
Associations of Childcare Arrangements with Adiposity Measures in a Multi-Ethnic Asian Cohort: The GUSTO Study

 , , , ,
, , , ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
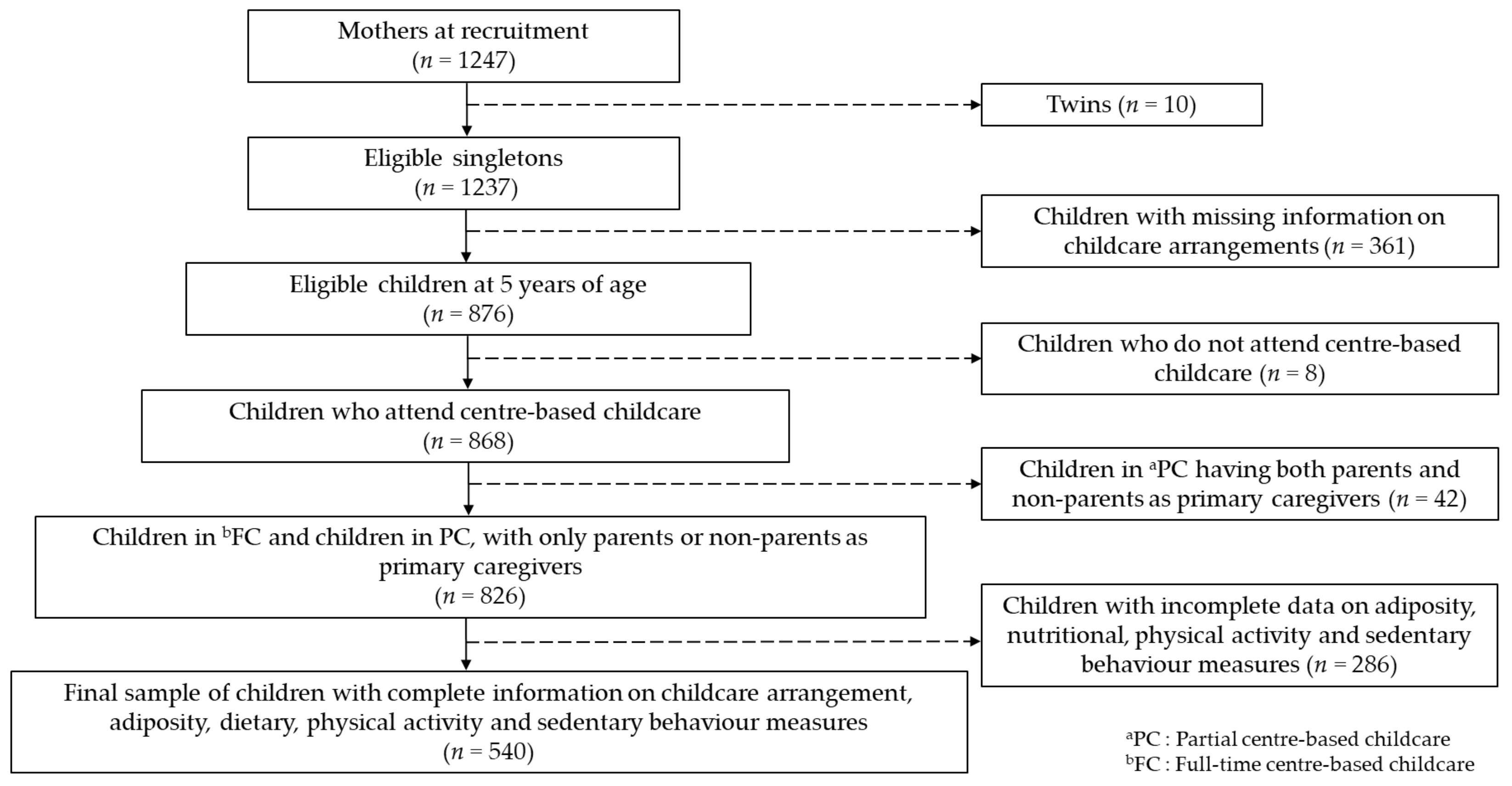
2.1. Study Background and Design
2.2. Assessment of Childcare Arrangement at Age 5
2.3. Dietary Measures at Age 5
2.4. Physical Activity, Sedentary Behaviour and Screen Time Measures at Age 5.5
2.5. Adiposity Measures at Age 6
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Study Sample Characteristics
3.2. Dietary Measures
3.3. Movement Behaviour Measures
3.4. Adiposity Measures
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Onis, M.; Blossner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Double Burden of Malnutrition: Priority Actions on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Pwint, M.K.; Lee, Y.S.; Wong, T.Y.; Saw, S.M. Prevalence of overweight and obesity in Chinese preschoolers in Singapore. Ann. Acad. Med. Singap. 2013, 42, 66–72. [Google Scholar] [PubMed]
- Litwin, S.E. Childhood obesity and adulthood cardiovascular disease: Quantifying the lifetime cumulative burden of cardiovascular risk factors. J. Am. Coll. Cardiol. 2014, 64, 1588–1590. [Google Scholar] [CrossRef] [Green Version]
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-related consequences of childhood obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef]
- Nader, P.R.; O’Brien, M.; Houts, R.; Bradley, R.; Belsky, J.; Crosnoe, R.; Friedman, S.; Mei, Z.; Susman, E.J.; National Institute of Child; et al. Childhood obesity: Causes and consequences. J. Family Med. Prim. Care 2015, 4, 187–192. [Google Scholar]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Family Med. Prim. Care 2015, 4, 187–192. [Google Scholar]
- Davison, K.K.; Birch, L.L. Childhood overweight: A contextual model and recommendations for future research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O. Development of eating behaviors among children and adolescents. Pediatrics 1998, 101 Pt 2, 539–549. [Google Scholar] [PubMed]
- Jones, R.A.; Hinkley, T.; Okely, A.D.; Salmon, J. Tracking physical activity and sedentary behavior in childhood: A systematic review. Am. J. Prev. Med. 2013, 44, 651–658. [Google Scholar] [CrossRef]
- Kremers, S.P.; de Bruijn, G.J.; Visscher, T.L.; van Mechelen, W.; de Vries, N.K.; Brug, J. Environmental influences on energy balance-related behaviors: A dual-process view. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. The Child Care Transition, Innocenti Report Card 8; UNICEF Innocenti Research Centre: Florence, Italy, 2008. [Google Scholar]
- Khoo, K.C. The shaping of childcare and preschool education in Singapore: From separatism to collaboration. Int. J. Child Care Educ. Policy 2010, 4, 23–34. [Google Scholar]
- Early Childhood Development Agency and Singapore. Biannual Report Statistics on ECDC Services; Early Childhood Development Agency: Singapore, 2020. [Google Scholar]
- Black, L.; Matvienko-Sikar, K.; Kearney, P.M. The association between childcare arrangements and risk of overweight and obesity in childhood: A systematic review. Obes. Rev. 2017, 18, 1170–1190. [Google Scholar] [CrossRef] [PubMed]
- Alberdi, G.; McNamara, A.E.; Lindsay, K.L.; Scully, H.A.; Horan, M.H.; Gibney, E.R.; McAuliffe, F.M. The association between childcare and risk of childhood overweight and obesity in children aged 5 years and under: A systematic review. Eur. J. Pediatr. 2016, 175, 1277–1294. [Google Scholar] [CrossRef]
- Wolfenden, L.; Barnes, C.; Jones, J.; Finch, M.; Wyse, R.J.; Kingsland, M.; Tzelepis, F.; Grady, A.; Hodder, R.K.; Booth, D.; et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst. Rev. 2020, 2, CD011779. [Google Scholar] [CrossRef]
- Geoffroy, M.C.; Power, C.; Touchette, E.; Dubois, L.; Boivin, M.; Seguin, J.R.; Tremblay, R.E.; Cote, S.M. Childcare and overweight or obesity over 10 years of follow-up. J. Pediatr. 2013, 162, 753–758.e1. [Google Scholar] [CrossRef]
- Sata, M.; Yamagishi, K.; Sairenchi, T.; Ikeda, A.; Irie, F.; Watanabe, H.; Iso, H.; Ota, H. Impact of Caregiver Type for 3-Year-Old Children on Subsequent Between-Meal Eating Habits and Being Overweight from Childhood to Adulthood: A 20-Year Follow-up of the Ibaraki Children’s Cohort (IBACHIL) Study. J. Epidemiol. 2015, 25, 600–607. [Google Scholar] [CrossRef] [Green Version]
- An, R.; Xiang, X.; Xu, N.; Shen, J. Influence of Grandparental Child Care on Childhood Obesity: A Systematic Review and Meta-Analysis. Child Obes. 2020, 16, 141–153. [Google Scholar] [CrossRef] [Green Version]
- McDonnell, T.; Doyle, O. Maternal employment and childcare during infancy and childhood overweight. Soc. Sci. Med. 2019, 243, 112639. [Google Scholar] [CrossRef] [PubMed]
- Benjamin Neelon, S.E.; Andersen, C.S.; Morgen, C.S.; Kamper-Jørgensen, M.; Oken, E.; Gillman, M.W.; Sørensen, T.I. Early child care and obesity at 12 months of age in the Danish National Birth Cohort. Int. J. Obes. 2015, 39, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; Kremers, S.P.J.; Stafleu, A.; Dagnelie, P.C.; de Vries, N.K.; van Buuren, S.; Thijs, C. Child-care use and the association with body mass index and overweight in children from 7 months to 2 years of age. Int. J. Obes. 2010, 34, 1480–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrady, M.E.; Mitchell, M.J.; Theodore, S.N.; Sersion, B.; Holtzapple, E. Preschool Participation and BMI at Kindergarten Entry: The Case for Early Behavioral Intervention. J. Obes. 2010, 2010, 360407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumeng, J.C.; Kaciroti, N.; Sturza, J.; Krusky, A.M.; Miller, A.L.; Peterson, K.E.; Lipton, R.; Reischl, T.M. Changes in body mass index associated with head start participation. Pediatrics 2015, 135, e449–e456. [Google Scholar] [CrossRef] [Green Version]
- Mandal, B.; Powell, L.M. Child care choices, food intake, and children’s obesity status in the United States. Econ. Hum. Biol. 2014, 14, 50–61. [Google Scholar] [CrossRef]
- Belfield, C.R.; Kelly, I.R. Early education and health outcomes of a 2001 U.S. birth cohort. Econ. Hum. Biol. 2013, 11, 310–325. [Google Scholar] [CrossRef]
- Flores, G.; Lin, H. Factors predicting severe childhood obesity in kindergarteners. Int. J. Obes. 2013, 37, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Koleilat, M.; Harrison, G.G.; Whaley, S.; McGregor, S.; Jenks, E.; Afifi, A. Preschool enrollment is associated with lower odds of childhood obesity among WIC participants in LA County. Matern. Child Health J. 2012, 16, 706–712. [Google Scholar] [CrossRef] [PubMed]
- Lehto, R.; Maki, P.; Ray, C.; Laatikainen, T.; Roos, E. Childcare use and overweight in Finland: Cross-sectional and retrospective associations among 3- and 5-year-old children. Pediatr. Obes. 2016, 11, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Zahir, N.; Heyman, M.B.; Wojcicki, J.M. No association between childcare and obesity at age 4 in low-income Latino children. Pediatr. Obes. 2013, 8, e24–e28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaren, L.; Zarrabi, M.; Dutton, D.J.; Auld, M.C.; Emery, J.C. Child care: Implications for overweight/obesity in Canadian children? Chronic Dis. Inj. Can. 2012, 33, 1–11. [Google Scholar] [CrossRef]
- Lin, S.L.; Leung, G.M.; Hui, L.L.; Lam, T.H.; Schooling, M.C. Is informal child care associated with childhood obesity? Evidence from Hong Kong’s “Children of 1997” birth cohort. Int. J. Epidemiol. 2011, 40, 1238–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, A.; Li, L.; Abbas, J.; Ferguson, B.; Graham, H.; Law, C.G. Millennium Cohort Study Child Health. Is childcare associated with the risk of overweight and obesity in the early years? Findings from the UK Millennium Cohort Study. Int. J. Obes. 2010, 34, 1160–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Promotion Board Singapore. Healthy Meals in Childcare Centres Programme (HMCCP) Toolkit; Health Promotion Board: Singapore, 2016. [Google Scholar]
- Soh, S.E.; Tint, M.T.; Gluckman, P.D.; Godfrey, K.M.; Rifkin-Graboi, A.; Chan, Y.H.; Stunkel, W.; Holbrook, J.D.; Kwek, K.; Chong, Y.S.; et al. Cohort profile: Growing Up in Singapore Towards healthy Outcomes (GUSTO) birth cohort study. Int. J. Epidemiol. 2014, 43, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Sugianto, R.; Chan, M.J.; Wong, S.F.; Shek, L.P.; Tan, K.H.; Chong, Y.S.; Godfrey, K.M.; Tai, B.C.; Chong, M.F. Evaluation of a Quantitative Food Frequency Questionnaire for 5-Year-Old Children in an Asian Population. J. Acad. Nutr. Diet. 2020, 120, 437–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quah, P.L.; Syuhada, G.; Fries, L.R.; Chan, M.J.; Lim, H.X.; Toh, J.Y.; Sugianto, R.; Aris, I.M.; Lee, Y.S.; Yap, F.; et al. Maternal feeding practices in relation to dietary intakes and BMI in 5 year-olds in a multi-ethnic Asian population. PLoS ONE 2018, 13, e0203045. [Google Scholar] [CrossRef]
- Dwyer, G.M.; Hardy, L.L.; Peat, J.K.; Baur, L.A. The validity and reliability of a home environment preschool-age physical activity questionnaire (Pre-PAQ). Int. J. Behav. Nutr. Phys. Act. 2011, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Bernard, J.Y.; Padmapriya, N.; Yao, J.; Goh, C.; Tan, K.H.; Yap, F.; Chong, Y.S.; Shek, L.; Godfrey, K.M.; et al. Socio-demographic and maternal predictors of adherence to 24-hour movement guidelines in Singaporean children. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 70. [Google Scholar] [CrossRef] [Green Version]
- Aris, I.M.; Bernard, J.Y.; Chen, L.W.; Tint, M.T.; Pang, W.W.; Lim, W.Y.; Soh, S.E.; Saw, S.M.; Godfrey, K.M.; Gluckman, P.D.; et al. Infant body mass index peak and early childhood cardio-metabolic risk markers in a multi-ethnic Asian birth cohort. Int. J. Epidemiol. 2017, 46, 513–525. [Google Scholar] [CrossRef] [Green Version]
- Word Health Organization. World Health Organization: Growth Reference 5–19 Years; Word Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Graham, J.W.; Olchowski, A.E.; Gilreath, T.D. How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prev. Sci. 2007, 8, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Robson, S.M.; Khoury, J.C.; Kalkwarf, H.J.; Copeland, K. Dietary intake of children attending full-time child care: What are they eating away from the child-care center? J. Acad. Nutr. Diet. 2015, 115, 1472–1478. [Google Scholar] [CrossRef] [Green Version]
- Kwok, C.S.L.; Wong, M.L.; Vijaya, K.; Sandhu, N.K. Nurturing healthy dietary habits among children and youth in Singapore. Asia Pac. J. Clin. Nutr. 2012, 21, 144–150. [Google Scholar]
- Toups, K.E. Global approaches to promoting whole grain consumption. Nutr. Rev. 2020, 78 (Suppl. 1), 54–60. [Google Scholar] [CrossRef]
- Dunford, E.K.; Popkin, B.M. 37 year snacking trends for US children 1977–2014. Pediatr. Obes. 2018, 13, 247–255. [Google Scholar] [CrossRef]
- Li, B.; Adab, P.; Cheng, K.K. The role of grandparents in childhood obesity in China—Evidence from a mixed methods study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 91. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Waters, C.N.; Compier, T.; Uijtdewilligen, L.; Petrunoff, N.A.; Lim, Y.W.; van Dam, R.; Muller-Riemenschneider, F. Understanding physical activity and sedentary behaviour among preschool-aged children in Singapore: A mixed-methods approach. BMJ Open 2020, 10, e030606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carson, V.; Kuzik, N. Demographic correlates of screen time and objectively measured sedentary time and physical activity among toddlers: A cross-sectional study. BMC Public Health 2017, 17, 187. [Google Scholar] [CrossRef] [Green Version]
- Health Promotion Board Singapore. National Physical Activity Guidelines for Children and Youth Aged up to 18 Years: Professional Guide; Health Promotion Board: Singapore, 2013. [Google Scholar]
- Cardon, G.M.; De Bourdeaudhuij, I.M. Are preschool children active enough? Objectively measured physical activity levels. Res. Q. Exerc. Sport 2008, 79, 326–332. [Google Scholar] [CrossRef]
- Costa, S.; Adams, J.; Phillips, V.; Neelon, S.E.B. The relationship between childcare and adiposity, body mass and obesity-related risk factors: Protocol for a systematic review of longitudinal studies. Syst. Rev. 2016, 5, 141. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.F.; Bian, Q.T.; Zhai, J.G. Analysis of psychological characteristics of obese children. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2665–2670. [Google Scholar] [PubMed]
- Notara, V.; Giannakopoulou, S.-P.; Sakellari, E.; Panagiotakos, D.B. Family-related characteristics and childhood obesity: A systematic literature review. Int. J. Caring Sci. 2020, 13, 61–72. [Google Scholar]
- Gray, L.A.; Alava, M.H.; Kelly, M.P.; Campbell, M.J. Family lifestyle dynamics and childhood obesity: Evidence from the millennium cohort study. BMC Public Health 2018, 18, 500. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Childcare Type | p-Value | |||
|---|---|---|---|---|
| FC (n = 272) | PCP (n = 192) | PCN (n = 76) | ||
| Child characteristics | ||||
| Sex | 0.629 | |||
| Male | 148 (54.4) | 96 (50.0) | 41 (53.9) | |
| Female | 124 (45.6) | 96 (50.0) | 35 (46.1) | |
| Birth order | 0.002 | |||
| First child | 128 (47.1) a | 64 (33.3) b | 41 (53.9) a | |
| Second child and above | 144 (52.9) a | 128 (66.7) b | 35 (46.1) a | |
| Childcare commencement (months) | <0.001 | |||
| Between 2 and 24 months | 145 (53.3) a | 23 (12.0) b | 15 (19.7) b | |
| Between 25 and 60 months | 127 (46.7) a | 169 (88.0) b | 61 (80.3) b | |
| Birth weight (kg) | 3.2 ± 0.4 | 3.1 ± 0.4 | 3.1 ± 0.5 | 0.155 |
| Sum of skinfold thicknesses at birth (mm) | 10.5 ± 2.1 | 10.3 ± 2.2 | 10.0 ± 2.3 | 0.136 |
| Maternal characteristics | ||||
| Age (years) | 31.0 ±5.4 a,b | 31.8 ± 5.0 a | 30.1 ± 5.0 b | 0.040 |
| Ethnicity | <0.001 | |||
| Chinese | 195 (71.7) a | 78 (40.6) b | 43 (56.6) c | |
| Malay | 49 (18.0) a | 63 (32.8) b | 17 (22.4) a,b | |
| Indian | 28 (10.3) a | 51 (26.6) b | 16 (21.1) b | |
| Highest education level | 0.015 | |||
| Secondary or lower | 69 (25.4) a | 72 (37.5) b | 14 (18.4) a | |
| Post-Secondary | 101 (37.1) | 59 (30.7) | 32 (42.1) | |
| University or above | 102 (37.5) | 61 (31.8) | 30 (39.5) | |
| Employment | <0.001 | |||
| Employed | 209 (76.8) a | 95 (49.5) b | 70 (92.1) c | |
| Unemployed | 63 (23.2) a | 97 (50.5) b | 6 (7.9) c | |
| Household income | 0.037 | |||
| <$2000 | 34 (12.5) a | 40 (20.8) b | 7 (9.2) a | |
| $2000–$5999 | 147 (54.0) | 103 (53.6) | 44 (57.9) | |
| >$6000 | 91 (33.5) | 49 (25.5) | 25 (32.9) | |
| Total physical activity at 6 years postpartum (min/week) | 0.019 | |||
| 0 | 108 (39.7) a | 55 (28.6) b | 25 (32.9) a,b | |
| >0–149 | 107 (39.3) | 72 (37.5) | 32 (42.1) | |
| ≥150 | 57 (21.0) a | 65 (33.9) b | 19 (25.0) a,b | |
| TV viewing at 6 years postpartum (min/week) | 0.094 | |||
| <60 | 143 (52.6) | 81 (42.2) | 43 (56.6) | |
| 60–120 | 95 (34.9) | 76 (39.6) | 24 (31.6) | |
| >120 | 34 (12.5) | 35 (18.2) | 9 (11.8) | |
| Weight status at 6 years postpartum (BMI) | 0.004 | |||
| Underweight/normal (<23 kg/m2) | 135 (49.6) a | 67 (34.9) b | 38 (50.0) a | |
| Overweight/obese (≥23 kg/m2) | 137 (50.4) a | 125 (65.1) b | 38 (50.0) a | |
| Childcare Type | p-Value | |||
|---|---|---|---|---|
| FC (n = 272) | PCP (n = 192) | PCN (n = 76) | ||
| Food group, median (IQR) | ||||
| Fruits (g/day) | 87.4 (103.0) | 85.4 (123.0) | 77.5 (85.9) | 0.079 |
| Vegetables (g/day) | 26.7 (41.7) | 26.3 (49.6) | 24.8 (41.1) | 0.622 |
| Whole grains (g/day) | 0.0 (23.7) a | 11.2 (45.0) b | 0.6 (36.9) a,b | 0.001 |
| Deep-fried food (g/day) | 17.5 (23.4) a | 25.7 (32.0) b | 22.1 (33.0) b | 0.003 |
| Fast food (g/day) | 12.9 (18.1) a | 15.7 (21.9) a,b | 17.9 (30.0) b | 0.035 |
| Sweet snacks (g/day) | 27.2 (33.1) | 29.7 (37.8) | 32.7 (39.1) | 0.145 |
| Sugar-sweetened beverages (mL/day) | 113.5 (142.5) | 110.2 (156.5) | 115.1(124.3) | 0.833 |
| Eating out frequency, n (%) | 0.314 | |||
| At least once per day | 15 (5.5) | 9 (4.7) | 3 (3.9) | |
| At least once per week | 180 (66.2) | 111 (57.8) | 50 (65.8) | |
| At least once per month or rarely or never | 77 (28.3) | 72 (37.5) | 23 (30.3) | |
| Snacking frequency, n (%) | 0.030 | |||
| Snacks all day but has meals | 35 (13.0) a | 46 (24.0) b | 17 (22.7) b | |
| Snacks only during tea time | 170 (63.2) | 111 (57.8) | 44 (58.7) | |
| Does not snack much | 64 (23.8) | 35 (18.2) | 14 (18.7) | |
| Type of Childcare | p-Value | |||
|---|---|---|---|---|
| FC (n = 272) | PCP (n = 192) | PCN (n = 76) | ||
| Physical activity measures | ||||
| Total physical activity (min/day) | 121.8 (140.7) | 107.1 (146.3) | 125.4 (141.4) | 0.284 |
| Total MVPA (min/day) | 59.9 (91.4) | 50.7 (91.1) | 50.4 (92.7) | 0.725 |
| Sedentary behaviour measures | ||||
| Total sedentary behaviour (min/day) | 187.9 (136.1) a | 216.8 (184.6) b | 260.4 (176.8) b | 0.005 |
| Total screen time (min/day) | 68.6 (83.6) a | 77.1 (119.8) a | 115.7 (117.5) b | <0.001 |
| Unadjusted Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|
| β | 95% CI | p-Value | β | 95% CI | p-Value | |
| BMI z-score | ||||||
| FC | Reference | Reference | ||||
| PCP | 0.23 | −0.001, 0.46 | 0.051 | 0.12 | −0.15, 0.38 | 0.387 |
| PCN | 0.38 | 0.07, 0.70 | 0.016 | 0.34 | 0.01, 0.66 | 0.042 |
| Sum of skinfold thicknesses | ||||||
| FC | Reference | Reference | ||||
| PCP | 2.46 | 0.19, 4.73 | 0.033 | 0.88 | −1.75, 3.51 | 0.511 |
| PCN | 4.46 | 1.34, 7.58 | 0.005 | 3.75 | 0.53, 6.97 | 0.022 |
| Overweight/Obese | |||
|---|---|---|---|
| Adjusted Odds Ratio | 95% CI | p-Value | |
| FC | Reference | ||
| PCP | 1.54 | 0.83, 2.87 | 0.169 |
| PCN | 3.55 | 1.78, 7.05 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, B.W.-X.; Toh, J.Y.; Sugianto, R.; Chia, A.; Tint, M.T.; Yuan, W.L.; Padmapriya, N.; Lança, C.; Saw, S.-M.; Lee, Y.S.; et al. Associations of Childcare Arrangements with Adiposity Measures in a Multi-Ethnic Asian Cohort: The GUSTO Study. Int. J. Environ. Res. Public Health 2021, 18, 12178. https://doi.org/10.3390/ijerph182212178
Wong BW-X, Toh JY, Sugianto R, Chia A, Tint MT, Yuan WL, Padmapriya N, Lança C, Saw S-M, Lee YS, et al. Associations of Childcare Arrangements with Adiposity Measures in a Multi-Ethnic Asian Cohort: The GUSTO Study. International Journal of Environmental Research and Public Health. 2021; 18(22):12178. https://doi.org/10.3390/ijerph182212178
Chicago/Turabian StyleWong, Beverly Wen-Xin, Jia Ying Toh, Ray Sugianto, Airu Chia, Mya Thway Tint, Wen Lun Yuan, Natarajan Padmapriya, Carla Lança, Seang-Mei Saw, Yung Seng Lee, and et al. 2021. "Associations of Childcare Arrangements with Adiposity Measures in a Multi-Ethnic Asian Cohort: The GUSTO Study" International Journal of Environmental Research and Public Health 18, no. 22: 12178. https://doi.org/10.3390/ijerph182212178
APA StyleWong, B. W. -X., Toh, J. Y., Sugianto, R., Chia, A., Tint, M. T., Yuan, W. L., Padmapriya, N., Lança, C., Saw, S. -M., Lee, Y. S., Shek, L. P. -C., Tan, K. H., Yap, F., Godfrey, K. M., Chong, Y. -S., Müller-Riemenschneider, F., Eriksson, J. G., Chan, S. -Y., & Chong, M. F. -F. (2021). Associations of Childcare Arrangements with Adiposity Measures in a Multi-Ethnic Asian Cohort: The GUSTO Study. International Journal of Environmental Research and Public Health, 18(22), 12178. https://doi.org/10.3390/ijerph182212178