
Co-Production within Child and Adolescent Mental Health: A Systematic Review


Abstract
:1. Introduction
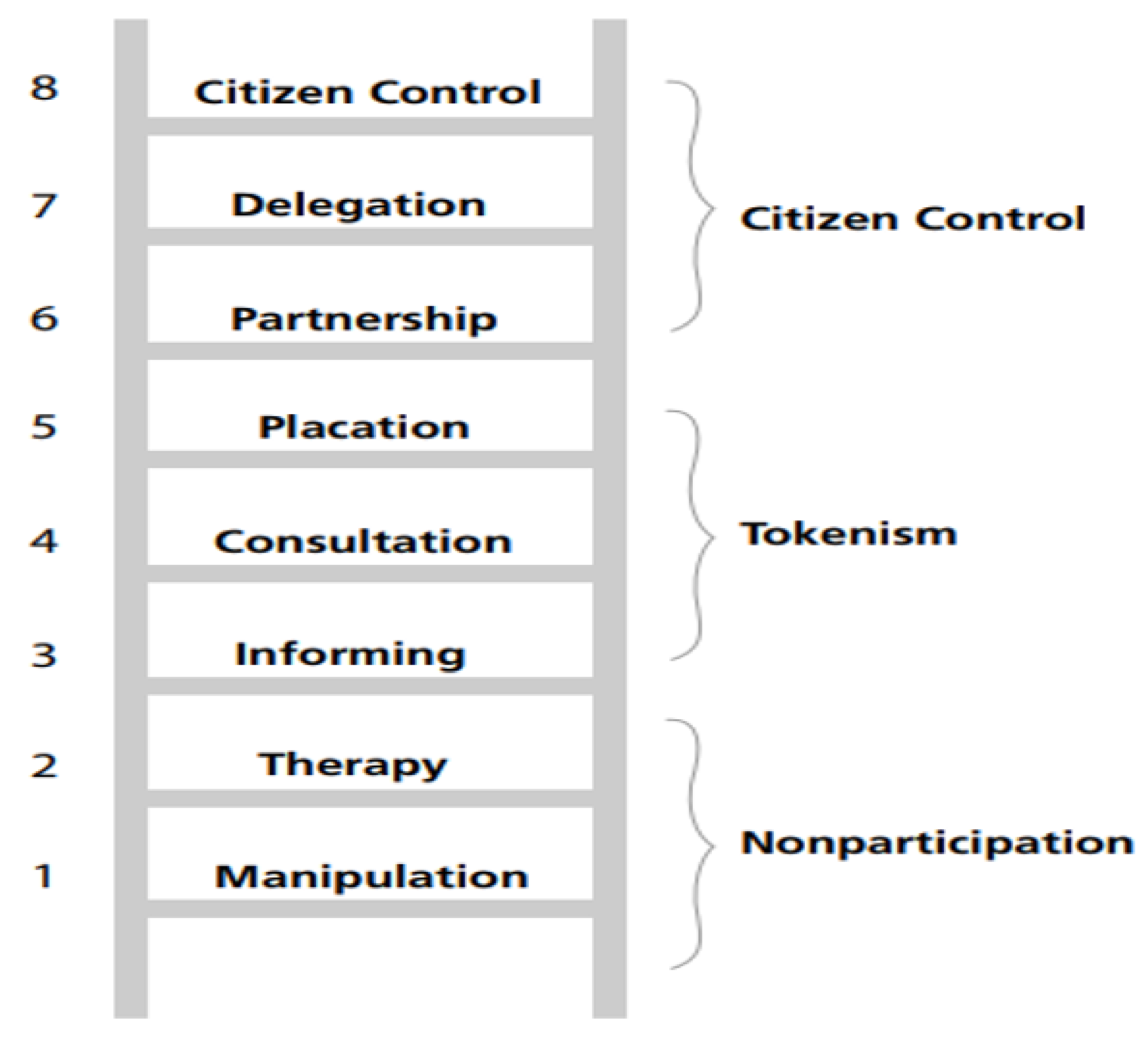
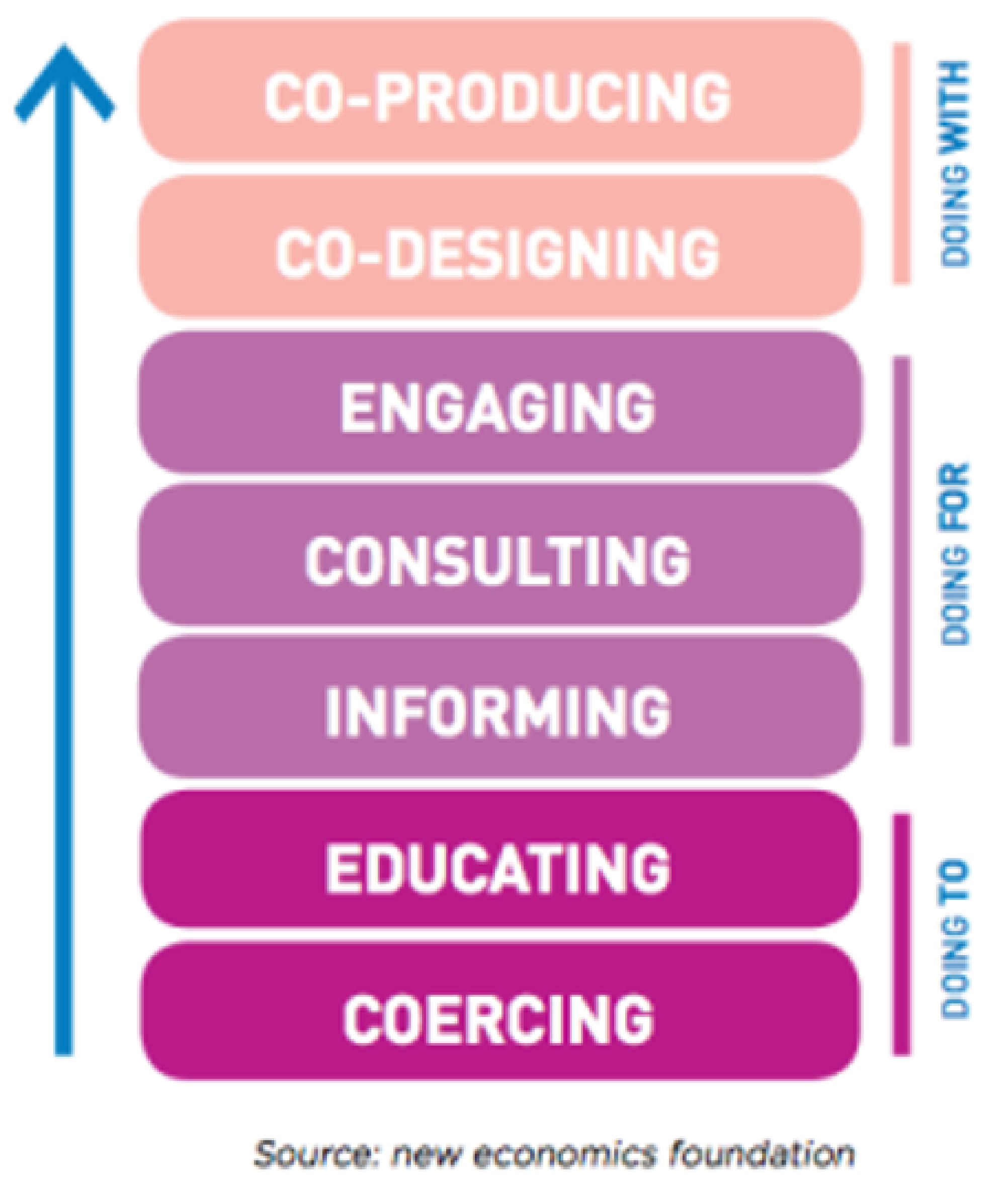
1.1. Co-Production—A Brief Introduction
1.2. Rationale
Objectives
- To determine the extent of the peer-reviewed literature into the concept of co-production within child and adolescent mental health,
- To synthesise and grade the available peer-reviewed literature captured within the search strategy,
- To create recommended actions to support the implementation of the principle for the next iteration of ‘A National Framework for Recovery in Mental Health’ and for those interested in implementing co-production within their local child and adolescent mental health service (CAMHS), and
- To make recommendations for future research into the concept of co-production within CAMHS.
2. Material and Methods
2.1. Epistemological Position
2.2. Eligibility Criteria
2.3. Information Sources
Search Strategy
- “young people” OR “children” OR “adolescents” OR “adolescence” OR “teenagers” OR “child”
- AND
- “co-production” OR “co-design” OR “co-delivery” OR “partnership working” OR “involvement” OR “participation” OR “co-creation” OR “co-innovation” OR “co-evaluation”
- AND
- “mental health” OR “mental illness” OR “psychiatric illness” OR “mental ill health” OR “mental” OR “psychiatric”
- AND
- “recovery” OR “mental health recovery” OR “mental well-being” OR “wellness” OR “self-care” OR “quality of life.”
2.4. Selection Process
Data Collection Process
2.5. Data Items
2.6. Risk of Bias Assessment
Assessing the Quality of Evidence
2.7. Synthesis Methods
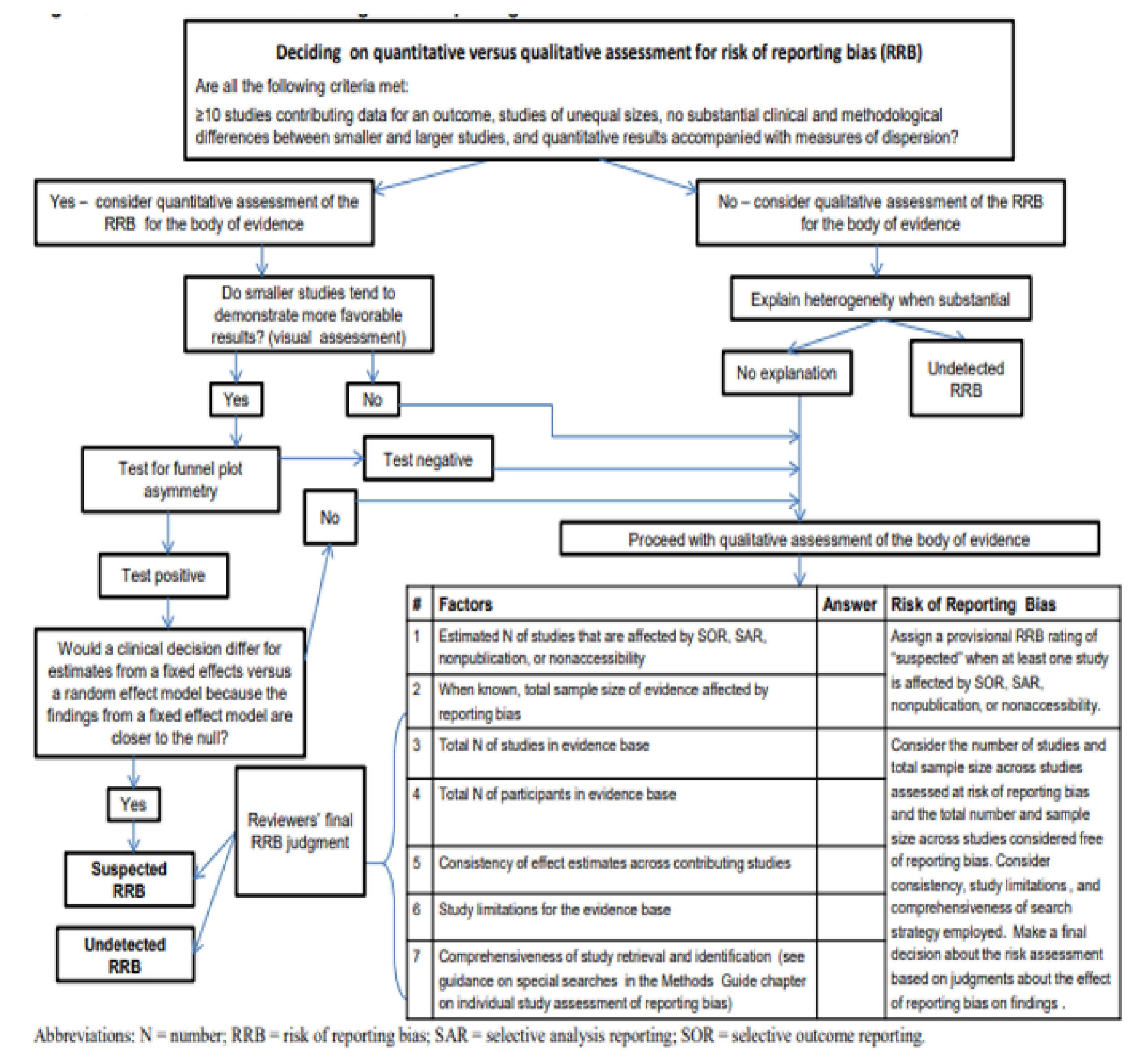
2.8. Reporting Bias Assessment
3. Results
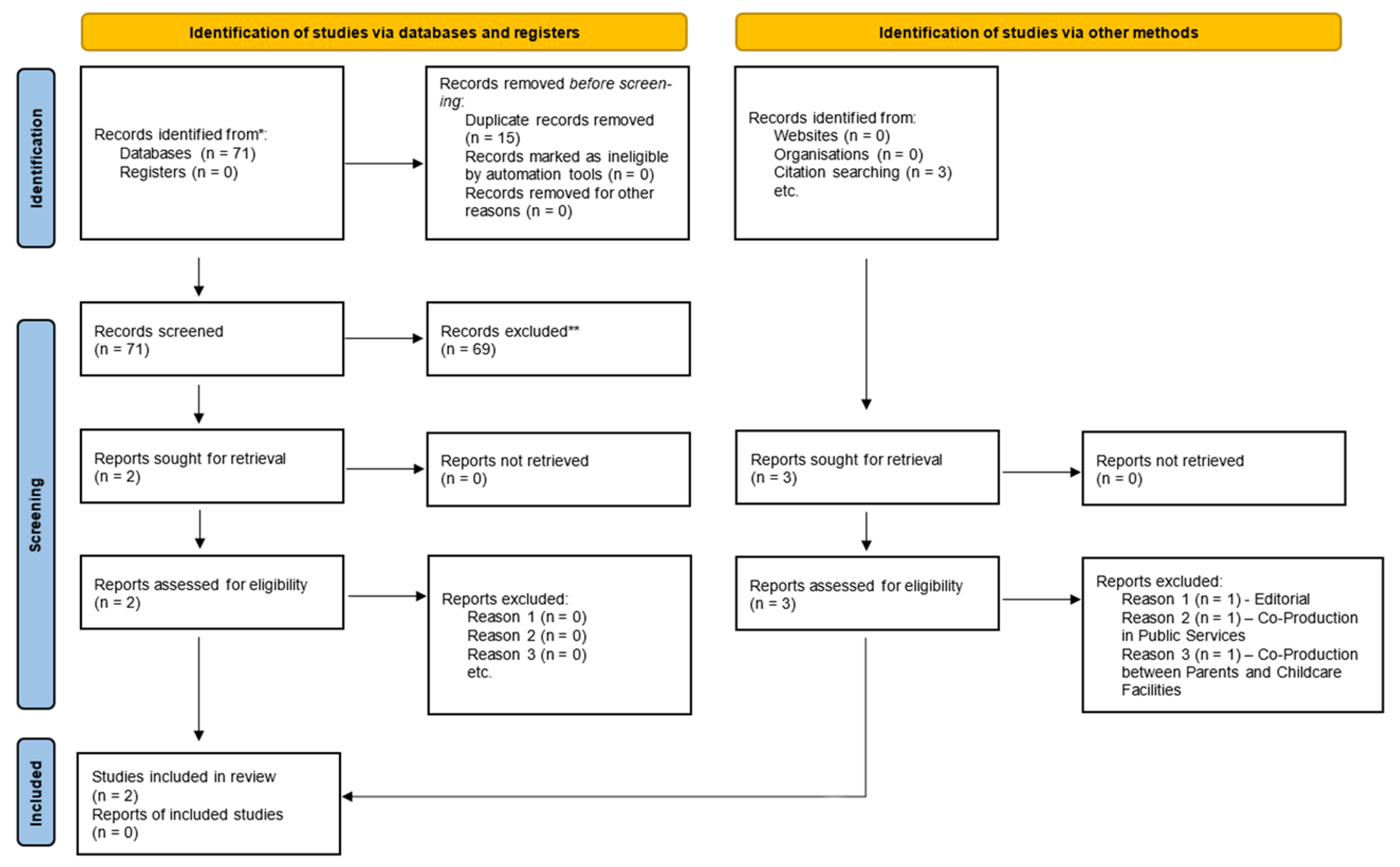
3.1. Study Selection
3.2. Study Characteristics
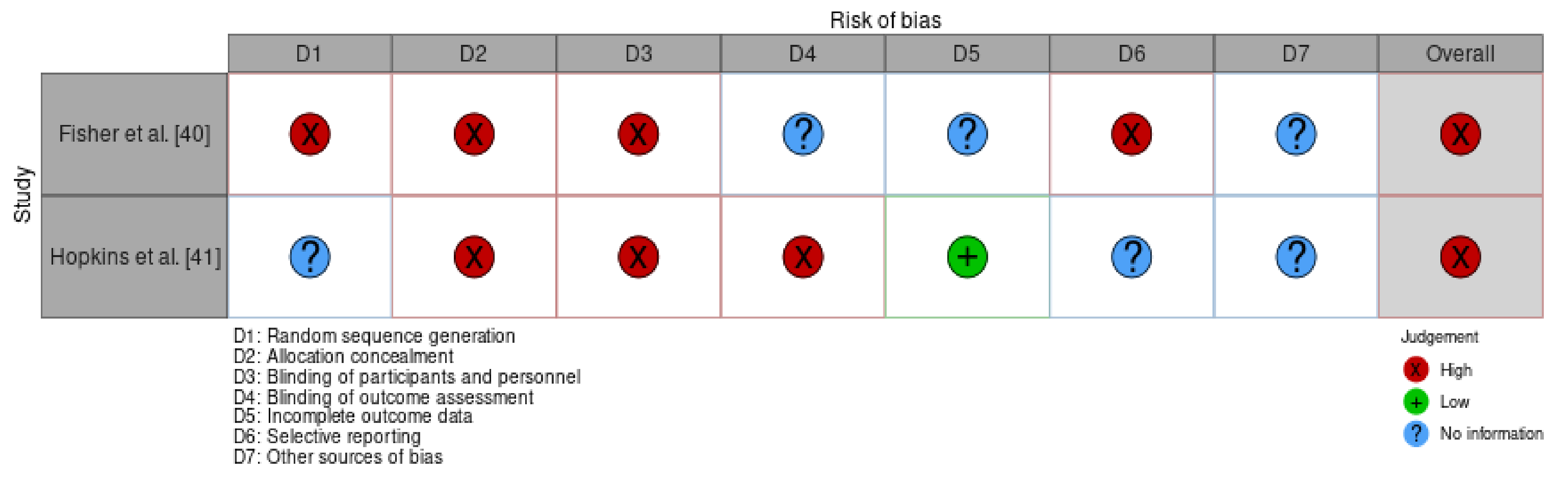
3.3. Risk of Bias in Studies
3.4. Results of Synthesis
3.4.1. Road Less Travelled
Identity in Society/Services
Acceptance
3.4.2. Co-Producing Equality
Re-Distribution of Power
Environment
Principles
- Assets rather than passive recipients of services
- Developing capacity by moving from deficit- to strength-based
- Encouraging mutuality in traditional relationships
- Blurring traditional boundaries that separate service providers from service users
- Network development to enable the transfer of knowledge between partners
- Facilitate rather than deliver services
3.5. Reporting Bias
4. Discussion
4.1. Results in the Context of the Current Literature and Areas for Future Research
4.2. Strengths and Weaknesses of the Current Review
5. Conclusions
6. Other Information
6.1. Registration and Protocol
6.2. Availability of Data, Code and Other Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Detailed Search Strategy
Appendix A.1. Search Strings

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| Qualitative, Mixed-Method Research Articles | Editorials, Quantitative Studies, Discussion Papers, Literature Reviews/Systematic Reviews/Meta-Syntheses, Meta-Analyses |
| English Language | |
| Peer Reviewed | |
| Child and Adolescent Mental Health Services | Addiction, Intellectual Disabilities, Physical Health, Older Person Services—Dementia, Delirium, etc., Dual Diagnosis |
| Dissertations | |
| Articles focused on co-production in young people | Article focused on co-production in older users of service |
Appendix A.2. Databases
Appendix A.3. Definition of Terms
Appendix A.4. Systematic Process
Appendix A.5. Results by Database
Appendix A.6. Pairing of Search Terms for Databases
Appendix A.7. Round 2 Article Inclusion/Exclusion
| Article | Included/Excluded | Rationale |
|---|---|---|
| Bovaird [42] | Excluded | Does not discuss co-production in CAMHS or with young people. Is not a qualitative study. |
| Broadhurst and Mason [43] | Excluded | Discusses co-presence—being in close proximity to a person to matter in what is being done. Not related to co-production. |
| Brophy et al. [44] | Excluded | Priorities for treatment, care, and support are discussed—not discussing co-production. |
| Cleofas [45] | Excluded | Is a research study on student participation. Participation is a lower level of involvement than co-production, and it was therefore excluded. |
| Collura et al. [46] | Excluded | Speaks of collaboration and not co-production. Collaboration is a lower level of involvement than co-production, as explained in the main body of text, and it was therefore excluded. |
| Conrad [47] | Excluded | Talks about social innovation in education, not co-production. |
| Cron [48] | Excluded | Discussion paper with no abstract. |
| Darra et al. [49] | Excluded | The research study is co-produced. It doesn’t discuss co-production. |
| Desha and Ziviani [50] | Excluded | Is a literature review. |
| Finkelstein et al. [51] | Excluded | Aim is to develop a children’s study intervention in co-occurring disorders. Does not speak of co-production. |
| Fisher et al. [40] | Included | Discusses how co-production is useful for survivors of childhood sexual abuse. |
| Fylan and Fylan [52] | Excluded | Study examines who should have access to health and social care records. No discussion of co-production or any level of involvement and was therefore excluded. |
| Garcia et al. [53] | Excluded | Talks about participatory research but not at the level of co-production. |
| Gerwin et al. [54] | Excluded | Talks of factors resulting in speech disorders in childhood, not co-production. |
| Gordon and O’Brien [55] | Excluded | An editorial—not a research study. |
| Granerud and Severinsson [56] | Excluded | Discusses how knowledge of social networks influences or impacts service providers’ practice. |
| Greenham et al. [57] | Excluded | A systematic review. |
| Haumann et al. [58] | Excluded | Talks of co-production in the corporate world. Not mental health related. |
| Hopkins et al. [41] | Included | Discusses participation and effects of attending co-produced recovery workshops for children and adolescents in mental health. |
| Horgan et al. [59] | Excluded | Sample consists of adults over the age of 18 years. |
| Hoyland et al. [60] | Excluded | Conference abstract. |
| Kendall et al. [61] | Excluded | Developing a participatory model for youth involvement in research. No mention of the higher-end involvement, including co-production. |
| Khoury [62] | Excluded | Discussion paper. |
| Lambert and Carr [63] | Excluded | Discussion paper. |
| Marston et al. [64] | Excluded | Talks about family involvement in creating a DVD resource for families. However, does not discuss higher-level involvement, including co-production. |
| McAnuff et al. [65] | Excluded | Discusses user participation in a research study. Does not discuss co-production. |
| McCauley et al. [66] | Excluded | Discusses the co-creation of an interview schedule to understand young adult mental health recovery. Only focuses on co-creation and not the entire co-production process. |
| McLeigh [67] | Excluded | Editorial paper. |
| McPherson et al. [68] | Excluded | A systematic scoping review. |
| Mundal et al. [69] | Excluded | RCT protocol. |
| Olasoji et al. [70] | Excluded | Discusses involvement in a nursing handover. No mention of co-production, which is a higher level of involvement. |
| Ott et al. [71] | Excluded | A policy-based analysis of narratives within school mental health. |
| Pavarini et al. [72] | Excluded | Discussion paper of co-production in research. |
| Pocobello et al. [73] | Excluded | Discusses co-production within adult services. |
| Riebschleger et al. [74] | Excluded | Talk of consumer parents’ recommendations for child psychoeducation. No co-production. |
| Robinson and Notara [75] | Excluded | Study involves young people’s relationships and connections with family. Not answering review question. |
| Robinson and Webber [76] | Excluded | A literature review. |
| Samuels et al. [77] | Excluded | Study examining factors that are associated with use and rejection of formal and informal resources. |
| Sattoe et al. [78] | Excluded | Study exploring patterns of autonomy and participation in young people’s services. No mention of possibility of higher-level involvement, such as that of co-production. |
| Schauer et al. [79] | Excluded | Study examining the value and use of shared decision making in mental health care. Once again, it is not clear if this shared decision-making is in line with co-production, and it was therefore excluded. |
| Simmons et al. [80] | Excluded | Study examining how peer workers can influence involvement of service users in shared decision making. Does not discuss co-production. |
| Souza et al. [81] | Excluded | Not related to co-production. |
| Stephenson et al. [82] | Excluded | Talks of co-production in adults and advanced decision making. |
| Stoyanov et al. [83] | Excluded | Explores how young people conceptualise and construct recovery. |
| Strokosch and Osborne [84] | Excluded | Looks at co-production with asylum seekers and not young people. |
| Susanti et al. [85] | Excluded | Looking at service user and carer perspectives of Patient and Public Involvement (PPI). |
| Tal-Seban et al. [86] | Excluded | Looks at what influences quality of life and participation in people with developmental coordination disorder. |
| Thom and Burnside [87] | Excluded | Discussion paper. |
| Trollvik et al. [88] | Excluded | Co-production in young people with physical co-morbidities. |
| Vis et al. [89] | Excluded | A scoping review. |
| Von Peter and Schulz [90] | Excluded | Psychiatrist perspective of what hinders co-production. |
| Walker et al. [91] | Excluded | Involvement of young people in research. Does not discuss higher-level involvement, including co-production. |
| Weaver [92] | Excluded | Discussion paper. |
| Wogden et al. [93] | Excluded | Shared decision making for physical co-morbidities. |
| Wright et al. [94] | Excluded | Talks of the co-occurrence of eating disorders and self-harm, not co-production. |
| Yeh et al. [95] | Excluded | Looks at the relationship between pain and mental health. |
| Article | Included/Excluded | Rationale |
|---|---|---|
| Fisher [96] | Excluded | Editorial Paper. |
| Osborne et al. [97] | Excluded | Focusses on co-production, but in public services. Not specific to health care and not specific to CAMHS. |
| Pestoff [98] | Excluded | Focusses on co-production between parents and childcare facilities in Europe. Not focused on CAMHS or child and adolescent mental health in general. |
Appendix B. Berkman and Colleagues’ Algorithm for Assessing Risk of Reporting Bias

References
- Dickinson, E. From madness to mental health: A brief history of psychiatric treatments in the UK from 1800 to the present. Br. J. Occup. Ther. 1990, 53, 419–424. [Google Scholar] [CrossRef]
- A Vision for Change: Report of the Expert Group on Mental Health Policy. Available online: https://www.hse.ie/eng/services/publications/mentalhealth/mental-health---a-vision-for-change.pdf (accessed on 16 August 2021).
- A National Service Framework for Mental Health. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/198051/National_Service_Framework_for_Mental_Health.pdf (accessed on 16 August 2021).
- Sharing the Vision: A Mental Health Policy for Everyone. Available online: https://www.gov.ie/en/publication/2e46f-sharing-the-vision-a-mental-health-policy-for-everyone/ (accessed on 18 August 2021).
- Swords, C.; Norton, M.J. Is sharing really caring? A vision or an aspiration? Ireland’s new mental health policy 2020. Ir. J. Psychol. Med. 2020, 1–2. [Google Scholar] [CrossRef] [PubMed]
- A National Framework for Recovery in Mental Health: A National Framework for Mental Health Service Providers to Support the Delivery of a Quality, Person Centred Service 2018–2020. Available online: https://www.hse.ie/eng/services/list/4/mental-health-services/advancingrecoveryireland/national-framework-for-recovery-in-mental-health/ (accessed on 16 August 2021).
- Co-Production in Practice Guidance Document 2018–2020: Supporting the Implementation of ‘A National Framework for Recovery in Mental Health 2018–2020’. Available online: https://www.hse.ie/eng/services/list/4/mental-health-services/advancingrecoveryireland/national-framework-for-recovery-in-mental-health/co-production-in-practice-guidance-document-2018-to-2020.pdf (accessed on 16 August 2021).
- Brudney, J.L.; England, R.E. Towards a definition of the co-production concept. Public Adm. Rev. 1983, 43, 59–65. [Google Scholar] [CrossRef]
- What is Co-Production. Available online: https://qi.elft.nhs.uk/wp-content/uploads/2017/01/what_is_co-production.pdf (accessed on 15 August 2021).
- Kleinman, A. Concepts and a model for the comparison of medical systems as cultural systems. Soc. Sci. Med. 1978, 12, 85–95. [Google Scholar] [CrossRef]
- Kleinman, A.; Benson, P. Anthropology in the clinic: The problem of cultural competency and how to fix it. PLoS Med. 2006, 3, e294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunston, R.; Lee, A.; Boud, D.; Broadie, P.; Chiarella, M. Co-Production and health system reform—From re-imagining to re-making. Aust. J. Public Adm. 2009, 68, 39–52. [Google Scholar] [CrossRef]
- The Challenge of Co-Production. Available online: https://neweconomics.org/2009/12/challenge-co-production/ (accessed on 15 August 2021).
- Vennik, F.D.; van de Bovenkamp, H.M.; Putters, K.; Grit, K.J. Co-production in healthcare: Rhetoric and practice. Int. Rev. Adm. Sci. 2016, 82, 150–168. [Google Scholar] [CrossRef]
- Brandsen, T.; Honingh, M. Distinguishing different types of co-production: A conceptual analysis based on the classical definitions. Public Adm. Rev. 2015, 6, 426–435. [Google Scholar] [CrossRef]
- Filipe, A.; Renedo, A.; Marston, C. The co-production of what? Knowledge, values and social relations in health care. PLoS Biol. 2017, 15, e2001403–e2001406. [Google Scholar] [CrossRef] [Green Version]
- Swords, C. Recovery and co-production: Understanding the diverging paradigms and potential implications for social work. Soc. Work. 2019. [Google Scholar]
- Norton, M. Implementing co-production in traditional statutory mental health services. Ment. Health Pract. 2019. [Google Scholar] [CrossRef]
- Arnstein, S.R. A ladder of citizen participation. J. Am. Inst. Plan. 1969, 35, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Foucault, M. Madness and Civilization: A History of Insanity in the Age of Reason; Random House Inc.: New York, NY, USA, 1988. [Google Scholar]
- Participation: It’s Impact on Services and the People Who Use Them. Available online: https://www.iriss.org.uk/resources/insights/participation-its-impact-services-and-people-who-use-them (accessed on 5 October 2021).
- Co-Production in Mental Health: A Literature Review. Available online: https://b.3cdn.net/nefoundation/ca0975b7cd88125c3e_ywm6bp3l1.pdf (accessed on 17 August 2021).
- Redman, S.; Greenhalgh, T.; Adedokun, L.; Staniszewska, S.; Denegri, S. The Co-production of Knowledge Collection Steering Committee. Co-Production of knowledge: The future. BMJ 2021, 372, n434. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Bryman, A. Social Research Methods, 4th ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Swords, C. An Exploration of How the Concept of Recovery in Mental Health is Socially Constructed and How It Impacts on the Delivery of Mental Health Services—An Irish Case Study; Unpublished; University of Dublin, Trinity College: Dublin, Ireland, 2021. [Google Scholar]
- Edwards, C.; Titchen, A. Research into patients’ perspectives relevance and usefulness of phenomenological sociology. J. Adv. Nurs. 2003, 44, 450–460. [Google Scholar] [CrossRef]
- Melnyk, B.M.; Fineout-Overholt, E.; Stillwell, S.B.; Williamson, K.M. The seven steps of evidence-based practice. Am. J. Nurs. 2010, 110, 51–53. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- McGuiness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An r package and shiny app for visualizing risk-of-bias assessments. Res. Synth. Methods 2020, 12, 55–61. [Google Scholar] [CrossRef]
- Hawker, S.; Payne, S.; Kerr, C.; Hardy, M.; Powell, J. Appraising the evidence: Reviewing disparate data systematically. Qual. Health Res. 2002, 12, 1284–1299. [Google Scholar] [CrossRef]
- Lorenc, T.; Petticrew, M.; Whitehead, M.; Neary, D.; Clayton, S.; Wright, K.; Thomson, H.; Cummins, S.; Sowden, A.; Renton, A. Crime, fear of crime and mental health: Synthesis of theory and systematic reviews of interventions and qualitative evidence. Public Health Res. 2014, 2, 1–398. [Google Scholar] [CrossRef] [Green Version]
- Norton, M.J.; Cuskelly, K. Family recovery interventions with families of mental health service users: A systematic review of the literature. Int. J. Environ. Res. Public Health 2021, 18, 7858. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Higgins, J.P.T. Tools for assessing risk of reporting bias in studies and synthesis of studies: A systematic review. BMJ Open 2018, 8, e019703. [Google Scholar] [CrossRef]
- McGauran, N.; Wieseler, B.; Kreis, J.; Schuler, Y.-B.; Kolsch, H.; Kaiser, T. Reporting bias in medical research—A narrative review. Trials 2010, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Burkman, N.D.; Lohr, K.N.; Ansari, M.; McDonagh, M.; Balk, E.; Whitlock, E.; Reston, J.; Bass, E.; Butler, M.; Gartlehner, G. Grading the strength of a body of evidence when assessing health care interventions for the effective health care program of the agency for healthcare research and quality: An update. In Methods Guide for Comparative Effectiveness Reviews; AHRQ Publication No. 13(14)-EHC130-EF; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013. Available online: https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/methods-guidance-grading-evidence_methods.pdf (accessed on 22 August 2021).
- Ludvigsen, M.S.; Hall, E.O.; Meyer, G.; Fegran, L.; Aagaard, H.; Uhrenfeldt, L. Using Sandelowski and Barroso’s meta-synthesis method in advanced qualitative evidence. Qual. Health Res. 2016, 26, 320–329. [Google Scholar] [CrossRef]
- Fisher, P.; Balfour, B.; Moss, S. Advocating co-productive engagement with marginalised people: A specific perspective on and by survivors of childhood sexual abuse. Br. J. Soc. Work 2018, 48, 2096–2113. [Google Scholar] [CrossRef]
- Hopkins, L.; Pedwell, G.; Lee, S. Educational outcomes of discovery college participation for young people. Ment. Health Soc. Incl. 2018, 22, 195–202. [Google Scholar] [CrossRef]
- Bovaird, T. Beyond engagement and participation: User and community co-production of public services. Public Adm. Rev. 2007, 67, 846–860. [Google Scholar] [CrossRef]
- Broadhurst, K.; Mason, C. Social work beyond the VDU: Foreground “co-presence” in situated practice—Why face-to-face practice matters. Br. J. Soc. Work 2014, 44, 578–595. [Google Scholar] [CrossRef]
- Brophy, L.; Bruxner, A.; Wilson, E.; Cocks, N.; Stylianou, M. How social work can contribute in the shift to personalized, recovery orientated psycho-social disability support services. Br. J. Soc. Work 2015, 45, i98–i116. [Google Scholar] [CrossRef]
- Cleofas, J.V. Student involvement, mental health and quality of life of college students in a selected university in Manila, Philippines. Int. J. Adolesc. Youth 2019, 25, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Collura, J.J.; Raffle, H.; Collins, A.L.; Kennedy, H. Creating spaces for young people to collaborate to create community change: Ohio youth-led initiative. Health Educ. Behav. 2019, 46, 42S–52S. [Google Scholar] [CrossRef] [PubMed]
- Conrad, D. Education and social innovation: The youth uncensored project—A case study of youth participatory research and cultural democracy in action. Can. J. Educ. 2015, 38, 1–25. [Google Scholar]
- Cron, T.O. The nature of “consumer health” as a public health concept. Public Health Rep. 1974, 96, 274–278. [Google Scholar]
- Darra, S.; Ward, M.R.M.; Jones, C.; Jones, S. Young parents’ experiences of a multi-agency young families project: Findings from a co-produced study. Child. Youth Serv. Rev. 2020, 116, 105146. [Google Scholar] [CrossRef]
- Desha, L.N.; Ziviani, J.M. Use of time in childhood and adolescence: A literature review on the nature of activity participation and depression. Aust. Occup. Ther. J. 2007, 54, 4–10. [Google Scholar] [CrossRef]
- Finkelstein, N.; O’Keefe, M.; Rechberger, E.; Gould, K.; Russell, L.A.; Mockus, S.; VanDeMark, N.R.; Rael, M.; Noether, C.D. Building resilience in children of mothers who have co-occuring disorders and histories of violence: Intervention model and implementation issues. J. Behav. Health Serv. Res. 2005, 32, 141–154. [Google Scholar] [CrossRef]
- Fylan, F.; Fylan, B. Co-creating social license for sharing health and care data. Int. J. Med Inform. 2021, 149, 104439. [Google Scholar] [CrossRef]
- Garcia, A.P.; Minkler, M.; Cardenas, Z.; Grills, C.; Porter, C. Engaging homeless youth in community-based participatory research: A case study from Skid Row, Los Angeles. Health Promot. Pract. 2014, 15, 18–27. [Google Scholar] [CrossRef]
- Gerwin, K.; Brosseau-Lapre, F.; Brown, B.; Christ, S.; Weber, C. Rhyme production strategies distinguish stuttering recovery and persistence. J. Speech Lang. Hear. Res. 2019, 62, 3302–3319. [Google Scholar] [CrossRef]
- Gordon, S.; O’Brien, A.J. Co-production: Power, problems and possibilities. Int. J. Ment. Health Nurs. 2018, 27, 1201–1203. [Google Scholar] [CrossRef] [Green Version]
- Granerud, A.; Severinsson, E. Knowledge about social networks and integration: A co-operative research project. J. Adv. Nurs. 2007, 58, 348–357. [Google Scholar] [CrossRef]
- Greenham, M.; Botchway, E.; Knight, S.; Bonyhady, B.; Tavender, E.; Schienberg, A.; Anderson, V.; Muscara, F. Predictors of participation and quality of life following major traumatic injuries in childhood: A systematic review. Disabil. Rehabil. 2020, 1–17. [Google Scholar] [CrossRef]
- Haumann, T.; Gunturkun, P.; Schons, L.M.; Wieseke, J. Engaging customers in co-production processes: How value-enhancing and intensity-reducing communication strategies mitigate the negative effects of co-production intensity. J. Mark. 2015, 79, 17–33. [Google Scholar] [CrossRef]
- Horgan, A.; Manning, F.; Bocking, J.; Happell, B.; Lahti, M.; Doody, R.; Griffin, M.; Bradley, S.K.; Russell, S.; Bjornsson, E.; et al. “To be treated as a human”: Using co-production to explore expert by experience involvement in mental health nursing education—The COMMUNE project. Int. J. Ment. Health Nurs. 2018, 27, 1282–1291. [Google Scholar] [CrossRef] [Green Version]
- Hoyland, M.; Moore, M.; Sanderson, L.; Geraghty, K. Challenging the status quo… Co-designing the future of child and youth mental health service with young people. Int. J. Integr. Care 2017, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kendal, S.E.; Milnes, L.; Welsby, H.; Pryjmachuk, S.; Coresearchers Group. Prioritizing young people’s emotional health support needs via participatory research. J. Psychiatr. Ment. Health Nurs. 2017, 24, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Khoury, E. Narrative matters: Mental health recovery—Considerations when working with youth. Child Adolesc. Ment. Health 2020, 25, 273–276. [Google Scholar] [CrossRef]
- Lambert, N.; Carr, S. “Outside the original remit”: Co-production in UK mental health research, lessons from the field. Int. J. Ment. Health Nurs. 2018, 27, 1273–1281. [Google Scholar] [CrossRef] [Green Version]
- Marston, N.; Reupert, A.; Mayberry, D.; Morgan, B. Working with and for parents to create a family focused DVD. Psychiatr. Rehabil. J. 2014, 37, 263–265. [Google Scholar] [CrossRef]
- McAnuff, J.; Brooks, R.; Duff, C.; Quinn, M.; Marshall, J.; Kolehmainen, N. Improving participation outcomes and interventions in neurodisability: Co-designing future research. Child Care Health Dev. 2016, 43, 298–306. [Google Scholar] [CrossRef]
- McCauley, C.-O.; McKenna, H.; Keeney, S.; McLoughlin, D. Service user engagement—A co-created interview schedule exploring mental health recovery in young people. J. Adv. Nurs. 2017, 73, 2361–2372. [Google Scholar] [CrossRef]
- McLeigh, J.D. Creating conditions that promote trust and participation by young people… and why it matters. Am. J. Orthopsychiatry 2015, 85, S67–S69. [Google Scholar] [CrossRef]
- McPherson, L.; Vosz, M.; Gatwiri, K.; Parmenter, N.; Macnamara, N.; Mitchell, J.; Tucci, J. What does research tell us about young people’s participation in decision making in residential care? A systematic scoping review. Child. Youth Serv. Rev. 2021, 122, 105899. [Google Scholar] [CrossRef]
- Mundal, I.; Grawe, R.W.; Hafstad, H.; Cuevas, C.D.L.; Lara-Cabrera, M.L. Effects of a peer co-facilitated educational programme for parents of children with ADHD: A feasibility randomized controlled trial protocol. BMJ Open 2020, 10, e039852. [Google Scholar] [CrossRef]
- Olasoji, M.; Plummer, V.; Shanti, M.; Reed, F.; Cross, W. The benefit of consumer involvement in nursing handover on acute inpatient unit: Post-implementation views. Int. J. Ment. Health Nurs. 2020, 29, 786–795. [Google Scholar] [CrossRef]
- Ott, M.; Hibbert, K.; Rodger SLeschied, A. A well place to be: The intersection of Canadian school-based mental health policy with student and teacher resiliency. Can. J. Educ. 2017, 40, 1–30. [Google Scholar]
- Pavarini, G.; Lorimer, J.; Manzini, A.; Goundry-Smith, E.; Singh, I. Co-producing research with youth: The NeurOx young people’s advisory group model. Health Expect. 2019, 22, 743–751. [Google Scholar] [CrossRef]
- Pocobello, R.; Sehity, T.E.; Negrogno, L.; Minervini, C.; Guida, M.; Venerito, C. Comparison of a co-produced mental health service to traditional services: A co-produced mixed-method cross-sectional study. Int. J. Ment. Health Nurs. 2020, 29, 460–475. [Google Scholar] [CrossRef]
- Riebschleger, J.; Onaga, E.; Tableman, B.; Byebee, D. Mental health consumer parents’ recommendations for designing psychoeducation interventions for their minor children. Psychiatr. Rehabil. J. 2014, 37, 183–185. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Notara, D. Building belonging and connection for children with disabilities and their families: A co-designed research and community development project in a regional community. Community Dev. J. 2015, 50, 724–741. [Google Scholar] [CrossRef]
- Robinson, K.; Webber, M. Models and effectiveness of service user and carer involvement in social work education: A literature review. Br. J. Soc. Work 2013, 43, 925–944. [Google Scholar] [CrossRef]
- Samuels, G.M.; Cerven, C.; Curry, S.R.; Robinson, S.R. “Nothing is for free…”: Youth attitudes about engaging resources while unstably housed. Cityscape A J. Policy Dev. Res. 2018, 20, 35–68. [Google Scholar]
- Sattoe, J.N.T.; Hilberink, S.R.; van Staa, A.; Bal, R. Lagging behind or not? Four distinctive social participation patterns among young adults with chronic conditions. J. Adolesc. Health 2014, 54, 397–403. [Google Scholar] [CrossRef]
- Schauer, C.; Everett, A.; del Vecchio, P.; Anderson, L. Promoting the value and practice of shared-decision making in mental health care. Psychiatr. Rehabil. J. 2007, 31, 54–61. [Google Scholar] [CrossRef]
- Simmons, M.B.; Batchelor, S.; Dimopolous-Bick, T. The choice project: Peer workers promoting shared decision making at a youth mental health service. Psychiatr. Serv. Adv. 2017, 8, 764–770. [Google Scholar] [CrossRef] [Green Version]
- Souza, L.B.d.; Panuncio-Pinto, M.P.; Fiorati, R.C. Children and adolescents in social vulnerability: Well-being, mental health and participation in education. Cardernos Bras. Ter. Ocup. 2019, 27, 251–269. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, L.A.; Gergel, T.; Keene, A.R.; Rifkin, L.; Owen, G. The PACT advanced decision-making template: Preparing for mental health act reform with co-production, focus groups and consultation. Int. J. Law Psychiatry 2020, 71, 101563. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Zelenko, O.; Staneva, A.; Kavanagh, D.J.; Smith, C.; Sade, G.; Cheers, J.; Hides, L. Development of the niggle app for supporting young people on their dynamic journey to well-being: Co-design and qualitative research study. JMIR Mhealth Uhealth 2021, 9, e21085. [Google Scholar] [CrossRef]
- Strokosch, K.; Osborne, S.P. Co-producing across organizational boundaries: Promoting asylum seeker integration in Scotland. Volunt. Int. J. Volunt. Non-Profit Organ. 2017, 28, 1881–1899. [Google Scholar] [CrossRef] [Green Version]
- Susanti, H.; James, K.; Utomo, B.; Keliat, B.-A.; Lovell, K.; Irmansyah, I.; Rose, D.; Colucci, E.; Brooks, H. Exploring the potential use of public and patient involvement to strengthen Indonesian mental health care for people with psychosis: A qualitative exploration of the views of service users and carers. Health Expect. 2020, 23, 377–387. [Google Scholar] [CrossRef] [Green Version]
- Tal-Seban, M.; Ornoy, A.; Parush, S. Young adults with developmental coordination disorder: A longitudinal study. Am. J. Occup. Ther. 2014, 68, 307–316. [Google Scholar] [CrossRef] [Green Version]
- Thom, K.; Burnside, D. Sharing power in criminal justice: The potential of co-production for offenders experiencing mental health and addiction in New Zealand. Int. J. Ment. Health Nurs. 2018, 27, 1258–1265. [Google Scholar] [CrossRef] [Green Version]
- Trollvik, A.; Eriksson, B.G.; Ringsberg, K.C.; Hummelvoll, J.K. Children’s participation and experiential reflections using co-operative inquiry for developing a learning programme for children with asthma. Action Res. 2012, 11, 31–51. [Google Scholar] [CrossRef]
- Vis, S.A.; Strandbu, A.; Holton, A.; Thomas, N. Participation and health—A research review of child participation in planning and decision-making. Child Fam. Soc. Work 2011, 16, 325–335. [Google Scholar] [CrossRef]
- Von Peter, S.; Schulz, G. “I-AS-We”—Powerful boundaries within the field of mental health co-production. Int. J. Ment. Health Nurs. 2018, 27, 1292–1300. [Google Scholar] [CrossRef] [Green Version]
- Walker, E.; Shaw, E.; Nunns, M.; Moore, D.; Thompson, J. No evidence synthesis about me without me: Involving young people in the conduct and dissemination of a complex evidence synthesis. Health Expect. 2021, 24, 122–133. [Google Scholar] [CrossRef]
- Weaver, B. Co-producing community justice: The transformative potential of personalization for penal sanctions. Br. J. Soc. Work 2011, 41, 1038–1057. [Google Scholar] [CrossRef]
- Wogden, F.; Norman, A.; Dibben, L. Treatment choice in adolescents with cleft lip and/or palate: The importance of shared decision-making. Cleft Palate-Craniofacial J. 2019, 56, 1220–1229. [Google Scholar] [CrossRef]
- Wright, F.; Bewick, B.M.; Barkham, M.; House, A.O.; Hill, A.J. Co-occurance of self-reported disordered eating and self-harm in UK university students. Br. J. Clin. Psychol. 2009, 48, 397–410. [Google Scholar] [CrossRef]
- Yeh, Y.-C.; Huang, M.-F.; Wu, Y.-Y.; Hu, H.-F.; Yen, C.-F. Pain, bullying involvement, and mental health problems among children and adolescents with ADHD in Taiwan. J. Atten. Disord. 2017, 23, 809–816. [Google Scholar] [CrossRef]
- Fisher, P. Co-production: What is it and where do we begin? J. Psychiatr. Ment. Health Nurs. 2016, 23, 345–346. [Google Scholar] [CrossRef] [Green Version]
- Osborne, S.P.; Radnor, Z.; Strokosch, K. Co-production and the co-creation of value in public services: A suitable case for treatment? Public Manag. Rev. 2016, 18, 639–653. [Google Scholar] [CrossRef] [Green Version]
- Pestoff, V. Citizens and co-production of welfare services: Childcare in eight European countries. Public Manag. Rev. 2006, 8, 503–519. [Google Scholar] [CrossRef]




| Inclusion | Exclusion |
|---|---|
| Qualitative, Mixed-Method Research Articles | Editorials, Quantitative Studies, Discussion Papers, Literature Reviews/Systematic Reviews/Meta-Syntheses, Meta-Analyses |
| English Language | |
| Peer Reviewed | |
| Child and Adolescent Mental Health Services | Addiction, Intellectual Disabilities, Physical Health, Older Person Services—Dementia, Delirium, etc., Dual Diagnosis |
| Dissertations | |
| Articles focused on co-production in young people | Articles focused on co-production in older users of service |
| Authors/Geographical Location | Study Aim | Sample and Sample Size | Age Range | Setting | Methodological Approach | Theoretical Orientation |
|---|---|---|---|---|---|---|
| Fisher et al. [40] United Kingdom | To examine the potential of co-production to combat power differentials and othering for survivors of childhood sexual abuse (CSA). | Authors of Paper [n = 2] | N/S | N/S | Autoethnographic Methodology | N/S |
| Hopkins et al. [41] Australia | To explore the reasons young people and adults enrol in Discovery College courses, what their experiences were, and whether attitudes towards education changed as a result of course participation. | Young People [n = 36] and Adults [n = 29] | N/S | Mental Health | Grounded Theory | N/S |
| Authors/Geographical Location | Synopsis of Included Studies |
|---|---|
| Fisher et al. [40] United Kingdom | Childhood sexual abuse has been known to cause power disparities not just in childhood but also in adulthood if not appropriately addressed. This study utilises an autoethnographic methodology to explore such power differential experiences while also examining the potential use of co-production to counteract such disparities of power and the associated othering that are experienced by survivors of such abuse. |
| Hopkins et al. [41] Australia | The Discovery College is a new initiative in Australia that aims to provide co-produced recovery education delivered through an andragogical approach, whereby facilitators and participants learn together through an equal relationship. Despite the growth in popularity of such initiatives in mental health services, little evidence thus far is available to demonstrate the effectiveness nor participant experiences of such colleges. This mixed-method study was therefore carried out to explore the reasons why young adults and adults enrol in such colleges and their experiences of participating and also to measure attitudinal changes resulting from course participation. |
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Overall |
|---|---|---|---|---|---|---|---|
| Fisher et al. [40] | High | High | High | Unclear | Unclear | High | High |
| Hopkins et al. [41] | Unclear | High | High | High | Low | Unclear | High |
| Study | Abstract/Title | Introduction/Aims | Method and Data | Sampling | Analysis | Ethics/Bias | Results | Generalisability | Implications | Total | Grade |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fisher et al. [40] | 3 | 3 | 3 | 3 | 1 | 1 | 2 | 2 | 3 | 21 | C |
| Hopkins et al. [41] | 4 | 4 | 4 | 2 | 2 | 1 | 3 | 3 | 4 | 27 | B |
| Themes | Sub-Themes |
|---|---|
| Road Less Travelled | Identity in Society/Services |
| Acceptance | |
| Co-Producing Equality | Redistribution of Power |
| Environment | |
| Principles |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norton, M.J. Co-Production within Child and Adolescent Mental Health: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11897. https://doi.org/10.3390/ijerph182211897
Norton MJ. Co-Production within Child and Adolescent Mental Health: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(22):11897. https://doi.org/10.3390/ijerph182211897
Chicago/Turabian StyleNorton, Michael John. 2021. "Co-Production within Child and Adolescent Mental Health: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 22: 11897. https://doi.org/10.3390/ijerph182211897
APA StyleNorton, M. J. (2021). Co-Production within Child and Adolescent Mental Health: A Systematic Review. International Journal of Environmental Research and Public Health, 18(22), 11897. https://doi.org/10.3390/ijerph182211897