
Impact of Working from Home on Cardiovascular Health: An Emerging Issue with the COVID-19 Pandemic

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
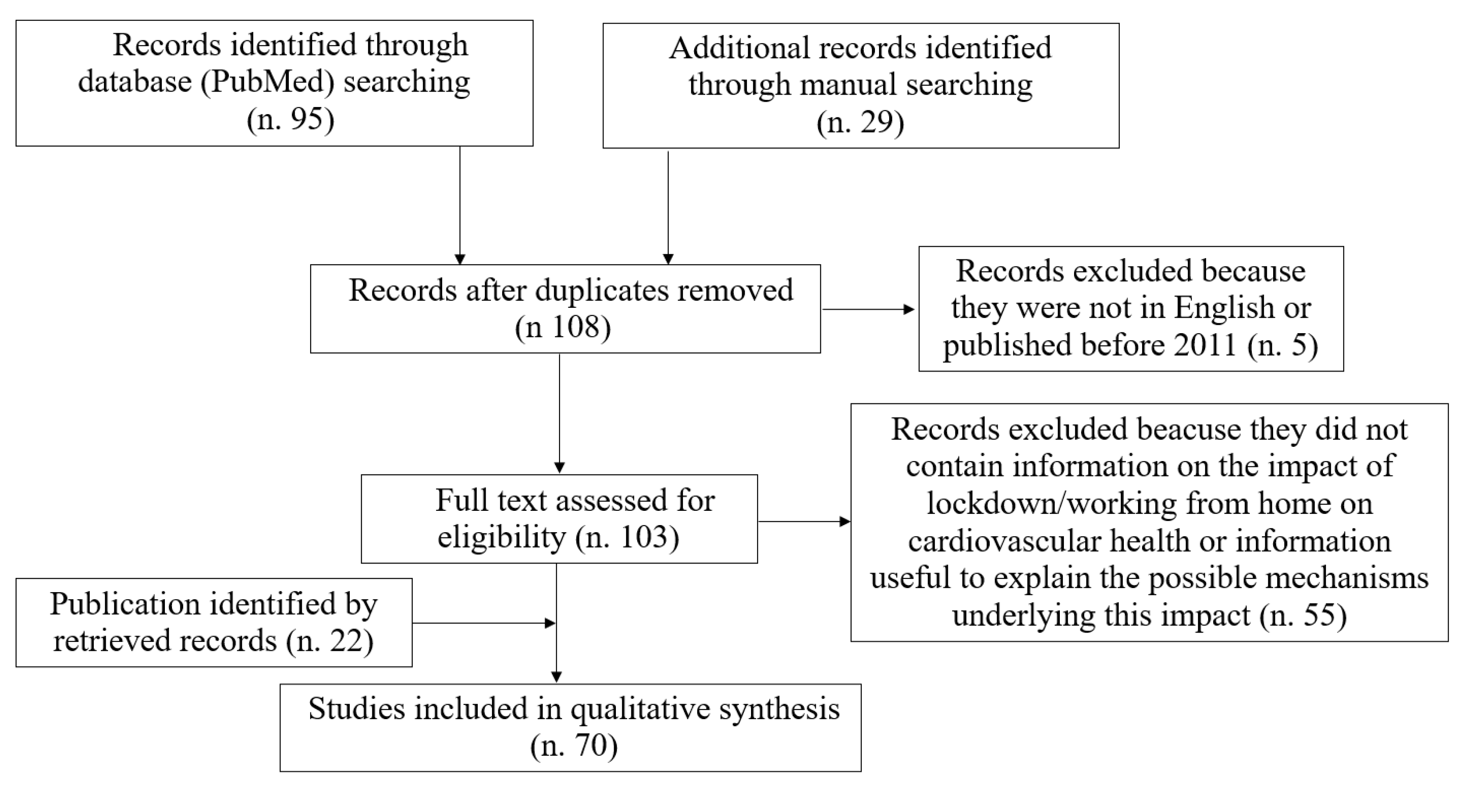
2. Literature Search Strategy
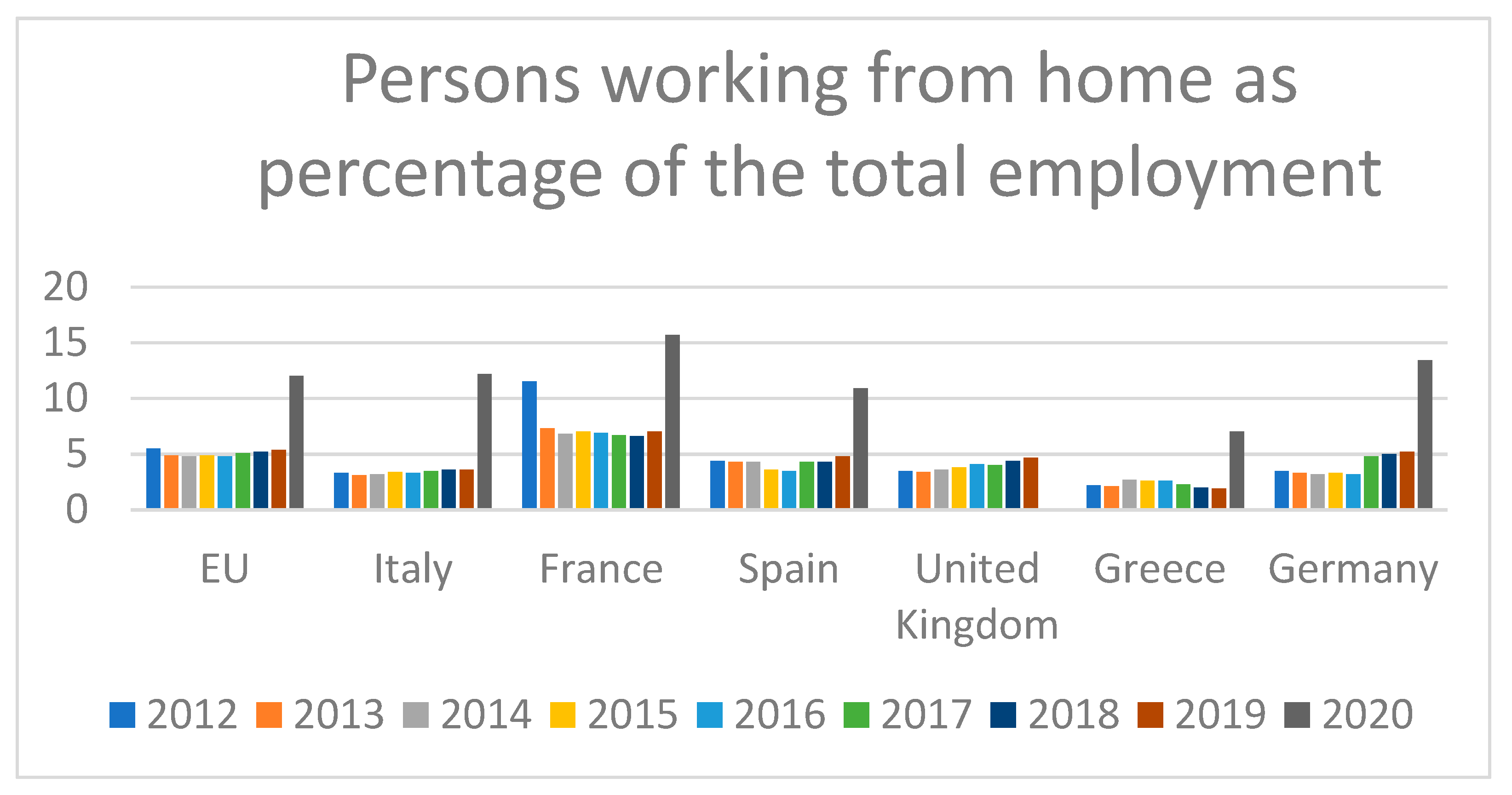
3. Scope of the Issue
3.1. Working from Home and Lifestyle Changes
3.2. Working from Home and Psychological Stress
3.3. Working from Home and Cardiometabolic Disease
4. Discussion
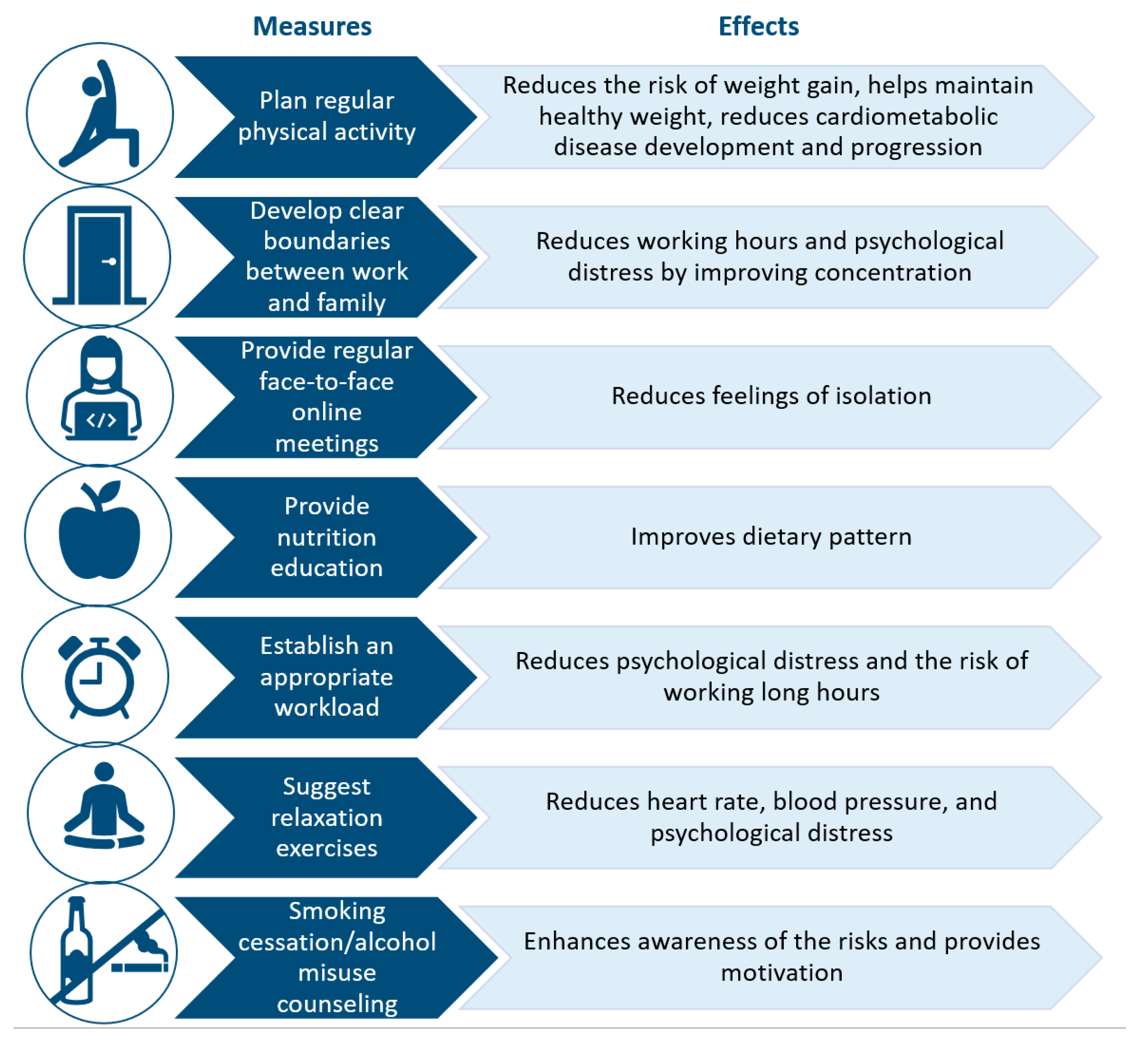
4.1. Future Perspectives
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
References
- World Health Organization WHO. Weekly Operational Update on COVID-19. Available online: https://www.who.int/publications/m/item/weekly-operational-update-on-covid-19---3-november-2021 (accessed on 10 November 2021).
- The Impact of Teleworking and Digital Work on Workers and Society. Think Tank (europa.eu). Available online: https://www.europarl.europa.eu/thinktank/en/document.html?reference=IPOL_STU(2021)662904 (accessed on 10 November 2021).
- IL MERCATO DEL LAVORO 2020 UNA LETTURA INTEGRATA. Available online: https://www.istat.it/it/files//2021/02/Il-Mercato-del-lavoro-2020-1.pdf (accessed on 10 November 2021).
- Working From Home in the EU. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/DDN-20180620-1 (accessed on 10 November 2021).
- Jones, J.M. In U.S., Telecommuting for Work Climbs to 37%. Available online: https://news.gallup.com/poll/184649/telecommuting-work-climbs.aspx (accessed on 10 November 2021).
- PubMed. Working from Home—Search Results—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/?term=working+from+home&sort=pubdate (accessed on 2 October 2021).
- Fukushima, N.; Machida, M.; Kikuchi, H.; Amagasa, S.; Hayashi, T.; Odagiri, Y.; Takamiya, T.; Inoue, S. Associations of working from home with occupational physical activity and sedentary behavior under the COVID-19 pandemic. J. Occup. Health 2021, 63, e12212. [Google Scholar] [CrossRef]
- Benefits and Risks Associated with Physical Activity. Available online: https://www.acsm.org/docs/default-source/publications-files/acsm-guidelines-download-10th-edabf32a97415a400e9b3be594a6cd7fbf.pdf?sfvrsn=aaa6d2b2_0 (accessed on 10 November 2021).
- McDowell, C.P.; Herring, M.P.; Lansing, J.; Brower, C.; Meyer, J.D. Working from Home and Job Loss Due to the COVID-19 Pandemic Are Associated with Greater Time in Sedentary Behaviors. Front. Public Health 2020, 8, 597619. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.; Owen, N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06. Eur. Heart J. 2011, 32, 590–597. [Google Scholar] [CrossRef]
- Kaptoge, S.; Di Angelantonio, E.; Lowe, G.; Pepys, M.B.; Thompson, S.G.; Collins, R.; Danesh, J. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: An individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [PubMed] [Green Version]
- Dempsey, P.C.; Larsen, R.N.; Dunstan, D.W.; Owen, N.; Kingwell, B.A. Sitting Less and Moving More: Implications for Hypertension. Hypertension 2018, 72, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Carnethon, M.; Whitsel, L.P.; Franklin, B.A.; Kris-Etherton, P.; Milani, R.; Pratt, C.A.; Wagner, G.R.; American Heart Association Advocacy Coordinating Committee; Council on Epidemiology and Prevention; Council on the Kidney in Cardiovascular Disease; et al. Worksite wellness programs for cardiovascular disease prevention: A policy statement from the American Heart Association. Circulation 2009, 120, 1725–1741. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekaran, B.; Rao, C.R.; Davis, F.; Arumugam, A. SMART STEP—SMARTphone-driven exercise and pedometer-based STEP intervention to promote physical activity among desk-based employees: Study protocol for a three-arm cluster randomized controlled trial. Work 2021, 69, 1229–1245. [Google Scholar] [CrossRef]
- Munir, F.; Biddle, S.J.H.; Davies, M.; Dunstan, D.; Esliger, D.; Gray, L.J.; Jackson, B.R.; O’Connell, S.E.; Yates, T.; Edwardson, C.L. Stand More AT Work (SMArT Work): Using the behaviour change wheel to develop an intervention to reduce sitting time in the workplace. BMC Public Health 2018, 18, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Leona, S.; Forerob, D.A.; Ruiz-D’ıaz, P. Recommendations for working from home during the COVID-19 pandemic (and beyond). Work 2020, 66, 371–375. [Google Scholar] [CrossRef]
- Prete, M.; Luzzetti, A.; Augustin, L.S.A.; Porciello, G.; Montagnese, C.; Calabrese, I.; Ballarin, G.; Coluccia, S.; Patel, L.; Vitale, S.; et al. Changes in Lifestyle and Dietary Habits during COVID-19 Lockdown in Italy: Results of an Online Survey. Nutrients 2021, 13, 1923. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.; Ramos-Campo, D.; Mielgo-Ayuso, J.; Dalamitros, A.; Nikolaidis, P.; Hormeño-Holgado, A.; Tornero-Aguilera, J. Nutrition in the Actual COVID-19 Pandemic. A Narrative Review. Nutrients 2021, 13, 1924. [Google Scholar] [CrossRef]
- Mascherini, G.; Catelan, D.; Pellegrini-Giampietro, D.E.; Petri, C.; Scaletti, C.; Gulisano, M. Changes in physical activity levels, eating habits and psychological well-being during the Italian COVID-19 pandemic lockdown: Impact of socio-demographic factors on the Florentine academic population. PLoS ONE 2021, 16, e0252395. [Google Scholar] [CrossRef]
- Sato, K.; Kobayashi, S.; Yamaguchi, M.; Sakata, R.; Sasaki, Y.; Murayama, C.; Kondo, N. Working from home and dietary changes during the COVID-19 pandemic: A longitudinal study of health app (CALO mama) users. Appetite 2021, 165, 105323. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 outbreak: Changes in diet and physical activity increase the risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.; Chang, B.P.I.; Hristov, H.; Pravst, I.; Profeta, A.; Millard, J. Changes in Food Consumption During the COVID-19 Pandemic: Analysis of Consumer Survey Data from the First Lockdown Period in Denmark, Germany, and Slovenia. Front. Nutr. 2021, 8, 635859. [Google Scholar] [CrossRef]
- Pristipino, C. Psychological Stress, Inflammation, Immunity, and Coagulation Intertwining in Ischemic Heart Disease. In Psychotherapy for Ischemic Heart Disease; Springer: Berlin/Heidelberg, Germany, 2016; pp. 45–58. [Google Scholar]
- Buomprisco, G.; Ricci, S.; Perri, R.; De Sio, S. Health and Telework: New Challenges after COVID-19 Pandemic. Eur. J. Environ. Public Health 2021, 5, em0073. [Google Scholar] [CrossRef]
- Garre-Olmo, J.; Turró-Garriga, O.; Martí-Lluch, R.; Zacarías-Pons, L.; Alves-Cabratosa, L.; Serrano-Sarbosa, D.; Vilalta-Franch, J.; Ramos, R.; Manté, X.A.; Casedevall, J.B.; et al. Changes in lifestyle resulting from confinement due to COVID-19 and depressive symptomatology: A cross-sectional a population-based study. Compr. Psychiatry 2021, 104, 152214. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Becerik-Gerber, B.; Lucas, G.; Roll, S.C. Impacts of Working from Home during COVID-19 Pandemic on Physical and Mental Well-Being of Office Workstation Users. J. Occup. Environ. Med. 2021, 63, 181–190. [Google Scholar] [CrossRef]
- Galanti, T.; Guidetti, G.; Mazzei, E.; Zappalà, S.; Toscano, F. Work from Home During the COVID-19 Outbreak: The Impact on Employees’ Remote Work Productivity, Engagement, and Stress. J. Occup. Environ. Med. 2021, 63, e426–e432. [Google Scholar] [CrossRef]
- Şentürk, E.; Sağaltıcı, E.; Geniş, B.; Toker, Ö.G. Predictors of depression, anxiety and stress among remote workers during the COVID-19 pandemic. Work 2021, 70, 41–51. [Google Scholar] [CrossRef]
- Barrea, L.; Pugliese, G.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Savastano, S.; Colao, A.; Muscogiuri, G. Does SARS-COV-2 threaten our dreams? Effect of quarantine on sleep quality and body mass index. J. Transl. Med. 2020, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Conroy, D.A.; Hadler, N.L.; Cho, E.; Moreira, A.; MacKenzie, C.; Swanson, L.M.; Burgess, H.J.; Arnedt, J.T.; Goldstein, C.A. The effects of COVID-19 stay-at-home order on sleep, health, and working patterns: A survey study of US health care workers. J. Clin. Sleep Med. 2021, 17, 185–191. [Google Scholar] [CrossRef]
- Tavares, A.I. Telework and health effects review. Int. J. Healthc. 2017, 3, 30. [Google Scholar] [CrossRef] [Green Version]
- Pega, F.; Náfrádi, B.; Momen, N.C.; Ujita, Y.; Streicher, K.N.; Prüss-Üstün, A.M.; Technical Advisory Group; Descatha, A.; Driscoll, T.; Fischer, F.M.; et al. Global, regional, and national burdens of ischemic heart disease and stroke attributable to exposure to long working hours for 194 countries, 2000–2016: A systematic analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ. Int. 2021, 154, 106595. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, D.; McKee, G.B.; Perrin, P.B.; Alzueta, E.; Caffarra, S.; Ramos-Usuga, D.; Arango-Lasprilla, J.C.; Baker, F.C. Sleeping when the world locks down: Correlates of sleep health during the COVID-19 pandemic across 59 countries. Sleep Health 2021, 7, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Matthews, K.A.; Pantesco, E. Sleep characteristics and cardiovascular risk in children and adolescents: An enumerative review. Sleep Med. 2016, 18, 36–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallman, D.M.; Januario, L.B.; Mathiassen, S.E.; Heiden, M.; Svensson, S.; Bergström, G. Working from home during the COVID-19 outbreak in Sweden: Effects on 24-h time-use in office workers. BMC Public Health 2021, 21, 528. [Google Scholar] [CrossRef]
- Ross, R.; Chaput, J.-P.; Giangregorio, L.M.; Janssen, I.; Saunders, T.J.; Kho, M.; Poitras, V.J.; Tomasone, J.R.; El-Kotob, R.; McLaughlin, E.C.; et al. Canadian 24-h Movement Guidelines for Adults aged 18–64 years and Adults aged 65 years or older: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab 2020, 45, S57–S102. [Google Scholar] [CrossRef]
- Oakman, J.; Kinsman, N.; Stuckey, R.; Graham, M.; Weale, V. A rapid review of mental and physical health effects of working at home: How do we optimise health? BMC Public Health 2020, 20, 1825. [Google Scholar] [CrossRef]
- Tušl, M.; Brauchli, R.; Kerksieck, P.; Bauer, G.F. Impact of the COVID-19 crisis on work and private life, mental well-being and self-rated health in German and Swiss employees: A cross-sectional online survey. BMC Public Health 2021, 21, 1–15. [Google Scholar] [CrossRef]
- Widar, L.; Wiitavaara, B.; Boman, E.; Heiden, M. Psychophysiological Reactivity, Postures and Movements among Academic Staff: A Comparison between Teleworking Days and Office Days. Int. J. Environ. Res. Public Health 2021, 18, 9537. [Google Scholar] [CrossRef]
- Darouei, M.; Pluut, H. Work from home today for a better tomorrow! How working from home influences work-family conflict and employees’ start of the next workday. Stress Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Stopping the Stress of Working from Home. Available online: https://www.heart.org/en/news/2020/03/26/stopping-the-stress-of-working-from-home (accessed on 2 October 2021).
- Okuyan, C.B.; Begen, M.A. Working from home during the COVID-19 pandemic, its effects on health, and recommendations: The pandemic and beyond. Perspect. Psychiatr. Care 2021. [Google Scholar] [CrossRef]
- Reynolds, C.M.; Purdy, J.; Rodriguez, L.; McAvoy, H. Factors associated with changes in consumption among smokers and alcohol drinkers during the COVID-19 ‘lockdown’ period. Eur. J. Public Health 2021, 31, 1084–1089. [Google Scholar] [CrossRef]
- Rozanski, A.; Blumenthal, J.A.; Davidson, K.; Saab, P.G.; Kubzansky, L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: The emerging field of behavioral cardiology. J. Am. Coll. Cardiol. 2005, 45, 637–651. [Google Scholar] [CrossRef] [Green Version]
- Colivicchi, F.; Di Fusco, S.A.; Santini, M. Psycho-educational Interventions and Cardiac Rehabilitation. In Psychotherapy for Ischemic Heart Disease; Springer: Berlin/Heidelberg, Germany, 2016; pp. 107–120. [Google Scholar]
- Kivimäki, M.; Virtanen, M.; Elovainio, M.; Kouvonen, A.; Väänänen, A.; Vahtera, J. Work stress in the etiology of coronary heart disease—A meta-analysis. Scand. J. Work Environ. Health 2006, 32, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Rozanski, A.; Blumenthal, J.A.; Kaplan, J. Impact of Psychological Factors on the Pathogenesis of Cardiovascular Disease and Implications for Therapy. Circulation 1999, 99, 2192–2217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Tecco, C.; Ronchetti, M.; Russo, S.; Ghelli, M.; Rondinone, B.M.; Persechino, B.; Iavicoli, S. Implementing Smart Working in Public Administration: A follow up study. Med. Lav. 2021, 112, 141–152. [Google Scholar]
- Khan, M.A.; Smith, J.E.M. “Covibesity,” a new pandemic. Obes. Med. 2020, 19, 100282. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in Weight and Nutritional Habits in Adults with Obesity during the “Lockdown” Period Caused by the COVID-19 Virus Emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Guler, M.A.; Guler, K.; Gulec, M.G.; Ozdoglar, E. Working from Home During a Pandemic. J. Occup. Environ. Med. 2021, 63, 731–741. [Google Scholar] [CrossRef]
- Ekpanyaskul, C.; Padungtod, C. Occupational Health Problems and Lifestyle Changes Among Novice Working-From-Home Workers Amid the COVID-19 Pandemic. Saf. Health Work. 2021, 12, 384–389. [Google Scholar] [CrossRef]
- Lin, T.-C.; Courtney, T.; Lombardi, D.A.; Verma, S.K. Association Between Sedentary Work and BMI in a U.S. National Longitudinal Survey. Am. J. Prev. Med. 2015, 49, e117–e123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverii, G.A.; Delli Poggi, C.; Dicembrini, I.; Monami, M.; Mannucci, E. Glucose control in diabetes during home confinement for the first pandemic wave of COVID-19: A meta-analysis of observational studies. Acta Diabetol. 2021, 58, 1603–1611. [Google Scholar] [CrossRef]
- Bonora, B.M.; Morieri, M.L.; Avogaro, A.; Fadini, G.P. The Toll of Lockdown Against COVID-19 on Diabetes Outpatient Care: Analysis from an Outbreak Area in Northeast Italy. Diabetes Care 2021, 44, e18–e21. [Google Scholar] [CrossRef]
- Ghosh, A.; Arora, B.; Gupta, R.; Anoop, S.; Misra, A. Effects of nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 917–920. [Google Scholar] [CrossRef]
- Auriemma, R.S.; Pirchio, R.; Liccardi, A.; Scairati, R.; Del Vecchio, G.; Pivonello, R.; Colao, A. Metabolic syndrome in the era of COVID-19 outbreak: Impact of lockdown on cardiometabolic health. J. Endocrinol. Investig. 2021, 26, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, R.; Sanders, S.; Michaleff, Z.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 pandemic on utilisation of healthcare services: A systematic review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef] [PubMed]
- Degli Esposti, L.; Buda, S.; Nappi, C.; Paoli, D.; Perrone, V. Implications of COVID-19 Infection on Medication Adherence with Chronic Therapies in Italy: A Proposed Observational Investigation by the Fail-to-Refill Project. Risk Manag. Healthc. Policy 2020, 13, 3179–3185. [Google Scholar] [CrossRef]
- Mitacchione, G.; Schiavone, M.; Curnis, A.; Arca, M.; Antinori, S.; Gasperetti, A.; Mascioli, G.; Severino, P.; Sabato, F.; Caracciolo, M.M.; et al. Impact of prior statin use on clinical outcomes in COVID-19 patients: Data from tertiary referral hospitals during COVID-19 pandemic in Italy. J. Clin. Lipidol. 2021, 15, 68–78. [Google Scholar] [CrossRef]
- Chow, R.; Im, J.; Chiu, N.; Chiu, L.; Aggarwal, R.; Lee, J.; Choi, Y.-G.; Prsic, E.H.; Shin, H.J. The protective association between statins use and adverse outcomes among COVID-19 patients: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0253576. [Google Scholar] [CrossRef]
- Bifulco, M.; Gazzerro, P. Statin therapy in COVID-19 infection: Much more than a single pathway. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 6, 410–411. [Google Scholar] [CrossRef]
- Castiglione, V.; Chiriacò, M.; Emdin, M.; Taddei, S.; Vergaro, G. Statin therapy in COVID-19 infection. Eur. Heart J. Cardiovasc Pharmacother. 2020, 6, 258–259. [Google Scholar] [CrossRef]
- McDowell, C.P.; Herring, M.P.; Lansing, J.; Brower, C.S.; Meyer, J.D. Associations Between Employment Changes and Mental Health: US Data from During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 631510. [Google Scholar] [CrossRef] [PubMed]
- Mulugeta, T.; Tadesse, E.; Shegute, T.; Desta, T.T. COVID-19: Socio-economic impacts and challenges in the working group. Heliyon 2021, 7, e07307. [Google Scholar] [CrossRef] [PubMed]
- Giovanis, E.; Ozdamar, O. Implications of COVID-19: The Effect of Working from Home on Financial and Mental Well-Being in the UK. Int. J. Health Policy Manag. 2021, 3752237. [Google Scholar] [CrossRef] [PubMed]
- Ipsen, C.; van Veldhoven, M.; Kirchner, K.; Hansen, J.P. Six Key Advantages and Disadvantages of Working from Home in Europe during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 1826. [Google Scholar] [CrossRef]
- Najafabadi, M.G.; Khah, A.S.; Rostad, M. Sedentary lifestyle among office workers and coronary heart disease risk factors due to the COVID-19 quarantine. Work 2020, 67, 281–283. [Google Scholar] [CrossRef]
- Moretti, A.; Menna, F.; Aulicino, M.; Paoletta, M.; Liguori, S.; Iolascon, G. Characterization of Home Working Population during COVID-19 Emergency: A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6284. [Google Scholar] [CrossRef]
- Nagata, T.; Ito, D.; Nagata, M.; Fujimoto, A.; Ito, R.; Odagami, K.; Kajiki, S.; Uehara, M.; Oyama, I.; Dohi, S.; et al. Anticipated health effects and proposed countermeasures following the immediate introduction of telework in response to the spread of COVID-19: The findings of a rapid health impact assessment in Japan. J. Occup. Health 2021, 63, e12198. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Fusco, S.A.; Spinelli, A.; Castello, L.; Mocini, E.; Gulizia, M.M.; Oliva, F.; Gabrielli, D.; Imperoli, G.; Colivicchi, F. Impact of Working from Home on Cardiovascular Health: An Emerging Issue with the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11882. https://doi.org/10.3390/ijerph182211882
Di Fusco SA, Spinelli A, Castello L, Mocini E, Gulizia MM, Oliva F, Gabrielli D, Imperoli G, Colivicchi F. Impact of Working from Home on Cardiovascular Health: An Emerging Issue with the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(22):11882. https://doi.org/10.3390/ijerph182211882
Chicago/Turabian StyleDi Fusco, Stefania Angela, Antonella Spinelli, Lorenzo Castello, Edoardo Mocini, Michele Massimo Gulizia, Fabrizio Oliva, Domenico Gabrielli, Giuseppe Imperoli, and Furio Colivicchi. 2021. "Impact of Working from Home on Cardiovascular Health: An Emerging Issue with the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 22: 11882. https://doi.org/10.3390/ijerph182211882
APA StyleDi Fusco, S. A., Spinelli, A., Castello, L., Mocini, E., Gulizia, M. M., Oliva, F., Gabrielli, D., Imperoli, G., & Colivicchi, F. (2021). Impact of Working from Home on Cardiovascular Health: An Emerging Issue with the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(22), 11882. https://doi.org/10.3390/ijerph182211882