
Factor Structure and Psychometric Properties for the PTSD Checklist of Chinese Adolescents in the Closed Period after the COVID-19 Outbreak

Abstract
:1. Introduction
The Current Study
2. Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Analytical Plan
3. Results
3.1. Descriptive Statistics
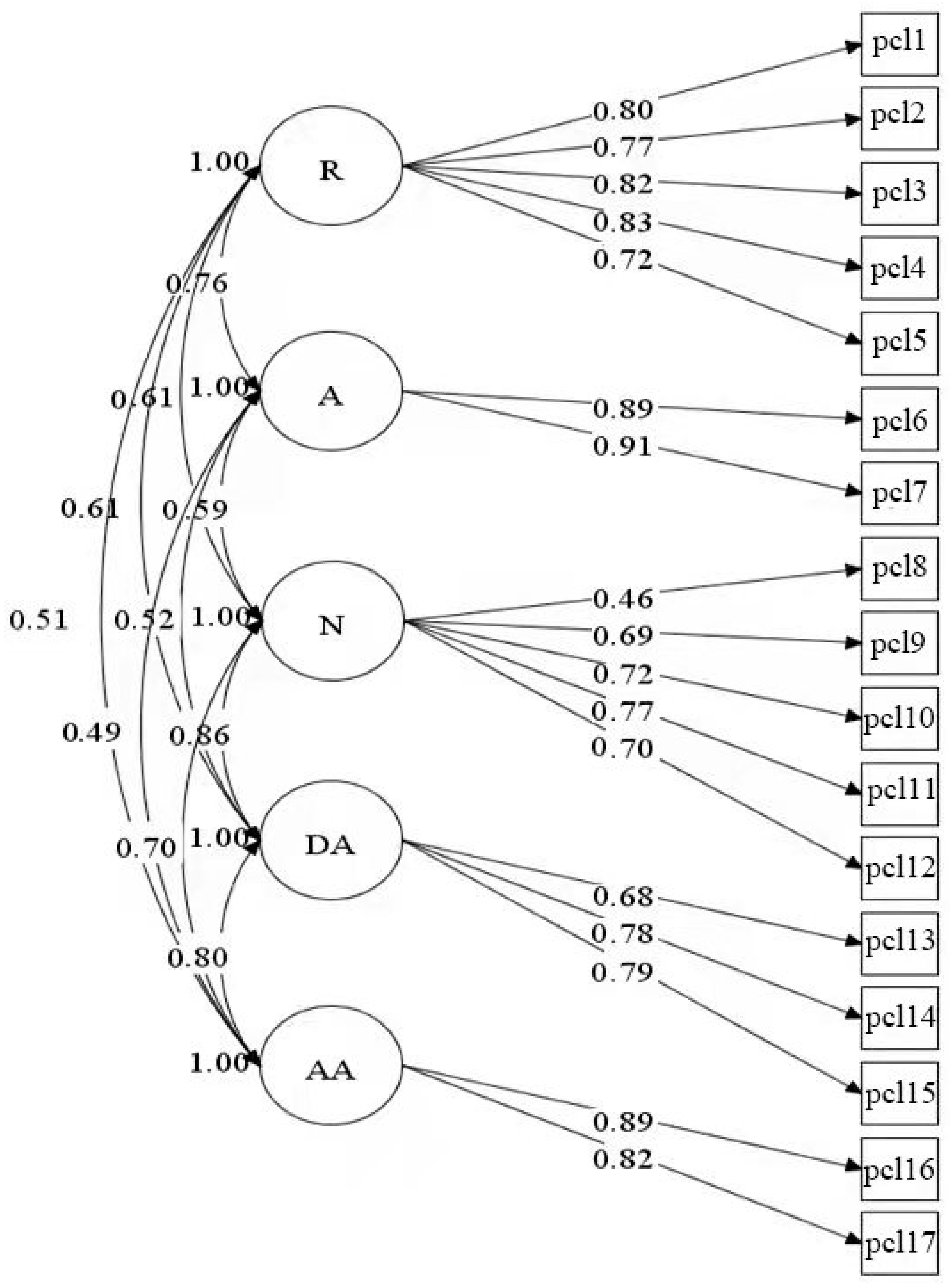
3.2. Factor Structure of the PTSD
3.3. Measurement Invariance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, M.C.; Lee, W.; Hur, J.; Park, D. Chest Computed Tomography Findings in Asymptomatic Patients with COVID-19. Respiration 2020, 99, 748–754. [Google Scholar] [CrossRef]
- Chang, M.; Baek, J.; Park, D. Lessons from South Korea Regarding the Early Stage of the COVID-19 Outbreak. Healthcare 2020, 8, 229. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.; Park, D. Incidence of Post-Traumatic Stress Disorder After Coronavirus Disease. Healthcare 2020, 8, 373. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Currier, G.W.; Zhao, X.; Jiang, Y.; Zhou, W.; Wei, J. Posttraumatic stress disorder in convalescent severe acute respiratory syndrome patients: A 4-year follow-up study. Gen. Hosp. Psychiatry 2009, 31, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Ho, S.C.; Chan, V.L. Risk factors for chronic post-traumatic stress disorder (PTSD) in SARS survivors. Gen. Hosp. Psychiatry 2010, 32, 590–598. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Boyraz, G.; Legros, D.N. Coronavirus Disease (COVID-19) and Traumatic Stress: Probable Risk Factors and Correlates of Posttraumatic Stress Disorder. J. Loss Trauma 2020, 25, 503–522. [Google Scholar] [CrossRef]
- Horesh, D.; Brown, A.D. Traumatic stress in the age of COVID-19: A call to close critical gaps and adapt to new realities. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 331–335. [Google Scholar] [CrossRef]
- Bo, H.-X.; Li, W.; Yang, Y.; Wang, Y.; Zhang, Q.; Cheung, T.; Wu, X.; Xiang, Y.-T. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol. Med. 2020, 51, 1052–1053. [Google Scholar] [CrossRef] [Green Version]
- Karatzias, T.; Shevlin, M.; Murphy, J.; Mcbride, O.; Ben-Ezra, M.; Bentall, R.P.; Vallières, F.; Hyland, P. Posttraumatic SO-VID-19 Pandemic in Ireland: A Population-Based Study. J. Trauma Stress 2020, 33, 365–370. [Google Scholar] [CrossRef]
- Haderlein, T.P.; Wong, M.S.; Yuan, A.; Llorente, M.D.; Washington, D.L. Association of PTSD with COVID-19 testing and infection in the Veterans Health Administration. J. Psychiatr. Res. 2020, 143, 504–507. [Google Scholar] [CrossRef]
- Guessoum, S.B.; Lachal, J.; Radjack, R.; Carretier, E.; Minassian, S.; Benoit, L.; Moro, M.R. Adolescent psychiatric disorders during the COVID-19 pandemic and lockdown—ScienceDirect. Psychiat Res. 2020, 291, 113264. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.; Bao, Y.; Huang, X.; Shi, J.; Lu, L. Mental health considerations for children quarantined because of COVID-19. Lancet Child Adolesc. Health 2020, 4, 347–349. [Google Scholar] [CrossRef] [Green Version]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Duan, W.; Chen, Z. Latent Profiles of the Comorbidity of Post-traumatic Stress Disorder and Generalized Anxiety Disorder among Children and Adolescents who are Potentially Infected with COVID-19. Child Youth Serv. Rev. 2020, 116, 105235. [Google Scholar] [CrossRef]
- Zhou, X.; Wu, X.C.; An, Y.Y.; Lin, C.D. Assessing the Latent Structure of PTSD among Chinese Adolescent after Earthquake. Psychol. Dev. Educ. 2017, 33, 206–215. [Google Scholar] [CrossRef]
- Geier, T.J.; Hunt, J.C.; Hanson, J.L.; Heyrman, K.; Deroon-Cassini, T.A. Validation of Abbreviated Four- and Eight-Item Versions of the PTSD Checklist for DSM-5 in a Traumatically Injured Sample: Abbreviated PCL-5 Validation in Traumatic Injury. J. Trauma Stress 2020, 33, 218–226. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Tsai, J.; Armour, C.; Mota, N.; Harpaz-Rotem, I.; Southwick, S.M. Functional significance of a novel 7-factor model of DSM-5 PTSD symptoms: Results from the National Health and Resilience in Veterans Study. J. Affect. Disord. 2015, 174, 522–526. [Google Scholar] [CrossRef]
- Boasso, A.M.; Steenkamp, M.M.; Fox, A.B.; Nash, W.P.; Larson, J.L.; Litz, B.T. The structure of PTSD in active-duty marines across the deployment cycle. Psychol. Trauma Theory Res. Pract. Policy 2016, 8, 127–134. [Google Scholar] [CrossRef]
- Armour, C.; Műllerová, J.; Elhai, J.D. A systematic literature review of PTSD’s latent structure in the Diagnostic and Statistical Manual of Mental Disorders: DSM-IV to DSM-5. Clin. Psychol. Rev. 2016, 44, 60–74. [Google Scholar] [CrossRef]
- Zhou, X.; Wu, X.; Zhen, R. Assessing the latent structure of DSM-5 PTSD among Chinese adolescents after the Ya’an earthquake. Psychiatry Res. 2017, 254, 33–39. [Google Scholar] [CrossRef]
- Yue, J.; Zang, X.; Le, Y.; An, Y. Anxiety, depression and PTSD among children and their parent during 2019 novel corona-virus disease (COVID-19) outbreak in China. Curr. Psychol. 2020, 14, 1–8. [Google Scholar]
- Brennan, C.; Worrall-Davies, A.; Mcmillan, D.; Gilbody, S.; House, A. The Hospital Anxiety and Depression Scale: A di-agnostic meta-analysis of case-finding ability. J. Psychosom. Res. 2010, 69, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Brähler, E. Normative values for the hospital anxiety and depression scale (HADS) in the general German population. J. Psychosom. Res. 2011, 71, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Guo, X.; Shang, Z.; Sun, Z.; Jia, Y.; Sun, L.; Liu, W. China experience from COVID-19: Mental health in mandatory quarantine zones urgently requires intervention. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S3–S5. [Google Scholar] [CrossRef] [PubMed]
- Mowbray, H. In Beijing, coronavirus 2019-nCoV has created a siege mentality. BMJ 2020, 368, m516. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R.A.; Nickerson, A.; Creamer, M.; O’Donnell, M.; Forbes, D.; Galatzer-Levy, I.; McFarlane, A.C.; Silove, D. Trajectory of post-traumatic stress following traumatic injury: 6-year follow-up. Br. J. Psychiatry 2015, 206, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Gelaye, B.; Zheng, Y.; Medina-Mora, M.E.; Rondon, M.B.; Sánchez, S.E.; Williams, M.A. Validity of the posttraumatic stress disorders (PTSD) checklist in pregnant women. BMC Psychiatry 2017, 17, 1–10. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Hamam, A.A.; Milo, S.; Mor, I.; Shaked, E.; Eliav, A.S.; Lahav, Y. Peritraumatic reactions during the COVID-19 pandemic—The contribution of posttraumatic growth attributed to prior trauma. J. Psychiatr. Res. 2021, 132, 23–31. [Google Scholar] [CrossRef]
- Alshehri, F.S.; Alatawi, Y.; Alghamdi, B.S.; Alhifany, A.A.; Alharbi, A. Prevalence of post-traumatic stress disorder during the COVID-19 pandemic in Saudi Arabia. Saudi Pharm. J. 2020, 28, 1666–1673. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation: Brochure, 2017. Available online: https://apps.who.int/iris/handle/10665/255416 (accessed on 16 November 2021).
- Wang, M.C.; Dai, X.Y.; Wan, J. Factor Structure of PTSD Checklist: A Confirmatory Factor Analysis Study in Adolescents from Earthquake Region. Chin. J. Clin. Psychol. 2009, 17, 420–423. [Google Scholar]
- Taylor, S.; Kuch, K.; Koch, W.J.; Crockett, D.J.; Passey, G. The structure of posttraumatic stress symptoms. J. Abnorm. Psychol. 1998, 107, 154–160. [Google Scholar] [CrossRef]
- Cordova, M.J.; Studts, J.L.; Hann, D.M.; Jacobsen, P.B.; Andrykowski, M.A. Symptom structure of PTSD following breast cancer. J. Trauma. Stress 2000, 13, 301–319. [Google Scholar] [CrossRef]
- King, D.W.; Leskin, G.A.; King, L.A.; Weathers, F.W. Confirmatory factor analysis of the clinician-administered PTSD Scale: Evidence for the dimensionality of posttraumatic stress disorder. Psychol. Assess. 1998, 10, 90–96. [Google Scholar] [CrossRef]
- Simms, L.J.; Watson, D.; Doebbelling, B.N. Confirmatory factor analyses of posttraumatic stress symptoms in deployed and nondeployed veterans of the Gulf War. J. Abnorm. Psychol. 2002, 111, 637. [Google Scholar] [CrossRef] [PubMed]
- Elhai, J.D.; Biehn, T.L.; Armour, C.; Klopper, J.J.; Frueh, B.C.; Palmieri, P.A. Evidence for a unique PTSD construct represented by PTSD’s D1-D3 symptoms. J. Anxiety Disord. 2011, 25, 340–345. [Google Scholar] [CrossRef]
- Cronbach, L.J.; Shavelson, R.J. My Current Thoughts on Coefficient Alpha and Successor Procedures. Educ. Psychol. Meas. 2004, 64, 391–418. [Google Scholar] [CrossRef]
- Perrot, B.; Bataille, E.; Hardouin, J.-B. validscale: A Command to Validate Measurement Scales. Stata J. Promot. Commun. Stat. Stata 2018, 18, 29–50. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating Goodness-of-Fit Indexes for Testing Measurement Invariance. Struct. Equ Modeling 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Church, A.T.; Alvarez, J.M.; Mai, N.T.; French, B.F.; Katigbak, M.S.; Ortiz, F.A. Are cross-cultural comparisons of per-sonality profiles meaningful? Differential item and facet functioning in the Revised NEO Personality Inventory. J. Pers. Soc. Psychol. 2011, 101, 1068–1089. [Google Scholar] [CrossRef] [PubMed]
- Shchebetenko, S.; Kaлyrин, A.Y.; Mishkevich, A.M.; Soto, C.J.; John, O.P. Measurement Invariance and Sex and Age Differences of the Big Five Inventory–2: Evidence from the Russian Version. Assessment 2019, 27, 472–486. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD Checklist: Reliability, Validity and Diagnostic Utility. Presented at the Meeting of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, October 1993; Available online: https://istss.org/clinical-resources/assessing-trauma/ptsd-checklist-dsm-5/ptsd-checklist-dsm-iv (accessed on 18 October 2021).
- Liu, A.; Tan, H.; Zhou, J.; Li, S.; Yang, T.; Sun, Z.; Wen, S.W. Brief Screening Instrument of Posttraumatic Stress Disorder for Children and Adolescents 7–15 Years of Age. Child Psychiatry Hum. Dev. 2007, 38, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Ying, L.-H.; Wu, X.-C.; Lin, C.-D. Longitudinal linkages between depressive and posttraumatic stress symptoms in adolescent survivors following the Wenchuan earthquake in China: A three-wave, cross-lagged study. Sch. Psychol. Int. 2012, 33, 416–432. [Google Scholar] [CrossRef]
- Dobie, D.J.; Kivlahan, D.R.; Maynard, C.; Bush, K.R.; McFall, M.; Epler, A.J.; A Bradley, K. Screening for post-traumatic stress disorder in female Veteran’s Affairs patients: Validation of the PTSD checklist. Gen. Hosp. Psychiatry 2002, 24, 367–374. [Google Scholar] [CrossRef]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef]
- StataCorp. Stata/MP 13.1 for Windows; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; The Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Satorra, A.; Bentler, P.M. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika 2001, 66, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Marsh, H.W.; Hau, K.T.; Wen, Z. In Search of Golden Rules: Comment on Hypothesis-Testing Approaches to Setting Cutoff Values for Fit Indexes and Dangers in Overgeneralizing Hu and Bentler’s (1999) Findings. Struct. Equ. Modeling 2004, 11, 320–341. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Raftery, A.E. Bayesian model selection in social research. Sociol. Methodol. 1995, 25, 111–163. [Google Scholar] [CrossRef]
- Peterson, R.A. A Meta-analysis of Cronbach’s Coefficient Alpha. J. Consum. Res. 1994, 21, 381–391. [Google Scholar] [CrossRef]
- Vandenberg, R. Toward a Further Understanding of and Improvement in Measurement Invariance Methods and Procedures. Organ. Res. Methods 2002, 5, 139–158. [Google Scholar] [CrossRef]
- Wang, L.; Cao, C.; Wang, R.; Zhang, J.; Li, Z. The dimensionality of PTSD symptoms and their relationship to health-related quality of life in Chinese earthquake survivors. J. Anxiety Disord. 2012, 26, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Boal, A.L.; Vaughan, C.A.; Sims, C.S.; Miles, J.N.V. Measurement invariance across administration mode: Examining the Posttraumatic Stress Disorder (PTSD) Checklist. Psychol. Assess. 2017, 29, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Cheung, G.W. Testing Factorial Invariance across Groups: A Reconceptualization and Proposed New Method. J. Manag. 1999, 25, 1–27. [Google Scholar] [CrossRef]


{kind=link}
| Items | Min | Max | M | SD | M6 | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|
| pcl1. Intrusive thoughts | 1 | 5 | 1.82 | 1.01 | RM ± SD = 7.90 ± 3.84 | 1.33 | 4.37 |
| pcl2. Nightmares | 1 | 5 | 1.36 | 0.78 | 2.69 | 10.84 | |
| pcl3. Reliving trauma | 1 | 5 | 1.65 | 1.02 | 1.63 | 5.03 | |
| pcl4. Emotional cue reactivity | 1 | 5 | 1.75 | 1.04 | 1.51 | 4.80 | |
| pcl5. Physiological cue reactivity | 1 | 5 | 1.32 | 0.73 | 2.87 | 12.04 | |
| pcl6. Avoidance of thoughts | 1 | 5 | 1.54 | 0.93 | AM ± SD = 3.06 ± 1.76 | 1.90 | 6.21 |
| pcl7. Avoidance of reminders | 1 | 5 | 1.52 | 0.92 | 1.99 | 6.64 | |
| pcl8. Trauma-related amnesia | 1 | 5 | 1.47 | 0.80 | NM ± SD = 7.47 ± 3.34 | 1.88 | 6.64 |
| pcl9. Loss of interest | 1 | 5 | 1.40 | 0.81 | 2.28 | 8.18 | |
| pcl10. Feeling detached | 1 | 5 | 1.55 | 0.91 | 1.85 | 6.14 | |
| pcl11. Feeling numb | 1 | 5 | 1.56 | 1.01 | 1.98 | 6.24 | |
| pcl12. Hopelessness | 1 | 5 | 1.49 | 0.94 | 2.13 | 7.07 | |
| pcl13. Difficulty sleeping | 1 | 5 | 1.62 | 1.05 | DAM ± SD = 5.14 ± 2.71 | 1.84 | 5.65 |
| pcl14. Irritable/angry | 1 | 5 | 1.76 | 1.10 | 1.48 | 4.33 | |
| pcl15. Difficulty concentrating | 1 | 5 | 1.77 | 1.07 | 1.41 | 4.27 | |
| pcl16. Overly alert | 1 | 5 | 1.93 | 1.25 | AAM ± SD = 3.86 ± 2.30 | 1.22 | 3.33 |
| pcl17. Easily startled | 1 | 5 | 1.93 | 1.22 | 1.21 | 3.41 | |
| PCL | 17 | 85 | 27.44 | 11.24 | - | - | - |
| Model | MLM χ2 | df | CFI | TLI | RMSEA | SRMR | AIC | BIC | ΔBIC |
|---|---|---|---|---|---|---|---|---|---|
| M1 | 1286.48 | 119 | 0.73 | 0.69 | 0.10 | 0.09 | 36,823.23 | 37,069.00 | |
| M2 | 606.02 | 118 | 0.89 | 0.87 | 0.07 | 0.05 | 35,468.54 | 35,719.13 | −1349.87 |
| M3 | 698.10 | 116 | 0.87 | 0.84 | 0.07 | 0.06 | 35,661.65 | 35,921.87 | 202.74 |
| M4a | 575.68 | 113 | 0.95 | 0.94 | 0.07 | 0.04 | 34,872.21 | 35,146.89 | −774.98 |
| M4b | 501.19 | 113 | 0.96 | 0.95 | 0.06 | 0.04 | 34,797.72 | 35,072.40 | −74.49 |
| M5a | 777.02 | 115 | 0.92 | 0.91 | 0.08 | 0.06 | 35,069.55 | 35,334.59 | 262.19 |
| M5b | 701.70 | 115 | 0.93 | 0.92 | 0.08 | 0.06 | 34,994.23 | 35,259.27 | −75.32 |
| M6 | 375.76 | 109 | 0.97 | 0.96 | 0.05 | 0.03 | 34,680.28 | 34,974.24 | −285.03 |
| Items | R | A | N | DA | AA |
|---|---|---|---|---|---|
| α | 0.89 | 0.90 | 0.80 | 0.79 | 0.84 |
| H | 0.53 | 0.55 | 0.50 | 0.56 | 0.52 |
| Hj-min | 0.64 | 0.82 | 0.34 | 0.54 | 0.74 |
| pcl1 | 0.75 | 0.58 | 0.42 | 0.39 | 0.35 |
| pcl2 | 0.73 | 0.55 | 0.45 | 0.43 | 0.34 |
| pcl3 | 0.76 | 0.56 | 0.47 | 0.46 | 0.41 |
| pcl4 | 0.77 | 0.62 | 0.42 | 0.44 | 0.40 |
| pcl5 | 0.67 | 0.52 | 0.47 | 0.46 | 0.33 |
| pcl6 | 0.64 | 0.81 | 0.47 | 0.40 | 0.40 |
| pcl7 | 0.65 | 0.81 | 0.51 | 0.44 | 0.42 |
| pcl8 | 0.31 | 0.34 | 0.40 | 0.35 | 0.29 |
| pcl9 | 0.40 | 0.40 | 0.61 | 0.53 | 0.43 |
| pcl10 | 0.43 | 0.44 | 0.65 | 0.51 | 0.46 |
| pcl11 | 0.45 | 0.40 | 0.65 | 0.62 | 0.50 |
| pcl12 | 0.36 | 0.34 | 0.60 | 0.58 | 0.47 |
| pcl13 | 0.40 | 0.35 | 0.56 | 0.57 | 0.51 |
| pcl14 | 0.46 | 0.40 | 0.58 | 0.67 | 0.58 |
| pcl15 | 0.45 | 0.36 | 0.62 | 0.67 | 0.57 |
| pcl16 | 0.43 | 0.41 | 0.56 | 0.64 | 0.73 |
| pcl17 | 0.39 | 0.40 | 0.52 | 0.59 | 0.73 |
| Model | MLM χ2 | df | CFI | TLI | RMSEA | SRMR | AIC | BIC | ΔCFI | ΔTLI |
|---|---|---|---|---|---|---|---|---|---|---|
| Across Gender | ||||||||||
| Female | 185.47 | 109 | 0.97 | 0.96 | 0.04 | 0.04 | 16,340.87 | 16,590.03 | ||
| Male | 138.87 | 109 | 0.99 | 0.98 | 0.02 | 0.03 | 18,326.45 | 18,580.54 | ||
| Configural | 597.25 | 218 | 0.96 | 0.95 | 0.06 | 0.04 | 34,667.33 | 35,255.24 | ||
| Weak | 615.73 | 230 | 0.96 | 0.95 | 0.06 | 0.04 | 34,661.80 | 35,191.88 | 0.00 | 0.00 |
| Scalar | 632.80 | 242 | 0.96 | 0.95 | 0.04 | 0.04 | 34,654.87 | 35,127.12 | 0.00 | 0.00 |
| Strict | 688.76 | 259 | 0.95 | 0.95 | 0.06 | 0.05 | 34,676.83 | 35,067.16 | −0.01 | 0.00 |
| Across with or without PTSD Symptom | ||||||||||
| With PTSD | 119.27 | 109 | 0.98 | 0.98 | 0.03 | 0.06 | 8104.46 | 8289.72 | ||
| Without PTSD | 206.46 | 109 | 0.95 | 0.94 | 0.03 | 0.05 | 22,656.89 | 22,939.76 | ||
| Configural | 465.62 | 218 | 0.94 | 0.93 | 0.05 | 0.05 | 30,696.44 | 31,284.34 | ||
| Weak | 513.16 | 230 | 0.93 | 0.92 | 0.05 | 0.05 | 30,719.98 | 31,250.06 | −0.01 | −0.01 |
| Scalar | 582.49 | 242 | 0.92 | 0.91 | 0.06 | 0.06 | 30,765.31 | 31,237.56 | −0.01 | −0.01 |
| Across early adolescents and late adolescents | ||||||||||
| early adolescents | 244.62 | 109 | 0.97 | 0.96 | 0.05 | 0.03 | 16,935.14 | 17,183.88 | ||
| late adolescents | 288.62 | 109 | 0.96 | 0.95 | 0.06 | 0.04 | 17,186.74 | 17,439.67 | ||
| Configural | 533.24 | 218 | 0.96 | 0.96 | 0.06 | 0.04 | 34,121.88 | 34,708.18 | ||
| Weak | 559.35 | 230 | 0.96 | 0.96 | 0.06 | 0.04 | 34,123.99 | 34,652.62 | 0.00 | 0.00 |
| Scalar | 568.81 | 242 | 0.96 | 0.96 | 0.06 | 0.04 | 34,109.45 | 34,580.41 | 0.00 | 0.00 |
| Strict | 615.46 | 259 | 0.96 | 0.96 | 0.06 | 0.04 | 34,122.10 | 34,511.37 | 0.00 | 0.00 |
| Across Time | ||||||||||
| T1 | 342.25 | 109 | 0.94 | 0.92 | 0.08 | 0.05 | 9816.92 | 10,042.65 | ||
| T2 | 280.46 | 109 | 0.94 | 0.92 | 0.07 | 0.05 | 11,353.39 | 11,579.32 | ||
| Configural | 1034.45 | 465 | 0.92 | 0.90 | 0.06 | 0.05 | 20,775.30 | 21,382.72 | ||
| Weak | 1059.36 | 477 | 0.92 | 0.90 | 0.06 | 0.05 | 20,776.21 | 21,339.18 | 0.00 | 0.00 |
| Scalar | 1090.63 | 489 | 0.91 | 0.90 | 0.06 | 0.05 | 20,783.48 | 21,302.01 | −0.01 | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.; Gao, R.; Yang, T. Factor Structure and Psychometric Properties for the PTSD Checklist of Chinese Adolescents in the Closed Period after the COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2021, 18, 12245. https://doi.org/10.3390/ijerph182212245
Chen W, Gao R, Yang T. Factor Structure and Psychometric Properties for the PTSD Checklist of Chinese Adolescents in the Closed Period after the COVID-19 Outbreak. International Journal of Environmental Research and Public Health. 2021; 18(22):12245. https://doi.org/10.3390/ijerph182212245
Chicago/Turabian StyleChen, Wei, Rongfen Gao, and Tao Yang. 2021. "Factor Structure and Psychometric Properties for the PTSD Checklist of Chinese Adolescents in the Closed Period after the COVID-19 Outbreak" International Journal of Environmental Research and Public Health 18, no. 22: 12245. https://doi.org/10.3390/ijerph182212245
APA StyleChen, W., Gao, R., & Yang, T. (2021). Factor Structure and Psychometric Properties for the PTSD Checklist of Chinese Adolescents in the Closed Period after the COVID-19 Outbreak. International Journal of Environmental Research and Public Health, 18(22), 12245. https://doi.org/10.3390/ijerph182212245