Bahat, H.S.; Takasaki, H.; Chen, X.; Bet-Or, Y.; Treleaven, J. Cervical kinematic training with and without interactive VR training for chronic neck pain—A randomized clinical trial. Man. Ther. 2015, 20, 68–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polat, M.; Kahveci, A.; Muci, B.; Günendi, Z.; Karataş, G.K. The Effect of Virtual Reality Exercises on Pain, Functionality, Cardiopulmonary Capacity, and Quality of Life in Fibromyalgia Syndrome: A Randomized Controlled Study. Games Health J. 2021, 10, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Gulsen, C.; Soke, F.; Eldemir, K.; Apaydin, Y.; Ozkul, C.; Guclu-Gunduz, A.; Akcali, D.T. Effect of fully immersive virtual reality treatment combined with exercise in fibromyalgia patients: A randomized controlled trial. Assist. Technol. 2020, 1–8. [Google Scholar] [CrossRef]
- Joo, Y.; Kim, E.-K.; Song, H.-G.; Jung, H.; Park, H.; Moon, A.J.Y. Effectiveness of virtual reality immersion on procedure-related pain and anxiety in outpatient pain clinic: An exploratory randomized controlled trial. Korean J. Pain 2021, 34, 304–314. [Google Scholar] [CrossRef]
- McSherry, T.; Atterbury, M.; Gartner, S.; Helmold, E.; Searles, D.M.; Schulman, C. Randomized, Crossover Study of Immersive Virtual Reality to Decrease Opioid Use during Painful Wound Care Procedures in Adults. J. Burn. Care Res. 2017, 39, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Pazzaglia, C.; Imbimbo, I.; Tranchita, E.; Minganti, C.; Ricciardi, D.; Monaco, R.L.; Parisi, A.; Padua, L. Comparison of virtual reality rehabilitation and conventional rehabilitation in Parkinson’s disease: A randomised controlled trial. Physiotherapy 2020, 106, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Santos, P.; Machado, T.; Santos, L.; Ribeiro, N.; Melo, A. Efficacy of the Nintendo Wii combination with Conventional Exercises in the rehabilitation of individuals with Parkinson’s disease: A randomized clinical trial. NeuroRehabilitation 2019, 45, 255–263. [Google Scholar] [CrossRef]
- Marques-Sule, E.; Arnal-Gómez, A.; Buitrago-Jiménez, G.; Suso-Martí, L.; Cuenca-Martínez, F.; Espí-López, G.V. Effectiveness of Nintendo Wii and Physical Therapy in Functionality, Balance, and Daily Activities in Chronic Stroke Patients. J. Am. Med. Dir. Assoc. 2021, 22, 1073–1080. [Google Scholar] [CrossRef]
- Park, Y.-S.; An, C.-S.; Lim, C.-G. Effects of a Rehabilitation Program Using a Wearable Device on the Upper Limb Function, Performance of Activities of Daily Living, and Rehabilitation Participation in Patients with Acute Stroke. Int. J. Environ. Res. Public Health 2021, 18, 5524. [Google Scholar] [CrossRef]
- Saeedi, S.; Ghazisaeedi, M.; Rezayi, S. Applying Game-Based Approaches for Physical Rehabilitation of Poststroke Patients: A Systematic Review. J. Health Eng. 2021, 2021, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.S.; France, C.R.; Applegate, M.E.; Leitkam, S.T.; Walkowski, S. Feasibility and Safety of a Virtual Reality Dodgeball Intervention for Chronic Low Back Pain: A Randomized Clinical Trial. J. Pain 2016, 17, 1302–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collado-Mateo, D.; Lavín-Pérez, A.; García, J.F.; García-Gordillo, M.; Villafaina, S. Effects of Equine-Assisted Therapies or Horse-Riding Simulators on Chronic Pain: A Systematic Review and Meta-Analysis. Medicina 2020, 56, 444. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Liu, T.; Zhang, J. Horse-riding simulators in treatment of chronic low back pain: A meta-analysis. Int. J. Clin. Pr. 2021, 75, e14198. [Google Scholar] [CrossRef]















| Author (Year) [Ref.] | Interventions | Session Duration | Frequency | Program Duration | Supervision | Adverse Events |
|---|---|---|---|---|---|---|
| Park et al. (2013) [26] | EG1: Physical therapy (50 min) + Nintendo Wii exercises (30 min) Game: Nintendo Wii sports. VR program: wakeboard, frisbee dog, jet ski, and canoe games. Participants controlled a virtual character on the screen by swinging, rowing, and tilting remote controllers with motion sensors. Participants chose which program they performed. Time using videogame: 30 min (2 min break every 10 min). | 80 min | 3 sessions per week | 8 weeks | - | - |
| EG2: Physical therapy (50 min) + Lumbar stabilization exercises (30 min) 7 positions based on the back bridge, hands and knees, and side bridge. Maintain each position for 15 s for 3 sets. | ||||||
| CG: Physical therapy (50 min) Hot pack (30 min), interferential current therapy (15 min), and deep heat with ultrasound (5 min). | 50 min | |||||
| Oh et al. (2014) [27] | EG1: Horse simulator riding (10 min) VR system: Horse simulator machine (HJL Co. Ltd., Korea). VR program: warmup (stretching 5 min + ordinary walking on the horse simulator 5 min) + work-out (sitting trotting and rising trotting 10 min) + cool-down (supine stretching 10 min). Time using videogame: 15 min. | 30 min | 5 sessions per week | 8 weeks | Supervised | - |
| EG2: Horse simulator riding (20 min) VR system: Horse simulator machine (HJL Co. Ltd., Korea). VR program: warmup (stretching 5 min + ordinary walking on the horse simulator 5 min) + work-out (sitting trotting and rising trotting 20 min) + cool-down (supine stretching 10 min). Time using videogame: 25 min. | 40 min | |||||
| EG3: Horse simulator riding (30 min) VR system: Horse simulator machine (HJL Co. Ltd., Korea). VR program: warmup (stretching 5 min + ordinary walking on the horse simulator 5 min) + work-out (sitting trotting and rising trotting 30 min) + cool-down (supine stretching 10 min). Time using videogame: 35 min. | 50 min | |||||
| CG: No intervention. | - | - | - | |||
| Yoo et al. (2014) [28] | EG: Horse simulator riding VR system: Horse simulator machine (HJL Co. Ltd., Korea). VR program: warmup (stretching 10 min) + work-out + cool-down (stretching 10 min). Workout: ordinary walking and sitting trotting (week 1), increase riding time and riding trotting (weeks 2–3), increase riding time and intensity (weeks 4–5), and increase riding time and intensity (weeks 6–8). Time using videogame: 10 min (week 1), 20 min (weeks 2–3), 30 min (weeks 4–5) and 40 min (weeks 6–8). | Week 1: 30 min Week 2–3: 40 min Week 4–5: 50 min Week 6–8: 60 min | 3 sessions per week | 8 weeks | Supervised | - |
| CG: No intervention. | - | - | - | |||
| Monteiro-Junior et al. (2015) [32] | EG: Core exercises and strength training + 8 Wii Fit Plus workout VR system: Nintendo Wii Motion and Wii Balance Board Games. Games: chair, tightrope walk, ski slalom, balance bubble, table tilt, sideways, rowing squat, lunge. VR program: familiarization, play games 2 times (3 initial sessions). Only one attempt for each game (from 4 session). Verbal stimulus and rest periods (1–2 min). Time using videogame: 30 min. | 90 min | 3 sessions per week | 8 weeks | Supervised by a physiotherapist | - Vertigo |
| CG: Core exercises and strength training Core exercises: postures (15–30 s, 3 series, rest 10–15 s) + Strength training: exercises (10 reps, 3 series). | ||||||
| Chen et al. (2016) [29] | EG: Lumbar strengthening exercise (15 min) + Horse simulator riding (15 min) VR system: indoor riding machine (Hongjin Leports, South Korea). VR program: the horse simulator riding used in this study simulated riding a real horse through the visual information that appeared on the front screen by the virtual environment. Time using videogame: 15 min. | 30 min | 3 sessions per week | 4 weeks | - | - |
| CG: Lumbar strengthening exercise The exercise program consisted of 6 movements for 1 set. Each movement was held for 5s with 8 reps. All the programs were repeated for 5 times for 1 set. | ||||||
| Zadro et al. (2019) [7] | EG: Wii Fit U exercises at home VR system: Nintendo Wii U console and Wii Fit U software. VR program: booklet with exercises preselected by the research team (flexibility, strengthening, and aerobic exercises). Categories: yoga, muscle, aerobic, and balance. Intensity: 13 on the Borg rating scale + symptoms 24 h after exercise. 1 day of rest between exercise sessions. Learning session: 1 or 2 h. Time using videogame: 60 min. | 60 min | 3 sessions per week | 8 weeks | Unsupervised: EG received fortnightly calls from a physiotherapist | No adverse events were reported |
| CG: No intervention. | - | - | - | - | ||
| Kim et al. (2020) [30] | EG: Simulated horseback riding VR system: Horse simulator (FORTIS-102; Daewon FORTIS, Republic of Korea). VR program: stretching and cooldown (10 min) + workout (30 min) + rest time (6 min). Workout: consisted of walking, slow trotting, and fast trotting of a real horse gait. Time using videogame: 30 min. | 46 min | 2 sessions per week | 8 weeks | Supervised by practitioner | No adverse events were reported |
| CG: Stabilization exercises Stretching and cooldown (10 min) + workout (30 min) + rest time (6 min). The stabilization exercises with suspension (Redcord AS, Norway) consisted of a supine pelvic lift, supine and prone bridging exercise, and side-lying hip abduction. Each movement was performed forabout 10 s. | ||||||
| Nambi et al. (2020) A [34] | EG1: VR training + Physiotherapy VR system: ProKin system PK252N (Pelvic Module balance trunk MF; TechnoBody, Lanusei, Italy). Game: VR balance training with shooting game. The game is controlled by moving the trunk back and forth and left and right according to the signs. The activities were made gradually more difficult with more participant muscle activity and movement. Level of difficulty was defined by the number of enemies, angle of throw, frequency of shoot, frequency of flashing of enemies, and number of balls appearing around the participant. Time using video game: 30 min. | 30 min + 25 min | 5 sessions per week | 4 weeks | Supervisor | - |
| EG2: Isokinetic training + Physiotherapy Warmup: stretching (5 min) + Isokinetic dynamometer: exercise at an angular speed of 60°, 90°, and 120° (15 reps of 3 sets and rest between sets 30 s and between pace 60 s). | − + 25 min | |||||
| CG: Conventional balance training + Physiotherapy Active isotonic exercise and isometric exercise (10–15 reps/day) + stretching (3 reps for 10 s). | − + 25 min | |||||
| Physiotherapy: Hot pack therapy (20 min) and ultrasound (5 min) + home-based exercise protocol. | 25 min | |||||
| Nambi et al. (2020) B [35] | EG1: VR training + Physiotherapy VR system: ProKin system PK252N (Pelvic Module balance trunk MF; TechnoBody, Lanusei, Italy). Game: VR balance training with shooting game. The game is controlled by moving the trunk back and forth and left and right according to the signs. The activities were made gradually more difficult with more participant muscle activity and movement. Level of difficulty was defined by the number of enemies, angle of throw, frequency of shoot, frequency of flashing of enemies, and number of balls appearing around the participant. Time using video game: 30 min. | 30 min + 25 min | 5 sessions per week | 4 weeks | Supervisor | - |
| EG2: Isokinetic training + Physiotherapy Warmup: stretching (5 min) + Isokinetic dynamometer: exercise at an angular speed of 60°, 90°, and 120° (15 reps of 3 sets and rest between sets 30 s and between pace 60 s). | − + 25 min | |||||
| CG: Conventional balance training + Physiotherapy Active isotonic exercise and isometric exercise (10–15 reps/day) + stretching (3 reps for 10 s). | − + 25 min | |||||
| Physiotherapy: Hot pack therapy (20 min) and ultrasound (5 min) + home-based exercise protocol. | 25 min | |||||
| Park et al. (2020) [31] | EG: Equine riding simulator VR system: Horse simulator (FORTIS 101, Daewon, Corp., Seoul, Korea). VR program: warmup (8 min) + workout (15 min) + cooldown (7 min). Work-out: walking (weeks 1–4), walking 10 min + trotting 5 min (weeks 5–8) and trotting 10 min + cantering 5 min (weeks 9–12). Time using videogame: 15 min. | 30 min | 3 sessions per week | 12 weeks | Supervised by researcher | - |
| CG: Watching video Participants sat on the horse and watched the video from the monitor | ||||||
| Tomruk et al. (2020) [37] | EG: Computer-based stability training VR system: Biodex Balance System. VR program: postural stability training, limits of stability training, weight shift training, and maze control training. 12 stability levels, 3 trials with 10 s rest in each condition. Time using videogame: 30 min. | 30 min | 2 sessions per week | 12 weeks | Supervised by physiotherapist | - |
| CG: Traditional training Traditional postural control exercises by giving them visual, vestibular, or proprioceptive stimulus under the cues of a physiotherapist. | ||||||
| Garcia et al. (2021) [33] | EG: EaseVRx at home VR system: Pico G2 4K all-in-one head-mounted VR device. VR program: the program delivers a multifaceted combination of pain relief skills training through a prescribed sequence of daily immersive experiences (3D images). Each VR experiences lasts between 2–16 min (average 6 min). Categories: pain education, relaxation/interoception, mindful escapes, pain distraction games and dynamic breathing. Time using video game: 2–16 min depending on the experience. | 2–16 min | 7 sessions per week | 8 weeks | Unsupervised | - Nausea - Motion sickness |
| CG: Sham VR at home VR system: Pico G2 4K all-in-one head-mounted VR device. VR program: sham VR headset displayed 2D nature footage with neutral music that was selected to be neither overly relaxing, aversive, nor distracting. The experience of Sham VR is similar to viewing nature scenes on a large-screen television and is not interactive. Twenty videos were rotated over the 56 sessions, with average duration of sessions closely matching those of EaseVRx. | ||||||
| Nambi et al. (2021) [36] | EG1: VR training + Physiotherapy VR system: Pro-Kin system PK 252N (Pelvic Module balance trunk MF; TechnoBody, Lanusei, Italy). Game: shooting game. The subjects are sitting on the virtual platform and visualizing the game on the computer display screen. The game was executed and controlled by moving the trunk back and forth and left and right according to the signs. The activities were made gradually more difficult with more participant muscle activity and movement. The level of difficulty was defined by the number of enemies, angle of throw, frequency of shoot, frequency of flashing of enemies, and number of balls appearing around the participant. Time using videogame: 30 min. | 30 min + 25 min | 5 sessions per week | 4 weeks | Supervised by physiotherapist | - |
| EG2: Combined physical rehabilitation + Physiotherapy The participant received balance training through a Swiss ball for core muscles. Exercises: wall squat, Russian twist, leg lift, plank saw, cobra and hip raise on the Swiss ball, 15 times per set for 3 sets. Maintain each position 10 s with a 3 s break between repetitions. | − + 25 min | |||||
| CG: Conventional balance training + Physiotherapy Active isotonic and isometric exercises for abdominal muscles, deep abdominal muscles, and back muscles. 10 to 15 reps. Stretching was focused on each muscle group for 3 reps for 10 s per muscle group. | − + 25 min | |||||
| Physiotherapy: Hot pack therapy (20 min) + ultrasound (5 min) + home-based exercise protocol. | 25 min | |||||
| Sato et al. (2021) [38] | EG: Nintendo Ring Fit Adventure Exergame VR system: Ring Fit Adventure of Nintendo Switch. VR program: Adventure mode (30 min) + low back pain improvement program (10 min). Ring Fit Adventure is a fitness role-playing game that uses a ring-shaped controller as a device for resistance training. The player advances the story while exercising as the movement of the player is linked to the main character on the screen. Time using videogame: 40 min. | 40 min | 1 session per week | 8 weeks | - | - |
| CG: Oral treatment Drugs: Nonsteroidal Anti-Inflammatory Drugs, Tramadol, and Duloxetine. Each drug was started at the standard dose, with patients coming in every 2 weeks to be interviewed for pain, and if pain relief was not adequate, then the dose was gradually increased to its highest recommended level. If pain relief was still inadequate, the next drug was added. | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brea-Gómez, B.; Torres-Sánchez, I.; Ortiz-Rubio, A.; Calvache-Mateo, A.; Cabrera-Martos, I.; López-López, L.; Valenza, M.C. Virtual Reality in the Treatment of Adults with Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Int. J. Environ. Res. Public Health 2021, 18, 11806. https://doi.org/10.3390/ijerph182211806
Brea-Gómez B, Torres-Sánchez I, Ortiz-Rubio A, Calvache-Mateo A, Cabrera-Martos I, López-López L, Valenza MC. Virtual Reality in the Treatment of Adults with Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. International Journal of Environmental Research and Public Health. 2021; 18(22):11806. https://doi.org/10.3390/ijerph182211806
Chicago/Turabian StyleBrea-Gómez, Beatriz, Irene Torres-Sánchez, Araceli Ortiz-Rubio, Andrés Calvache-Mateo, Irene Cabrera-Martos, Laura López-López, and Marie Carmen Valenza. 2021. "Virtual Reality in the Treatment of Adults with Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomized Clinical Trials" International Journal of Environmental Research and Public Health 18, no. 22: 11806. https://doi.org/10.3390/ijerph182211806
APA StyleBrea-Gómez, B., Torres-Sánchez, I., Ortiz-Rubio, A., Calvache-Mateo, A., Cabrera-Martos, I., López-López, L., & Valenza, M. C. (2021). Virtual Reality in the Treatment of Adults with Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. International Journal of Environmental Research and Public Health, 18(22), 11806. https://doi.org/10.3390/ijerph182211806