
“Do Elite Sport First, Get Your Period Back Later.” Are Barriers to Communication Hindering Female Athletes?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
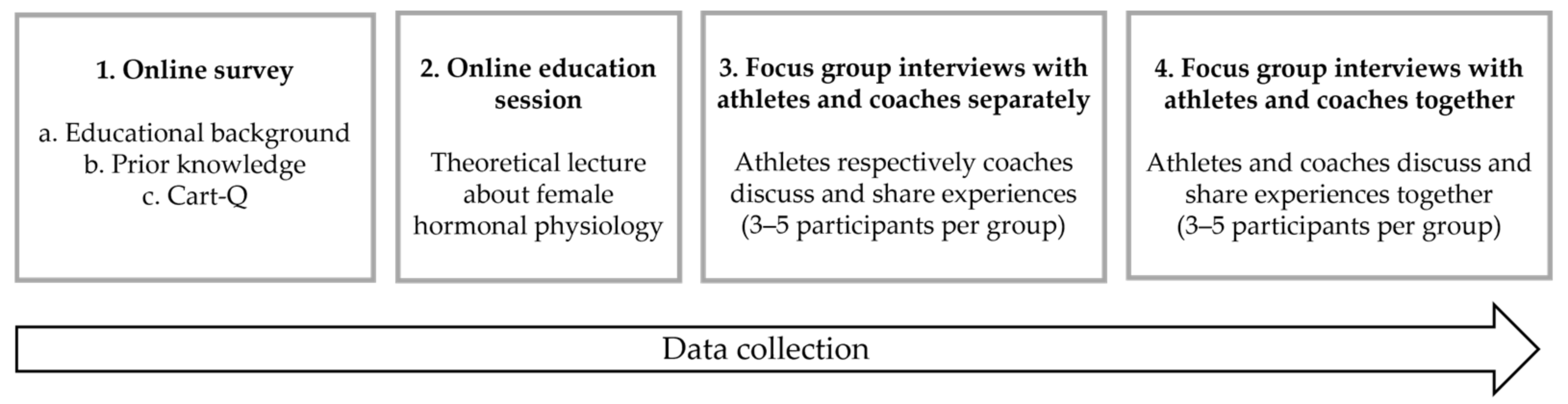
2.2.1. Overview
2.2.2. Online Survey
2.2.3. Online Education Session
2.2.4. Focus-Group Interviews
2.3. Data Analysis
3. Results
3.1. Online Survey
3.2. Focus-Group Interviews
3.2.1. Theme 1: Knowledge Barriers
“I think, because you don’t have so much knowledge about it [the female hormonal cycle], then… I feel that when I start to talk about it I don’t really know what’s right or wrong. Or maybe there is no right or wrong. But it might be that you don’t really know so much about it.”(Kristina)
“There is some kind of uncertainty and you don’t really know [what’s right or wrong], so it’s hard to share that much with others when you don’t really know.”(Gunilla)
“So, contraceptives have sort of more functions than how I think men [male coaches] see contraceptives. Like, contraception isn’t only to stop us from getting pregnant, as many men think, I think. But contraception also has the ability to reduce hormonal fluctuations, it has the ability to reduce period pains and you end up maybe more in balance. So it’s not necessarily just in terms of protecting yourself against becoming pregnant. So I think it can be important to talk about it regardless [of why we use contraceptives]. Yeah, but like… who should take it up, I don’t know.”
“I think I… To talk about contraceptives for me, that feels a bit tough, in general.”
“If you take the pill it’s like: “No, that [training according to the MC] doesn’t affect me anyway”, so instead you can hardly be bothered to listen… and maybe that’s stupid.”
“I remember when I was a junior I heard this thing about menstruation. Yeah, kind of like, if you have your period then you’re not training enough.”(Celine)
“I have experience of that from when I went to the ski high school and was at that age that when I missed my period and, like, told my parents and maybe my ski high school coaches, it was more: ‘That’s completely normal… that’s what happens when you train a lot. Then it [your period] will disappear.’ And then I didn’t think there was anything wrong with me.”(Lotta)
“I have a practical example [an athlete], in fact, who has done that actually since May, so planned according to it [the menstrual cycle]. And I can say that I have become more… even more questions now, half a year later, than I had back in the spring. There are no regularities in… there are regularities in menstruation, but not in performance.”(Samuel)
“It’s damn hard! There are so many factors. We can’t standardize and say that this is because of the MC… there are so many parameters that affect form, so it’s hard.”(Oskar)
“We shouldn’t barge into this area. Yeah, but [if an athlete asks]: ‘Shall we try and change contraception methods?’ ‘Yeah, I think so!’ I can’t stand there and say that! Well I can, but it wouldn’t be good!” [The group laughs]
3.2.2. Theme 2: Interpersonal Barriers
“If I’d had bigger problems, and felt that it affected me noticeably, then I might have mentioned it [my MC]. Because I think it’s important to perform well like, but I don’t think that’s a problem … No, so I don’t talk about it…”(Helena, who rated closeness to her coach as 7.0)
“Of course it feels private, but it also feels quite important. I’ve sometimes thought, like, is it [contraceptive use] dangerous? Or will it harm my performance if I take this [contraception]? Like, you think about it and you kind of want to know, can I take this contraception without it negatively affecting me in some way? Because it’s kind of like… It still affects the body, so it’s more like that. You don’t know that much. You want to know more about it, like…”
“Yeah, in the beginning, the first years, I could say to the coach that I had a stomach ache and I could go home, like. I mean, I didn’t even dare to say that I was on my period. And then I came back the next day, like. But, people have always been a bit like that. At least I have.”
“I think it’s good to take this up as a junior too… Now I can be open and honest about it [menstruation], but I couldn’t have been like that as a junior. I couldn’t have talked about menstruation then… I didn’t have a single thought about talking to coaches about it, because I wouldn’t have dared.”
“But I think it would have been easier to talk about if it had been a female coach, for sure. Because that feels natural, like.”
“I don’t know if it would be different if I had a female coach. If that makes a difference too. Or that it kind of feels more… that they understand more. Even though… I don’t think it feels embarrassing to talk about the menstrual cycle. But just the understanding, that it might be easier to talk to a female coach.”
“We have our own experiences, but it’s our body and no menstruation is the same. So just because I’ve had it one way doesn’t mean that all of my athletes experience it in the same way I have, that’s how it is… But then I know what period pains are and I know what it’s like to lie in bed in the fetal position for 24 hours, I know what that’s like… but that’s so different for everyone, so it’s really important even for us female coaches to broaden our knowledge and understand…”
“Us guys are a bit more out of our depth there. It’s a bit… there’s an extra barrier, so you need even more trust, I think, to be able to talk about this.”
“It can be difficult knowing whether the athlete you are meeting will feel the same… “Why should I share this with you?”, like: “Why do you want to know about that?”, or like: “Why is that relevant?”, and so on… And somehow it’s also quite private.”
“When I have training talks with my athletes a natural question is: “How is your training going?”, “How are you feeling about this [your MC]?”. And thank goodness, I’ve hardly had any athletes with a problem … I’ve never had anyone with problems… I always have it [the MC] as a standard question in all meetings with my [female] athletes. I’ve never had any problems bringing it [the MC] up.”
“I wouldn’t say it’s so bad that no-one talks about it at all. But it [talking about the MC] does require that you know them [the athletes] pretty well.”
3.2.3. Theme 3: Structural Barriers
“So I think they [the athletes] play along. The ones who have some idea about this, they know that they can say that they don’t have their period because they take the pill and that’s true in a way, but really it’s because they are too thin and that’s damn hard to deal with if you [the coach] can’t follow up on this [the athlete’s health] whenever needed.”
“To get a regular period we might have to increase the body weight and then there will be a clash for the athlete… “gain weight, [but] I need to compete for some more years, so what do I do?” And then you have created a bigger problem in their minds, so it isn’t easy.”
“The best thing for your body is to not do elite sport, as you do. The best thing in the world, that’s to have some regularity [in your menstrual cycles], yes, but: ‘Now I’ll eat more fat to get my period back’… that doesn’t go hand-in-hand with elite sport.”
“When I started to discuss this with the coaches it was more like: ‘Yeah, maybe you should do one thing at a time; do elite sport first and get your period back later. Maybe you can’t expect to have both at the same time…’ And that felt a bit like: That’s not how I want it to be, I feel like it should be possible to have periods and optimize [my] performance.”
“Based on what a year of training looks like it’s quite difficult to find the time to make changes, because you can’t do it during the season and it wouldn’t add so much doing it in April during the recovery period where the training volume is lower.”
“It sounds exciting when you hear of studies about how strength training and stuff can have an effect… and then you had hoped that you could include it in your own training plan. I took it up with Oskar and Tommy, that: Now I’ve stopped taking the pill, so I’ll let you know when I get my period back [so that I could train according to my menstrual cycle]. And then half a year later: No, it’s not time yet [I still haven’t got my period back].”
“Yeah, but I don’t feel very comfortable with it. It’s probably not, like, me who brings it up in the first place either.”
“I started taking the pill when I was maybe 15, and it was the nurse back home in [hometown] or [another town]… and since then it’s just carried on. I haven’t, like, asked anyone else what they do. So that was an eye-opener for me [discussing the female hormonal cycle with other teammates in an organized way].”
“I would say that it’s very, very rare, if it even happens at all, that the girls take it up. It’s more like the opposite, that you have to ask.”(Hampus)
4. Discussion
4.1. Limitations
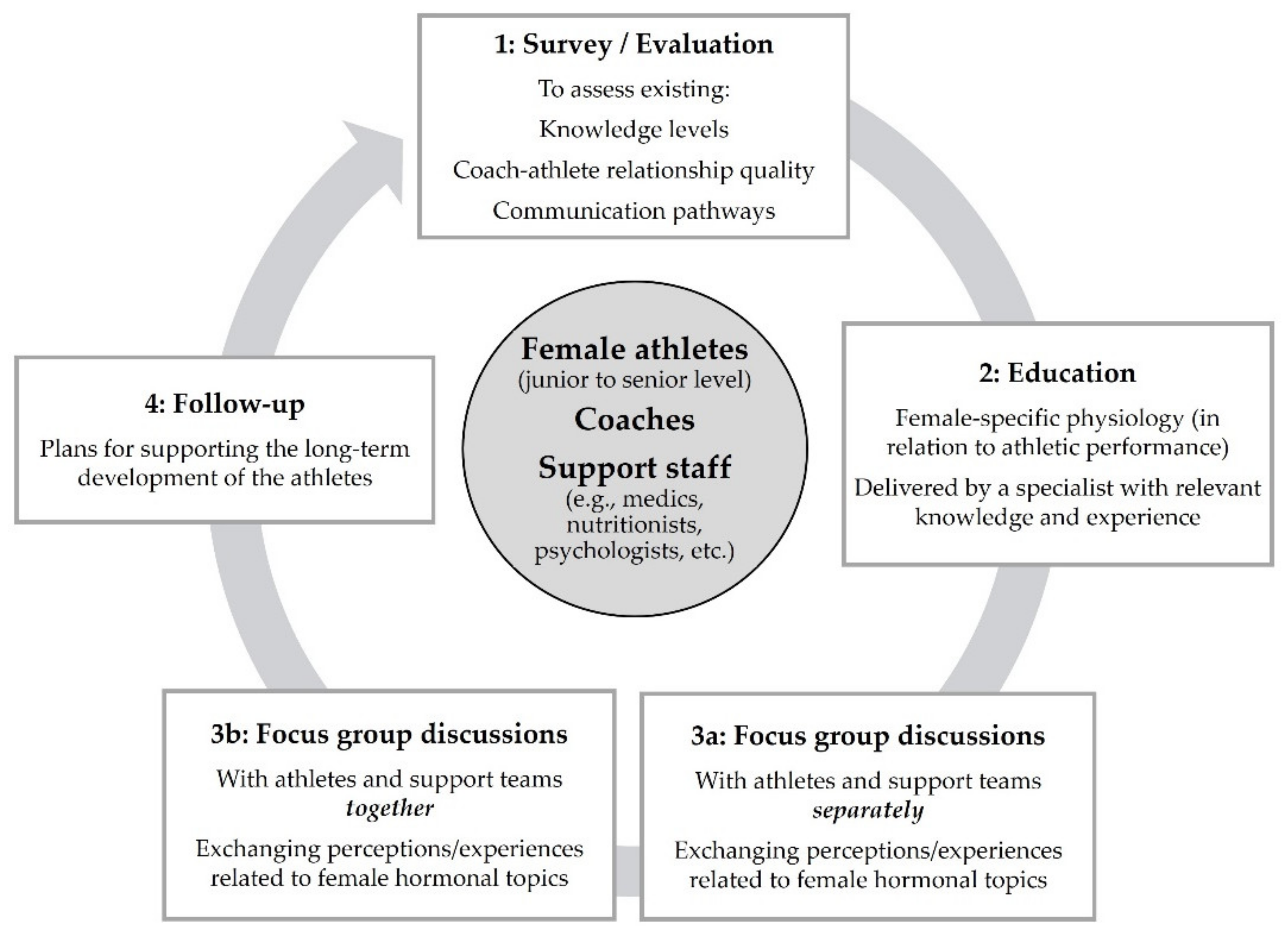
4.2. Practical Applications and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Jowett, S.; Poczwardowski, A. Understanding the coach-athlete relationship. In Social Psychology in Sport; Jowett, S., Lavalle, D., Eds.; Human Kinetics: Champaign, IL, USA, 2007; pp. 3–10. [Google Scholar]
- Jowett, S. Coaching effectiveness: The coach-athlete relationship at its heart. Curr. Opin. Psychol. 2017, 16, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinberg, R.S. Goal setting in sport and exercise: Research and practical applications. Rev. Educ. Fis. 2013, 24, 171–179. [Google Scholar] [CrossRef]
- Jowett, S.; Ntoumanis, N. The Coach-Athlete Relationship Questionnaire (CART-Q): Development and initial validation. Scand. J. Med. Sci. Sports 2004, 14, 245–257. [Google Scholar] [CrossRef]
- Rhind, D.; Jowett, S.; Yang, S. A comparison of athletes’ perceptions of the coach-athlete relationship in team and individual sports. J. Sport Behav. 2012, 35, 433–452. [Google Scholar]
- Lorimer, R.; Jowett, S. Empathic accuracy in coach–athlete dyads who participate in team and individual sports. Psychol. Sport Exerc. 2009, 10, 152–158. [Google Scholar] [CrossRef]
- Lorimer, R.; Jowett, S. Feedback of information in the empathic accuracy of sport coaches. Psychol. Sport Exerc. 2010, 11, 12–17. [Google Scholar] [CrossRef]
- Davis, L.; Jowett, S.; Tafvelin, S. Communication strategies: The fuel for quality coach-athlete relationships and athlete satisfaction. Front. Psychol. 2019, 10, 2156. [Google Scholar] [CrossRef] [PubMed]
- Bruinvels, G.; Burden, R.J.; McGregor, A.J.; Ackerman, K.E.; Dooley, M.; Richards, T.; Pedlar, C. Sport, exercise and the menstrual cycle: Where is the research? Br. J. Sports Med. 2017, 51, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Costello, J.T.; Bieuzen, F.; Bleakley, C.M. Where are all the female participants in sports and exercise medicine research? Eur. J. Sport Sci. 2014, 14, 847–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, A.; Govus, A.; Donaldson, A. What male coaches want to know about the menstrual cycle in women’s team sports: Performance, health, and communication. Int. J. Sports Sci. Coach. 2021, 16, 544–553. [Google Scholar] [CrossRef]
- Kroshus, E.; Sherman, R.T.; Thompson, R.A.; Sossin, K.; Austin, S.B. Gender differences in high school coaches’ knowledge, attitudes, and communication about the female athlete triad. Eat. Disord. 2014, 22, 193–208. [Google Scholar] [CrossRef]
- Armour, M.; Parry, K.A.; Steel, K.; Smith, C.A. Australian female athlete perceptions of the challenges associated with training and competing when menstrual symptoms are present. Int. J. Sports Sci. Coach. 2020, 15, 316–323. [Google Scholar] [CrossRef]
- Findlay, R.J.; Macrae, E.H.R.; Whyte, I.Y.; Easton, C.; Forrest, L.J. How the menstrual cycle and menstruation affect sporting performance: Experiences and perceptions of elite female rugby players. Br. J. Sports Med. 2020, 54, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Solli, G.S.; Sandbakk, S.B.; Noordhof, D.A.; Ihalainen, J.K.; Sandbakk, Ø. Changes in self-reported physical fitness, performance, and side effects across the phases of the menstrual cycle among competitive endurance athletes. Int. J. Sports Physiol. Perform. 2020, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Anderl, C.; Li, G.; Chen, F.S. Oral contraceptive use in adolescence predicts lasting vulnerability to depression in adulthood. J. Child. Psychol. Psychiatry Allied Discip. 2020, 61, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Lebrun, C.M.; Petit, M.A.; Mckenzie, D.C.; Taunton, J.E. Decreased maximal aerobic capacity with use of a triphasic oral contraceptive in highly active women: A randomised controlled trial. Br. J. Sports Med. 2003, 37, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, M.A.; Jenkins, D.G.; Janse De Jonge, X.A.K.; Emmerton, L.M.; Skinner, T.L. Oral contraceptive use dampens physiological adaptations to sprint interval training. Med. Sci. Sports Exerc. 2017, 49, 717–727. [Google Scholar] [CrossRef]
- Martin, D.; Sale, C.; Cooper, S.B.; Elliott-Sale, K.J. Period prevalence and perceived side effects of hormonal contraceptive use and the menstrual cycle in elite athletes. Int. J. Sports Physiol. Perform. 2018, 13, 926–932. [Google Scholar] [CrossRef] [Green Version]
- Brown, N.; Knight, C.J.; Forrest, L.J. Elite female athletes’ experiences and perceptions of the menstrual cycle on training and sport performance. Scand. J. Med. Sci. Sports 2020, 31, 52–69. [Google Scholar] [CrossRef]
- Larsen, B.; Morris, K.; Quinn, K.; Osborne, M.; Minahan, C. Practice does not make perfect: A brief view of athletes’ knowledge on the menstrual cycle and oral contraceptives. J. Sci. Med. Sport 2020, 23, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.X.; Jowett, S. Psychometric properties of the Coach-Athlete Relationship Questionnaire (CART-Q) in seven countries. Psychol. Sport Exerc. 2012, 13, 36–43. [Google Scholar] [CrossRef]
- Gratton, C.; Jones, D. Research Methods for Sports Studies, 3rd ed.; Gratton, C., Jones, D.I., Eds.; Routledge: Oxon, UK, 2014. [Google Scholar]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice, 4th ed.; SAGE: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Vaughn, S.; Schumm, J.S.; Sinagub, J. Focus Group Interviews in Education and Psychology; SAGE Publications: Thousand Oaks, CA, USA, 1996. [Google Scholar]
- De Souza, M.J.; Nattiv, A.; Joy, E.; Misra, M.; Williams, N.I.; Mallinson, R.J.; Gibbs, J.C.; Olmsted, M.; Goolsby, M.; Matheson, G. Expert Panel. 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad: Proceedings of 1st International Conference, USA, San Francisco, California, May 2012 and 2nd International Conference held in Indianapolis, Indiana, May 2013. Br. J. Sports Med. 2014, 48, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kingsberg, S.A.; Schaffir, J.; Faught, B.; Pinkerton, J.V.; Parish, S.J.; Iglesia, C.B.; Gudeman, J.; Krop, J.; Simon, J.A. Female sexual health: Barriers to optimal outcomes and a roadmap for improved patient-clinician communications. J. Women’s Health 2019, 28, 432–443. [Google Scholar] [CrossRef] [Green Version]
- Rubinsky, V.; Gunning, J.N.; Cooke-Jackson, A. “I thought I was dying:” (Un)supportive communication surrounding early menstruation experiences. Health Commun. 2020, 35, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.W.; Lindblom, H.P.; Karlsson, Ø.; Andersson, E.P.; McGawley, K. Anthropometric, physiological, and performance developments in cross-country skiers. Med. Sci. Sports Exerc. 2021, 53, 2553–2564. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pseudonym | Age (y) | Highest Level of Education | Prior Education * | Commitment | CART-Q Closeness | Complementarity |
|---|---|---|---|---|---|---|
| Lena | 20–25 | Upper secondary school | 3–4 | 6.0 (1.4) | 7.0 (0.0) | 6.3 (1.3) |
| Celine | 20–25 | University, other | 1–2 | 5.3 (1.2) | 6.8 (0.4) | 6.3 (0.4) |
| Helena | 20–25 | University, other | 1–2 | 6.7 (0.5) | 7.0 (0.0) | 7.0 (0.0) |
| Josefin | 20–25 | University, sport sci | 1–2 | 6.0 (1.4) | 7.0 (0.0) | 7.0 (0.0) |
| Greta | 20–25 | University, other | 1–2 | 5.0 (2.8) | 7.0 (0.0) | 7.0 (0.0) |
| Alexandra | 20–25 | University, sport sci | 3–4 | 7.0 (0.0) | 6.8 (0.4) | 5.0 (1.2) |
| Lotta | 20–25 | University, other | 1–2 | 5.0 (2.8) | 7.0 (0.0) | 7.0 (0.0) |
| Bodil | 20–25 | University, other | 1–2 | 6.5 (0.5) | 7.0 (0.0) | 7.0 (0.0) |
| Jennifer | 26–35 | University, other | 0 | 6.0 (1.4) | 7.0 (0.0) | 7.0 (0.0) |
| Kristina | 26–35 | University, other | 1–2 | 6.0 (0.0) | 6.3 (0.4) | 5.3 (0.4) |
| Marie | 26–35 | University, other | 1–2 | 5.7 (1.2) | 7.0 (0.0) | 6.8 (0.4) |
| Gunilla | 26–35 | Upper secondary school | 1–2 | 5.0 (2.2) | 7.0 (0.0) | 7.0 (0.0) |
| Amanda | 26–35 | University, sport sci | 1–2 | 5.7 (1.2) | 5.5 (0.9) | 6.0 (0.0) |
| Mean (SD) | 5.9 (0.6) | 6.8 (0.4) | 6.5 (0.7) |
| Pseudonym | Age (y) | Highest Level of Education | Prior Education * | Commitment | CART-Q Closeness | Complementarity |
|---|---|---|---|---|---|---|
| Elisabet (F) | 30–45 | University, sport sci | >5 | 6.0 (0.8) | 6.5 (0.5) | 6.5 (0.5) |
| Erika (F) | 46–60 | University, coach education | 0 | 5.7 (1.2) | 7.0 (0.0) | 6.8 (0.4) |
| Daniel (M) | 30–45 | University, sport sci | >5 | 5.7 (1.2) | 6.8 (0.4) | 6.5 (0.5) |
| Samuel (M) | 30–45 | University, coach education | 1–2 | 7.0 (0.0) | 7.0 (0.0) | 7.0 (0.0) |
| Tommy (M) | 46–60 | University, sport sci | 1–2 | 7.0 (0.0) | 7.0 (0.0) | 6.5 (0.9) |
| Hampus (M) | 46–60 | University, coach education | 3–4 | 6.3 (0.5) | 6.5 (0.5) | 6.8 (0.4) |
| Oskar (M) | 46–60 | University, other | 1–2 | 6.3 (0.9) | 6.8 (0.4) | 6.3 (0.4) |
| Arild (M) | 46–60 | University, other | >5 | 5.0 (1.4) | 7.0 (0.0) | 6.8 (0.4) |
| Mean (SD) | 6.1 (0.6) | 6.8 (0.2) | 6.6 (0.2) |
| Main Theme | Athlete Perspective | Coach Perspective |
|---|---|---|
| Knowledge | Limited knowledge (e.g., not knowing what is right or wrong) Concerns expected to be outside the knowledge area of the coach (e.g., contraceptives) General MC recommendations perceived as vague in relation to the elite athlete context Believing that MC matters do not concern them, such as HC use | Lack of MC-/HC-specific knowledge and frameworks/guidelines Concerns considered to be outside their knowledge area (e.g., contraceptives) Challenging to incorporate MC research into sport-specific practice (e.g., training plans, individual variation and complexity of athlete performance—lack of useful guidelines) Doubts regarding potential benefits of training according to the MC (e.g., optimizing athlete performance is the highest priority, the MC is just one piece of the puzzle) |
| Interpersonal | Not having any, or large enough, MC-related problems Feeling uncomfortable/inexperienced discussing the MC and HC use with coaches or teammates (but more natural talking to a female coach) Coach–athlete relationship (e.g., closeness, level of trust and confidence between coach and athlete) | Perceived taboo and respecting athletes’ privacy Topic beyond the comfort zone or feeling unsure how to help athletes (e.g., timing and approach) Coach–athlete relationship (e.g., closeness, level of trust and confidence between coach and athlete) |
| Structural | Lack of formal or organized discussion forums/education No or little experience of teammates sharing their hormonal matters or questions with each other The endurance athlete dilemma (e.g., the importance of being light weight and training enough versus having a regular MC) | Lack of formal or organized discussion forums/education Lack of structures in place for discussing the female hormonal cycle with athletes, coaches and support staff (e.g., medical, nutritionist, etc.) The coach dilemma (e.g., the importance of athletes being light weight and training enough versus having a regular MC) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Höök, M.; Bergström, M.; Sæther, S.A.; McGawley, K. “Do Elite Sport First, Get Your Period Back Later.” Are Barriers to Communication Hindering Female Athletes? Int. J. Environ. Res. Public Health 2021, 18, 12075. https://doi.org/10.3390/ijerph182212075
Höök M, Bergström M, Sæther SA, McGawley K. “Do Elite Sport First, Get Your Period Back Later.” Are Barriers to Communication Hindering Female Athletes? International Journal of Environmental Research and Public Health. 2021; 18(22):12075. https://doi.org/10.3390/ijerph182212075
Chicago/Turabian StyleHöök, Martina, Max Bergström, Stig Arve Sæther, and Kerry McGawley. 2021. "“Do Elite Sport First, Get Your Period Back Later.” Are Barriers to Communication Hindering Female Athletes?" International Journal of Environmental Research and Public Health 18, no. 22: 12075. https://doi.org/10.3390/ijerph182212075
APA StyleHöök, M., Bergström, M., Sæther, S. A., & McGawley, K. (2021). “Do Elite Sport First, Get Your Period Back Later.” Are Barriers to Communication Hindering Female Athletes? International Journal of Environmental Research and Public Health, 18(22), 12075. https://doi.org/10.3390/ijerph182212075